
Abstract
Background:
The clinical research nurse (CRN) plays a key role in conducting and managing clinical trials, ensuring patient safety, and aiding the advancement of care. However, a dearth of research has explored their role, responsibilities, motivations, and career aspirations of research nurses.
Aims:
To explore the motivations, experiences, and aspirations of CRNs.
Methods:
A qualitative descriptive design, employing semi-structured online interviews were conducted with CRNs (n = 23), recruited via social media, between February and March 2023. Data were analysed using thematic analysis with inductive coding. COREQ reporting guidelines were used.
Results:
Three themes were identified related to the CRN’s role and aspirations: misconceptions and misunderstandings of the CRN role, role of the CRN and motivations, and professional identity and values.
Conclusions:
The role of the CRN is believed to be misunderstood within and across professionals’ groupings. This was attributed to a lack of standardisation regarding job titles, scope of practice, professional identity, and career progression resulting in the role being undervalued. Recognising the unique identity and practice of CRNs is necessary to reduce misconceptions and build this career pathway for others.
Keywords
Introduction
Globally, the role of the clinical research nurse (CRN) has been identified as essential to improving health outcomes (Johnson, 2022). However, there is no international consensus on the title, competencies, or responsibilities associated with the role (Backman Lönn et al., 2022; Fisher et al., 2022; Xing et al., 2024). Titles vary widely, including ‘Clinical Research Nurse’, ‘Research Nurse’, ‘Clinical Trials Nurse’, and ‘Study Coordinator’ (Fisher et al., 2022). Consequently, only estimates exist regarding the number of nurses working in these roles, with figures ranging from 5545 in the United States (Johnson, 2022) to 7469 in the United Kingdom and Ireland (NIHR, 2023).
Traditionally, a CRN is an autonomous registered nurse (Backman Lönn et al., 2022) who may manage trials, coordinate teams, mentor staff, and ensure patient safety (Xing et al., 2024). However, the role differs internationally. In Australia and New Zealand, CRNs can act as principal investigators while managing other studies (Brinkman-Denney, 2013; International Association for Clinical Research Nurses and American Nurses Association, 2016; Whitehouse and Smith, 2018; Australian College of Nursing, 2022). In contrast, in Italy, the role is practice-focused with no management responsibilities (Martucci et al., 2020); whereas in Sweden, there is no consensus regarding the scope of practice or preparation (Backman Lönn, 2023).
Despite the prevalence and value of CRNs, the role remains largely invisible within major policy frameworks (Colquhoun et al., 2025) and is associated with limited professional development opportunities and formal credentials, which undermines both role identity and career progression (Kunhunny and Salmon, 2017;Colquhoun et al., 2025). Most research on the CRN workforce has focused on oncology trials (Purdom et al., 2017; Biswell et al., 2021), perceptions of the role’s value (McCabe et al., 2019), and challenges faced in practice (Hernon et al., 2020). However, there is little exploration of the motivations for becoming a CRN and the factors influencing their career aspirations within the UK context.
Historically, CRNs have been reported as an undervalued and misunderstood component of the nursing workforce (Hunt, 1983; Jones, 2015; Tinkler et al., 2018; Tinkler and Robinson, 2020; Adan, 2023). This has been attributed to the lack of standardisation in title, role, and preparation, which collectively pose barriers to implementation and understanding in practice (Tinkler et al., 2018; Backman Lönn et al., 2022).
Although dated, early research (Hunt, 1983) indicated that ward-based nursing colleagues held negative perceptions of CRNs, showing little support or value in their role. More recently, a continued lack of awareness and visibility among nursing colleagues has been reported (Whitehouse and Smith, 2018; Faulkner-Gurstein et al., 2019; Adan, 2023). Faulkner-Gurstein et al. (2019) suggested that such misunderstanding deters potential nursing colleagues from viewing this as a career pathway, with many entering the specialism in an ad-hoc manner.
Some studies have explored why nurses are drawn into the CRN role. Faulkner-Gurstein et al. (2019) reported a key motivator was the opportunity to maintain patient interaction while engaging in research activities, offering the ‘best of both worlds’ from a nurse’s perspective. However, there is no formalised career pathway for CRNs (Brandenburg and Ward, 2022), and entry requirements vary with regard to knowledge, experience, qualifications, and skill set (Backman Lönn et al., 2022; Avery et al., 2023). In Sweden, CRN education is often informal (Backman Lönn et al., 2022), whereas in the United Kingdom, qualifications related to clinical research are not mandatory. Consequently, Faulkner-Gurstein et al. (2019) found that 25 CRNs employed in London healthcare had diverse backgrounds, qualifications, and experiences, with many accessing most training after entering the role.
Research exploring the CRN role reveals complexity (Hernon et al., 2020; Biswell et al., 2021), particularly regarding uncertainty about boundaries of practice (Faulkner-Gurstein et al., 2019; Hernon et al., 2020). This has resulted in reports of conflicting imperatives for professional identity and research delivery (Tinkler et al., 2018), inconsistent contracts with limited progression (Bozzetti et al., 2025), professional isolation (Hernon et al., 2020), and inappropriate utilisation during staff shortages to fill gaps in clinical teams (Faulkner-Gurstein et al., 2019). Although in recent years there has been a wide range of research on clinical research nursing (Cleaver, 2020; Tinkler et al., 2022; Bozzetti et al., 2025), there remains a lack of studies exploring the motivations behind becoming a CRN and the factors influencing their career aspirations.
