
Abstract
Background:
Globally, many children and young people (CYP) obtain insufficient good quality sleep. School nurses (SNs) are ideally-placed to support sleep health, but few studies have explored their practical experiences.
Aims:
To explore SNs’ experiences, perceived barriers and priorities (including training and resource requirements) in providing sleep-related support to CYP and their caregivers.
Method:
A convenience sample of eighteen SNs from the United Kingdom took part in two in-person focus groups (n = 8; n = 8) and one online focus group (n = 2) in June 2024. Qualitative data were inductively reflexively thematically analysed.
Results:
Seven themes were identified. Nurses reported that Sleep issues present as secondary concerns; and identified Perceived causes of delayed bedtimes and insufficient sleep. They faced barriers to practice including Challenges engaging families with sleep-supportive changes; Systemic barriers to successful delivery of sleep services and Challenges in identifying appropriate resources. To overcome such challenges, they emphasised School nurse training requirements; and The need for a trusted directory of resources.
Conclusions:
SNs in England regularly support families around sleep health but face significant challenges. To support their practice, policy changes recognising sleep as a public health priority and increased investment in staffing, training, and resources are needed.
Introduction
Sleep is essential for good physical and mental health. Globally around 20–25% of school-aged children and adolescents experience sleep problems (e.g. difficulties falling and/or staying asleep and early waking; Gradisar et al., 2011; Lewien et al., 2021; Liang et al., 2021; Newton et al., 2020). Insufficient sleep, particularly on school nights, has been identified in around half of adolescents globally (Evans-Whipp and Gasser, 2019; Gradisar et al., 2011). This is concerning because disturbed or insufficient sleep in school-aged children and young people (CYP) is associated with poorer physical, cognitive, and mental health functioning and outcomes, including obesity, impaired glucose metabolism, reduced memory and attention and depression, anxiety and behaviour problems (Chaput et al., 2016; Liu et al., 2024; Matricciani et al., 2019). CYP’s sleep disturbance can also affect their caregivers’ sleep, mood, and daytime functioning (Meltzer and Westin, 2011; Varma et al., 2020).
Sleep has been acknowledged as a global public health concern due to the high prevalence and serious consequences of insufficient and/or poor quality sleep (Chattu et al., 2018; Hafner et al., 2017; Lim et al., 2023). However, policy developments in the area have been limited in England and worldwide (Department of Health and Social Care, 2019; Lim et al., 2023). Sleep is not explicitly recognised as a public health priority in the same way as diet and physical activity. For example, in England, sleep management (apart from safer sleep) is not covered in universal Health and Wellbeing contacts for 0–19 year-olds (Office for Health Improvement and Disparities, 2023).
School nurses (SNs) have been proposed as ideally placed professionals to support improvement of sleep health in CYP and caregivers (Willgerodt and Kieckhefer, 2012). SNs work in schools in 102 countries globally to promote and support school-aged CYP’s health and well-being (Baltag and Saewyc, 2017). Internationally, their role includes promoting school health by supporting health literacy and health promotion, as well as individualised one-to-one assessment and interventions to support health and well-being (Pawils et al., 2023). Due to their skills related to both medical and psychosocial factors and their ability to engage with caregivers and families to support CYP health, SNs are well-positioned to provide sleep-promoting education, undertake sleep-related assessment, deliver individualised sleep-related support and generate referrals into other services as appropriate (Willgerodt and Kieckhefer, 2012). Involving caregivers is important as for CYP, sleep-promoting factors (e.g. sleep environment, sleep routines, diet and access to physical activity, and screens) are often in the control of caregivers, with more independence gained with age. However, SNs’ role in promoting and supporting CYP sleep health is largely overlooked (e.g. Pawils et al., 2023).
Limited evidence has explored SNs’ work around CYP sleep health internationally: in Denmark increased SN contact has been associated with reduced use of medication for sleep difficulties in CYP (Borup et al., 2010), an SN-delivered sleep intervention reported improved short-term CYP sleep outcomes in Australia (Hiscock et al., 2019), and CYP in Sweden reported that SNs are trusted sources of sleep support (Jakobsson et al., 2024). Previous qualitative research has reported that SNs in Sweden regularly support CYP around sleep, but face barriers to their practice including lack of motivation from students, unsupportive parents, and lack of clinical time and training around sleep (Hilli and Pedersen, 2021; Jakobsson, 2024). Internationally, it is known that many primary and secondary care providers lack knowledge, training and confidence around supporting and addressing sleep-related issues and topics (Honaker and Meltzer, 2016; Meaklim et al., 2020).
Recent international and United Kingdom (UK)-based calls for public health agendas to include sleep health promotion to advance population health (Department of Health and Social Care, 2019; Lim et al., 2023) have noted increasing challenges to young people’s sleep health (Illingworth, 2020). Whilst barriers to support are known in a Swedish SN context (Hilli and Pedersen, 2021; Jakobsson, 2024), it is currently unknown whether UK SNs support sleep health in CYP, if they face any challenges in doing so, and how service delivery could best be enhanced to improve sleep health in CYP. The extent to which a gap exists in UK school nursing practice in this area remains unclear due to the absence of current research on the topic.
As healthcare providers, including SNs, reportedly lack confidence and knowledge around sleep (Hilli and Pedersen, 2021; Honaker and Meltzer, 2016; Jakobsson, 2024; Meaklim et al., 2020), the Knowledge, Attitudes, and Practices (KAP) model was used to understand knowledge, attitudes and practices in this un-explored area including providing a useful framework for how these factors may be related. This theoretical model assumes that interaction of knowledge and attitudes influence behaviour (Andrade et al., 2020) and is widely used in healthcare research where there is a limited knowledge base.
The current study aimed to address three research questions:
What are SNs’ experiences of supporting CYP and their caregivers around sleep?
What barriers do SNs perceive to successfully supporting CYP and their families with sleep?
What do SNs perceive is needed to facilitate their work in supporting CYP and caregivers with their sleep?
Method
Study design
This was a cross-sectional exploratory, descriptive study using focus groups, which aimed to explore SNs’ experiences of supporting CYP sleep health and their perceived barriers to practice and needs for delivery of support around sleep.
