
Abstract
Background:
The Clinical School Model connects professorial staff from the university directly to practitioners in the National Health Service to promote evidence informed practice and develop clinical academic careers. These are promoted widely, but strategic adoption into organisational culture and workforce plans are challenging to overcome.
Aims:
To describe the development of the Clinical School Model in Cornwall and explore how it generates impact through staff engagement activities to support clinical academic career pathways. Structure, process and outcomes developments over the last 3-years are reported.
Methods:
Donabedian’s framework (structure, process and outcome) was used to report on the development and impact of the Clinical School Model.
Results:
Structural and process activities are reported, illustrating strong foundations to embed clinical academic career pathway opportunities. In the absence of empirical reporting standards for such developments, quantitative and qualitative outcomes are reported against the Clinical School’s 5-year strategic plan.
Conclusions:
This paper responds to the lack of reported evidence on developing organisational infrastructure to address the clinical academics aspirations of nurses and their employers. This important contribution leads a call for more organisations to report to the evidence base, enabling shared learning and shaping future research.
Keywords
Introduction
England’s National Health Service (NHS) aspires to the highest standards of excellence and through it’s Constitution, commits to conduct and use research to improve the health and care of its population (Department of Health and Social Care, 2021). Organisations that have deliberately integrated research into organisational structures demonstrate improved healthcare performance (Boaz et al., 2015). England’s Chief Nursing Officer (CNO) launched a guide for Chief Nurses to lead acceleration of evidence into practice and research activity in NHS Trusts (NHS England and NHS Improvement, 2020), together with a strategic plan for research (NHS England and NHS Improvement, 2021). This plan sets out five key themes: aligning nurse-led research with public need, releasing nurses’ research potential, building the best research system, developing future nurse leaders of research and digitally enabled nurse-led research (NHS England and NHS Improvement, 2021). The ‘building the best research system’ theme acknowledges national variability in opportunities for nurses and strategically calls for a ‘cohesive system’ to be built to underpin the plan – an equitable infrastructure at national and regional level for nurses to lead and deliver cutting edge research and the adopt research findings into practice.
One tangible infrastructure enabler is the National Institute for Health and Care Research’s (NIHR) Integrated Clinical Academic Programme. Integrated Clinical Academics (ICAs) refer to non-medical health and social care professionals who develop their career to combine clinical research and doctoral-level research leadership with continued practice and professional development (National Institute for Health Research, 2021); however, opportunity and outcomes remain variable. Challenges faced by ICAs are articulated by Gibson (2019); these are especially difficult when competing clinical expertise disadvantages the individual if directly compared to solely academic colleagues and institutional research impact matrices (quantity of grants and peer-reviewed publications). Disadvantage is also recognised in the NIHR’s own 10-year review of their national clinical academic training programme. Despite an overall rise in trainees and their success over this period, it highlights ‘a particular concern’ over the low number and success rates for nurses across their academic clinical fellowship programmes, seeing research engagement as the barrier (National Institute for Health Research, 2017: 11). Olive et al. (2020) respond citing reported success in promoting clinical internships that engage nurses in research through improvement science skills as a means to redress this imbalance.
Models of clinical academic development
There has been an explosion in reference to clinical academics in papers relating to nurses, midwives and allied health professions (NMAHPs) in the last 5 years. These focus on specific elements of clinical academic career developments: research culture of organisations (Luckson et al., 2018), clinical academic internships (Di Bona et al., 2019), exploration of success factors (Olive et al., 2020), impact of research internships (Long, 2019; Oostveen et al., 2017), organisational research culture (Cowley et al., 2020; Nightingale et al., 2020), clinical academic career progression (Avery et al., 2021; Trusson et al., 2019) and practically addressing post-doctoral needs of clinical academics (Hampshaw et al., 2022; Orton et al., 2022; Sanders et al., 2020).