Methodology
Aim
The aims of this study were to explore the motivations, role, and career aspirations of CRNs in the United Kingdom.
Design
A qualitative, exploratory research design was employed to gain an in depth understanding of CRNs’ experiences (Creswell, 2014). The study was underpinned by a social constructionist perspective, enabling exploration of (in)consistency and (in)congruences in their roles and aspirations in a comprehensive manner. Brief demographic and workplace data were collected prior to conducting online interviews. This report adheres to the Consolidated Criteria for Reporting Qualitative research checklist (COREQ), a 32-items checklist (Tong et al., 2007, Supplemental File 1).
Participants
Convenience sampling was employed to recruit participants via online professional social media platforms (Green and Thorogood, 2018).
An invitation link to participate in an interview was posted on Facebook and X (formerly Twitter). Interested individuals were directed to contact the researcher (LH). Subsequently, an information pack – including a participant information sheet, outlining the study aim, confidentiality, and withdrawal procedures – was emailed to potential participants. Upon receipt of the consent form, eligibility was confirmed, questions were clarified, and an interview time was arranged.
Data collection
Online interviews were collected between February and March 2023 via MS Teams, accommodating the wide geographical distribution of participants. All interviews were carried out by LH (a registered nurse studying MSc in Nursing) who had received training in qualitative interviewing. The interview schedule (Table 1) was developed in response to the aim of the study and existing literature (Creswell, 2014) and included open-ended and focused questions, with prompts used to elicit deeper responses. One pilot interview was conducted, with no modifications required.
The interview schedule.
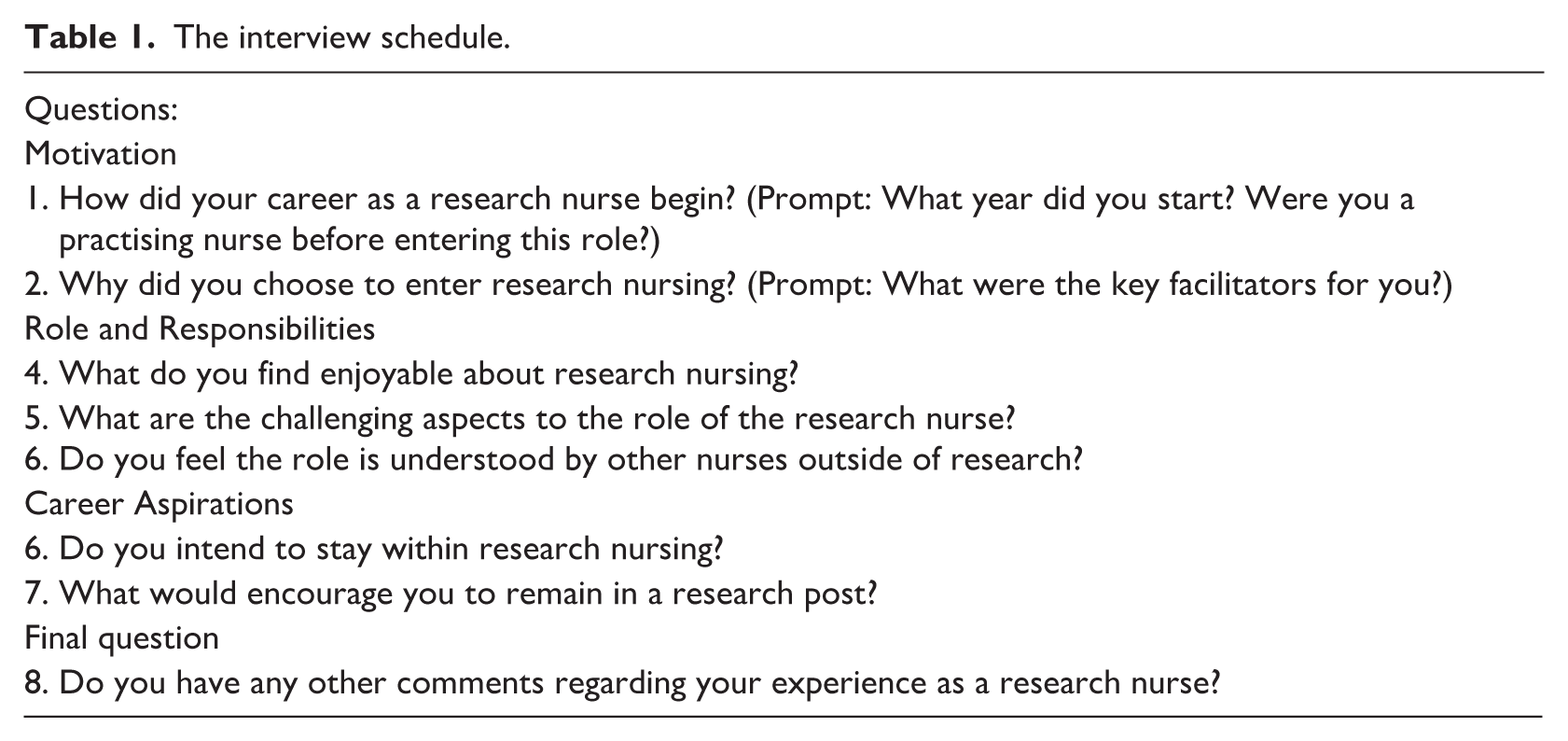
Participants were not required to use video during interviews; only audio recordings were captured. Interviews were scheduled outside working hours and lasted approximately 20–45 minutes. Field and reflective notes were recorded after each interview to capture nuances (Creswell, 2014). Written informed consent was obtained prior to interviews. Data collection continued until thematic saturation was reached, confirmed by two additional interviews in which no new themes emerged. The researcher (LH) had no prior relationship with any participant.
