
Abstract
Nipple pain is a common reason for premature cessation of breastfeeding. Despite the benefits of breastfeeding for both infant and mother, clinical support for problems such as maternal nipple pain remains a research frontier. Maternal pharmaceutical treatments, and infant surgery and bodywork interventions are commonly recommended for lactation-related nipple pain without evidence of benefit. The pain is frequently attributed to mammary dysbiosis, candidiasis, or infant anatomic anomaly (including to diagnoses of posterior or upper lip-tie, high palate, retrognathia, or subtle cranial nerve abnormalities). Although clinical protocols universally state that improved fit and hold is the mainstay of treatment of nipple pain and wounds, the biomechanical parameters of pain-free fit and hold remain an omitted variable bias in almost all clinical breastfeeding research. This article reviews the research literature concerning aetiology, classification, prevention, and management of lactation-related nipple–areolar complex (NAC) pain and damage. Evolutionary and complex systems perspectives are applied to develop a narrative synthesis of the heterogeneous and interdisciplinary evidence elucidating nipple pain in breastfeeding women. Lactation-related nipple pain is most commonly a symptom of inflammation due to repetitive application of excessive mechanical stretching and deformational forces to nipple epidermis, dermis and stroma during milk removal. Keratinocytes lock together when mechanical forces exceed desmosome yield points, but if mechanical loads continue to increase, desmosomes may rupture, resulting in inflammation and epithelial fracture. Mechanical stretching and deformation forces may cause stromal micro-haemorrhage and inflammation. Although the environment of the skin of the nipple–areolar complex is uniquely conducive to wound healing, it is also uniquely exposed to environmental risks. The two key factors that both prevent and treat nipple pain and inflammation are, first, elimination of conflicting vectors of force during suckling or mechanical milk removal, and second, elimination of overhydration of the epithelium which risks moisture-associated skin damage. There is urgent need for evaluation of evidence-based interventions for the elimination of conflicting intra-oral vectors of force during suckling.
Keywords
Introduction
Despite the known benefits of breastfeeding for both infant and mother, 1 interventions for clinical problems, such as breast inflammation and pain remain a research frontier.2,3 Overuse of pharmaceutical and surgical interventions is an increasingly serious international problem in health care.4,5 Both patients and clinicians typically overestimate the benefits of medical interventions and underestimate potential harms.6 –8 It is not surprising then, given the relative lack of research into clinical breastfeeding support, that overmedicalization and overtreatment is widespread in the care of breastfeeding women and their babies when inflammation, pain, and visible damage of the nipple–areolar complex emerge.9 –16
This is the third of three articles which consider aetiology, classification, and management of benign lactation-related inflammatory conditions of the breast. The first article focuses on breast alveoli, ducts, and stroma to propose a new mechanobiological model, in which excessive intra-luminal pressures trigger inter-lactocyte tight junction disruption and basement membrane rupture, which trigger inflammatory cascades and alveolar apoptosis. 17 The second article builds on this mechanobiological model to re-think classification, prevention, and management of the range of breast inflammations commonly known as engorgement, blocked ducts, phlegmon, subacute mastitis, mastitis, and abscess. 18
This third article addresses the common lactation-related problem of pain of the nipple–areolar complex, including of the nipple stroma (i.e. structural connective tissue of the mammary papilla in which vasculature, ducts, and nerve fibres are embedded). It does not aim to address all nipple–areolar complex pathology that may present during lactation. Clinicians should maintain a high index of suspicion for viral infection (in particular, herpes simplex and also herpes zoster viruses) in breastfeeding women with nipple pain (Box 1).
Viral infection of the nipple–areolar complex in the lactating breast: a rare but important condition.

The evolutionary and complex systems approach to lactation-related breast inflammation detailed in this three-part series forms part of the foundational breastfeeding domain of the programmes known as Neuroprotective Developmental Care (NDC or ‘the Possums programs’). 25 The NDC breastfeeding domain also includes the gestalt biomechanical model of infant suck and its clinical translation into the gestalt method of fit and hold (also referred to as ‘latch and positioning’).9,26,27 NDC has been developed and delivered in Australia since 2011. NDC synthesizes the latest evidence concerning early life care across the interrelated and interacting domains of breastfeeding, cry-fuss problems, infant sleep, and parental mood applying evolutionary and complex systems frames, and translates this synthesis into clinical practice. The breastfeeding domain is foundational, influencing each other domain.13,28 –35
Prevalence of lactation-related nipple pain and damage
Nipple pain is one of the most common reasons for introducing formula or ceasing breastfeeding.36,37 In Li et al.’s 38 study of 1323 mothers in the United States, more than a quarter stopped breastfeeding in the first month postpartum; 29.3% cited pain and 36.8% cited sore, cracked, or bleeding nipples as an important reason.
Nipple pain, with or without visible damage, occurs most often in the first-week post-birth. In 2014, Buck et al. 39 found that 79% of 317 first-time breastfeeding Australian mothers experienced nipple pain by the time they were discharged home after birth of their baby, despite being motivated to breastfeed, well-educated, and in a ‘Baby Friendly’ accredited institution with extensive postnatal support. A 2021 study of 58 Spanish women found that 97% experienced nipple soreness at 48 h postpartum, and a higher pain score was associated with skin-to-skin contact lasting more than two uninterrupted hours in the immediate postpartum. 40 A 2014 Cochrane review concluded that nipple pain reduced to mild levels 7–10 days after birth for a majority of breastfeeding women, regardless of treatment used. 41
Unfortunately, it is not possible to know which women will go on to develop persistent nipple pain and damage. In a 2020 online survey of 1084 women in the United Kingdom who had finished breastfeeding in the past 2 years, 76% reported having experienced latch-related nipple pain at some time. 42
Over half of women with nipple pain develop visible damage or wounds. Visible signs include blisters, bruises, erythema, oedema, cracks or fissures, ulcers, and exudate. These visible signs of damage are associated with increased pain. 43 Using the Numeric Rating Scale of 0–10, women with nipple damage reported a mean score of 6.2 in the first week and 5.8 after that period; women without visible damage reported a mean of 2.7. 44
Even at 8 weeks post-birth in Buck et al.’s 39 study, 20% of 340 respondents reported current nipple pain and 8% current nipple damage; 58% reported experiencing nipple pain at some time post-birth. In 2015, an audit of the Western Australia Breastfeeding Centre found that 36% of 1177 consultations by International Board Certified Lactation Consultants (IBCLCs) were for nipple pain. 45
Large studies suggest that nipple pain occurs more commonly in Australia, the United States, and the United Kingdom than in other parts of the world, such as Brazil, Denmark, South Africa, or Peru, emphasizing the importance of environmental factors.45 –50 To give an example of possible environmental variables, a popularly taught fit and hold strategy (shaping the breast with cross-cradle hold) is associated with a fourfold increase in nipple pain. 51 Method of fit and hold intervention remains an omitted variable bias in most nipple pain studies, typically alluded to without clarification under a statement that the participant received IBCLC support.
Lactation-related nipple pain predisposes to other conditions
Nipple pain is a distressing sensory and emotional experience which interferes with maternal mood, activity, and sleep, whether or not there is visible damage. Not surprisingly, it also predisposes to postnatal depression.43,52,53
Nipple pain is linked with an increased risk of breast inflammation (e.g. engorgement and mastitis). 54 Building on the mechanobiological model of breast inflammation detailed in the first article of this series, 17 this article hypothesizes that the conflicting intra-oral vectors of force which result in nipple pain and inflammation also compress lactiferous ducts, resulting in elevated intra-luminal backpressures and increased risk of breast inflammation. That is, the link between nipple pain and breast inflammation is associative, not causative.