Strickland (2017) reported on a literature review to identify research infrastructure to support clinical academics with visits to leading clinical academic programmes worldwide. In the United States, one hospital, integrated with a university dedicated nursing research centre, led by doctoral prepared nurses that supported and mentored sponsored research fellows in applied practice-based research. They conducted regular ‘nursing grand rounds’ and had protected time to undertake and publish research. Strickland (2017) also reported on two United Kingdom examples, in Southampton and Oxford. Both saw university and NHS collaborations in place supporting clinical academic developments and grant writing support, and both models were facilitated by joint professorial appointments. Two useful case studies are presented in the CNOs guide to Chief Nurses (NHS England and NHS Improvement, 2020). The first is a Centre for NMAHP Research, hosted within an NIHR Biomedical Research Centre. This strives to foster a culture in which interested NMAHPs can apply research evidence into practice through a series of funded internships and production of an in-house journal that reports this impact, all funded through the hospital’s charity. The second example is where nursing and midwifery evidence-based practice is promoted via a shared-governance model; a model of de-centralised leadership through local decision-making councils. Here, improvement activity is encouraged through evidence-informed decision-making, stimulating research interest and activity. However, neither of these two examples present outcome or impact data, factors that are often poorly reported. There is evidence from one collaborative model between a university and its NHS partners that reports impact on delivering capacity and success in ICA awards (Westwood et al., 2018). They describe their regional Clinical Academic Partnership Model, focused on providing access to clinical academic pathway opportunities from master’s level to post-doctoral awards. They promote practice relevant research topics, harness strategic and funding capacity to co-ordinate partnership activities such as providing shared facilities, a skills training programme and mentoring capacity. They also facilitate work to translate findings to improve healthcare outcomes through leadership skill development and training. In 10 years, they attribute 74 professionals completing master-level study, five doctoral and eight at post-doctoral level study to the implementation of the model.
Responding to limited evidence on clinical academic service delivery models and infrastructure to support national research strategy delivery, this paper aims to present the Clinical School Model as a newly evaluated case study. A service evaluation framework is used to support others reporting future models. The paper describes the development of the Clinical School Model and explores how its infrastructure generates impact through staff engagement activities to support clinical academic career pathways. Structure, process and outcomes developments over 3 years are reported to evaluate and critique this model.
Methodology
Donabedian’s framework (structure, process and outcome; Ayanian and Markel, 2016; Donabedian, 2005) is used to report the development of the Cornwall Clinical School Model and to consider its impact and opportunities for the future. Donabedian (2005) stated that reporting outcome is the ultimate validator of the intervention or initiative, however, warned that it does not give insight to the valuable attributes (positive and negative) of how the outcome is achieved. To address this, an examination of the process is introduced leading to the outcome and the antecedent to process – structure.
Cornwall’s Clinical School’s development has been locally documented and reported to oversight groups. These reports reference and evidence the description of structure, process and outcome framework. Donabedian (2005) recognised such records as important source documents, but highlighted limitations in their use, such as incompleteness and inaccuracy (bias in original reporting) being inevitable, and a threat to reliability. To counter this problem, an independent judge (Donabedian, 2005) was included on the reporting team to independently evaluate the accuracy of statements being made PR.
The reporting period goes back to the Clinical School’s inception in 2014; however, impact for this case study focuses on the last 3-year activity – 2020 to 2022. Key papers, for example initiation and strategy documents, development reports, annual reports and minutes of leadership group meetings, had all been previously presented to the NHS organisation’s professional strategic leadership group, some received further approval by hospital sub-Trust Board groups.
Reporting is in line with Standards for Quality Improvement Reporting Excellence (SQUIRE 2.0) guidelines for reporting new knowledge about how to improve healthcare (Ogrinc et al., 2016).
Results
Introduced to the South West of England from developments started in the Australia by two Clinical Academic Professors, the Clinical School Model brings professorial academic staff from the university closer to NHS practitioners. This direct connection to nurses in practice aims to break down barriers between academic theory and research, and practice reality. The universal aim of the Clinical School is to promote the adoption of evidence informed practice and to develop clinical academic career opportunities. The Clinical School described here is one of five in the region that were established from 2014, all connected to the same University but all with slightly different structural-level arrangements between local NHS partners. The Clinical School in Cornwall is a collaboration between two NHS trusts, an acute and specialist healthcare provider and a mental health and community trust, and with a university’s School of Nursing and Midwifery, reaching over 5000 NMAHPs.
Results from data analysis are presented under the three Donabedian headings: structure, process and outcome.