Ethical considerations
Ethical approval for this study was obtained (Protocol approval number: FCNUR-22-087 17.11.2022). Participants were screened for eligibility and provided with detailed information about the study. They were given the opportunity to ask questions before providing both verbal and written informed consent. Participants were informed that they could withdraw from the study at any time without any negative consequences. No participants withdrew after consenting. All interview transcripts were anonymised during transcription, and each participant was assigned a unique study identification number, which is presented alongside quotations.
Data analysis
Interview transcripts were downloaded, with errors removed to enable coding and analysis. Data analysis was conducted manually by the team, following the principles of thematic analysis (Burnard, 1991). This involved repeated reading of transcripts, open coding, grouping codes into categories and the development of overarching themes. Analytical decisions were documented throughout the process to enhance transparency and rigour, with reflexive consideration given to the researchers’ influence on interpretation. To support reflection and interpretation, the lead researcher created memos after each interview to capture initial impressions and emerging ideas, which informed the sense-making process. The primary researcher (LH), and the secondary researcher (FH), a PhD qualified university lecturer with expertise in nursing workforce, read transcripts multiple times to achieve data immersion. All members of the research team identified as female.
Pseudonyms were assigned to each participant and recorded in a password-protected file, fulfilling the ethical duty of confidentiality. Data analysis followed an inductive approach. Transcripts were read independently to gain an overall impression and identify initial recurring codes. Emerging codes (n = 20) were compared, and the two researchers engaged in several discussions to merge similar codes and remove redundancies. These codes were subsequently collapsed into broader categories, from which overarching themes emerged, corresponding to the subheadings in the results section. Due to time constraints, member checking was not undertaken, which is recognised as a limitation of the study. In the final analysis stage, the researchers selected quotes to support the themes identified.
Rigour
Lincoln and Guba’s (1985) criteria were applied to ensure the rigour of the study. Transferability was supported by providing descriptions of the research context, setting, participant selection rationale and interview procedures. To enhance dependability, audio recordings of each interview were compared against the transcripts to ensure accuracy. Additionally, independent data analysis by two authors strengthened both dependability and credibility. Participant quotes included in the findings offer thick descriptions of their experiences.
Further supporting transferability, the use of social media platforms facilitated recruitment from a wide geographic area, ensuring diversity in participant experiences. Reflexivity was embedded throughout the qualitative process (Polit and Beck, 2010). The primary author (LH), who has a research nursing background and currently works as a CRN, maintained a reflective diary to document subjective responses during the study. In addition to reflective notes, an audit trail of coding decisions was maintained to demonstrate transparency and rigour.
Results
Characteristics of participants
The characteristics of the 23 participants are presented in Table 2. The majority were female (87%) which aligns with findings from previous studies in this area (Backman Lönn et al., 2022). Participants’ experience varied: 43% (n = 10) had less than 5 years of experience as a CRN, whereas 39% (n = 9) had over 15 years of experience. All participants were employed within the NHS, and over a third (35%) reported covering multiple disease areas and specialities within their research role. These included neurological, infectious diseases, oncology, and gastrointestinal across both adult and paediatric healthcare, patterns observed in earlier research (MacArthur et al., 2014). Most participants (60%) held postgraduate qualifications; however, only 43% (n = 11) reported completing specific research module training. Two participants (9%) had undertaken an MSc in Research, and one had completed a PhD. It remains unclear whether other postgraduate qualifications included research-focused modules, as this was not explicitly captured.
Characteristics of participants.