Even without visible trauma, nipple pain is associated with low supply.45,55 Some hypothesize that this is because nipple pain disrupts sensory nerve signals from the nipple to the hypothalamus, impairing oxytocin release, and milk ejection. 56 However, there is no evidence that pain is causally linked to decreased oxytocin levels or less effective and less frequent milk ejections.
Instead, this article hypothesizes that two factors explain the association between low milk production and nipple pain. First, women experiencing pain with breastfeeds are more likely to restrict breastfeeding frequency, which downregulates milk production. Second, the same conflicting intra-oral vectors of force, which result in nipple inflammation and pain also compress lactiferous ducts and impair milk transfer, downregulating milk production.9,17,18,26,27 This is corroborated by the finding that infants whose mothers have nipple pain may transfer less milk (Box 2).57,58
Analysis of ultrasound and vacuum studies corroborates the mechanobiological model of nipple pain in breastfeeding.

IBCLC: International Board Certified Lactation Consultant; NHSPJ: distance from the nipple tip to the junction of the hard and soft palate.
The lactating nipple–areolar complex is characterized by unique protective factors and unique exposure to risks relative to other human skin sites
The following key protective systems interact in the skin of the lactating nipple–areolar complex to maintain health and homeostasis (Appendix 1):
Host immune system.
Skin and milk microbiomes.
Adaptation to repeated mechanical loads (Box 3).
Wound-healing inflammation (Appendix 3).
Skin adapts to protect against mechanical forces.

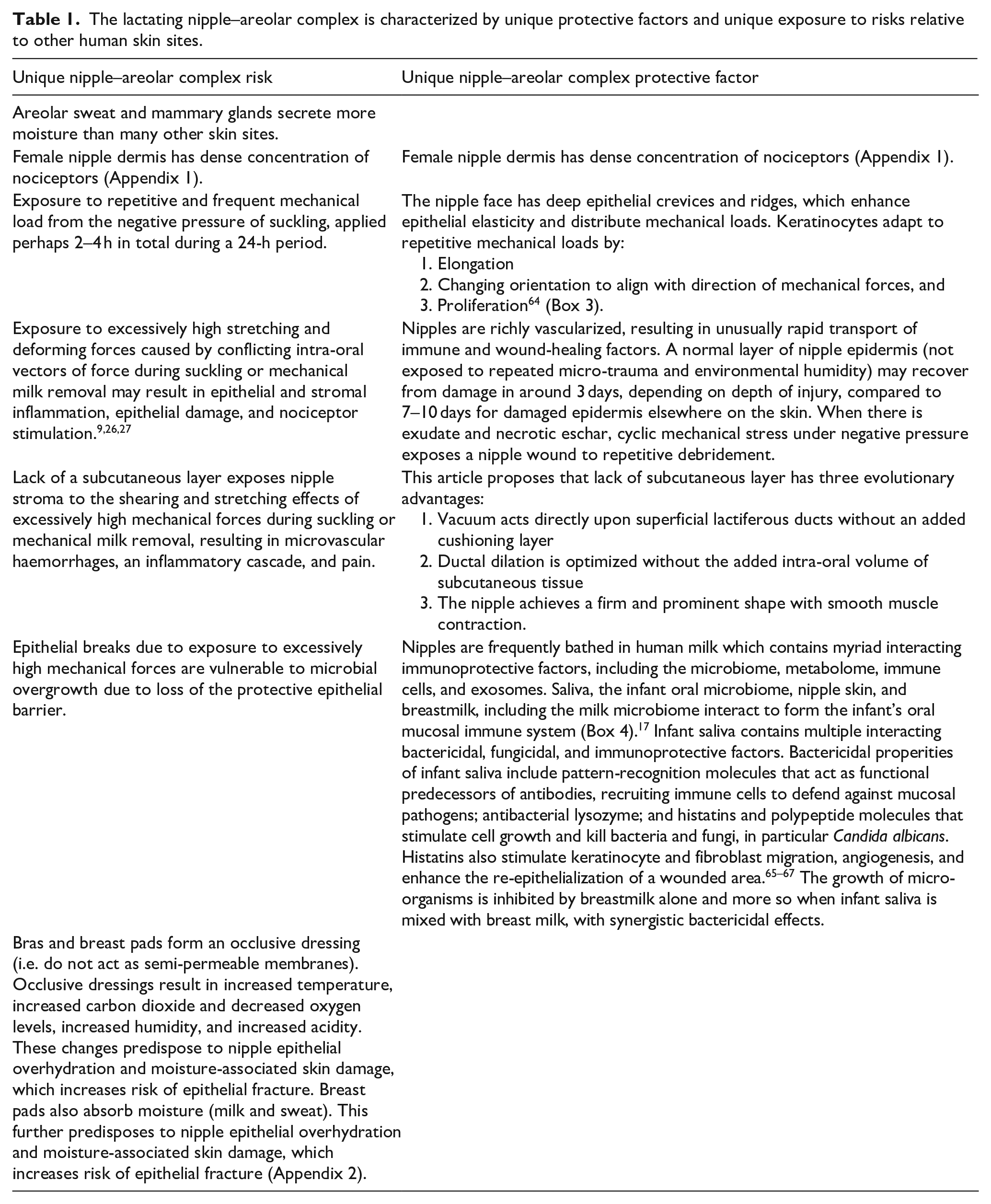
The lactating nipple–areolar complex is characterized by unique protective factors and also exposed to unique risks, relative to other parts of human skin (Table 1). Applying this series’ mechanobiological model, prevention of and intervention for nipple pain and damage demand that innate protective factors are optimized, and risk factors minimized.
The lactating nipple–areolar complex is characterized by unique protective factors and unique exposure to risks relative to other human skin sites.
Aetiology: the mechanobiological model of lactation-related nipple pain and damage
Nipple pain in the absence of visible damage is caused by excessively high intra-oral mechanical loads
This article proposes a new mechanobiological model of lactation-related nipple pain and damage.
During suckling, the nipple epidermis, dermis, stromal core, and other intra-oral breast tissues stretch in response to the mechanical force of vacuum (Box 3). Vacuum is generated as the infant’s mandible drops in the context of the seal against the breast and the seal closing off the nasopharangeal space.9,26,27 Elasticity of breast tissue and nipple–areolar complex skin varies widely between women. But epithelium begins to tighten at high stretch loads, known as the ‘yield point’, as the desmosome locking mechanism is triggered (Figure 1).61,63
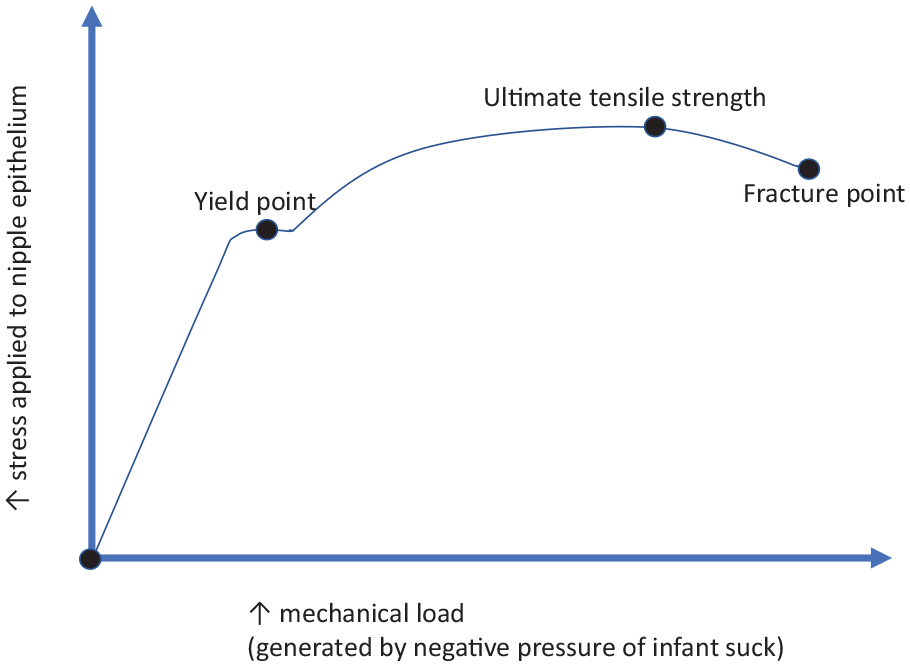
The mechanobiological model of nipple epithelium yield and fracture.