This design was chosen as it allowed for an in-depth exploration of SNs’ knowledge, attitudes, perspectives and real-world experiences and is particularly valuable when there is limited existing evidence (Hunter et al., 2019). As the study aimed to generate initial information in an area with little pre-existing evidence around practice, the KAP model informed development of the focus groups topic guide (see Supplemental Material 1). For example, items 1, 2, 3 and 6 were designed to understand SNs’ current practice, items 4, 5 and 7 to explore how knowledge and attitudes may influence practice. An inductive, data-driven analytical approach was taken to prioritise participants’ experiences, given the limited evidence in this area. The KAP model was then again used to interpret results in the ‘Discussion’ section to identify strengths and potential barriers for service delivery.
COnsolidated criteria for REporting Qualitative research (COREQ) guidelines were followed (Tong et al., 2007; see Supplemental Material 2).
Study setting and recruitment
An opportunity sample of SNs was recruited which resulted in two face-to-face focus groups (FG1, n = 8; FG2, n = 8 participants) from a single NHS trust in the South East of England and one online focus group (FG3, n = 2 participants) from South East and South West England. To generate sufficient ‘information power’ (Malterud et al., 2016) to answer the research questions, it was determined that an online focus group would be held in addition to face-to-face focus groups to gather perspectives from more than one NHS Trust.
Three separate recruitment pathways were used in which participants were provided with a link containing study details, contact details for the research team for any questions, an online informed consent form and demographic questionnaire. The three pathways specifically were:
With permission from the team manager, SNs in one NHS trust were emailed an invitation to participate in face-to-face focus groups via their Trust e-mail list by a member of the research team who was an SN within that Trust.
SNs who had taken part in a related online survey study were invited to leave an email address if they were interested in participating in online, follow-up focus groups and were emailed directly (n = 4).
An online advert was shared by professional organisations including the Community Practitioners and Health Visitors’ Association (CPHVA), School and Public Health Nurses Association (SAPHNA) via social media and membership email lists. The research team also shared the advert via their social media and professional networks. Those who expressed interest in the online focus groups (n = 10) were emailed directly.
Participants received a complimentary lunch in thanks for taking part in face-to-face focus groups (carried out at Oxford Brookes University). No incentives were offered for taking part online.
Inclusion criteria
Inclusion criteria were being (1) aged 18 years old and above, (2) registered with the National Midwifery Council (NMC), (3) currently working as an SN (defined as being a nurse within a school nursing team or a student undertaking the Specialist Community Public Health Nurse [SCPHN] school nursing qualification)) in the United Kingdom and (4) having sufficient English language skills to take part in a focus group in English.
Measures
A topic guide was developed with open-ended, non-judgemental questions (see Supplemental Material 1) to create a comfortable environment where participants could express their views freely without fear of censure (Krueger and Casey, 2015). The topic guide was initially prepared by FT, GC, and LW and was then discussed with the wider research team (TH, JK, and RH). Research team members with school nursing expertise agreed that the topic guide was appropriate for capturing SNs’ professional experiences; thus, no piloting was deemed necessary. Minor adaptations were made to take account of findings from an online survey of SNs’ experiences of supporting CYP around sleep carried out by the authors, for example, SNs were asked if the commonly raised sleep topics identified from survey data reflected their own experiences. Topic guide questions explored SNs’ experiences such as which sleep topics were commonly raised with SNs and how these were raised, barriers SNs experienced in supporting CYP and caregivers around sleep, what SNs thought they needed to support their work around sleep and anything else they wished to raise about the topic.
Data collection
All focus groups (n = 3) took place in June 2024. Two face-to-face focus groups, each lasting 2 hours were conducted by FT and GC at Oxford Brookes University. The online focus group was conducted by GC and LW via Zoom and lasted for 1 hour.
Facilitators took field notes during the focus groups, which were later written up and uploaded to the research team’s shared Google drive. Focus groups were audio-recorded and later transcribed by FT. The online focus group was automatically transcribed by Zoom and FT checked the transcript for accuracy, amending as needed. Transcripts were then entered into NVivo software (Lumivero, version 14.0) for analysis.
Qualitative data analysis
Braun and Clarke’s six-stage reflexive thematic analysis process was used to analyse qualitative data (Braun and Clarke, 2006, 2019). This approach involves (1) familiarisation with the dataset, (2) coding of the data, (3) grouping codes into initial themes, (4) reviewing themes, (5) defining and naming themes and (6) writing up themes (Braun and Clarke, 2006). A semantic approach was taken, which reflected participants’ surface-level, rather than latent meanings. An inductive, data-driven approach was taken to prioritise participants’ meanings, meaning that no theoretical framework was used to inform data analysis.
FT carried out the data familiarisation phase by transcribing, reading and re-reading the focus group transcripts and field notes from the focus groups, then initially coded the transcripts with the three research questions in mind using NVivo 14 software. FT then grouped related codes for each of the research questions and identified initial themes pertaining to each question. Initial themes were extensively discussed with GC and LW as part of an iterative process of theme construction to ensure their coherence and relevance to the research questions. FT initially wrote up themes with illustrative participant quotations drawn from the three focus groups. Theme iterations were cross-referenced with transcripts and field notes from the three focus groups to prioritise participants’ views, rather than the researcher’s own interests. This was also an iterative process, with ongoing review and discussion between FT, GC and LW to further refine themes and theme names. Final themes were reviewed by TH, JK and RH, and minor amendments for clarity were made. Where required to make participants’ meanings clear, square brackets were used to insert relevant contextual information from the discussion, for example, adding ‘[CYP]’ where a participant referred to ‘they’. All results are the perceptions of participants and should be interpreted in this light.
Ethical considerations
Ethical approval was obtained from Oxford Brookes University Research Ethics Committee (241790). All participants gave their written informed consent to participate, and prior to focus groups commencing, participants were reminded of their rights and further verbal consent was taken.
Rigour and reflexivity
Researchers included a professor (LW), a research fellow (GC) and a post-doctoral research assistant (FT) who all hold doctorates in sleep-related research. Healthcare professionals (HCPs) on the research team were an SN practice assessor at Oxford Health NHS Trust with extensive experience of school nursing practice, teaching and assessing (TH) and two healthcare professionals, now practising academics, with extensive experience of school nursing teaching (JK, a Principal Lecturer in school nursing and RH, a lecturer in school nursing at Oxford Brookes University). The team members were all female and five were parents. There was a potential existing professional relationship between some members of the research team and some participants due to their role as practising SNs and involvement in school nursing education roles, however, it was not known to these team members whether particular individuals did or did not participate in focus groups. Participants knew the research team’s occupations, credentials and reasons for undertaking the research.