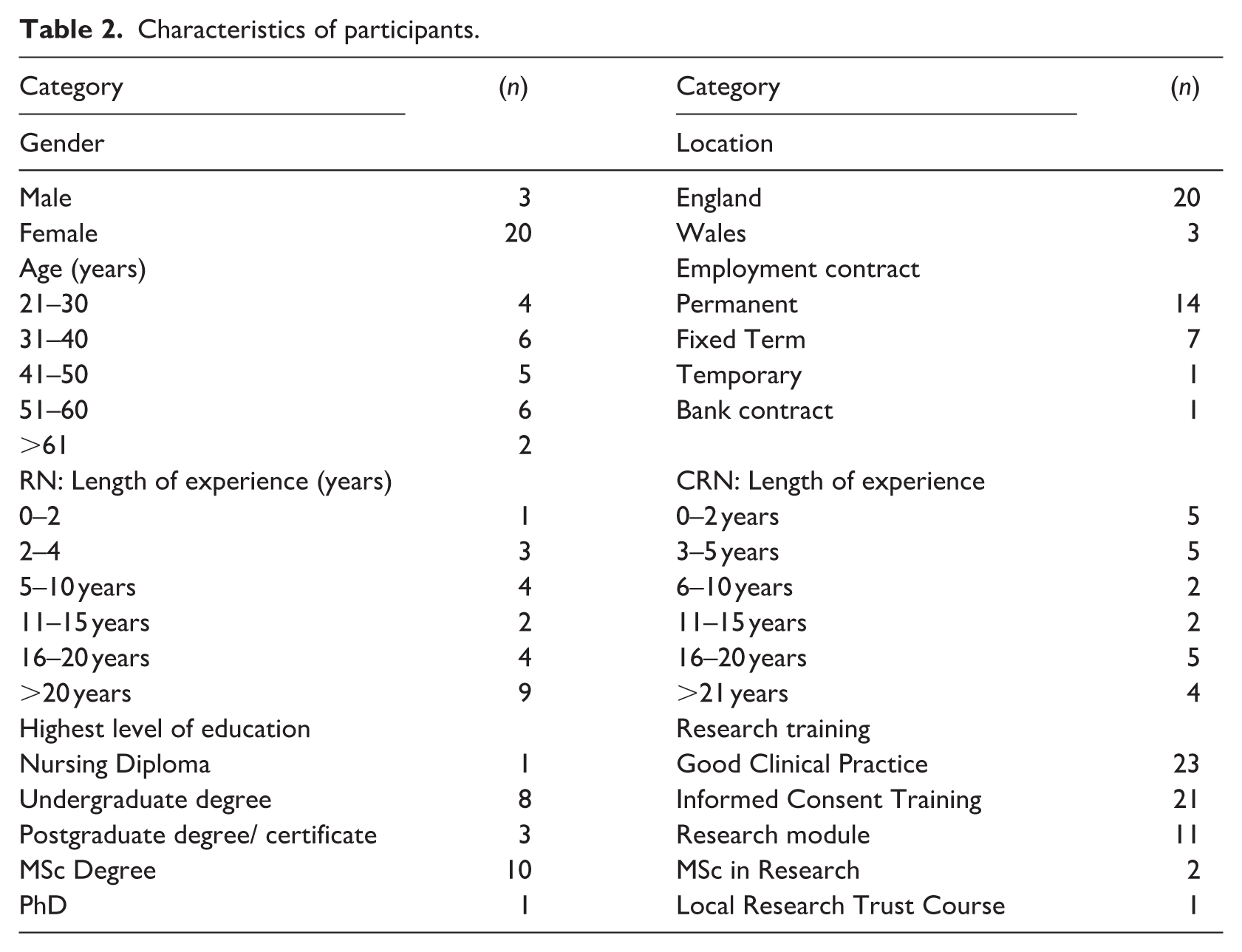
CRNs form part of a highly educated workforce, with mandatory training such as Good Clinical Practice and Informed Consent required before commencing research activities. Many CRNs pursue further education, including university-based research modules, MSc degrees, and PhDs. Although some undertake their own research studies within their local departments or as part of postgraduate qualifications, the primary focus of the CRN role is delivering clinical trials sponsored by pharmaceutical companies, universities, and charities, working under the direction of a Principal Investigator.
Three main themes describing CRNs’ roles and aspirations were identified: (1) misconceptions and misunderstandings of the CRN role, (2) role of the CRN and motivations, and (3) professional identity and value.
Theme 1: Misconceptions and misunderstandings of the CRN role
One of the strongest themes related to widespread misconceptions and misunderstanding surrounding the CRN role was misconceptions and misunderstandings of the CRN role. Several common stereotypes were reported, including that their role was ‘an easy job’, ‘hidden’, where nurses ‘sit in an office all day’ and ‘walk around with clipboards’. The CRN was often not viewed as a ‘clinical’ nurse and was more frequently mistaken for academic researcher. In some cases, the role was considered an ‘added extra’ rather than an integral part of nursing practice. Consequently, all participants expressed that their role was poorly understood within their own profession, across services or organisations.
I was told research is where nurses go to retire (Participant 17) My previous colleagues didn’t understand why I was moving into research – they thought it was a dead end, easy job. (Participant 6)
Within the nursing profession, misunderstanding of the CRN role was attributed to several factors. Firstly, participants highlighted a lack of emphasis on clinical research education and ineffective teaching strategies to engage undergraduate nursing students with research opportunities. Secondly, misconceptions were reinforced by the limited clinical exposure to the CRN role during pre-registration placements. Participants noted the absence of opportunities to engage and mentor student nurses during these placements, resulting in missed chances to promote understanding of the role and its contribution to patient care and research.