This model proposes two mechanical causes of nipple pain which result from suckling and also from mechanical milk removal. First, nipple pain results when stretching forces are not evenly distributed over a large surface area of nipple, areolar and breast skin, so that desmosomes in the nipple epithelium are subject to repetitive and excessively high mechanical loads (Box 3). This causes the release of cytokines and histamines, triggering inflammatory cascades in the absence of visible tissue damage. If very high stretching or deformational forces are applied, a shearing load may also arise between the epidermis and dermis and the more stable interior collagen structure of the nipple, also causing release of cytokines and histamines and further inflammatory cascades.
Second, stromal micro-haemorrhage results from vascular micro-trauma when the nipple is exposed to repetitive stretching, bending, or deformational forces. Micro-haemorrhages trigger signalling pathways and an inflammatory cascade. Resultant increased stromal tension or swelling further perpetuates cascades of inflammatory responses. The collagen-rich, highly vascular core of the nipple is threaded through with nerve bundles, which may also be vulnerable to the effects of high stretching or deformational mechanical loads and the effects of local inflammation (Appendix 1).
Desmosome strain and inflammation in the nipple skin stimulate dermal nociceptors, triggering maternal nociception and perception of pain. Stromal microvascular haemorrhage and perhaps also neural irritation trigger stromal inflammation, maternal nociception and perception of pain. Persistent nipple pain results from persistent repetitive mechanical micro-trauma in the epithelium, dermis or stroma, which causes persistent inflammation. Inflammatory responses and associated nociceptor stimulation do not cease when an episode of suckling or mechanical milk removal ceases. Before the inflammation has had time to resolve the nipple is again exposed to the mechanical load of milk removal.
Nipple pain with visible damage results when excessively high intra-oral mechanical loads fracture the epithelium
If epithelium can no longer adapt to the mechanical strain of stretching, bending, and shearing forces (Box 3), and desmosomes have locked but the stretching force continues to increase, epithelium ruptures at the ‘fracture point’. 61 In the mechanobiological model of lactation-related nipple pain, the weakest part of the nipple–areolar complex epithelium, or the part placed under the most constant and severe elastic tension in the baby’s mouth, breaks apart (Figure 1). This results in visible trauma, including cracks, grazes, and ulcers, with associated pain and inflammation. Blisters result when horizontal shearing forces cause partial fracture and inflammatory serum collects in a pocket of fluid between layers of skin. Bruising results from vascular damage and haemorrhage.
Cracks are often located at the base of the nipple or in the epithelial crevices on the nipple face. Skin cracks nucleate (i.e. commence) in the stratum corneum along the plane of maximum shear stress, as desmosomes rupture. Fracture of the cells themselves is uncommon. Cracks then propagate along the topographical canyon features of the epithelium. 68
It may be on occasions possible to determine the direction of the intra-oral conflicting force from the location of a crack. For instance, if the crack is at 6 o’clock at the base of the nipple adjacent to the areola, the infant may be suckling from the breast at a height above the natural gravity-induced breast fall, causing the mechanical strain of upwards tension on the intra-oral nipple and breast tissue.9,26,27
The hypothesis that nipple pain and damage is caused by tongue friction or the tongue pinching or compressing the nipple against the palate or upper alveolar ridge is not supported by evidence
The hypothesis that maternal nipple pain and damage results from abnormal tongue movement which pinches or rubs the nipple against the palate or upper alveolar ridge has resulted in widespread overtreatment of breastfeeding infants with frenotomy and bodywork exercises.11,12,14–16,69 This hypothesis is not supported by ultrasound or magnetic resonance imaging of the biomechanics of infant suckling, nor anatomic dissection of the infant floor of mouth fascia.70–72 Studies of breastfeeding women with nipple pain have been interpreted as showing that nipple pain is due to either particular tongue contour and movement attributed to infant oral connective tissue tightness, or innately high vacuum generation.57,59 However, the gestalt biomechanical model, described elsewhere, proposes that these findings are more accurately interpreted as tongue contour changes in response to variable intra-oral breast tissue volumes, aligned with this article’s mechanobiological model (Box 2).9,26,27
Similarly, clinicians and researchers have hypothesized that pacifiers and bottle teats alter neural pathways coordinating tongue movement and sucking patterns, resulting in nipple pain. But this theory is based on misconceptions about the role of tongue in milk transfer. A 2015 systematic review of 14 articles found little evidence of a causal relationship between pacifier and bottle teat use, and nipple confusion.37,58,73
The tongue is a muscular hydrostat, which changes shape and contour without alteration in volume. 74 Applying the gestalt biomechanical model, the infant tongue is a supple adaptive organ, which does not compress the nipple and breast tissue to extract milk or drive milk transfer. Mandibular excursion generates peak intra-oral vacuum, as the anterior and mid-tongue track down en bloc with the mandible. Tongue shape and contour dynamically conform to available intra-oral breast tissue volume. The volume of nipple and breast able to be drawn up into the suckling infant’s mouth decreases in the presence of conflicting intra-oral vectors of force, also known as breast tissue drag.9,26,27
Clinicians and researchers have hypothesized that abnormal infant tongue contour and movement in breastfeeding due to restricted infant oral connective tissues causes a friction burn or graze of the nipple. But a burn or graze caused by friction would be expected to present differently to the cracks and ulcers which characterize lactation-related nipple damage (Box 4). A friction burn or graze is likely to cause a broad area of epithelial damage, on the aspect of the nipple which rests against the dorsum of the tongue during breastfeeding. But nipple cracks and ulcers are commonly located at the base of the nipple and on the nipple face, consistent with epithelial rupture due to tensile mechanical forces. Moreover, if the protective mucosal saliva and mucin layer were to disappear, the hypothesized friction burns would be as likely to occur on the surface of the infant tongue as on the maternal nipple–areolar complex, but maternal nipple damage in breastfeeding does not coincide with infant tongue mucosal damage (Box 4).
Infant saliva protects oral mucosa from friction burn.

MRI: magnetic resonance imaging.
Classification: signs and symptoms of excessively high stretching or deformational mechanical loads during milk removal
Lactation-related nipple pain, persistent nipple pain, and wounds of the nipple
Women describe symptoms of nipple and breast pain and discomfort along a spectrum of intensity with highly variable descriptors, including terms such as cutting, throbbing, pinching, burning, radiating, and stabbing. 43 Erythema and swelling are signs of nipple–areolar complex skin and nipple stromal inflammation. A fine white scale may result from a hyperkeratotic response of the stratum corneum, which occurs in the context of repetitive micro-trauma or moisture-associated skin damage (MSAD) (Appendix 2). Itchiness is hypothesized to result from histamine release, which stimulates nerve cells during the proliferative phase of wound healing (Appendix 3). 74
In a separate review of the research literature, this author has demonstrated that the symptoms of burning, radiating, stabbing, or itching pain which occur between breastfeeds, and which may be associated with signs of a shiny pink nipple and fine white skin flakes, are not indicative of mammary candidiasis. 13 These symptoms and signs are, however, consistent with inflammation, which results from excessively high stretching or deformational mechanical loads applied during suckling or mechanical milk removal. Effects of the inflammatory response continue between feeds.