The team’s prior academic and professional experiences may have influenced data collection and analysis. For example, researchers with sleep expertise may have followed up participants’ comments related to key areas in the sleep research literature relating to CYP’s sleep or noticed known challenges to CYP’s sleep when analysing data. Researchers with public health and community nursing expertise may have been more likely to notice patterns relating to wider social determinants of sleep health and systemic barriers. To mitigate such influences as far as is possible and enhance rigour, inductive data analysis and extensive team discussion were undertaken with care to reflect the surface-level meanings of SNs’ words to prioritise their practical experiences of supporting CYP around sleep, closely following the principles of the reflexive thematic analysis (Braun and Clarke, 2006, 2019). Crystallisation took place throughout the analytical process (Tracy, 2010), with the variety of professional experiences within the team enhancing the range of interpretations and presentation of the data.
Results
Participant characteristics
A total of 18 SNs participated, representing ~2% of the qualified workforce in England (SAPHNA, 2024). All participating SNs were female, and all worked in state schools, with one additionally working in an alternative education provider. Seventeen were based in South-East and one in South-West England. The majority (n = 13) held the SCPHN qualification. Participants had been working as an SN for between 1 and 21 years (m = 6.11 years, SD = 5.47). See Table 1 for demographic and professional characteristics of participants.
Frequency and percentage of key sample demographic and professional characteristics.

For in person focus groups (FG1, n = 8; FG2, n = 8), 80% of those directly emailed participated. For the online focus group (FG3, n = 2), of ten SNs who expressed interest, two did not reply to emails, four did not join and two joined then left. Reasons for choosing not to participate are unknown.
Results from the focus groups
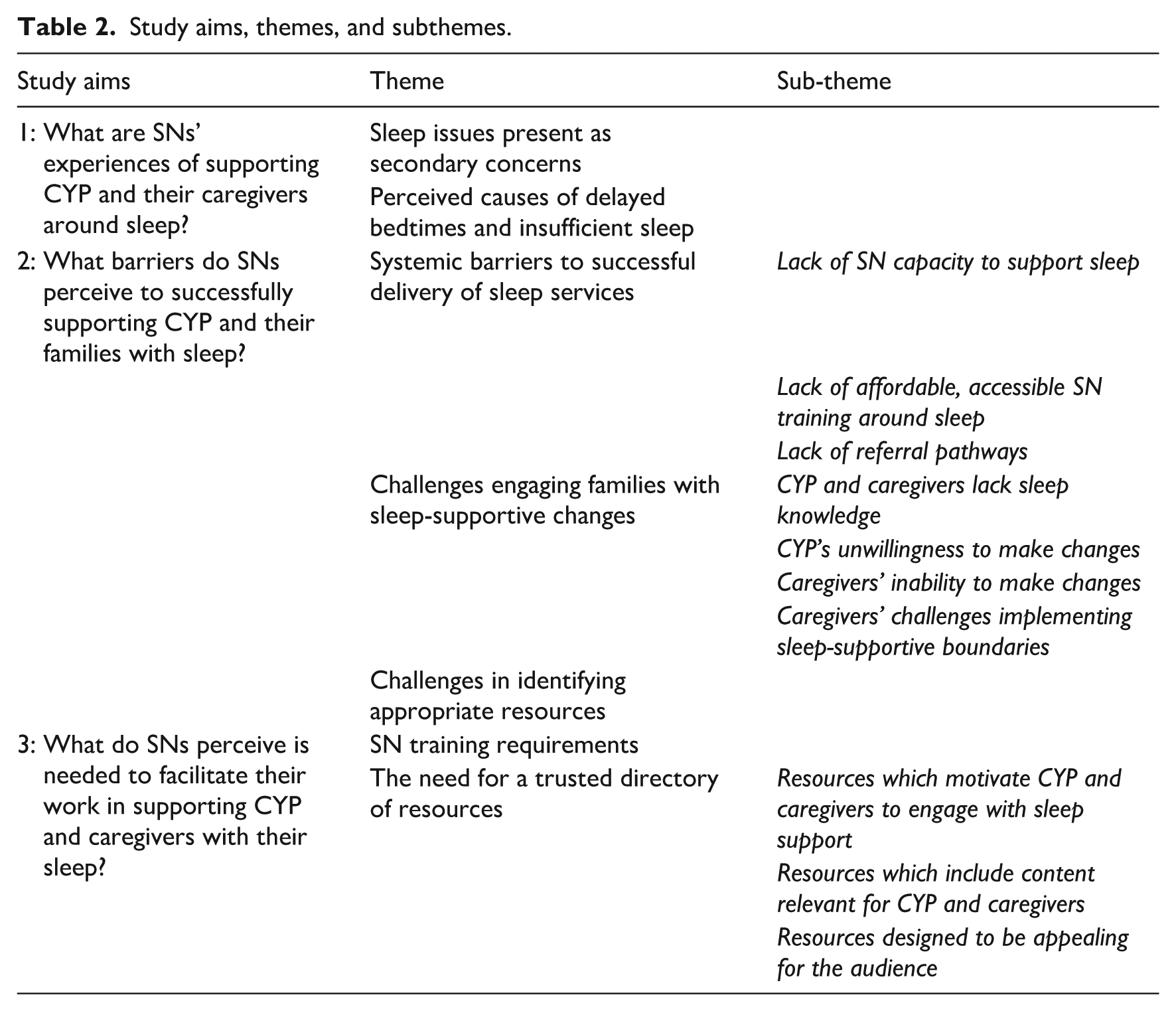
Results described the experiences of SNs in supporting CYP and caregivers around sleep in relation to the three study aims. A thematic map indicating relationships between themes is presented in Figure 1. Identified themes and sub-themes for each study aim are presented in Table 2.