I know for a fact that one of my former colleagues almost resented research – they didn’t see it as important. I think it's quite an archaic view. Historically, research has been seen as something, like an ivory tower, or not necessarily as an important role. (Participant 3) When I was a student nurse, I asked the lecturer if there was any way I could get involved in research. Their response was simple ‘no, not really’, that was it. (Participant 3)
Misunderstanding about the CRN role was perceived to persist among nursing colleagues, resulting in resistance to recruiting patients for trials. This was often viewed as adding to the workload of already overstretched ward nurses. Such perceptions created relationship conflicts in the workplace and ultimately the success of patient trials. Many participants reported that these challenges were influenced by the clinical setting, the degree of role embedment, and the level of exposure to the CRN role. One participant reflected engaging with the endoscopy unit, which enabled nurses to develop a better understanding of the CRN compared to nurses working on the ward: Sometimes the staff's absolutely run ragged, and it can be tricky to ask them to do additional tasks because research is happening in their department. So, we do try to give back as much as we can. For example, in endoscopy we’re recruiting patients into our studies, we will work with our endoscopy colleagues and help with tasks like cannulations. (Participant 22)
Differing levels of misinterpretation was believed to extend across multi-professional groups and organisational cultures. Symbolically, several participants commented that the lack of standardised role title and the interchangeable use of terms – often omitting ‘clinical’ from the title – reinforced stereotypes. Others reflected that their role sat outside the traditional nursing directorate within the organisational structure, contributed to further misconceptions about the role.
No time is made for research, it is seen as an afterthought, an added extra (Participant 9)
Such misconceptions had a profound impact. Personally, participants reported feeling demoralised and frustrated, with some considering leaving the role. Professionally, the lack of understanding among nursing and other non-research colleagues, exposed them to daily resistance and conflict – hindering their ability to perform their duties. These misconceptions not only shaped their own experiences but were also believed to influence the perceptions of those preparing to enter this line of work.
These misunderstandings were believed to contribute to the professional undervaluation of the CRN role. One participant stated that within their trust, lip service was paid to research, with little genuine support provided. Several reported feeling that during the COVID-19 pandemic, they were easily redeployed to other clinical areas, perceived as easy targets – confirming the low status attributed to their role and contribution to patient care. Many expressed frustrations at the dichotomy of being removed from clinical trials, despite such engagement being central to the development of vaccines and treatments for COVID-19. At a societal level, participants perceived that the pandemic increased public awareness of research, offering hope for greater recognition.
However, participants felt that the opportunity to capitalise on this momentum to educate nursing colleagues and others was missed. Some also perceived that routes to accessing the CRN role were inhibited due to misunderstandings about the role among others.
Student nurses tend to be more in tune with research and more open to it than other nurses. (Participant 11) Within my trust, decision-makers often don’t know anything about research nurse’s role. Research is seen as an optional extra, . . ..and we aren’t given any respect. (Participant 10)
Recommendations to improve education were commonly reported. These included promoting research across the nursing profession, beginning with embedding research within pre-registration curricula and providing clinical exposure to the CRN role. Professionally, participants suggested initiatives such as appointing ‘research champions’, leveraging programmes like NIHR’s 70@70 – which develops senior nurses as research leaders in the United Kingdom; and using resources such as NHS England’s Matron’s Handbook, which provides guidance for nursing leadership, to promote research awareness and integrate research into clinical practice among nurses.
Theme 2: Role of the CRN and motivations
Reported reasons for choosing the CRN role varied and included personal and professional domains. Personally, the most frequently cited motivations included a strong interest in research, enthusiasm for the medical specialty in which the research was focused, the desire for a better work–life balance, and the opportunity to work in a nursing role that offered more predictable ‘9–5’ hours.
I love feeling that we have changed lives – seeing improvements in quality of life and even life expectancy. (Participant 3) . . . it’s probably a better work-life balance, that probably I take for granted. But that wasn’t the reasons I went into research – it just happened that way. But it's definitely a nice factor. (Participant 6) Research nursing is like marmite; you either love it or hate it. (Participant 18)
Professionally, reasons for choosing the CRN role included seeking a change from traditional ward nursing, desiring a less physically demanding role, and wanting to engage in something unique that advanced patient outcomes while supporting career progression through higher banding and secondments. Participants also shared reasons for remaining in the role, with three key motivating factors emerging. Firstly, being part of a trial team that contributed to improved clinical treatments and innovative healthcare delivery was highly valued. Secondly, many enjoyed the variety of research work, the collaborative teamwork, and the autonomy afforded by the nurse-led nature of the role. Work–life balance was frequently mentioned, with participants highlighting the absence of weekend and shift work as contributing to better mental health and job satisfaction. Finally, unlike traditional nursing roles, the CRN position facilitated the development of therapeutic relationships with patients. Tasks such as pre-screening, recruitment, continuous monitoring, and communication allowed substantial patient interaction, enabling holistic care and stronger therapeutic bonds.
Day-to-day, I like the fact that there is a mix of patient-focused and office-based work. I’m not running around . . . doing a very physical job for the full shift, but I'm also not stuck in an office without using my nursing skills. So, I get to have the best of both worlds. (Participant 20) It’s very different from a relationship you have as a nurse in clinical practice, you might look after somebody for a couple of days and . . . get to know them quite almost acutely and you may never see them again. In research, when you're following up, you develop an in-depth relationship with them. They learn about you, you learn about them, and that makes the role really rewarding. You’re their first contact . . . and it’s great being at the cutting edge. (Participant 23)
Findings revealed the complexity of the CRN role, which involves balancing the delivery of safe, ethically sound, patient-centred care with the demands of managing complex clinical trials. Within this pivotal role, CRNs frequently liaised and collaborated with large multidisciplinary teams, including consultants, pharmacists, laboratory staff, and radiology personnel, among others. However, the day-to-day remit of the role varied considerably depending on the clinical specialty, team structure, and organisational context.
