
Abstract
Cancer survivors are at increased risk of chronic disease and diminished quality of life. The presence of overweight and obesity can exacerbate these health risks. Fortunately, even small weight losses have been found to produce clinically meaningful health outcomes. However, effective obesity treatment is difficult to access, and recently, efforts have been made to disseminate interventions using eHealth or distantly delivered technology. This review aims to focus on the efficacy and limitations of these technologies for female cancer survivors. Suggestions are also provided to encourage further meaningful work in this area.
Introduction
According to the American Cancer Society, there are over 8,000,000 female cancer survivors in the United States. 1 According to the National Cancer Institute, a person is considered a survivor from the time of diagnosis until the end of her life. A large proportion of these women are overweight or obese. 2 Overweight and obesity have been related to an increased risk of cancer recurrence and decreased survival.3–4 In addition, compared with individuals without a history of cancer, cancer survivors have an increased risk for future cancer, 5 diabetes mellitus type II and cardiovascular disease6–7 and may experience poorer health-related quality of life.8–9
Weight loss has been associated with a better health-related quality of life and overall well-being and a decreased risk of cardiovascular disease, type II diabetes and mortality in cancer survivors.10–11 Weight loss as little as 5%–10% of body weight has been shown to result in clinically relevant health benefits.12–13 In light of this evidence, the American Cancer Society 14 and the Institute of Medicine have advocated for research to address obesity in cancer survivors. 15 In fact, a few, small randomized behavioral weight loss trials among breast cancer survivors have demonstrated at least a 5% weight loss at 6 months 16 with some larger trials showing 3.6% and 4.7% weight loss at 18–24 months.17–18 Therefore, it is clear that clinically relevant weight loss is possible for these women.
The gold standard method for effective weight loss involves behavioral treatment, including a diet and exercise component, with in-person counseling. 19 An obstacle to in-person weight loss counseling is the inconvenience of having to travel to distant locations for treatment. From a health care service delivery perspective, there are many barriers inherent to the delivery of these intensive interventions in the context of clinical care. 20 For patients, the time and resources required to travel and attend such programs are often significant. 21 This is particularly true for cancer survivors who may need to travel significant distances to get to a medical center just to receive their cancer care. Programs that are delivered distantly may offer a distinct advantage in this regard. In particular, interventions utilizing telephone counseling or other technological approaches (such as eHealth or mHealth modalities, for example, text messages, e-mail and other Internet interfaces) may offer the repeated contacts necessary to promote both initiation and maintenance of behavior change in a diverse and growing cancer survivor population.22–23 While barriers still exist to the health care system, such as staff time and the continual need to update technology, electronic and/or mobile health platforms can still hold immense promise to deliver behavioral interventions that are embedded into individuals’ daily routines, that are highly personalized to individuals’ behaviors and health conditions and have the potential to reach diverse populations.
Weight loss interventions that produce weight reduction of clinically relevant magnitude are only recently being developed for dissemination to cancer survivors. The goal of this review was to gain more insight into the current state of these distantly delivered interventions, specifically for female cancer survivors. Specifically, the objectives are to (1) understand current levels of efficacy, (2) evaluate current limitations and (3) provide suggestions for future work in this area to move the field forward.
Literature available
For the purposes of this review, distantly delivered technology included the use of telephone sessions for counseling or the use of some aspect of eHealth or mHealth technology. eHealth or “electronic health” refers to any health care practice supported by electronic processes and communication, while mHealth or mobile health, a subset of eHealth, involves the use of any mobile technology, such as mobile phones and wireless sensors, to deliver and share health information. 24 Aside from the focus on distantly delivered technology, other goals included a decision to focus specifically on female cancer survivors and restrict review to studies that reported on behavioral interventions for weight loss versus medication or surgical procedures. Studies were included if all participants were female, had completed active cancer treatments (specifically, radiation, surgery and/or chemotherapy) and provided information on weight change in their results. Studies were not included if the manuscript was not written in English, was only available in abstract form, participants were male, or if participants were actively engaged in cancer treatment at the time of the intervention. Finally, papers were not included if the primary form of intervention was other than telephone or eHealth technology. For example, if treatment was done in person and telephone or e-mail reminders were sent to participants, this was not considered an eHealth or telephone-based intervention. By the above definition, the search strategy identified only five papers that used some form of eHealth techniques as the primary intervention to encourage weight loss.25–29 Six additional papers that used telephone counseling to deliver intervention distantly were identified.30–35 All telephone-based intervention papers are described in Table 1. All eHealth/mHealth papers are presented in Table 2.