Lactation-related vasospasm of the nipple
Breastfeeding women may describe shooting, stabbing, radiating, or burning nipple and breast pain at the same time as they notice visible blanching of the nipple face, referred to as vasospasm (Box 5). In 2014, Buck et al. 39 found that almost a quarter of 323 Australian breastfeeding women reported nipple vasospasm in the first 8 weeks after birth. Although these women had higher pain scores overall than women without nipple vasospasm, a majority also reported that their vasospasm was not problematic.
What is vasospasm?

All nipple pain guidelines acknowledge that mechanical breastfeeding trauma is a likely cause of vasospasm.76,77 Paradoxically, painful nipple vasospasm is nevertheless confused with the diagnosis of Raynaud’s syndrome and treated as a primary phenomenon which lacks a known underlying cause, requiring pharmaceutical intervention (Box 5).
In 2004, Anderson et al. studied 12 women who suffered from extremely painful breastfeeding. These women also experienced blanching of the nipple followed by cyanosis and/or erythema, precipitated by cold temperatures. Because 10 of these mothers were evaluated by IBCLCs who reported confidence that breastfeeding technique did not contribute, the authors concluded that poor positioning and poor attachment or latch were not responsible. Half of the women in this small case series were then diagnosed with Raynaud’s disease and prescribed nifedipine. All six reported prompt relief of pain. But this small methodologically weak study lacks a control for the placebo effect, and fit and hold remains an omitted variable bias. 78
The mechanobiological model proposes that nipple vasospasm in breastfeeding women results from repetitive mechanical micro-trauma, which causes inflammation. This inflammation impacts on the autonomic nervous system, destabilizing the homeostatic smooth muscle mechanisms in the walls of the rich vascular bed of the nipple stroma and dermis (Box 5). The subsequent tendency to vasospasm may occur either during breastfeeding or between feeds. That is, the distinction made between nipple vasospasm episodes which occur during or immediately after a feed, and nipple vasospasm episodes which occur between feeds, is not diagnostically helpful or relevant.
A history of autoimmune disease or diagnosis of Raynaud’s syndrome prior to lactation increases the likelihood of a vasospasm response to the inflammation of nipple dermis or stroma which results from excessive mechanical loads during breastfeeding or mechanical milk removal. Similarly, environmental factors, such as cold or touch are more likely to trigger a vasospasm response in nipple dermis or stroma which is inflamed due to intermittent experience of excessive mechanical loads during breastfeeding or pumping. Lactation-related nipple vasospasm is more accurately conceptualized as a secondary Raynaud’s syndrome, which occurs in response to inflammation from repetitive exposure to excessively high mechanical loads.
Lactation-related white spots
From the perspective of this article’s mechanobiological model of nipple pain and damage, there are three kinds of white spots. The first two are conceptualized as signs of localized epithelial inflammation.
Mitchell et al. hypothesize that white spots result from subacute mastitis and mammary dysbiosis, in which ductal biofilm formation extends to the nipple epithelium (Box 6).79,80 Their hypothesis builds on the 2017 Rodriguez and Fernandez hypothesis that breast inflammation results from biofilm blockages within lactiferous ducts. 81
The hypothesis that white spots are caused by mammary dysbiosis is not supported by evidence.
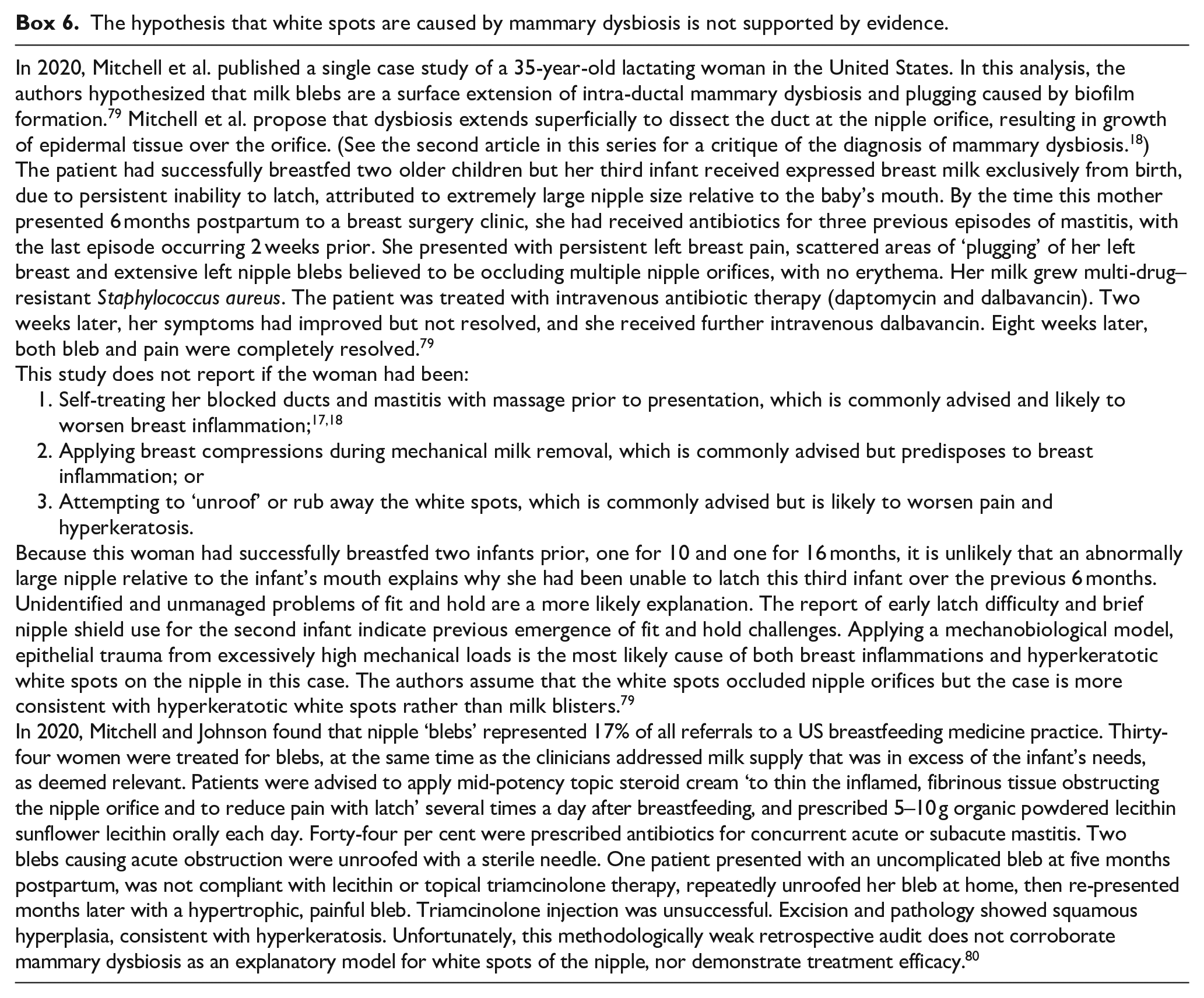
The first two articles of this series on lactation-related breast inflammation argue that diagnoses of mammary dysbiosis and subacute or subclinical mastitis are not supported by the evidence, and that the hypothesis that breast inflammation is caused by intra-ductal biofilm is unconvincing. Pathogenic biofilm formation may be an occasional late stage development in a cascade of severe breast inflammation, not causative. Similarly, there is no convincing evidence-based rationale to suggest that white spots are an extension of intra-ductal biofilm to the face of the nipple (Box 6). These pathogenic bacterial models result in widespread prescription of short or prolonged courses of antibiotics for lactating women, with little evidence of benefit relative to the passage of time, and contribute to the global problem of antimicrobial resistance.17,18
Milk blister
A milk blister is an exquisitely painful white spot or lesion on the nipple face, usually with a clearly demarcated border. It is sometimes associated with a lump or cord-like area extending from the nipple blister into the breast.