Structure
Structures were formed when the initiative first started and have been under regular annual revision. The core collaboration between the university and the trusts secured dedicated time of two senior colleagues; a clinically focused university professor and an nursing associate director in the NHS trust. These co-directors formed an essential structural partnership, with strong leadership support from their respective organisations. This partnership team of two influenced the organisational reporting structures between the Clinical School and the trust’s CNO and regional co-ordinating group. A Clinical School Leadership Group reports monthly into the CNOs Clinical Cabinet. This provides strategic opportunities to promote the Clinical School’s presence and performance and is a forum used to foster engagement and acquire support for future developments. Reports are discussed and approved through this structure for organisational dissemination and adoption and can pass upward to Trust Board.
Key structural collaborations have been developed and enhanced over the past 3 years, including: local health library; local and regional research and development teams; local education and training teams; local clinical effectiveness, audit and quality improvement teams. These collaborations support practitioners access to professional development support and training.
In 2017, a 5-year strategy was produced (Table 1). Six ambitions listed below shaped the Clinical School’s work programme. This provided an important structural framework to build future Clinical School developments.
The Clinical School strategy: 2018–2022.
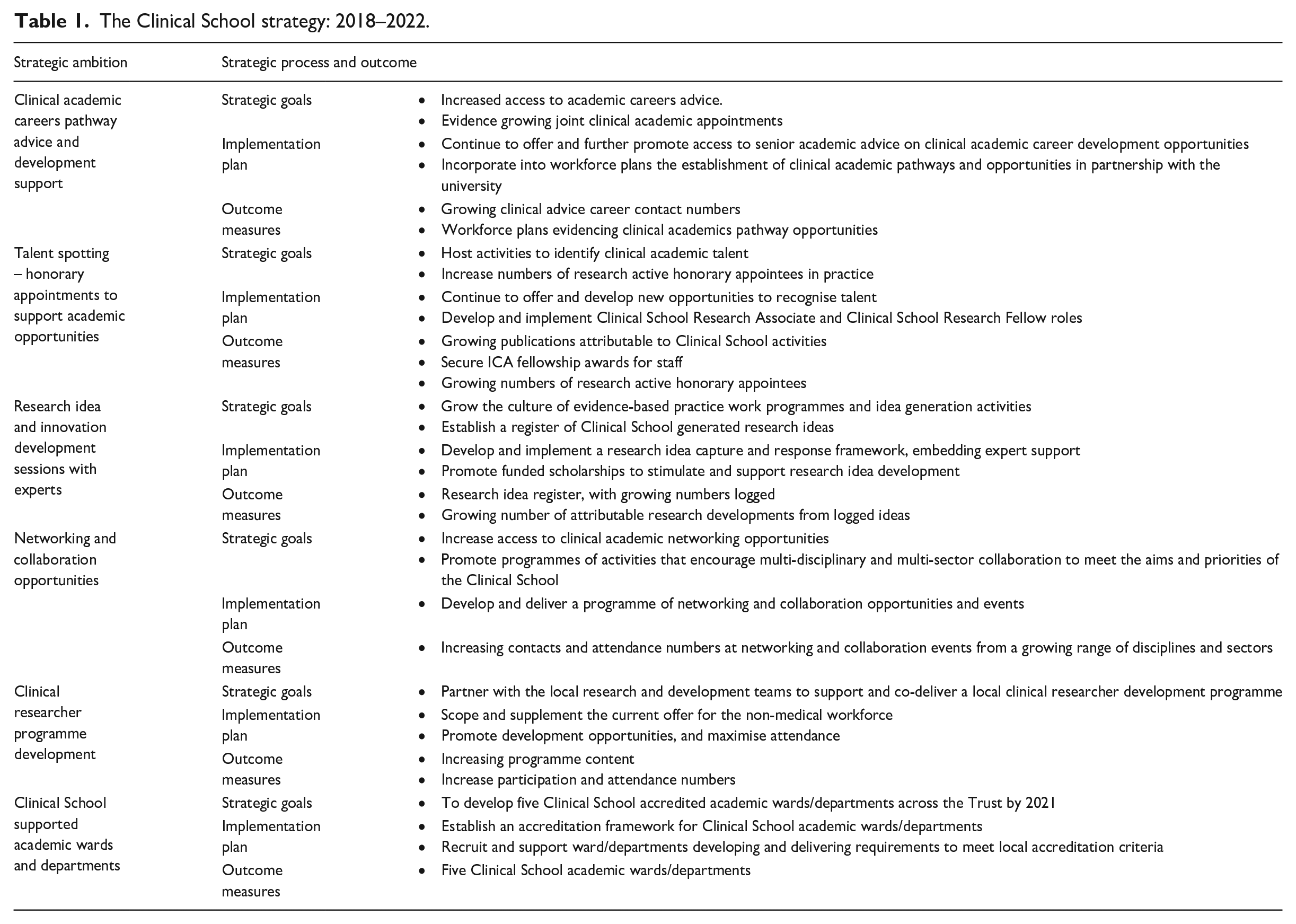
The co-directors have dedicated time in their job plans to drive forward the strategic goals of the Clinical School. Committed to this from the outset of the initiative, a reciprocal day-a-week (0.2 whole-time equivalent) arrangement has been significantly strengthened by the Trusts and now sees an additional 0.6 whole-time equivalent commitment, including additional senior nurse support to the partnership. Furthermore, agreement to have reciprocal arrangements in place for targeted staff in both organisations through honorary appointments adds further formal structure to the partnership arrangements, allowing research active staff in practice and in the classroom to hold honorary Clinical School Associate and Clinical School Research Fellow positions. All consultant-level practitioners are linked to the Clinical School with an honorary appointment supporting their role requirement of established higher education institution links and further build structural capacity to support wider engagement and research activity.