Distantly delivered interventions.

RCT: randomized controlled trial; IP: in-person; UC: usual care; BMI: body mass index; WW: weight watchers; RD: Registered Dietitian.
Significantly different than control; **not significant; ***significant loss from baseline.
eHealth/mHealth interventions.
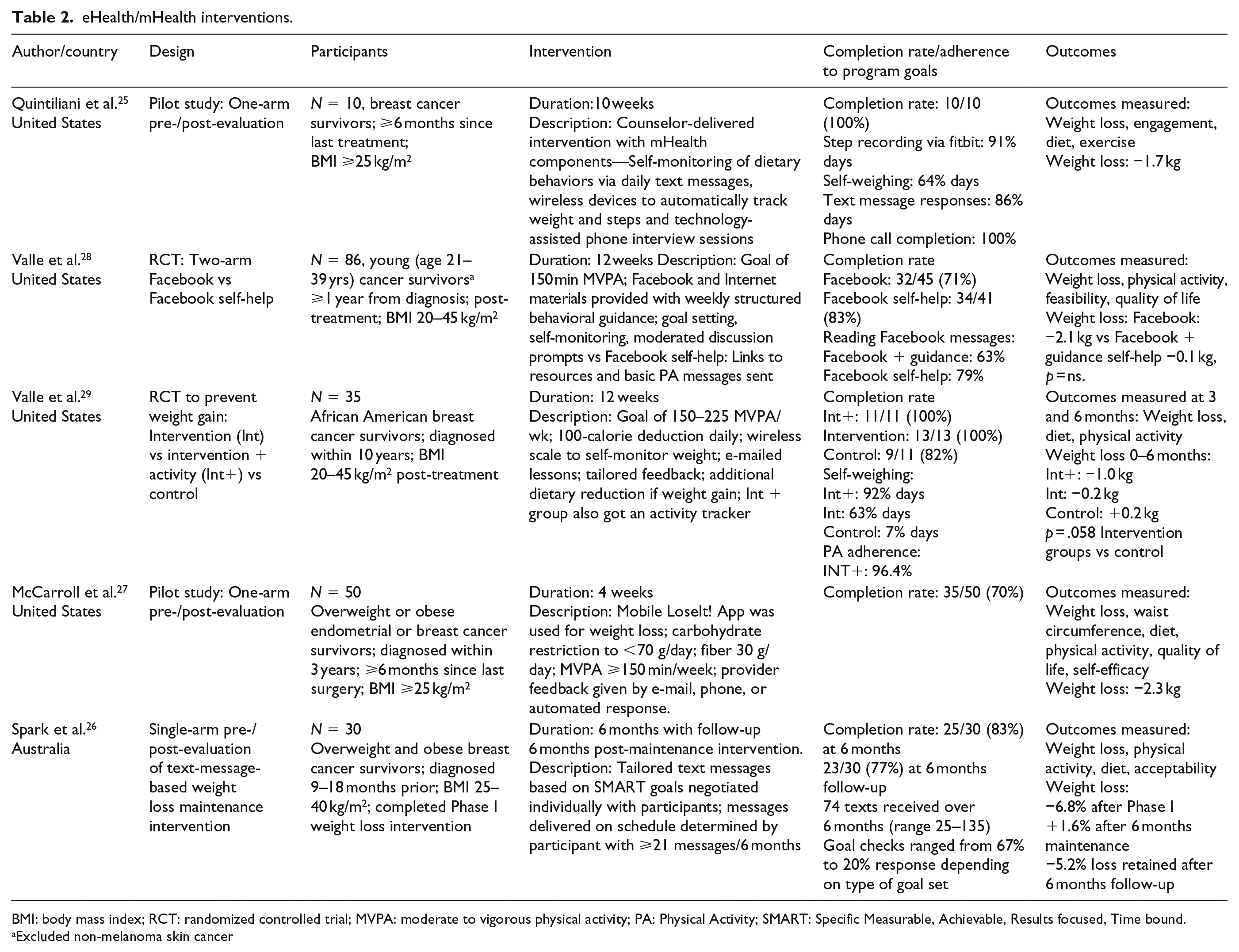
BMI: body mass index; RCT: randomized controlled trial; MVPA: moderate to vigorous physical activity; PA: Physical Activity; SMART: Specific Measurable, Achievable, Results focused, Time bound.