This article proposes that microscopic epithelial inflammation in the region of a duct orifice, most likely due to mechanical trauma, may heal so that the stratified squamous epithelium which extends 2 mm inside the orifice fuses during the inflammatory process of wound healing (Appendix 1). There may be a build-up of milk in the main duct behind the resultant milk blister, resulting in elevated intra-luminal pressure in the glandular tissue drained by branches of that duct. The latter triggers inflammation and high white cell counts, 82 explaining the inspissated milk that is sometimes released or expressed when a milk blister is released.
Hyperkeratosis
This article hypothesizes that a hyperkeratotic spot of the nipple is an area of stratum corneum which has thickened in response to a focus of repetitive and excessively high mechanical trauma during breastfeeding or mechanical milk removal. A hyperkeratotic spot is often exquisitely painful in response to even mild pressure, perhaps because the thickened plaque of stratum corneum places pressure on the dermis, which is highly vascular and dense with sensory nerve endings.
A hyperkeratotic spot may appear pale white, cream, or yellowish, though colour alters during milk removal due to the effects of moisture and epithelial hydration. A hyperkeratotic spot may be larger with more diffuse borders than a milk blister. Multiple, irregular sized hyperkeratotic spots may form on the face of a nipple which is subject to repetitive micro-trauma. Attempts to unroof a hyperkeratotic spot, mistaking it for a milk blister, will worsen hyperkeratosis.
In 2012, a US medical practitioner Dr O’Hara published an abstract (only), which reported histological analysis of punch biopsies of painful white spots from five breastfeeding women. The tissue was characterized as rubbery and scar-like. Analysis found no bacteria or fungi, but leukocytes and fibrin were identified, signalling inflammation. The women reported that their symptoms resolved shortly after biopsy removal. These histological analyses are consistent with the diagnosis of hyperkeratosis. 83
O’Hara reported that patients with white spots who subsequently presented to that clinic (number not stated) were effectively treated with a short daily course of mid-potency steroid under occlusion. A moist wound dressing (plastic wrap) was applied to enhance penetration of steroid into inflamed and fibrotic tissue. The author concluded that ‘nipple blebs are an inflammatory response to nipple trauma. . . . Clinicians should check for and treat any underlying causes of the recurrent trauma’. 83
Milium
A milium is a painless, small white dermal cyst of keratin, lined by a layer of stratified squamous epithelium, which may appear in the crevices of the nipple face. A milium cyst may appear prominent and very white after a breastfeed or mechanical milk removal. It usually disappears in time, and no treatment is required.
The hypothesis that persistent nipple pain during lactation is nociplastic (due to central sensitization) conflicts with international criteria for nociplastic pain
Persistent nipple pain has been defined in the 2016 Academy of Breastfeeding Medicine Clinical Protocol #26: Persistent Pain with Breastfeeding as pain that persists for more than 2 weeks in a breastfeeding woman, and which has not responded to (undefined) interventions by IBCLCs. Clinical protocols for persistent lactation-related nipple pain list allodynia and hyperalgesia as differential diagnoses, requiring referral for psychological or pain clinic support, or medications, such as propranolol or selective serotonin reuptake inhibitors.76,84,85
The International Association for the Study of Pain defines nociplastic pain
The biomedical model conceptualizes pain as a direct consequence of tissue damage: the more severe an injury, with its associated inflammation, the more severe the pain. As tissue damage resolves, pain resolves. But this reductionist conception of pain is outdated.
An individual’s perception of pain emerges out of interactions between multiple factors. 86 During acute tissue damage, pain perception is predominantly affected by the extent and nature of the injury. Relatively unspecialized nerve cell endings known as nociceptors send a threat signal to the brain. The brain evaluates the extent of threat by drawing on information from current and past experiences, and this perception is moderated by the psychological state of the brain. Even in the case of acute injury, psychosocial and genetic factors, psychological state, and past experiences of pain interact to modulate pain perception. The International Association for the Study of Pain (IASP) states that pain is an experience of sensations and emotions and is always subjective. No pain, even acute pain in response to obvious tissue trauma, can be conceptualized as purely nociceptive.
The IASP defines chronic pain as pain which is present for at least 3 months and/or beyond normal healing time. 87 The experience of chronic pain emerges from:
Nociceptive stimulation (inflammation and tissue damage which stimulate nociceptors and initiate perception of pain),
Neuropathic stimulation (damage to peripheral nerves which initiates perception of pain), and
Nociplastic influences (central nervous system processing alteration or dysfunction, resulting in central sensitization or disruption of perception of pain signals). 88
The IASP defines nociplastic pain as ‘pain that arises from altered nociception despite no clear evidence of actual or threatened tissue damage causing the activation of peripheral nociceptors or evidence for disease or lesion of the somatosensory system causing the pain’. 89 When pain is chronic, it no longer reflects the state of the tissues since most injuries heal within a few months. Central sensitization or nociplastic pain has been studied with cancer pain, rheumatoid arthritis, fibromyalgia, low back, and musculoskeletal pain, and increasingly with long COVID. Multifaceted care is required because social, psychological, and physical domains interact in pain perception. Pharmaceutical and non-pharmacological techniques including psychological support are required.88,90
Lactation-related nipple pain is acute even when persistent
This article argues that it is inappropriate to extrapolate management of functional chronic pain syndromes to the care of breastfeeding women with persistent nipple pain. Instead, this article proposes that the perception of nipple pain is triggered by acute tissue damage and inflammation, even when modulated by genetically moderated pain sensitivity, psychological state, and the impact of psychosocial factors. 91 It is important to note that although anxiety and depression modulate pain thresholds, anxiety and depression also result from the experience of pain with breastfeeding. 53
The nipple dermis is dense with nociceptors; nipple stroma is richly vascularized and threaded with nerve fibres (Appendix 1); both are vulnerable to inflammation caused by mechanical stretching and deformational forces. Inflammation caused by repetitive application of excessively high mechanical loads on the nipple skin or by stromal micro-haemorrhages, and perhaps also the effects of stretching deformational mechanical loads on stromal nerve fibres, send powerful nociceptive signals to the brain and should not be mistaken for nociplastic pain. Lactation-related nipple pain remains an acute pain according to the IASP definitions, even when nipple pain is persistent. The physical and psychological stress of breastfeeding in the presence of pain may exert effect by causing unconscious muscle tension, which results in elevation of shoulders and arms or difficulty making adjustments to fit and hold (micro-movements), worsening conflicting intra-oral vectors of force.9,26,27
In 2012, McClellan et al. noted that ‘lack of research describing the pain severity and characteristics for breastfeeding women may lead some clinicians to question the pain threshold of women experiencing persistent pain’, but suggested that the effects of excessively high intra-oral vacuums measured in women with nipple pain may be the predominant reason for ongoing pain perception, rather than central sensitization. 43 But ultrasound and vacuum studies of women experiencing nipple pain corroborate the mechanobiological model of lactation-related nipple pain (Box 2).