It’s draining, having to put yeourself out there constantly. (Participant 8)
Across the interviews, participants highlighted the variable nature of clinical trials, which resulted in inconsistent workload patterns. They described periods of relative quiet while waiting for studies to open, followed by episodes of intense activity with demands from multiple sources. Participants spoke about the significant time and effort required for tasks such as writing protocols and securing ethical and governance approvals, expressing frustration when trials closed early or failed to start, rendering prior work wasted. Labour-intensive activities, such as months of pre-screening, were also reported as not always leading to successful patient recruitment, particularly when eligible patient populations were unavailable. Some participants noted that these challenges were compounded by sponsor-driven pressure to recruit, which created feelings of significant stress and negatively impacted morale.
The amount of time spent, I spend on recruiting patients and pre-screening is unreal, only to find they are not eligible . . .. then you have research teams, funders and sponsors all on your back . . . it’s just stress. (Participant 22)
Several participants touched on the contractual dependency of their role which reflects the episodic nature of research funding and the time-limited structure of many research projects. This reliance on short-term contracts can create some uncertainty for CRNs, impacting their sense of job security and career progression. For some, the lack of role permanency led to some considering leaving when funding ends, leading to a cycle of recruitment and training that disrupts continuity.
I really want to stay as a research nurse, but I’m anxious about my contract ending soon. (Participant 3) I think one of the challenges that we have is our contracts and that a lot of research nurses have fixed term contracts. I’ve had permanent contracts and now I’ve moved on to a fixed term contract which is a little bit of a worry. (Participant 23) Research nurses must have a personality to persevere. (Participant 16)
Although most participants stated they planned to remain in the CRN role, describing it as ‘fulfilling’ and expressing that they ‘loved the role’, some indicated intentions to change careers, pursue a PhD, or transition from the NHS to private sector research roles. Analysis revealed several challenges and areas for improvement to enhance retention. Employment contracts varied widely, ranging from permanent to fixed term and temporary arrangements, with participants strongly advocating for permanent contracts. A lack of progression within research nursing was frequently noted, with no clear career pathway and a perceived ‘ceiling’ at Bands 6 and 7, and few Band 7 roles available in practice. Developing and implementing structured career pathways was identified as a key factor to support progression and retention, as participants reported ‘no rewards or incentives for increased responsibility’ (Participant 2) at present. Better engagement from doctors acting as Principal and Sub-Investigators, as well as from colleagues outside research, was also seen as essential. Participants suggested that career pathways should include opportunities to lead nurse-led studies as Principal Investigators and to engage more actively in local research. Additionally, greater access to continuing professional development was viewed as critical to encouraging retention within the role.
Theme 3: Professional identity and value
A recurring theme across interviews was the perceived lack of professional identity and value attributed to the CRN role by management, employers, and key stakeholders. These beliefs were reflected in participants’ experiences from induction through the day-to-day realities of the role. Many described a ‘big jump’ when transitioning from ward-based nursing to research nursing, noting that induction programmes varied nationally. Although some trusts offered bespoke programmes with extensive support, many participants reported a lack of structure and poor support, with an emphasis on ‘on-the-job learning’. Working within small teams often compounded feelings of isolation, despite the responsibility of managing large and complex research portfolios, often in physically compromised settings.
Examples of variable support were commonly cited across the data. Most participants highlighted issues with inadequate working spaces and lack of room for essential equipment. Although some CRNs worked in purpose-built clinical research facilities, others described sharing cramped office spaces, likening them to a ‘broom cupboard’. This lack of space often made it difficult to conduct patient visits or accommodate clinical research associates during monitoring visits.
We have no space; it’s logistically challenging – no space to see our patients or store of trial equipment. (Participant 23)
Many described unpredictable cycles of ‘quiet times during set-up’ followed by intense recruitment phases, leading to inconsistent workloads. Support structures also varied; some CRNs had access to administrative teams or clinical research laboratories for processing patient samples, whereas others described their role as being a ‘jack of all trades’. Many reported undertaking a wide range of tasks beyond their core responsibilities, including administrative work, financial reporting, organising patient travel, and other clerical duties. Additionally, some participants noted having to operate complex laboratory equipment independently, further contributing to workload pressures.