Excluded non-melanoma skin cancer
Distantly delivered interventions
Telephone
A total of six interventions for female cancer survivors were delivered using either group31,34 or individual phone calls.30,32,33,35 Women had body mass indices (BMIs) at baseline ⩾24 kg/m2, were within 10 years of diagnosis and, at a minimum, had been finished with treatment for at least 4 weeks. Intervention length ranged from 12 weeks to 24 months with the intervention dose (number of phone calls planned) being much more variable. The majority of studies started with front-loading calls by providing weekly contact for the first 3–6 months, then tapering calls to bi-weekly or monthly as time progressed. The dose of contact ranged from 11 calls planned in a 6-month period 30 to a high of 30 scheduled in a 12-month intervention. 35 All of the studies, save two,31,34 provided individual phone calls to women. The content of the calls was generally the same across studies with all counselors focused on diet, exercise and behavior modification techniques. Survivorship issues were reported to be a frequent source of conversation as well. Two of the studies31,34 included meal replacements as part of the dietary prescription, but the remainder all required a calorie (and sometimes dietary fat) restriction along with an exercise goal generally prescribed in minutes/week of moderate to vigorous physical activity (MVPA).
All but one study 34 used a randomized design and had either a control or usual care group or a treatment comparison arm. Harrigan 30 compared individual telephone counseling to individual in-person (or usual) care; however, two other studies mixed in-person versus telephone delivery with group versus individual contact. Both Harris 35 and Djuric 32 had participants meet in person in groups, but all telephone contact was individual. Given the evidence for the superiority of group intervention, 36 the inconsistency of group versus individual assignment within studies makes results, at times, difficult to interpret.
The dose of the interventions was also variable; yet across the first 6 months, Harrigan, 30 Harris, 35 and Goodwin 33 each provided between 11 and 16 individual calls over a 6-month period, and each obtained approximately equal weight losses of 4.8, 4.0 and 4.3 kg, respectively. This is about half of what would be expected with an in-person behavioral intervention, yet the dose of 11–16 calls is lower than the 24 in-person meetings that are typically scheduled over 6 months in an in-person program. 37 Therefore, the dose, not the medium of communication, may be an issue.
With regard to adherence, compliance and attrition, all studies reported a completion or follow-up rate, and only one of these studies did not report completion by treatment group. 32 Attention to adherence is particularly important when evaluating the benefits of new interventions or new modalities for intervention delivery. While overall study completion rates ranged from 68% to 94% across all treatment arms, completion specifically for the telephone intervention arms ranged from 68% to 91% when telephone arm attrition was compared to the other treatment arms. In the four studies where telephone arm completion was directly compared to an in-person or mail-based treatment, the telephone arm experienced greater attrition30,31,33,35 and therefore lower completion rates. In the two studies that could directly compare in-person session attendance to telephone call completion,30,35 attendance at in-person counseling sessions was superior with 61% and 87% attending in-person meetings where 47% and 68% completed scheduled phone calls (30 and 35, respectively).
By virtue of inclusion in this review, all studies reported on weight loss outcomes. Many studies also collected other behavioral measures, and some included biomarker or cancer symptom checklists. Outcome measures collected are listed in Tables 1 and 2, but only weight loss outcomes are enumerated here. To provide some frame of reference, effective behavioral interventions produce approximately 9 kg of weight loss over a 6-month period 37 and, as stated previously, clinically relevant weight loss can be obtained with body weight reduction as little as 5% of baseline. In the in-person Intensive Lifestyle Intervention arm of the Diabetes Prevention Program, participants lost an average of 6.8 kg, 7.2%, after 1 year of intervention. 38 Weight losses in the telephone arms of the cancer survivor studies ranged from 4.0 to 11.6 kg over 6 months. Excluding the 11.6 kg in the Befort 34 study which was obtained partially using meal replacements, the losses range from 4.0 to 8.0 kg. These losses are then somewhat lower than what could be expected with the “gold standard” in-person intervention but are comparable and likely approach clinical relevance. When phone interventions were compared to usual care or mail-based treatment arms, phone-based interventions were always superior either at producing more weight loss or at maintaining more weight loss. The only exception to this is the Harris 35 study where subjects in the phone arm continued to lose weight during the maintenance phase of the intervention where the in-person group gained 1.3 kg. This difference approached statistical significance (p = .056).
eHealth/mHealth
A total of five papers used eHealth or mHealth interventions to encourage weight loss in female cancer survivors. Of these five papers, two were pilot and feasibility studies (25, 27; n = 60 between them), one was a single-arm pre–post design (26, n = 30) and two were randomized controlled trials (RCTs; 28, 29; n = 121 between them). Therefore, over five studies, only 211 survivors have participated. Nevertheless, these five studies represent a diversity of eHealth techniques.