When application of mechanical forces cease altogether, in the absence of ongoing sucking or mechanical milk removal, inflammation of the nipple skin and stroma rapidly resolves and the experience of pain ceases. This explains why women with persistent nipple pain are more likely to prematurely cease lactation. 36
In a 2018 US case series of three lactating women with nipple and/or breast pain, Mudunna et al. assessed pain using a cotton-bud and pin-prick touch, which the authors proposed were non-painful stimuli, moving from the lateral edge of each breast quadrant in towards the nipple. The women demonstrated heightened breast skin sensitivity to the stimuli, and the authors stated that their pain resolved with oral antihistamines and beta-blockers. Mudunna et al. wrote: Allodynia is perceiving a non-painful stimulus as painful. Other [breastfeeding] individuals experience increased pain from a normally painful stimulus (hyperalgesia). For a lactating woman with allodynia, an anatomically normal latch may be perceived as painful. Similarly, a woman with hyperalgesia may experience slight nipple compression during let down as excruciating.
85
But Mudunna et al. also hypothesize that persistent local inflammation due to repetitive exposure to micro-trauma is likely to sensitize the nociceptors and mechanoreceptors of nipple skin due to release of histamines and cytokines. Similarly, increased interstitial tension associated with the vasodilation and hypervascularity of breast inflammation triggers release of histamines and cytokines, sensitizing surrounding tissues. Mechanical pressure by a cotton bud or pin prick in the context of acute nipple or breast inflammation is likely to trigger nociceptive pain perception. This article argues that the local sensitivity effects of nipple and breast inflammation should not be confused with central sensitization.
Diagnoses of nociplastic pain, central sensitization, allodynia, and hyperalgesia may harm a lactating woman with nipple pain and damage. This is because these diagnoses may:
Invalidate her lived experience, which is that suckling or mechanical milk removal causes her pain and that if she were to cease this altogether, her pain would rapidly resolve;
Disempower her, since she is not helped to resolve the pain herself (as is the case, for example, with the gestalt method of fit and hold) but is advised that she requires pharmaceutical intervention and multi-disciplinary teams;
Re-traumatize her if she is a sexual abuse survivor by taking a sexual trauma history in a breastfeeding consultation, then proposing that persistent nipple pain is linked to sexual trauma and associated nociplastic effects;
Invite her to shift attention away from her experience of nipple pain. She may also feel pressured to divert her attention away from her nipple pain, so that she is not perceived as ‘exaggerating’ the pain in her brain. Not paying attention to nipple sensations and pain typically worsens conflicting intra-oral vectors of force during milk removal. From the perspective of the gestalt method, increased attention to nipple and breast sensation is required, drawing on psychological strategies which support contact with the present moment, as she applies micro-movements to eliminate breast tissue drag and resolve tissue damage and inflammation; 9,26,27
Place her at risk of side-effects of pharmaceutical interventions without evidence of benefit; and
Result in financial burden of treatments without evidence of benefit.
Prevention and management of lactation-related nipple pain
Evidence-based prevention and management of lactation-related nipple pain and persistent pain is detailed in Table 2. The mechanobiological approach to nipple pain translates into two key preventive or treatment strategies:
Elimination of repetitive mechanical micro-trauma due to excessively high stretching or bending mechanical loads during milk removal and
Avoidance of epithelial overhydration and MASD.
Evidence-based management of lactation-related nipple pain and wounds.

Does photobiomodulation therapy help resolve breastfeeding-related nipple pain and damage?

RCT: randomized controlled trial.
Key strategy 1: eliminate repetitive mechanical micro-trauma
A. Optimize fit and hold to eliminate conflicting intra-oral vectors of force during breastfeeding
Studies examining the causes of lactation-related nipple pain and clinical management and clinical protocols universally agree that poor infant positioning or latch is the most common cause of nipple pain. Guidelines advise that suboptimal fit and hold should be addressed before any other treatment is instituted.37,41,45,48,76,77
Yet the way an infant fits into the maternal breast and body, which has direct impact upon the biomechanics of suckling, remains an omitted variable bias in almost all nipple pain research. Commonly taught approaches to fit and hold when problems emerge rely upon outdated biomechanical models of infant suck (Box 8). 107 Much of what is offered women with breastfeeding difficulty, including interventions for fit and hold, is based upon experience or opinion (Box 8).2,108 –111 In 2016, Thompson et al. demonstrated in a retrospective analysis of the medical records of 635 mother–baby pairs that symmetrical apposition of the infant’s chin, cheeks and nose against the breast decreased nipple pain fourfold, compared with cross-cradle hold in which the mother used one hand to shape her breast as she brought the baby on. Although this study elucidated one aspect of fit and hold required to optimize intra-oral breast tissue volume, it does not offer explanatory biomechanical models or develop an evidence-base for a fit and hold intervention. 51
Commonly applied fit and hold strategies lack an evidence base.

UNICEF: United Nations Children’s Fund.
The failure of current approaches to fit and hold to effectively resolve repetitive biomechanical micro-trauma during breastfeeding leads to widespread overmedicalization and overtreatment of both breastfeeding women and their babies, risking unintended outcomes. Examples include inappropriate diagnosis of mammary candidiasis resulting in unnecessary treatment with anti-fungals; overtreatment with infant frenotomy for inappropriate diagnoses of oral connective tissue restrictions; inappropriate diagnoses of cranial nerve dysfunctions and pathologizing of palate shape, tongue length, and shape of mandible resulting in unnecessary treatment with bodywork exercises;69,97,98 diagnoses of idiopathic vasospasm or Raynaud’s syndrome resulting in overtreatment with calcium channel blockers; inappropriate diagnoses of nipple white spots as subacute mastitis or mammary candidiasis resulting in unnecessary treatment with antibiotics and anti-fungals; and inappropriate diagnoses of functional pain or central sensitization, resulting in use of medications without evidence of efficacy.11–13,14,16
In 2015, Kent et al. reported that 42% of cases presenting to the Breastfeeding Centre of Western Australia showed lack of improvement with fit and hold and other interventions offered by IBCLCs, noting that though some studies claim to show that certain fit and hold interventions improved nipple pain outcomes,114,116,117 other studies could not replicate these findings.118 –120 They observed: ‘Nipple pain is often attributed to suboptimal positioning and attachment of the infant although conclusive evidence is yet to be provided regarding which aspect(s) of positioning may be most important’. The IBCLCs went on to diagnose ankyloglossia and palatal anomaly in 36% of the infants of women presenting with nipple pain. 45
Given the international evidence demonstrating overdiagnosis of ankyloglossia, and the normality of a wide variety of palatal contours, this article proposes another explanation: that scientific investigation of the elements of fit and hold which impact on maternal pain remains a research frontier.