Sometimes I feel like, um. . . . like the nursing role isn’t always clearly defined or it gets very blurred. . . . you feel that you have to do a wide range of things and it’s hard to know when the nursing role stops and starts. There is a lot of paperwork . . . a new environment getting used to the finance and the administrative teams behind the scenes. (Participant 1) I love going out recruiting patients . . . working with such a vast array of people you know, your commercial partners . . . your academics, your medics . . . and you’re advising. And one of the main challenges is for us at the moment is we’ve got about 150 studies open, many more still in follow up and a huge amount set up. People are live, manage and and making sure that the service is covered. (Participant 21)
The lack of standardised support reinforced feelings of diminished professional identity and value among CRNs. Despite recognising their role as that of a specialist nurse, many participants felt they were not regarded with the same status as other specialist nurses. Consequently, they perceived their role as undervalued and not taken seriously by other healthcare professionals. This lack of appreciation for the complexity of research was further evidenced during the pandemic, when CRNs were seen as ‘easy targets’ for redeployment. Although participants expressed willingness to assist during the crisis, they voiced concerns about the impact on patients enrolled in trials and felt senior managers did not share these concerns. Overall, participants believed research was not prioritised within their organisations, attributing this to decision-makers at management level having a poor understanding of the pragmatic aspects of research.
It’s always the research team who get asked to support on the ward in the clinical areas and stuff, because there's this misconception that research nurses sit behind a computer not busy, and they can just drop everything. (Participant 15)
Participants also reported a lack of recognition of the ethical dilemmas inherent in the CRN role. Pressures to recruit to trials from sponsors and Principal Investigators were described as challenging, often placing CRNs in the difficult position of balancing the best interests of patients against recruitment targets, deadlines, and expectations for results. Many commented on the frustrations of navigating ‘red tape’ and governance processes when setting up studies, as well as the difficulties of accessing patient populations without adequate organisational support. Participants suggested that success in the role requires confidence and strong interpersonal skills to network effectively and recruit patients. Collectively, these findings suggest that CRNs do not feel adequately respected, valued, or prioritised within the health service.
Discussion
Previous studies have highlighted the diversity of the CRN role, the lack of career progression, and misconceptions surrounding the position. Findings from this study confirm that misconceptions persist and directly influence the construction of professional identity and perceived value (Hernon et al., 2020; Tinkler et al., 2022). Participants attributed these misconceptions to limited education and clinical exposure to research nursing within pre-registration curricula. Many reported having little or no knowledge of the CRN role prior to accepting their post, contributing to a broader lack of awareness across the nursing workforce. These challenges have been documented in both national (Faulkner-Gurstein et al., 2019; Kunhunny and Salmon, 2017;) and international literature (Bozzetti et al., 2025; Johnson, 2022). The lack of a standardised title was viewed as contributing to misunderstanding, reflecting previous research (Fisher et al., 2022). For example, the title ‘clinical research nurse’ was often incorrectly conflated with ‘nurse researcher’. However, these roles differ significantly: CRNs typically manage externally sponsored studies, whereas nurse researchers design and implement their own research (MacArthur et al., 2014). To address these issues, there is a need for well-defined career pathways that enable CRNs to move seamlessly between contributing to research teams and leading studies, supported by titles that accurately reflect these roles. However, this progression is complicated by longstanding cultural assumptions – such as questioning the necessity of a nursing degree and associating research exclusively with academia – which continue to shape perceptions of nursing research leadership and create barriers to advancement.
Consistent with earlier findings (Kunhunny and Salmon, 2017), this study reports that the CRN role is not widely perceived as valued across nursing, healthcare, education, and management and remains poorly understood by those outside research. Many participants expressed frustration at being regarded as ‘supernumerary’ or redeployed to cover nursing shortages, most notably during the COVID-19 pandemic – a sentiment echoed by Hernon et al. (2020). Cleaver (2020) argued that such misunderstanding can lead to the role being under-utilised. Nurses, however, need to recognise that research is an essential component of their professional role – ranging from critically reviewing evidence to inform everyday clinical decisions to leading complex, multi-site trials. Embracing this continuum of research activity is vital for advancing patient care and strengthening the evidence base within nursing practice.
Key motivations for entering the CRN role included the desire to improve work–life balance, with participants valuing a more traditional nine-to-five schedule compared to twelve-hour ward shifts. Several highlighted that this pattern complemented family commitments and improved mental health. These findings align with Cleaver (2020), who reported increased job satisfaction and enhanced work–life balance among research nurses. Other motivators included opportunities to build on existing skills, develop a specialism, achieve a higher pay grade, and work in a less physically demanding environment. In the United Kingdom, the NHS People Plan (NHS England, 2019) prioritises well-being and flexible working, which aligns with CRN motivations; however, the absence of clear progression routes highlights a disconnect between policy ambitions and operational reality. Addressing these gaps requires cultural change and system-level action to normalise research as part of everyday clinical nursing practice (NHS England, 2020).
Despite these benefits, participants reported challenges such as variability in workload, recruitment pressures, poor engagement from medical staff, and inadequate working environments. Numerous ‘unseen’ tasks – such as trial set-up, pre-screening and recruitment – often felt wasted when studies closed early or failed to start, reducing morale. Success in the role was perceived to require confidence and proactivity, as CRNs often needed to engage patients and network effectively. Pressure to recruit and meet targets from Principal Investigators and sponsors was also highlighted as a significant source of stress. These challenges mirror the general workload pressures currently experienced across nursing, where increasing demands and resource constraints contribute to heightened stress and reduced morale.