Funding, apart from salary costs and some shared administration capacity, is allocated to the co-directors; there are no budgets allocated from operational activity. Local charitable funds support engagement activities, used to fund prizes and awards, with limited professional development funds drawn down from education budgets or directly from clinical services. Indirect costs, such as support from Health Library services are recognised but not quantified.
The physicality of the Clinical School changed in the last 3 years with the opening of a formal shared office space, able to host a co-director with additional flexible desk spaces. The office is co-located within one of the Trust’s research and development department and provides access to university and hospital information technology and system infrastructure. The university now host a web-based platform for a number of Clinical School initiatives, including an online formal journal of practitioner disseminating evidence informed initiatives written as part of a 400 words writing competition.
The Clinical School predominantly communicates through email, websites and social media platforms, such as X, to communicate core messages. Much changed during the COVID-19 pandemic in the way staff accessed and interacted with resources. The Clinical School embraced the movement to access a greater virtual world and continues to conduct its activities such a journal clubs, support groups and meetings online. Given the reach of the Clinical School across two large NHS trusts and the rural geography of this English county, this has been seen as a positive enabler for visibility and accessibility.
Process
From the start of the initiative, a philosophical underpinning of the Clinical School’s operational processes drew from the evidence base. Implementation science bridged the research practice gap. Adoption of the Knowledge to Action Framework (Graham et al., 2006) influenced knowledge generation and implementation actions, best seen in a Clinical School supported PhD thesis of Underwood (2020). In the last 2 years, a move to adopt the JBI evidence-based healthcare model (Jordan et al., 2019) and its evidence implementation framework (Porritt et al., 2020) has served to connect strongly to the University’s international JBI collaborating centre and provides a clear evidence-informed model to support Clinical School process activities.
Clinical staff engagement has been central to the Clinical School’s administration of activities, talent spotting and support (second ambition) being approximately two-thirds of the Clinical School’s work. Table 2 highlights a wide range of activities that have been developed to fulfil this ambition.
A list of Clinical School engagement activities.
