
Abstract
Background:
COVID-19 has created mental health challenges for nurses. However, it is unknown if there is a gendered influence on nurses’ experiences during the pandemic.
Aim:
The aim of this study was to explore the experiences of male nurses during COVID-19, including their mental health and experiences of providing emotional support.
Methods:
We conducted semi-structured interviews using Zoom with nine male nurses and analysed the interviews using thematic analysis.
Findings:
Male nurses experienced negative mental health outcomes from the pandemic, but participants attributed these outcomes to the context. Male nurses provided emotional support for patients, students, families and other staff and did not describe emotional support as a difficult part of their work. Participants identified their role as a ‘breadwinner’ of being part of their concern during COVID-19. Participants used a variety of approaches to manage the stressors from the pandemic and cautioned against alcohol as a coping strategy.
Discussion and Conclusions:
Participants provided emotional support routinely as part of their work and went to great lengths to do so. This finding differs from most published literature that suggests male nurses struggle with emotional and interpersonal aspects of nursing. Male nurses require emotional support and employers can note that need for support may present differently by gender.
Background
The COVID-19 pandemic has placed increased pressure on nurses worldwide with nurses reporting significant changes to their work routines (Arcadi et al., 2021). Alongside increased workloads and long-term fatigue, nurses working during COVID-19 have reported increased levels of anxiety, depression and worry about contracting and transmitting the virus (Arcadi et al., 2021; Chen et al., 2020; Labrague and De los Santos, 2020; Mo et al., 2020; Shen et al., 2020). Nurses have been further challenged in providing emotional support for dying patients during COVID-19 while managing restricted visiting, personal protective equipment, and the need for either phone or digital conversations with families (Selman et al., 2020). These changes have negatively influenced nurses’ well-being and work experiences (Bruyneel et al., 2021; Huang et al., 2020).
Prior to COVID-19, researchers reported gendered differences in nurses’ job stress, burnout, social support and emotional exhaustion (Xian et al., 2020). Male nurses are often expected to be emotionally absent and lack compassion when it comes to patient care (Smith et al., 2020). According to Saleh et al. (2020), male nurses often receive poor education on emotion management, despite demonstrating a desire to emotionally support patients. There may be gendered considerations around mental health outcomes and emotional support during the pandemic that merit further consideration.
While there is a need to understand the consequences of the pandemic on nurses and provide them with support during the pandemic, there is a lack of research exploring gendered experiences or nurses working during COVID-19. It is important to understand the unique considerations of male nurses in this context to ensure that adequate support is available to meet their unique needs.
This study is a part of the second phase of a larger research project on nurses’ experiences during COVID-19 (Nowell et al., 2021). We conducted an international survey to better understand Registered Nurses’ experiences during the pandemic. In our survey analysis we identified that more male than female nurses reported facing challenges in providing emotional support for their colleagues and patients (p = 0.044). To explore this finding further, we conducted a second phase of the study with male nurses to learn more about their perceptions about their mental health and their experiences in providing emotional support for patients, students, families and colleagues. To the best of our knowledge, this paper presents the first known study focusing male nurses’ experiences during COVID-19.
Aim
Our aim in conducting this study was to explore male nurses’ experiences during COVID-19 including their mental health and experiences of providing emotional support.
Methods
Design
We conducted qualitative, semi-structured interviews with male nurses and analysed these data using thematic analysis.
Sampling and recruitment
In the first phase of the study, we distributed a questionnaire about COVID-19 for Registered Nurses using social media, email lists and word-of-mouth (Nowell et al., 2021). Nurses in any country were invited to complete the questionnaire. Participants were asked if they would be willing to provide an email address to be contacted for a follow up interview. In the current study, all participants who self-identified as male and consented to be contacted were sent an email invitation to participate (n = 14). Participants were invited to book an interview via Zoom and were sent one reminder email invitation. In total, nine participants agreed to be interviewed.