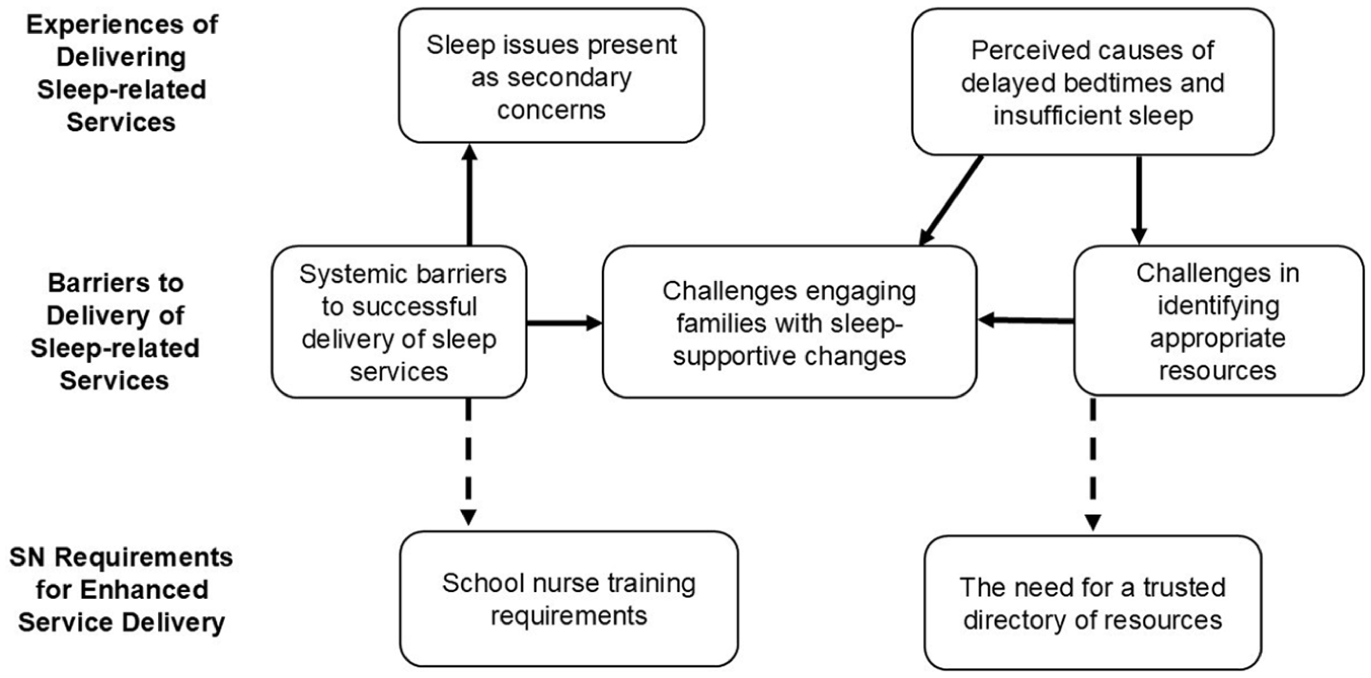
Thematic map illustrating relationships between themes*.
Study aims, themes, and subthemes.
What are SNs’ experiences of supporting CYP and their caregivers around sleep?
Sleep issues present as secondary concerns
Sleep issues were usually identified through holistic assessments when CYP were referred for wider issues recognised by educational professionals such as lack of attendance, falling asleep in school, or safeguarding: ‘The vast majority of my referrals seem to come from schools’. Parents of primary school-aged CYP typically sought advice for issues other than sleep, such as behaviour or emotional challenges, rather than sleep itself. SNs perceived that ‘there needs to be something going on for them to see sleep as an issue’. In secondary school-aged CYP, self-referral for mental health difficulties, such as anxiety, were common. SNs then uncovered sleep issues as they carried out comprehensive health assessments with CYP: ‘when you start asking questions, that will come up within the sleep [section of assessment]’. Referrals purely for sleep issues were relatively uncommon, but sleep problems often formed part of a wider picture of neglect, difficulties with school or poor mental health.
A key exception was that, where SNs were approached directly about sleep, this was typically in the context of coexisting concerns, such as neurodiversity or mental health problems: ‘that’s quite common . . . children with ADHD and they [parents] are really struggling with it, child not sleeping’. In such cases, CYP sleep was often raised due to the challenge it posed for caregivers’ own functioning and for CYP’s school attendance.
Perceived causes of delayed bedtimes and insufficient sleep
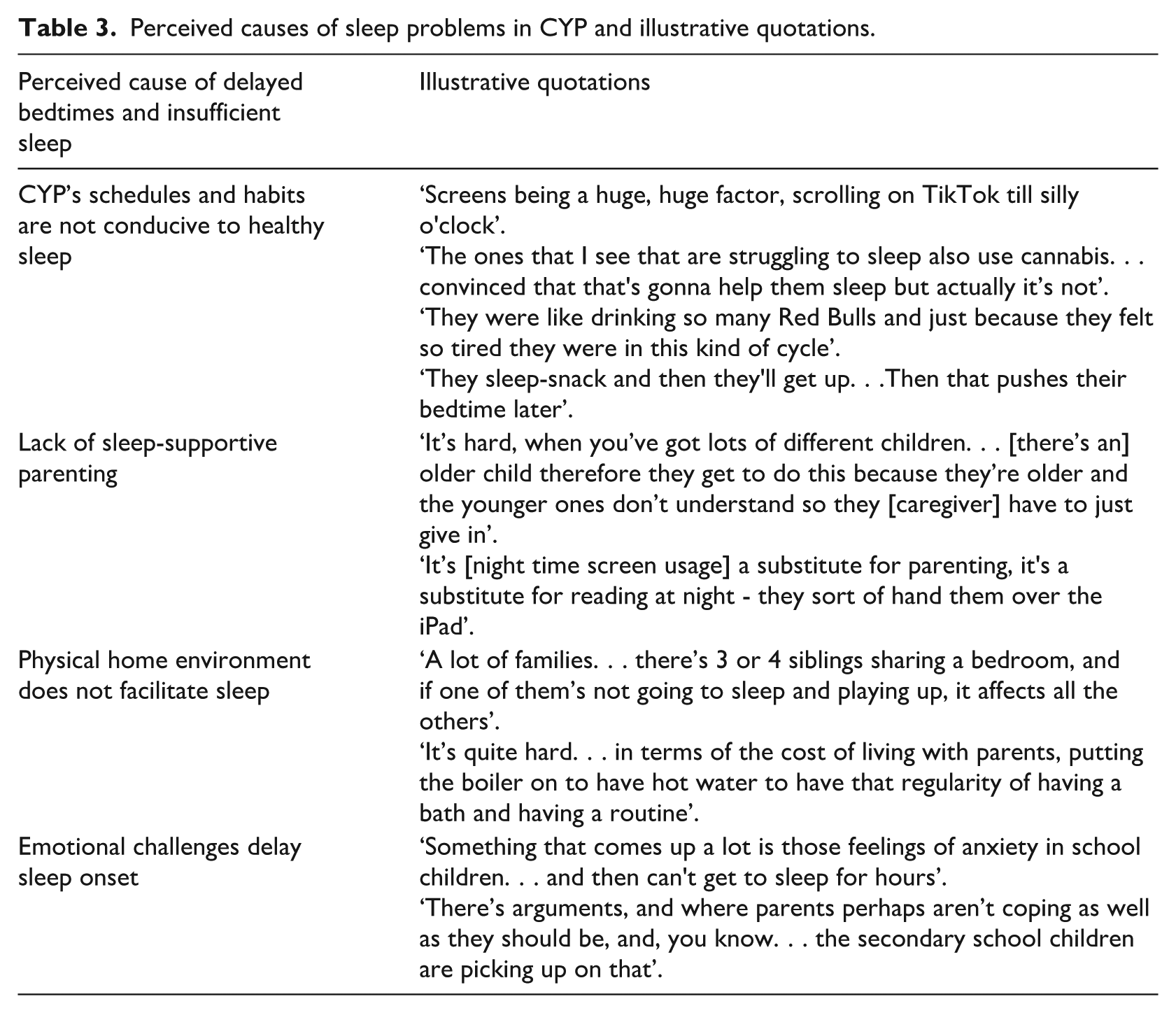
SNs identified that sleep problems in CYP were widespread, with delayed bedtime a common issue, which led to consequent insufficient sleep: ‘they’re so tired because they haven’t slept properly and they’ve gone to bed late’. They perceived four underlying causes of the delayed bedtimes and resulting insufficient sleep: CYP’s schedules and habits were often not conducive to sleep; parenting often did not support CYP sleep; some physical home environments made sleep difficult and emotional challenges kept some CYP awake. Illustrative quotations for these perceived causes are presented in Table 3.
Perceived causes of sleep problems in CYP and illustrative quotations.
What barriers do SNs perceive to successfully supporting CYP and their families with sleep?
Systemic barriers to successful delivery of sleep services
SNs identified a range of obstacles, some specific to their role and some related to the context in which they worked, ‘to be able to deliver everything to everybody’ in relation to sleep. Four main challenges impacted SNs’ capacity to support CYP’s sleep: Lack of capacity; lack of affordable, accessible training, lack of referral pathways and challenges in identifying appropriate resources to use in their clinical practice.
Lack of SN capacity to support sleep
SNs highlighted their own lack of time and capacity to ‘do our job properly on a public health aspect’. SNs were enthusiastic about undertaking public health work such as identifying key sleep-related concerns in the schools they worked with and delivering education according to needs. They felt that, although part of their role, such work was crowded out by competing priorities. In particular, safeguarding caseloads were extensive and took priority. SNs also identified that to achieve behaviour change, individual CYP often needed longer-term support than they were able to provide: ‘you need to be constantly in there for at least 6 weeks . . . but sometimes find that you’re not able to with the Caseload that you hold’. For some, service organisational considerations, such as not being attached to specific schools were also a challenge to carrying out sleep-related public health education.