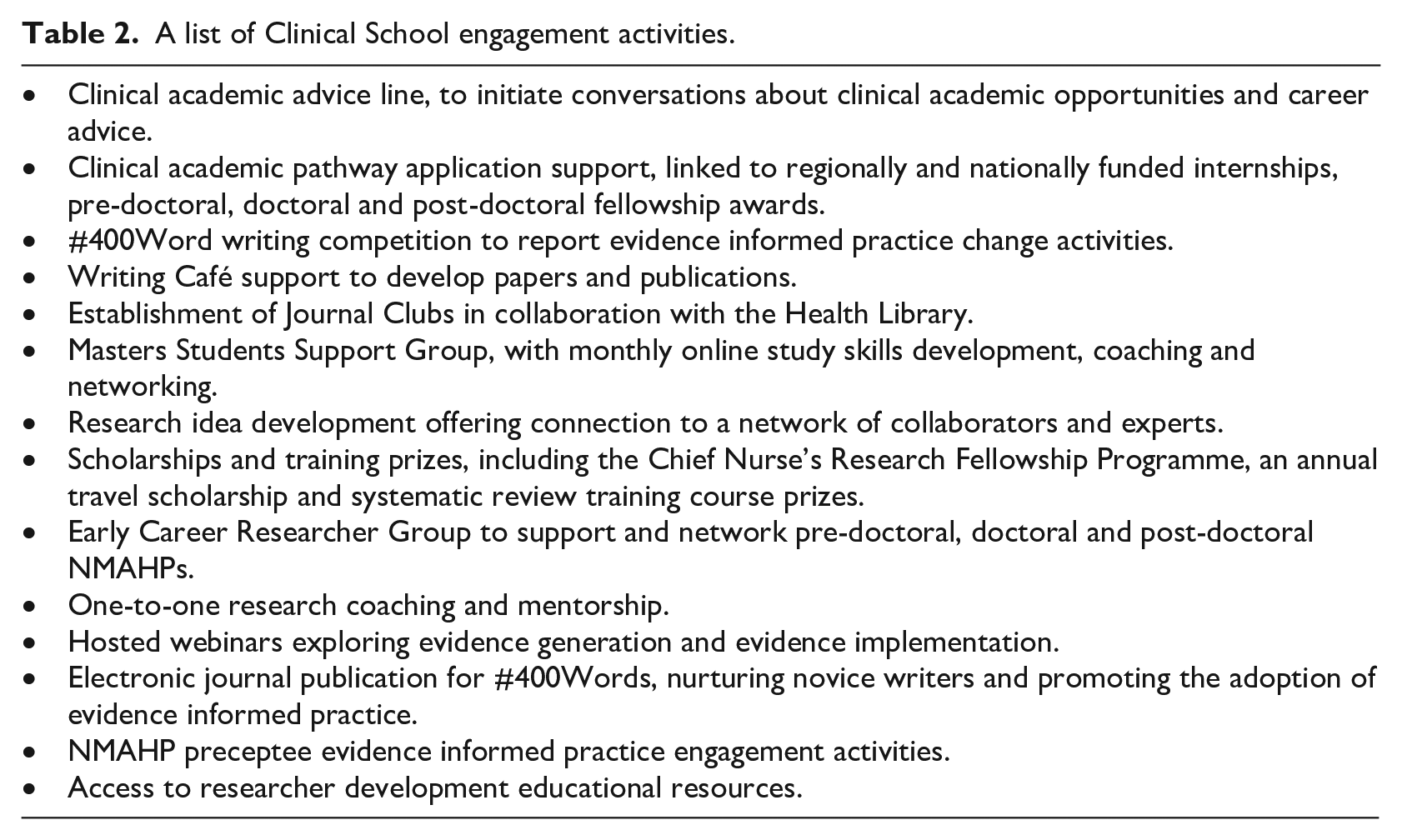
All engagement activities link back to the Clinical School’s strategy. The progress and process to create accredited clinical academic wards and departments (sixth ambition) have been harder to achieve. Numerous engagement barriers have been recognised. Following feedback from ward and department leaders, a strategic shift in language used by the Clinical School has taken place, from being ‘research’ focused to adopting language such as ‘evidence-informed’ and ‘evidence enquiry’ (Olive et al., 2020). Anecdotally, this has seen more staff engage in activities and come forward for support. Additionally, questions in the trust’s local accreditation programme (Underwood et al., 2020) were strengthened to score positively if evidence of Clinical School engagement was shown on inspection. This reinforces the link between research engagement and higher performing and safe clinical areas. Such process changes to achieve this ambition continue. The aim to develop a hierarchy of engagement activities to achieve accreditation is planned, for example the next-step seeing an active journal club in the area. Progress on one unit started well, but then set back by the necessary COVID-19 pandemic response and priorities during that time.
The process of applying the Clinical School in practice is continuous as, in a world of competing priorities, the need to represent and refresh the proposition to practice requires constant consideration.