Participants in these studies were all, save one, 28 breast and/or endometrial cancer survivors who were all at least 9 months but not more than 10 years from diagnosis and had completed treatment at least 6 months prior to the trial starting. Mean BMI ranged from at least 25 to 45 kg/m2; one trial included only young (21–39 years) survivors 28 with one recruiting only African American women. 29
The length of the studies was much more variable than the telephone-based studies. Due to the pilot and feasibility nature of these studies, treatment length ranged from 4 weeks to 6 months with only one study being as long as 24 weeks. 26 The interventions themselves were equally diverse, thus making comparisons difficult and overall conclusions preliminary. Two interventions used e-mailed lessons and feedback,27,29 one used tailored text messages, 26 one provided participant input and advice via Facebook 28 and one delivered the intervention via phone yet had subjects report dietary intake using text messages while weight and physical activity were obtained with wireless devices. 25 The use of technology then was mixed both across and within the studies available. As stated previously, only two of the five studies offered any kind of comparison group, and both of these used a technology-based comparator. In Valle, 29 e-mailed lessons with tailored feedback were compared to e-mailed tailored lessons with an activity tracker, thus isolating the benefit of offering an activity tracker. In another study by the same research group, Valle, 28 Facebook was used as the medium through which study staff provided intervention delivery in the form of behavioral guidance, goal setting and self-monitoring, and this was compared to a Facebook self-help group that received basic, generic messages and links to resources. Therefore, instead of isolating the value of Facebook, the study evaluated the benefit of a behavioral intervention versus non-specific advice. All other studies used a one-arm, pre-/post-design.
In terms of adherence and completion rates, overall study completion ranged from 70% to 100% of subjects with study duration not having an appreciable impact as the 70% follow-up in McCarroll 27 was delivered over a 4-week time frame where Spark 26 ran a 6-month trial with 83% completion. Most studies reported on some process measures, therefore making the goal of feasibility and acceptability a bit easier to assess. Adherence to program goals appeared generally high, ranging from a low of 64% of participants reporting meeting self-weighing goals in the Quintiliani study 25 to over three quarters meeting step recording, self-weighing, text message and Facebook goals in other studies.26,28,29
While attrition appeared to be low and overall adherence appeared to be high, the weight losses reported in these five studies were far less than observed in the telephone-based trials reviewed above. However, this is possibly due to the drastically reduced intervention length. With one exception, 26 all of the eHealth/mHealth studies were no longer than 12 weeks or about half of the length of time the phone-based studies ran. Weight losses in the reviewed eHealth/mHealth studies ranged from 0.2 to 2.3 kg. This is approximately half the weight loss of the telephone trials in half the time. Although it is not accurate to predict that longer trials would result in enhanced weight loss, this typically happens 39 and should certainly be evaluated in the future.
Discussion
The stated purpose of this review was to evaluate the efficacy and current limitations of distantly delivered and eHealth/mHealth interventions for weight loss in female cancer survivors. Through this evaluation, suggestions for future directions can be provided. In terms of efficacy, the findings from the telephone-based studies reviewed are similar to what has been reported in reviews for primarily in-person weight control interventions in cancer survivors in which studies were primarily in person.16,22,23,40
Additionally, the results of the telephone-based interventions concur with those done in the general population.41,42 As such, there is considerable support for the efficacy of telephone-delivered interventions among female cancer survivors. However, questions remain. Specifically, issues needing further study and examination include dose (Would more phone calls be better?); intervention delivery (Is one-on-one better than group?); factors that influence adherence and compliance (Why are participants more likely to attend in-person meetings than phone calls given the inconvenience of meeting in person?) and timing of phone calls (Is it better to use phone-based interventions for maintenance or initiation of weight loss?). Despite these remaining issues, telephone-based interventions produced consistently more weight loss than usual care or mail-based programs. For this reason alone, they are a valid and easily disseminable technique for distant delivery of weight loss interventions.