Participants and sample
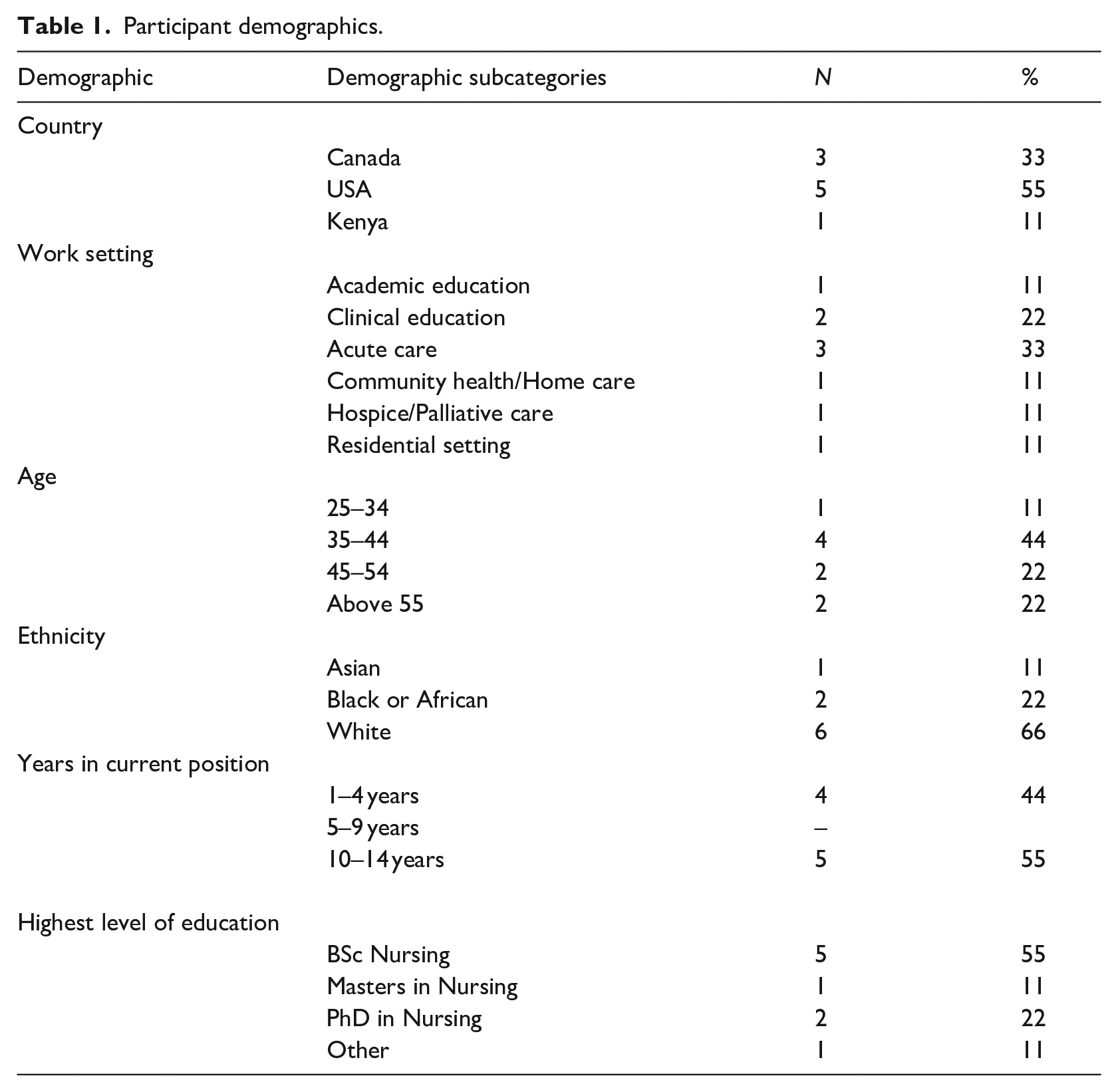
Participant demographic information is presented in Table 1. There was a total of nine male participants who were interviewed by our research team. Six participants worked clinically and three participants were nurse educators. For the participants who worked clinically, their experiences of providing support related to patients, family members and colleagues. The participants who were nurse educators provided emotional support to students and colleagues. These experiences overlapped sufficiently to include both groups in the study analysis.