Outcome
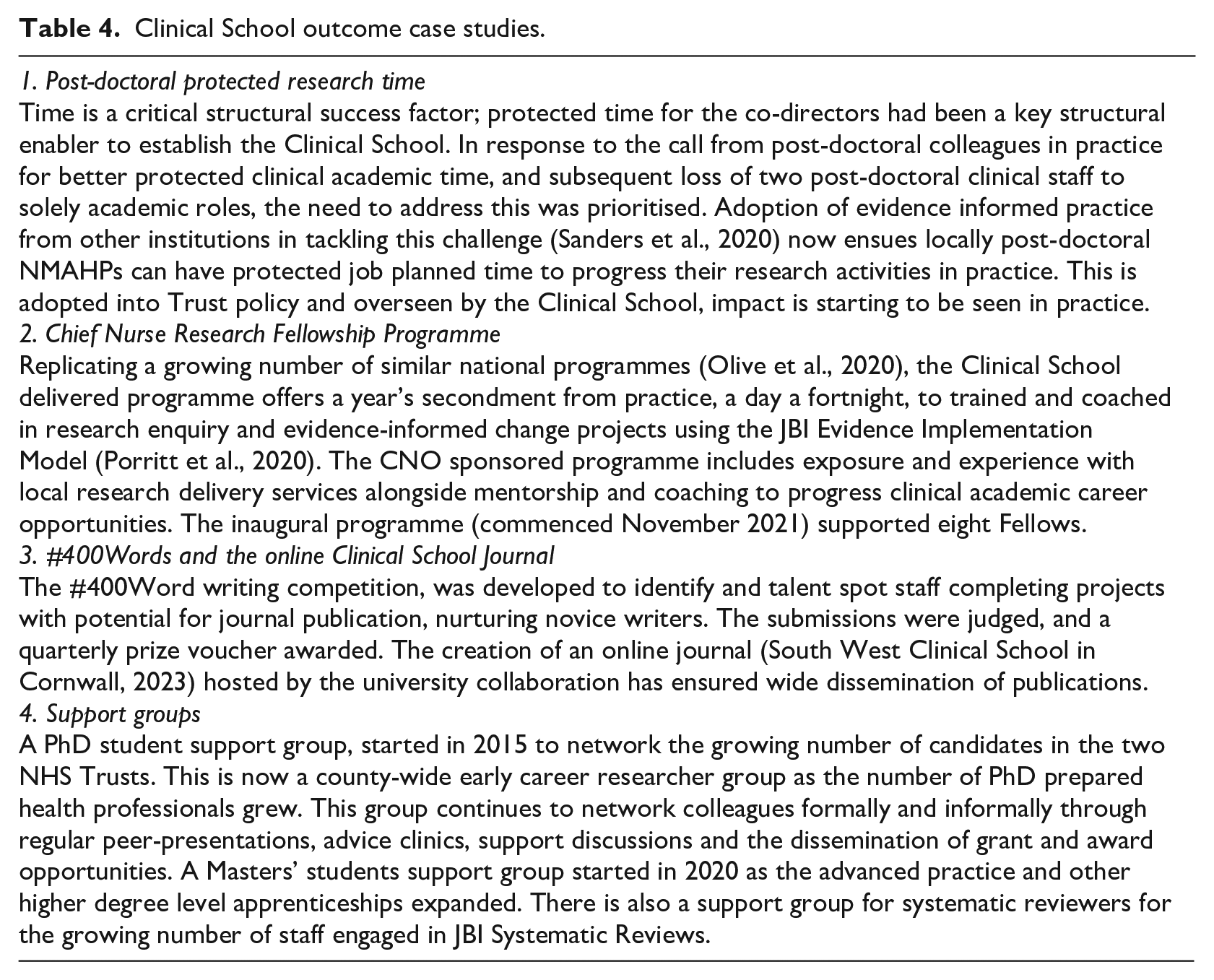
Donabedian (2005) wrote on measurement in terms of judgement against standards, which can be empirical or normative. In the context of this Clinical School initiative, empirical benchmarking standards are missing. Data are presented reflecting outcome information reported in earlier studies comparing, for example the number of supported doctoral candidates or numbers graduating. In this section, four brief case studies are included alongside additional locally measured and reported impact measures.