Lack of affordable, accessible SN training around sleep
SNs reported that accessing training around sleep to support their own practice was challenging. Where training was available, it was prohibitively expensive for SNs to attend: ‘it's being able to access appropriate training and appropriate price and things like that’. This meant that SNs lacked current, up-to-date training opportunities, with one nurse who had experienced helpful training stating that it was 10 years ago.
Lack of referral pathways
SNs perceived a lack of onward referral pathways for those who required additional assessment and/or sleep support. Some SNs expressed lack of knowledge of specialist sleep service referral pathways: ‘I think what would be really useful is to understand what services we have for sleep’. Those who had utilised such pathways reported limited success: ‘I’ve managed to get two referrals accepted in like four years’. The lack of referral pathways was particularly challenging for families of potentially neurodiverse CYP, for whom referrals to Child and Adult Mental Health Services for diagnosis could take years.
Challenges engaging families with sleep-supportive changes
SNs found that giving information about changes to sleep was often insufficient to address the sleep problems they identified in CYP, as CYP and caregivers struggled to implement the advice. Engaging CYP with sleep advice and interventions could be challenging; nonetheless, their engagement was seen as crucial to the behaviour change necessary to improve their sleep: ‘you have to get the student on board with what you're doing, because otherwise. . . they’re just not gonna do it’. Similarly, it was often difficult to engage caregivers with implementing advice: ‘They'll ask for the help, and then you give them help and they actually don’t want to put in the work’. SNs expressed mixed views around the need to involve caregivers to improve CYP sleep. Many felt that the motivation of CYP was the determining factor in successful practice; however, some felt that involving caregivers led to the most successful outcomes for CYP.
Four subthemes identified challenges in securing CYP and caregivers’ engagement: CYP and caregivers’ lack of sleep knowledge; CYP’s unwillingness to make changes; caregivers’ lack of capacity for change and caregivers’ difficulties implementing sleep-supportive boundaries.
CYP and caregivers lack sleep knowledge
A primary difficulty was CYP and caregivers’ lack of knowledge about the importance of healthy sleep, which negatively impacted motivation to engage with sleep advice: ‘I think the main barrier is they don’t recognise the benefits of improving sleep: it’s not necessarily a priority for them’. CYP and caregivers often lacked knowledge of impacts of sleep on areas such as mental and physical health, as well as academic performance.
Inadequate knowledge also meant that sleep problems were not always recognised: ‘it doesn’t really occur to them [CYP] that, you know, what’s happening for them with sleep is anything unusual or not – how it should be or could be improved’. The appropriate amounts of sleep needed at different ages were not widely known by caregivers: ‘there’s a lack of understanding [in] parents of how much the younger secondary school age children, even primary age, how much they need’. This meant that CYP and caregivers were often unaware that CYP were experiencing insufficient or poor quality sleep, or that their sleep habits were not conducive to healthy sleep.
Two key factors were perceived as contributing to inadequate sleep knowledge for caregivers and CYP. Firstly, lack of early years sleep information and support through health visitors and children’s centres meant that SNs had to ‘go in at crisis’ once CYP’s sleep had become in many cases established and problematic. Secondly, a lack of curriculum time and focus on other public health issues, for example, healthy diet, meant that sleep education was not prioritised in schools.