The foundational importance of laid-back or baby-led breastfeeding
The physiologic or mammalian approach to breastfeeding initiation, including skin-to-skin contact postpartum, has been a major advance in the field of clinical breastfeeding support over the past two decades, with positive impacts on breastfeeding outcomes.121 –124
A 2020 systematic review of 11 Chinese randomized controlled trials (RCTs) and one Italian RCT investigating ‘biological nurturing’ or ‘laid-back breastfeeding’ approaches found that when women are taught baby-led or laid-back breastfeeding in hospital immediately after the birth, the incidence of nipple pain and damage decreases for up to 8 weeks. 125 The Italian RCT randomized 180 women to either biological nurturing at birth or a control group, and showed decreased nipple pain and damage, engorgement, and mastitis during the hospital stay, and 58% decrease in cracked nipples at discharge in the intervention group. But biological nurturing made no difference to the rates of nipple shield use, breast problems at 30 days post-birth, or to rates of exclusive breastfeeding at 4 months. 126
A 2021 Chinese RCT of 504 pairs demonstrated that implementing baby-led self-attachment from birth results in a 12% increase in exclusive breastfeeding at day 3, and an 8% and 5% decrease in the number who reported nipple pain at 3 days and 3 months postpartum, respectively. 127
While biological nurturing or baby-led approaches are demonstrated in these studies to be foundationally important for prevention of breastfeeding difficulties from birth, baby-led approaches have not been demonstrated to be effective therapeutic interventions for emergent breastfeeding problems. A 2013 Swedish RCT of 103 mothers with infants up to 16 weeks of age with severe latch-on difficulties found that a baby-led or skin-to-skin intervention did not increase the likelihood that the infant would latch on. 128
Applying the mechanobiological model, this article proposes that although laid-back or baby-led breastfeeding methods are essential from birth, they do not integrate new knowledge about the biomechanics of infant suck to address the mechanical forces that cause nipple pain and damage. That is, the biological nurturing approaches are not enough to prevent breastfeeding problems including nipple pain and damage for many women.
The gestalt method is the only available clinical approach to fit and hold which integrates the principles of laid-back or baby-led breastfeeding with an evidence-based model of the biomechanics of infant suckling, translated into a reproducible, flexibly applied clinical intervention.9,26,27
Normal maternal and infant anatomies are highly variable
Human anatomy, including infant tongue length, mandibular shape, and palate contour and height, and maternal breast, nipple, areola, upper and forearm length, and abdominal contour are highly variable. Labelling, that is, medicalizing or pathologizing, the wide range of normal maternal and infant anatomy disempowers and discourages breastfeeding women, and unnecessarily exacerbates parental anxiety. In the gestalt model, it is understood that certain normal anatomic variations may increase vulnerability to the emergence of problems in the complex adaptive system of the breastfeeding mother–baby pair. This emphasizes the importance of preventive and management approaches to fit and hold which optimize intra-oral breast tissue volume and eliminate breast tissue drag.9,26,27
Infant oral connective tissues, including the lingual and labial frenula, also display wide anatomic variability which are currently pathologized and inappropriately treated with either surgery or courses of bodywork therapy. The normal spectrum of labial frenula anatomy is not linked with breastfeeding problems, and should not be pathologized as restricted or ‘tied’.129–131 There is no anatomic or functional basis for the diagnosis of posterior tongue-tie.72,94,95,132 The latter two diagnoses are examples of overmedicalization of breastfeeding problems, resulting in exponential increase in unnecessary infant oral surgery and bodywork exercises.11,12,14–16,97,98,133 Studies that claim to show benefits of frenotomy for diagnoses of posterior or upper lip-ties are methodologically flawed, demonstrating bias.134,135 Unintended consequences of frenotomy include infant pain, haemorrhage, worsened feeding, oral aversion, damage to lingual nerve branches altering tongue sensation, sublingual mucocele, and weight loss.72,136 –139 The gestalt model proposes that behaviours during breastfeeding of fussing, back-arching, pulling off the breast, and ‘shallow latch’ are all signs of suboptimal fit and hold and are not attributable to infant oral connective tissue restrictions, neurological weakness or motor dyscoordination.9,25 –27
Certain poorly defined anatomic variations have been shown in preliminary studies to have links with breastfeeding problems, including nipple pain. A 2009 Iranian study showed that 50 newborns of mothers with flat nipple, inverted nipple, large breasts and/or large nipples had a mean decrease in weight by day 7 compared to 50 newborns whose mothers did not have these breast variations. 140 A 2013 Thai study of 449 women showed that nipple lengths of less than 7 mm were associated with less success in bringing baby to the breast and initiating breastfeeding in the first 24 h, but no conclusions about breastfeeding success or capacity to latch after the first day could be drawn. 46 In 2020, Ventura et al. 141 studied 119 women in a US breastfeeding centre, showing that various combinations of wider, longer nipples and denser areolas were associated with difficulty latching, sore nipples, low milk supply, and slow infant weight gain. But there is no reliably established link between nipple shape and breastfeeding failure.
This article proposes that multiple morphological factors interact with multiple modifiable biomechanical factors to determine an infant’s capacity to transfer milk efficiently from his or her mother’s breast, without causing her pain. The gestalt model applies a complexity science perspective to clinical breastfeeding support, which aims to optimize intra-oral breast tissue volume across the wide diversity of maternal and infant anatomies. In this way, anatomic and other vulnerabilities within the complex adaptive system of the mother–baby pair are compensated for, because the protective effect of multiple other factors is optimized.9,25–27
Impact of anatomic abnormality
Ankyloglossia is a congenital abnormality of the lingual frenulum, which significantly restricts movement of the infant’s tongue and has been linked with maternal nipple pain. Prevalence estimates vary between 3% and 10%, in the absence of agreed definitions and demonstrated overdiagnosis. 96 Although many infants have a prominent and membranous frenulum, which may attach anywhere along the ventral surface of the tongue, a tongue-tie is a variation of frenulum which may attach close to the tip of tongue, often to the alveolar ridge instead of the floor of the mouth, and is assessed clinically as impacting on the infant’s capacity to suckle without causing maternal nipple pain. Lack of consensus definition of ankyloglossia is a methodological flaw in all investigations into this condition, and there are no studies comparing the effects of optimal fit and hold intervention with frenotomy. A small case series of breastfeeding pairs showed that the effects of a brief gestalt intervention on tongue contour, measured by ultrasound imaging, was the same as had been measured elsewhere post-frenotomy. 27 A classic tongue-tie typically requires a simple scissors frenotomy.94,142
B. Eliminate conflicting vectors of force during mechanical milk removal
Conflicting vectors of force (breast tissue drag) applied to the nipple during pumping may cause persistent nipple pain and damage. Hands-free mechanical milk removal, with pump flanges supported in an elastic band, may increase the risk of breast tissue drag and epithelial damage. Mechanical milk removal may also result in an erythematous, slightly swollen ring rash on the areola, a sign that the areola is repetitively drawn into the flange and exposed to friction. Pain-free, thickened discoloration, and hyperkeratosis of the nipple face, caused by repetitive ischaemia, may result from exclusive pumping.
The following strategies aim to minimize damage to nipple–areolar complex skin and nipple stroma during mechanical milk removal.
Ensure nipple moves freely without rubbing on inside of the flange tunnel, and that minimal areola is drawn up into the tunnel;
Invite a woman to experiment between different sized flanges;
Invite her to experiment with different flange options, for example, Pumpin’ Pals or Milkdrop cushions;
Hand expression of one breast while pumping the other, then swap the next time;
Pump on lowest effective vacuum setting and for short periods of time, for example, 10 min, because frequent short pumping is more effective in milk removal and milk generation than less often, longer periods; 18
Do not use hands-free pumping (because hands-free pumping, curtails a woman’s capacity to eliminate breast tissue drag which conflicts with the direction of the vacuum;
Consider applying olive oil as lubricant.
Key strategy 2: avoid epithelial overhydration and moisture associated skin damage
Topical applications to nipples during lactation, including anti-fungal treatments, mupirocin antibiotic cream, hydrogel discs, lanolin, vitamins A and E, Vaseline, sundry emollients, and ‘All Purpose Nipple Ointment’ have been shown to be ineffective for nipple pain and damage, and risk epithelial overhydration and MASD (Table 3; Appendix 2). MASD results in an erythematous rash with clearly defined edges visible on the areola, corresponding with topical application. Overhydration and MASD may be confused with an irritant contact dermatitis or an allergic contact dermatitis. 22 Overhydration and MASD place the nipple–areolar complex at risk of damage or delayed healing (Appendix 2).