Although participants expressed commitment and satisfaction with their role (Hill, 2018; Kunhunny & Salmon, 2017; McCabe et al., 2019; Tinkler et al., 2018), many voiced frustrations at the absence of an established career pathway. Several aspired to progress into roles as Principal Investigators, but identified significant barriers, as these positions are historically viewed as the domain of consultants. Leadership roles exist within research-oriented trusts; however, they were described as difficult to access due to limited opportunities and poorly defined progression pathways (Hernon et al., 2020). Some participants indicated that, to achieve their career ambitions, they might leave research nursing altogether, transitioning into academia or the private sector. Although NHS People Plan priorities on well-being and flexible working align with CRN motivations, the absence of clear progression routes highlights a disconnect between policy ambitions and operational reality. Addressing these gaps requires cultural and systemic change to embed research roles within the nursing workforce planning and leadership strategies, as emphasised in UK national frameworks such as the NHS Long-Term Plan and NIHR Clinical Research Nursing Strategy (NHS England, 2019; NIHR, 2020). These frameworks underscore the importance of research as a core element of nursing practice and leadership.
To support retention and professional development, several strategies should be considered. These include establishing a defined career pathway, increasing the use of permanent contracts to promote job security, and creating opportunities for CRNs to act as Principal Investigators and lead nurse-led research studies. Promoting awareness of the CRN role among newly qualified nurses and incorporating mandatory training programmes among qualified nurses and other healthcare professionals may help to foster awareness. These measures would help align operational practice with national policy ambitions to embed research as a core function of the NHS.
Strengths and limitations
A strength of this study lies in the diversity of the sample, which included CRNs of varying ages and lengths of experience, potentially enhancing the transferability of findings across multiple settings. Further strengths of this paper include the use of the COREQ checklist to guide reporting, alongside the incorporation of thick descriptions and illustrative quotes that capture and reflect the strong voice of participants.
However, several limitations should be acknowledged. The study was conducted exclusively within the United Kingdom and included only NHS-employed CRNs, limiting diversity and potentially reducing generalisability in an international context. Although social media was used for recruitment, there remains a risk of selection bias, as participants’ experiences may not represent the wider CRN workforce. This geographic and network-based focus may limit the transfer of findings to CRNs working in other regions or those not affiliated with professional networks, who may have different experiences and perspectives. This may also restrict both the transferability and international applicability of the findings. Finally, member checking was not undertaken, meaning the themes generated may not fully reflect participants’ intended meanings.
Conclusions
The findings of this study highlight a significant variation in the role, responsibilities, and career aspirations of CRNs across the United Kingdom. Persistent misconceptions and misunderstandings of the CRN role by other healthcare staff often led to friction and reinforced the perception that research is an additional ‘extra’ rather than a core component of care. Despite these challenges, most CRNs expressed enjoyment and commitment to their role, citing satisfaction from contributing to medical breakthroughs and improving patient outcomes. However, opportunities for career progression varied considerably between trusts, with some nurses indicating they would need to leave clinical research to advance their careers.
To address the challenges identified, a coordinated approach across education, practice, healthcare systems and research is essential. Nursing education should integrate research awareness and skills into pre-registration curricula, supported by structured research training and exposure to research placements for qualified nurses. In practice, research must be embedded into everyday care through protected time, research champions, and clear career pathways that enable nurses to move fluidly between contributing to and leading studies, supported by titles that accurately reflect these roles. At a system level, research roles should be incorporated into workforce planning and leadership strategies, with permanent contracts and bridging funding to promote stability, aligning with national frameworks such as the NHS Long-Term Plan and NIHR Clinical Research Nursing Strategy. Finally, further research should explore international comparisons of CRN career structures, evaluate the impact of educational interventions on research engagement, and examine strategies to overcome cultural barriers and improve retention. Collectively these measures would normalise research as a core function of nursing practice and strengthen the evidence base for patient care.
Key points for policy, practice and/or research
Recent research has explored the complexity of the CRN role, but little attention has been given to motivations for entering the role or career aspirations.
Participants reported misconceptions and misunderstandings of the CRN role by other staff, often leading to friction and a perception that research is an ‘added extra’ rather than a priority.
Most CRNs enjoyed their role and did not intend to leave research; however, career progression opportunities varied significantly between trusts, with some nurses stating they would need to leave research to advance.
Clear role definitions and fluid pathways enabling varied roles within a research focused career should be set up.
There is a critical need to advance nurse-led and nursing-focused research to drive evidence-based practice and improve patient outcomes.
Further research is recommended to identify strategies for supporting the CRN role and improving career development pathways.
Supplemental Material
sj-docx-1-jrn-10.1177_17449871261419727 – Supplemental material for Exploring the role and responsibilities, motivations, and career aspirations of clinical research nurses: a qualitative study
Supplemental material, sj-docx-1-jrn-10.1177_17449871261419727 for Exploring the role and responsibilities, motivations, and career aspirations of clinical research nurses: a qualitative study by Leah Hammond and Felicity Hasson in Journal of Research in Nursing
Footnotes
Acknowledgements
The authors would like to acknowledge the CRN community for their participation and support of this study.
Author contributions
Data availability statement
Anonymised data can be shared upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study has been ethically approved. We affirm that all participants involved have been provided with comprehensive information about the purpose and potential implications of the research. Consent was obtained from each participant.
Supplemental material
Supplemental material for this article is available online.