CYP’s unwillingness to make changes
SNs often found that CYP were reluctant to make necessary changes to sleep schedules and habits to improve their sleep: ‘they won’t get into a routine. . . ‘they’re like “well, I don’t want to give up my phone. I want to watch YouTube, I want to chat to my friends”’. Social pressure to be online and addictive behaviours around gaming were often more attractive to CYP than sleeping, which meant SNs could find it difficult to motivate them to introduce healthier sleep habits.
In addition to specific advice being unpalatable, the long-term effort required to resolve sleep issues could contribute to CYP’s unwillingness to make sustained changes: ‘they just want that quick fix, that magic wand’. If CYP had already attempted to implement some sleep strategies, but without the required behavioural consistency for success, the failure of any attempt resulted in them being: ‘quite negative. . . they say “I’ve tried everything and it doesn’t work”’.
Caregivers’ inability to make changes
SNs also perceived that some caregivers were unable to introduce sleep-supportive behaviours: ‘parents haven’t got the capacity to make changes’. This was particularly perceived in families with multiple CYP, where caregivers could feel ‘outnumbered’ and ‘defeated before they start’. SNs identified that where children had health conditions and/or additional needs, sleep could be a low priority for caregivers, despite its potential to bring positive changes to the family environment.
Working outside the home could also make implementing new habits challenging, or impossible, due to emotional and practical impacts of long hours on families. Employment alongside childcare responsibilities could mean caregivers had little time or energy: ‘If they’re working and they’ve got to come home, cook supper. . . settle the child, do the dishes, give the child their time and then settle them - You know they’re tired’. Work schedules were also perceived to impact upon familial sleep as they could make ‘age-appropriate bedtimes’ difficult to achieve when caregivers returned home late.
Caregivers’ challenges implementing sleep-supportive boundaries
Parenting could be a barrier to improving CYP’s sleep as some caregivers were not perceived to be sufficiently authoritative to implement appropriate changes: ‘A lot of local families don’t have that kind of parental relationship with their children where “I’m in charge”. . . where their phone goes in the kitchen at 8 and it’s not negotiable’. Caregivers avoided implementing new routines or habits due to fear of ‘caus[ing] World War 3’, such as where CYP had always been allowed unrestricted access to electronic devices, or where bedtimes had been too late.
Some SNs perceived that parents faced difficulties in implementing or maintaining appropriate routines as CYP grew older. Around the transition from primary to secondary school, many caregivers felt they should be withdrawing their input into their child’s behaviour: ‘because they’re [CYP] going to school by themselves. . .they [caregivers] naturally progress to “They’re more independent”’. SNs perceived that caregivers lacked guidance at this important stage about the importance of maintaining healthy sleep habits in their CYP.
Challenges in identifying appropriate resources
A lack of standardised, suitable and free-to-access resources was a key problem. Some SNs had identified some resources, but others had not, and some had created their own: ‘Everyone uses different resources as professionals. We all use different things because we make it up’. The need to find their own materials combined with the lack of SN time and capacity was challenging. The sheer number of, for example, sleep-related apps made it difficult for SNs to find time to assess whether they were ‘evidence-based. . .nothing dodgy about it’. This meant that some felt: ‘there’s not enough there that I can recommend’. A lack of materials for universal sleep education, particularly for primary-aged CYP, was also perceived.
What do SNs perceive is needed to facilitate their work in supporting CYP and caregivers with their sleep?
SN training requirements
As previously noted, the lack of SN training around sleep was a barrier to SN practice. SNs highlighted the need for accessible training for themselves around sleep: ‘I think definitely, more training needs to be more available’. Such training needed to be up-to-date and cost-effective.
The need for a trusted directory of resources
SNs additionally wanted a trusted directory to access resources they could use in practice: ‘a national place where you could get resources’. Such a directory should include reviews of websites apps for sleep, to ensure they were evidence-based and safe for children, for example, did not contain chat features or any inappropriate content.
SNs additionally perceived that development of resources was needed, which both delivered relevant information and included tools and strategies to help motivate CYP and caregivers. The design of these resources needed to address three key areas: Resources which motivate CYP and caregivers to engage with sleep support, Resources which include content relevant for CYP and caregivers and Resources designed to be appealing for the audience.
Resources which motivate CYP and caregivers to engage with sleep support
Relevant information should inform CYP and caregivers about the potential long-term benefits of healthy sleep, particularly benefits for emotional health: ‘how much of an impact sleep . . . diet and exercise play in the mental health because actually a lot of what we see is mental health and parents at secondary and primary are reaching in about that’. Simple explanations of underlying biological mechanisms linking sleep and mental health were thought to be needed.
Features which supported behaviour change and motivated sustained engagement with sleep-supportive changes were also thought to be important. SNs reported that reflecting back CYP’s success over time helped to motivate their sleep-related behaviour changes: ‘it’s identifying the changes and the progress that has been made and making them feel good about that’. SNs also felt that identifying short-term benefits and rewards was important for engagement of both CYP and caregivers.
Resources which include content relevant for CYP and caregivers
Having appropriate informational content of resources was seen as crucial for educating CYP and caregivers, but SNs emphasised that it should also be developmentally relevant so that it resonated for them. Content should include expectations on ‘sleep needs across ages’ and advice at key developmental stages, particularly the transition to secondary school.
When considering sleep management strategies, SNs described the importance of providing choice, with the preferred approach being an ‘evidence-based, age-appropriate list of possibilities’. This could be personalised and made relevant to individual CYP and families: ‘we give them the generic advice. . . But okay, what would that look like for you?’. The ability to tailor and personalise advice was thought to be a key component of successfully supporting behaviour change.
Resources designed to be appealing for the audience
Resources needed to be supportive, practical, realistic, and flexible to appeal to CYP and caregivers. How material was packaged and delivered was seen as crucial to foster engagement, for example, a non-judgemental tone: ‘If you’re coming across as being judgy, there’s no point doing it’. SNs thought that including real-life accounts of successfully implementing sleep advice from other caregivers would be beneficial. Resources also needed to be available on demand to be attractive to busy caregivers whenever they had time to access.