Interventions which

RCT: randomized controlled trial; APNO: all-purpose nipple ointment; IBCLC: International Board Certified Lactation Consultants.
Environmental humidity from occlusion, including from a bra and breastpad, alters skin pH and microbiome, and hydrates the epithelium. This interferes with the cohesive strength of the desmosomes, resulting in worsened epithelial deformation in response to mechanical load, increased length of crack propagation pathways, secondary crack formation, and oblique crack interfaces in the stratum corneum (Appendix 2). A study of skin (from a woman’s breast but not during lactation) found that at 7% relative humidity, the sheer crack plane was aligned with the direction of the stress, but with 100% relative humidity, the cracks were longer, with increased area of crack interface, and an increased energy cost of tissue rupture. 68
Prevention and management of lactation-related nipple–areolar complex wounds
The two key strategies of (1) elimination of repetitive mechanical micro-trauma and (2) avoidance of epithelial overhydration and MASD, above, are fundamental to both the prevention and management of nipple–areolar complex wounds.
There is currently no international consensus on optimal skin wound care even after common skin procedures and excision, with patients receiving a wide variety of recommendations. 149 It is not surprising, then, given the frontier status of clinical breastfeeding support, that there is little research elucidating breastfeeding-related nipple wound healing.
The NDC evolutionary and complex systems approach to prevention and management of inflammatory nipple pain and damage in breastfeeding mirrors a paradigm shift occurring in the treatment of skin wounds. In wound care, the pathogenic micro-organism model which results in antibiotic treatment is increasingly replaced by multi-lateral interventions which aim to optimize the healthy function of the interacting biological systems of host immunity, including the skin microbiome.
Current clinical protocols for the management of breastfeeding-related nipple damage confuse the pathophysiology of acute wounds with that of chronic wounds. A chronic wound regardless of initial insult fails to heal due to endogenous dysregulation of the immune response. 144 A chronic wound is characterized by excessive levels of pro-inflammatory macrophages and an overabundance of inflammatory mediators, as the inflammatory phase of wound healing fails to resolve. This becomes difficult to control clinically due to formation of pathogenic bacterial biofilms, perpetuated by a dysregulated immune environment. The chronic wounds of diabetic foot ulcers, vascular ulcers, and pressure ulcers feature pathogenic biofilm formation, chronic exudation, tissue necrosis, defective re-epithelization, and decreased angiogenesis. 150 In contrast, acute wounds occur in response to external insult and undergo a series of molecular events which result in restoration of structural integrity (Appendix 3). This article argues that although lactation-related nipple pain and damage may be persistent, the injury remains acute. Once the source of repeated mechanical insult ceases, damaged epithelium heals rapidly due to the unique features of the nipple–areolar complex (Table 1).
Table 2 details evidence-based management of lactation-related nipple pain and nipple–areolar complex wounds. Table 3 lists commonly applied strategies which are not effective.
The role of antibiotics
The pathogenic model of wound management assumes that a reduction in microbial load reduces wound infection, and that more or longer antibiotic or anti-fungal treatment is necessary if a wound does not heal. But the pathogenic microbiota paradigm of skin wounds is vigorously contested, including by this article, in the context of the global crisis of antimicrobial resistance and the urgent need for responsible antimicrobial use.151 –154 As the Director General of the World Health Organization stated in 2020: ‘Antimicrobial resistance is a slow tsunami that threatens to undo a century of medical progress’. 151
Research elucidating biofilm development in chronic wounds (such as burns, diabetic, or vascular ulcers) has been erroneously extrapolated to inform clinical protocols for management of nipple skin showing signs of lactation-related inflammation and damage.144,150 Clinical protocols advise that when a purulent exudate is visible on an area of nipple damage, bacterial infection is likely and topical mupirocin or oral antibiotics should be prescribed, citing research which shows that Staphylococcus aureus has been isolated from the nipple of about one-third of women with persistent nipple pain.41,115
But skin microbiomes commonly include S. aureus in the absence of pain or damage. Healthy skin biofilms are strong and dynamic ecological structures created by dense network associations of bacteria and fungi, and integral to the host’s immune defence (Appendix 1). 13 Antibiotics have been shown to destabilize the skin microbiome without altering the diversity or relative abundance of specific targeted species. This may explain why antimicrobial approaches which have proven so effective for internal infections have minimal efficacy against skin wound infections. Several topical formulations of antibiotics have been shown to be ineffective in chronic skin wounds, yet risk bacterial resistance, contact dermatitis, and MASD. 144 A number of studies conclude that most existing approaches to skin wound care are ineffective, and some interfere with healing. 155
Lactation-related nipple damage only rarely requires topical or oral antibiotic application. Wound exudate is mostly protective. A severely purulent exudate which is thick, grey green or yellow, and has a strongly unpleasant odour may warrant topical antibiotic treatment. Oral antibiotics may be required if cellulitis develops beyond the wound border, presenting as erythematous, spreading peri-wound inflammation and swelling, or for impetiginous changes of the nipple–areolar complex with weeping, yellow crusting blisters that do not respond to topical antibiotics.
Conclusion
Nipple pain and damage is common in breastfeeding women. It is associated with low supply and mood disruption and substantially increases the risk of premature cessation of breastfeeding. Nipple pain and damage is a common reason for women to engage in mechanical milk removal rather than direct breastfeeding. However, mechanical milk removal to predominantly feed an infant with expressed breast milk is a work-intensive practice that increases occupational fatigue.
All current clinical protocols for lactation-related nipple pain and damage emphasize the importance of fit and hold (‘latch and positioning’) problems as the primary cause of nipple pain and damage. But clinical breastfeeding support remains a research frontier; commonly applied fit and hold interventions for nipple pain and damage are experience-based only. Fit and hold continues to be an omitted variable bias in clinical breastfeeding research. Given this context and the worldwide trend to overdiagnosis and overtreatment, it is not surprising that management of lactation-related nipple pain and damage is overmedicalized. A wide range of diagnoses and interventions are applied which have been demonstrated to be ineffective, lack an evidence base, and place mothers and babies at risk of unintended outcomes.
This article builds on two previous articles concerning lactation-related breast inflammation, to propose a mechanobiological model of lactation-related nipple pain and wounds. New research concerning skin responses to mechanical stress and the impacts of MASD is translated into clinical approaches. Interventions which avoid inappropriate medicalization but address the underlying mechanical causes of nipple pain and damage in breastfeeding are explicated. These strategies have been delivered over the past decade in clinical contexts in Australia, as part of the foundational breastfeeding domain of NDC (or ‘the Possums programs’).
Evaluation of the clinical implications of the mechanobiological model of lactation-related nipple pain and damage is urgently required, if breastfeeding rates are to increase.
Footnotes
Appendix 1
Appendix 2
Appendix 3
Author contribution(s)
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author is Medical Director of Possums & Co. www.possumsonline.com, a charity which educates health professionals in Neuroprotective Developmental Care (NDC or ‘the Possums programs’), including in the gestalt approach to clinical breastfeeding support. Possums & Co. offers many free resources but also sells access to the Milk & Moon programmes ![]() which provide parents with breastfeeding information and peer support, and to education resources for providers at ndceducationhub.com. The charity invests all revenue raised back into education and research which supports the well-being of mothers and babies.
which provide parents with breastfeeding information and peer support, and to education resources for providers at ndceducationhub.com. The charity invests all revenue raised back into education and research which supports the well-being of mothers and babies.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The charity Possums & Co. funded the open-access publication fee.
Ethical approval
No ethics approval was required for this paper.