Participant demographics.
Data collection
We conducted semi-structured interviews with participants via Zoom. The interviews were led by a male masters-prepared research associate, with extensive interviewing experience (MH). We conducted the interviews in July–August 2020, they ranged from 30 to 60 minutes in length. Each participant was interviewed once. The interview guide focused on participants’ work, mental health and emotional support, and how participants’ experiences were affected by COVID-19. Participants were asked specific questions about their impressions regarding the gendered differences in providing emotional support to patients and colleagues that were identified in the survey analysis. They were also asked general questions about their unique experiences as male nurses. The Zoom interviews were audio-recorded and transcribed verbatim by a professional transcriptionist to expedite the data analysis process.
Data analysis
Our data analysis method was thematic analysis, which is used for ‘identifying patterns of meaning (themes) across a data set’ (Braun and Clarke, 2012, p. 57). The purpose of thematic analysis is to understand experiences and identify shared meaning among different participants (Braun and Clarke, 2021). The hallmark of thematic analysis is inductive coding of text, to create themes that represent participants’ experiences (Vaismoradi et al., 2016). Themes are created through a process of coding, where codes may refer to relationships, concepts, the setting or context, participant perceptions or participant experiences (Vaismoradi et al., 2016). Researchers compare codes among participant interviews, and identify overlap among participant experiences, through a process of constant comparison (Vaismoradi et al., 2016).
We implemented a data analysis strategy focused on inductive, iterative coding. The first stage of the analysis was conducted by a research assistant (FG) and focused on identifying codes in the interviews that were relevant to the study aim. The primary investigator (JJ) and research assistant met to discuss early findings and the progression of coding. The research assistant then continued the analysis with other interviews. This process of coding and discussing was repeated until four themes were refined. The whole research team met to review the themes and select quotes to illustrate the participants’ experiences.
Ethical considerations
Ethical approval for all phases of this study was obtained from the local university research ethics board, protocol number REB20-0633 on 29 April 2020. Participants provided e-signatures on written consent forms, prior to participating in an interview. Participants were reminded that they could end an interview at any time or skip any of the questions, although no participants chose to do so. Participants were not considered a vulnerable population and all consented to participate in the study. The transcriptionist signed a confidentiality pledge and the interviewer anonymised the transcripts, so that no other team members accessed any identifying information. We used alpha-numeric codes to identify the interviews during data analysis. All study materials were kept on a secure university server and there were no paper records associated with the study.
Rigour
We used several rigour enhancing strategies in this study. There was alignment between our research aim, study method and participant population (Carnevale, 2016). The interviews were transcribed by a professional transcriptionist and verified by a research assistant (Richards and Morse, 2012). We used data management software (NVivo v12 Plus) for the organisation of transcripts and coding. The research team had ongoing reflexive discussions to encourage peer review and reflection (Braun and Clarke, 2021). The themes that emerged during analysis were also reviewed by the interviewer to confirm that the topics that were discussed were accurate and representative of the discussions. We also used an analysis journal and file naming conventions to carefully track our progress and establish an audit trail.