In particular, SNs thought caregiver resources needed to be succinct, and for primary-aged CYP, information delivery should be fun: ‘stories. . . singing. . . pictures. . . cartoons’. For secondary-aged CYP, teenagers’ preferred ways of accessing information should be considered: ‘like WhatsApp. . . Instagram. . . TikTok. . . having maybe information on there that is educational’. For older adolescents, marketing was perceived as important, with consideration of factors such as celebrities, influencers and key messages to appeal to key concerns of the age group.
Discussion
This study aimed to explore UK SNs’ experiences, barriers to supporting CYP, and to identify any gaps in their needs when delivering sleep-related support. SNs frequently identified sleep issues in CYP, both as a result of broad screening assessments and also when addressing other specific concerns and regularly supported CYP and their caregivers with improving CYP sleep health. They perceived a range of causes to the delayed bedtimes and consequent insufficient sleep which they regularly saw. Barriers to improving sleep health in CYP were challenges engaging CYP and caregivers with sleep-supportive behaviour changes, systemic barriers to service delivery including lack of SN training and capacity, policy neglect of sleep, and a lack of appropriate resources to use in practice. SNs identified two key priorities for enhanced service delivery: training around sleep for themselves and development of appropriate resources, which engaged and motivated families with behaviour change, as well as providing information.
The KAP model offers a useful framework to understand knowledge, attitudes and practices in this previously unaddressed area, including how these domains may impact upon one another and identification of strengths and priorities for service improvement.
Knowledge
All SNs showed knowledge of links between sleep and wider issues of mental health and behavioural concerns. They recognised inter-related challenges to CYP’s sleep health due to biological changes, inappropriate schedules, lack of sleep-supportive parenting, challenges in the home environment, and emotional difficulties. They knew that behaviour change required motivation, achievable goals, and focus on positive progress. SNs also understood the multiple challenges families faced in improving CYP sleep health, and the need for sustained and motivating interventions, as well as broader sleep-related education.
However, SNs widely lacked comprehensive training around sleep biology and approaches to managing sleep problems. Training opportunities were scarce, outdated, and often prohibitively expensive. They also lacked knowledge of referral pathways for sleep disorders and appropriate resources to recommend in practice.
Attitudes
SNs perceived that improving sleep health in CYP was an important part of their wider public health role. However, they expressed frustration around lack of capacity and policy gaps, which were perceived as contributing to challenges in delivering effective services. They also emphasised the need for engaging, personalised and non-judgemental support, and empathised with challenges families faced.
SNs held mixed attitudes about their ability to support CYP sleep health. Some felt they were knowledgeable about sleep and were able to motivate and engage families. However, others felt this was difficult as they lacked knowledge, behaviours were often entrenched and sleep was a low priority for families, only considered when linked to concerns such as mental health or behaviour. Attitudes towards involving caregivers with supporting sleep in secondary-school aged CYP were also mixed. Some perceived caregiver involvement as crucial to implementing and sustaining change, whereas others thought that motivation of CYP alone was required for success.
Practice
SNs often identified sleep issues when conducting assessments related to wider issues. They provided tailored advice and worked individually with CYP, using strategies like progress tracking and short-term rewards to motivate behaviour change over time.
However, SNs faced major barriers to their practice, including their own lack of capacity and lack of training and therefore knowledge around sleep, unclear and limited onward referral pathways, and systemic underinvestment in CYP sleep health. Sleep issues were often entrenched by the point of intervention, due to lack of early sleep support for families, meaning caregivers struggled to introduce recommended changes and CYP were reluctant to change habits. Identifying and validating appropriate resources to support behaviour change was also difficult. Available resources often lacked standardisation, evidence base, and age-appropriate design. Consequently, some SNs created their own resources, which was inconsistent and time-consuming.
Priorities for service delivery
The present research supports the notion that SNs are ideally placed professionals to support CYP sleep health (Willgerodt and Kieckhefer, 2012). SNs in England, as in Sweden, reported regularly providing practical and tailored advice around sleep to CYP and families (Borup et al., 2010; Hilli and Pedersen, 2021; Jakobsson, 2024). Improving CYP sleep health likely requires multi-stakeholder approaches with understanding of population-specific sleep challenges and barriers to intervention success, followed by appropriate tailoring of interventions, as educational interventions alone have not shown efficacy (Gaskin et al., 2024; Gruber, 2017). The present findings indicate that SNs already work in this way as part of their current role are motivated to promote and support CYP sleep health and can bring detailed insight into sleep challenges within school-specific populations. However, key priorities for enhancing service delivery emerge from the present findings.
Firstly, introducing screening for sleep problems could be a way of providing targeted support to those CYP most at risk (Hiscock et al., 2019). SNs reported that they often identified sleep issues in CYP as part of a wider picture of concerns for CYP, families and schools such as school non-attendance and behavioural, emotional, and mental health difficulties, all of which have previously been associated with sleep problems in CYP (Cook et al., 2021; Lollies et al., 2022; Van Veen et al., 2021). This is concerning and suggests that sleep problems, even if present, may not be a key presenting complaint and some sleep difficulties could be being overlooked. As a modifiable target, improving sleep can potentially have great benefits for CYP and families, as well as helping to address the societal and public health challenges associated with CYP sleep difficulties (Hafner et al., 2017). To deliver such services, given the scale of CYP sleep health challenges, greater recognition, development, and resourcing of SNs’ important role in supporting CYP sleep health is needed.
Secondly, SNs require sleep-related training and resources to support their work. SNs’ reported lack of sufficient and up-to-date training around sleep appeared to lead to inconsistent provision around sleep for CYP and families. Lack of training around sleep is a challenge for healthcare professionals internationally, including SNs (Honaker and Meltzer, 2016; Jakobsson 2024; Meaklim et al., 2020). In the present research, SNs reported the need for training on biological mechanisms underpinning sleep and approaches to managing behavioural sleep problems, including the underlying principles of treatment. To identify possible further training gaps, an audit of the sleep content of nursing curricula would be helpful. SNs also emphasised their need for access to resources which support the motivation and engagement of CYP and caregivers with sleep-supportive changes. International studies have broadly demonstrated that information alone does not lead to behaviour change around CYP sleep (Gaskin et al., 2024; Gruber, 2017), and engaging caregivers and CYP can be challenging (Jakobsson, 2024). Although there are many excellent informational resources on CYP sleep health available worldwide, the present study highlights the need for development of resources which are evidence-based yet also motivate and engage CYP and caregivers with behaviour change.