Process activities (Table 2) take front-line nurses and others through opportunities to explore evidence in practice and then to support them in using implementation models to adopt and improve practice. The next step often explores evidence synthesis and individual research idea development, leading on to career development opportunities, offering fellowship ICA fellowship application input and later post-doctoral support.
Outcome data are presented quantitively in Table 3 and more qualitatively in Table 4. The discussion section comments further on these data.
Clinical School impact grid.
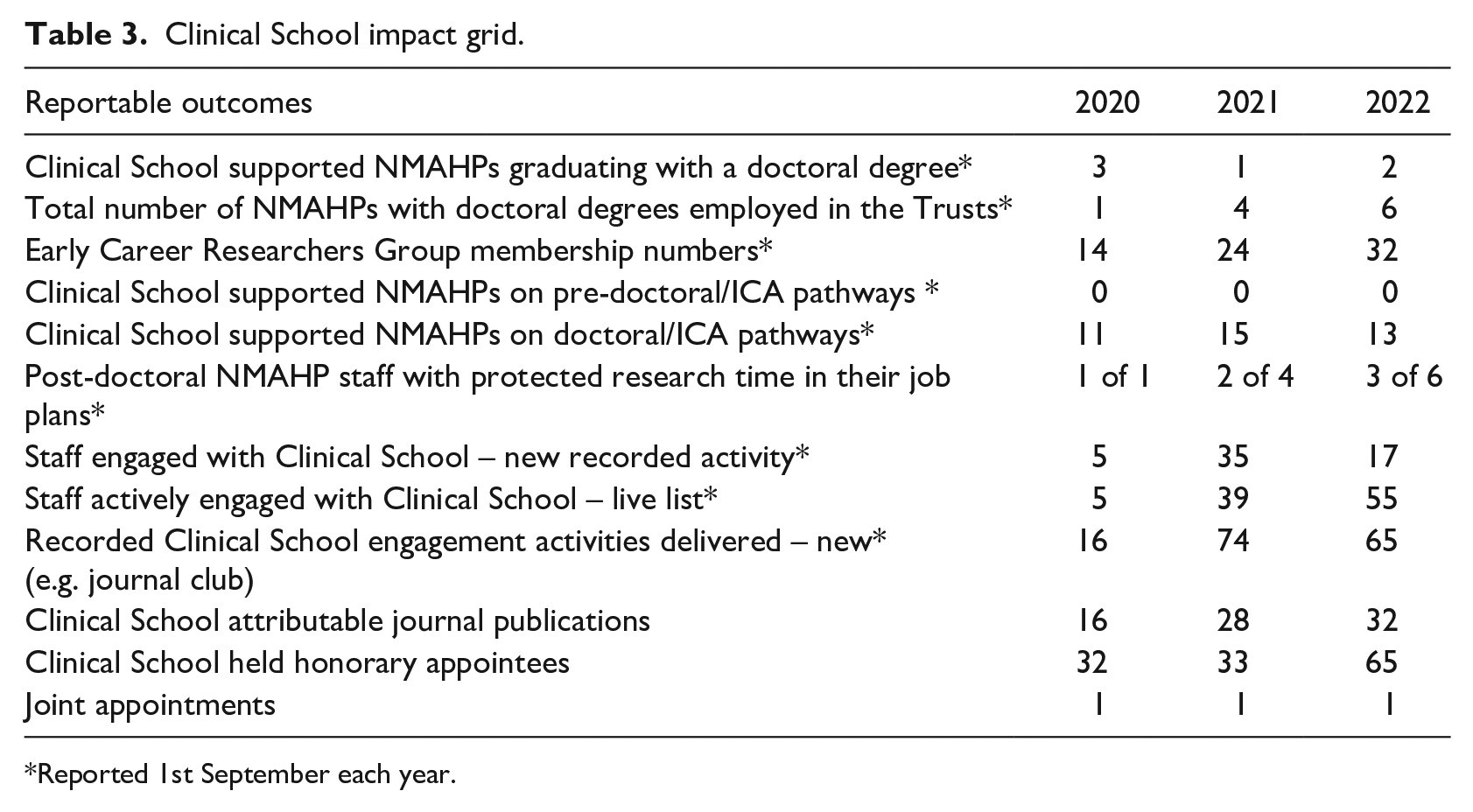
Reported 1st September each year.