By contrast, there was a notable lack of studies using eHealth or mHealth technologies that were not merely pilot and feasibility studies. So not only were there few completed studies to evaluate but they were very small in scope and sample size. The lack of studies using some sort of eHealth or mHealth technology was surprising, particularly when there has been a dramatic increase in weight loss trials for the general population using newer communications methods.43–45 The inclusion of pilot studies which are generally underpowered at least highlights the ongoing research in this field. Studies that are adequately powered to detect hypothesized effects are certainly needed. Moreover, based on the studies available, it is difficult to discern which technologies (text messages, e-mail, wireless scales and activity monitors) or combinations of technologies are most meaningful. Studies that have enough statistical power or are designed a priori with multiple treatment arms to deconstruct the relative contribution of each of these technologies are important and will move the field forward.
Another limitation of the eHealth/mHealth studies is the very short duration of most. The lack of evidence for long-term maintenance of weight loss highlights an opportunity for future intervention and investigation of the potential value of distantly delivered technologies. Similar to adults without cancer, it is likely that cancer survivors will face challenges to maintaining weight loss 46 Distantly delivered intervention modalities appear ideal as they have the potential to offer a cost-effective and more easily accessible means of delivering the repeated contacts necessary to sustain behavior change.40,41 In fact, two of the studies reviewed used either the telephone 31 or text messages 26 as a way to specifically discourage weight regain after weight loss. Both were successful in facilitating weight maintenance and suggest a valuable contribution of distantly delivered technologies. Moreover, in the study by Harris and colleagues, 35 the phone-based group maintained better weight loss than the in-person participants from months 6 to 12 of intervention again, suggesting a valuable use for distantly delivered technology as a way to sustain contact with survivors after treatment ends.
One aspect of distantly delivered technologies that needs further scrutiny is the issue of cost-effectiveness. Analysis of costs associated with intervention delivery or cost-effectiveness is rare. While less weight loss may be produced using various versions of technology, more women can be reached and perhaps at a significantly reduced cost compared to in-person interventions. Befort et al. 31 performed a cost-effectiveness analysis of a group-based phone intervention (26 sessions) but compared it to a much lower dose (10 sessions) mail-based intervention. It is not then surprising that the group phone-based program costs more per participant even considering the large difference in amount of weight lost between conditions. However, previous cost-effectiveness analyses of an Internet-delivered weight loss program compared to an in-person intervention did find significant savings attributable to the Internet-based intervention. 47 This suggests that when “apples” are compared to “apples,” technology may generally prove to be more cost-effective. However, these studies need to be done on cancer survivors as well as the general population.
Finally, rapid advances in technology provide endless opportunities and also significant challenges. In the time from funding acquisition to RCT completion, a technology deemed to be “effective” may be nearly obsolete—or have changed enough to require complete restructuring of an intervention. It is also the case that continual advances in eHealth or mHealth modalities present barriers to technology compatibility between participants and protocols. Therefore, while the digitizing of health care presents exciting opportunities for dissemination and reach, there are practical considerations that are often overlooked.
Conclusion
In summary, distantly delivered weight loss programs may provide a means to meet the needs of a growing and disparate group of cancer survivors and, based on the findings from this review, have potential to facilitate weight loss and maintenance of weight loss. It is important to note, however, that the vast majority of studies have been done on breast cancer survivors, therefore limiting these conclusions primarily to this subgroup of survivors. Moreover, the link between weight loss and actual improvement in survivorship has yet to be firmly established. Despite this, the growing body of evidence supports the continued investigation of eHealth and mHealth techniques. The overall strength of the current phone-based literature suggests that this modality is currently preferable for weight loss, at least until more is known about the efficacy of other technologies. Future research should continue to evaluate issues of dose, timing and adherence. Isolating specific types of technologies and evaluating cost-effectiveness are also very important. Finally, when these questions are answered, attention should turn to the integration of these methodologies into clinical care and survivorship programs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by National Institutes of Health Center of Biomedical Research Excellence Award P20GM103644 from the National Institute of General Medical Sciences (NIGMS) and R01 DK056746 from the National Institute of Diabetes, Digestive and Kidney Diseases (awarded to Dr Harvey). The content is solely the responsibility of the authors and does not necessarily represent the official views of NIGMS or NIH.