Thirdly, sleep health should be recognised as a public health priority. SNs reported considerable challenges around supporting CYP sleep, exacerbated by underinvestment in the public health nursing workforce and failure to include sleep health as a priority in public health agendas. Compounding this, SNs in England lacked time for the sustained individual interventions needed to improve CYP sleep health, and in-school sleep education was often unfeasible due to limited capacity and curricula prioritising other public health agendas. Present findings in the United Kingdom align with reports that lack of SN capacity impairs sleep service delivery in Sweden and Australia (Hilli and Pederson, 2021; Hiscock et al., 2019; Jakobsson, 2024). The present research also illustrates how policy neglect exacerbates capacity issues by permitting sleep issues in CYP to become entrenched, consequently requiring greater resources to address. Potential implications of SNs’ frustration for workforce morale and retention are further reasons to address policy-related barriers to service delivery.
Despite acknowledgement of the importance of sleep for public health, policy developments in the area have been limited in England and worldwide (Department of Health and Social Care, 2019; Lim et al., 2023). To improve sleep health and its associated physical and mental health and developmental outcomes, introduction of targeted public health and education programmes are needed globally (Lim et al., 2023). With greater numbers and training, SNs may be an ideally placed workforce to deliver such policies. Globally, however, numbers of SNs are insufficient, and their numbers are currently in decline in the United Kingdom (Maughan and Baltag, 2024; SAPHNA, 2024). Workforce investment and inclusion of sleep in public health agendas are therefore needed so that SNs have the time, resources and mandate needed to appropriately support CYP.
Strengths and limitations
To our knowledge, this is the first qualitative study to examine SNs’ experiences in England of supporting sleep and the first internationally to explore what SNs need to better assist CYP and caregivers.
As a semantic qualitative study, findings reflect participants’ perceptions alone. A strength of the small sample was the ability to capture detailed insights, including policy-related challenges. A limitation was that most participants were from one NHS Trust in the South of England, meaning that experiences may not reflect those of SNs elsewhere in the United Kingdom. This focus, however, clarified that variability in practice resulted from differences in training and resources rather than organisational factors. Furthermore, only female SNs participated and, while sleep challenges of both boys and girls were discussed, discussion of parenting focused on mothers’ roles and did not consider fathers’ experiences. Future research including male SNs could shed further light on any gendered dimensions of supporting sleep health in CYP.
The use of an opportunity sample may mean participants were more interested and knowledgeable about sleep than other SN colleagues, as was evident in the online focus group. Larger face-to-face groups enabled discussion of diverse knowledge and attitudes, whereas participants in the smaller online group offered deeper reflection on their own and their colleagues’ experiences. Despite differences in group size and dynamics, experiences around supporting sleep were strikingly similar. Notably, findings also align with and extend previous reports of Swedish SNs’ experiences (Jakobsson, 2024) and likely have applicability to international contexts.
Conclusion
This is the first UK-based qualitative study to explore SNs’ experiences with sleep health in CYP. SNs in England regularly support CYP and their caregivers around sleep health; however, they face numerous barriers in doing so. SNs’ unique role as school-based healthcare professionals make them the ideal workforce to support the improvement of CYP sleep health through tailored, multi-stakeholder approaches. Changes to health and education policies, which acknowledge that sleep is a global public health priority, are urgently required to support SNs in improving CYP sleep health. To better support their clinical practice, increased investment in numbers as well as training and resourcing of SNs around sleep are needed.
Key points for policy, practice and/or research
SNs may be an underutilised workforce in addressing the global public health challenge of sleep health in CYP. They regularly explore complex aetiologies of sleep problems and promote behaviour change through personalised plans and liaison with schools and caregivers, but face systemic barriers to their practice.
SNs hold positive attitudes towards increasing their public health role in promoting sleep health with CYP, their caregivers and in schools. This important aspect of their role requires greater recognition and resourcing.
To best support CYP sleep health, SNs require greater training around sleep and access to evidence-based resources, which motivate and engage CYP and caregivers in sleep-supporting behaviour changes. Future research should audit sleep-related content of nursing curricula and identify key areas for introduction/development.
Co-production with CYP, caregivers, and SNs is needed to develop an evidence-based suite of engaging resources which support improvement of CYP sleep health.
Global public health agendas should acknowledge the need to address CYP sleep health with targeted support and education, particularly in early years and primary schools.
Supplemental Material
sj-xlsx-1-jrn-10.1177_17449871251410567 – Supplemental material for School nurses’ experiences of supporting children and young people and their caregivers around sleep: a focus group study
Supplemental material, sj-xlsx-1-jrn-10.1177_17449871251410567 for School nurses’ experiences of supporting children and young people and their caregivers around sleep: a focus group study by Fiona Tierney, Luci Wiggs, Tikki Harrold, Rachel Hobin, Jennifer Kirman and Georgia Cook in Journal of Research in Nursing
Supplemental Material
sj-xlsx-2-jrn-10.1177_17449871251410567 – Supplemental material for School nurses’ experiences of supporting children and young people and their caregivers around sleep: a focus group study
Supplemental material, sj-xlsx-2-jrn-10.1177_17449871251410567 for School nurses’ experiences of supporting children and young people and their caregivers around sleep: a focus group study by Fiona Tierney, Luci Wiggs, Tikki Harrold, Rachel Hobin, Jennifer Kirman and Georgia Cook in Journal of Research in Nursing
Footnotes
Acknowledgements
The authors would like to thank the SNs who kindly gave their time and shared their professional experiences and opinions as part of this study.
Author contributions
Data availability statement
The data for this study are available in Arkivum for collaborative research purposes, as part of the research team at Oxford Brookes University, upon request from the Associate Dean of Research and Knowledge Exchange (Oxford Brookes University).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted as part of an Oxford Brookes University Faculty of Health and Life Sciences pump priming pilot research award.
Ethical approval
Ethical approval was obtained from Oxford Brookes University Research Ethics Committee (241790) on 29 April 2025.
Consent to participate
Participants individually gave informed consent via an online survey to participate in focus groups. Further verbal informed consent was obtained from each individual immediately prior to focus groups commencing.
Consent for publication
Participants individually gave informed consent via an online survey for their words to be used in publications. Further verbal informed consent was obtained from each individual immediately prior to focus groups commencing.
Supplemental material
Supplemental material for this article is available online.