Clinical School outcome case studies.
Discussion
Research findings identify an important association between the engagement of individuals and healthcare organisations in research and their subsequent high performance (Boaz et al., 2015). The CNO for England’s strategic plan for research has a focus on ‘building the best research system’ for nurses in England’s NHS (NHS England and NHS Improvement, 2021). This paper reports a local service improvement initiative to create organisation-level infrastructure to drive the creation of an evidence-informed culture across nursing and other non-medical professions. The idea of bringing academics from universities closer to practice is not new (Strickland, 2017), but embedding them in practice to build an effective, beyond self-serving, partnership, built on reciprocity, is much more unique. Clinical School activity reported in this paper is intended to prompt a wider discussion across clinical and academic worlds to address how best research ‘poor’ organisations (NHS England and NHS Improvement, 2021) can structurally develop to maximise their workforce’s contribution to research and evidence-informed practice and, in turn, optimise organisational performance and safety.
Reciprocal investment in Clinical School leadership and honorary appointments has fostered an internal structural-level bond between partners; this is seen as a crucial foundation to a mutually beneficial partnership. For practitioners involved, the honorary appointment offers broader structural system access, and, importantly, external recognition of their commitment to the Clinical School, which in turn contributes to the Clinical School’s wider strategic goals. Targeted-clinical academic commitment and activity in both organisations are easy impact examples and measures to report, and as in Table 3 could be compared to other studies (Strickland, 2017; Westwood et al., 2018)
With no empirical standards for such initiatives, reporting of outcomes can reflect biases and may neglect to illustrate honestly where challenges or failing may lie. The strategic plan for the Clinical School (Table 1) provides an objective framework to evaluate local impact, its intentions set out 5 years ago. Over the last 3 years, the Clinical School strategically shifted its language away from ‘research’ to focus more on ‘evidence’ discovery and implementation, reflecting on the reported successes of Olive et al. (2020). The sixth strategic ambition to create five clinical academic departments has not been delivered. Opportunities to learn from others regionally and nationally, ahead on developing such units, along with reviewing international literature could optimise the development of future clinical academic departments.
This paper reports data on the last 3 years; the sustainability of the model has been created through the reciprocal time commitment in job plans for the Clinical School leaders; however, time to reach this point is much longer at 8 years. There is a recognised maturity trajectory within wider Clinical School developments across the region that when reported will contribute further to the evidence-base.
This paper has limitations; in that, it reports openly on an infrastructure development aimed at fostering clinical academic career pathway opportunities; however, it is presented solely from the perspective of the provider. By others contributing to the literature their infrastructure developments, the opportunity to strengthen knowledge though evidence synthesis becomes more realistic.
Conclusion
The South West Clinical School in Cornwall is a practice-oriented research infrastructure development that aligns to England’s strategic ambitions for research capacity and capability building. Eight-year old, the model’s structure and process are reported alongside details of outcomes over the last 3 years. The paper describes a local service improvement initiative to inform debate, standardises elements of impact and evaluation and informs further research. Core to its reported success is the unique reciprocal investments made between two NHS healthcare Trusts and a Higher Education Institution (University).
Key points for policy, practice and/or research
Infrastructure to support the clinical academic growth of nurses is crucial. This paper describes one local initiative as part of the South West Clinical School Network.
There is a lack of reported evidence on developing organisational infrastructure to address the clinical academic aspirations of nurses working in NHS Trusts.
Higher education institutions are key enablers to build collaborative partnerships with healthcare providers to develop local clinical academic pathways and strengthen research capacity.
Structural support to develop clinical academic nurses to meet important strategic ambitions requires a stronger evidence-based foundation.
In the absence of empirical reporting standards, this paper makes an important descriptive contribution to the evidence-base, enabling shared learning and shaping future clinical academic research.
Footnotes
Acknowledgements
We would like to thank all members of the University of Plymouth’s South West Clinical Schools Regional Group, without which the outcome of the local initiative reported here would not have been possible.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have or have had a direct interest with this initiative which could have conflicted reporting. Reporting has been monitored and moderated to ensure that all facts can be substantiated against recorded and reportable evidence.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
No formal ethical approval was sought to report and disseminate the evaluation of this service improvement initiative.