Findings
Overview of findings
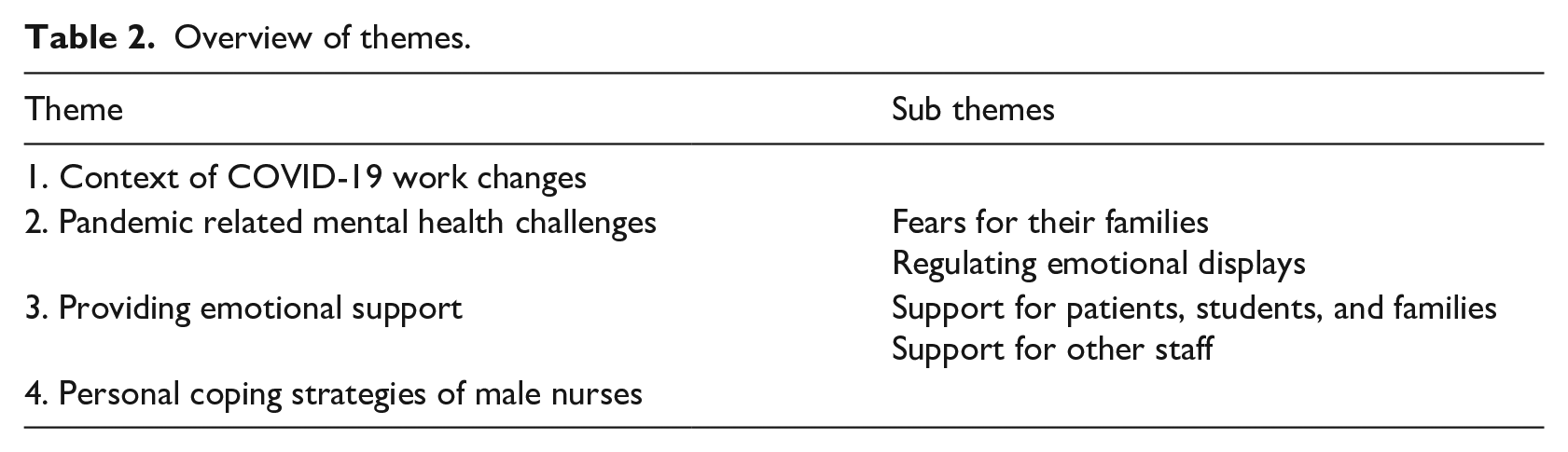
Participant experiences were captured through four themes, illustrated in Table 2. Participants reported marked changes in their work, which created the context for their experiences. Participants discussed the influence of the pandemic on their mental health and their ability to provide emotional support to patients, students, families and each other. Participants also reported their personal coping strategies for managing during the pandemic. These themes are explored in detail in the following sections.
Overview of themes.
Theme 1: Context of COVID-19 work changes
Male nurses described a large increase in their workload, including new COVID-19 responsibilities. These duties included additional personal protective equipment (PPE) donning and doffing, increased complexity of care, barriers to connecting with families, complex staff management and coordination, and a switch to new daily routines. One participant explained how home care visits changed, due to COVID-19: I’ve got an area designated in my car with one brown paper bag and that’s for my trash. It’s for my used rubber gloves or any PPE that I’ve used. I take it off outside the door of the home after I leave. I pretend essentially that I’m leaving an isolation room in a critical care unit. And doing it on the porch or whatever. In another part of my car, I’m maintaining another paper bag and we figured out that paper bags were the best way to do this. We used to carry cloth bags of stuff for infection control so that’s changed. I do the whole donning and doffing thing (P4).
This participant had to reorient his equipment to avoid contamination and develop a complex process to visit clients safely in the community. Participants described these changes as a huge adjustment from their previous routines. They also created adaptations in the context of changing evidence, a lack of equipment, and high levels of uncertainty. The experience of changing work routines was described as stressful and taxing.
These changes were not exclusive to clinical work. Participants reported that their work changed in all settings, including education. There have been massive changes to my work, of course. We actually left the university physically mid March and we have not returned to the university (P8). This participant highlighted how the physical location of work changed, and in turn, all his work shifted online. These changes created the context for male nurses’ mental health and their provision of emotional support. Participants had to interact with patients and students differently as a result of measures like physical distancing and working from home.
Theme 2: Male nurse mental health
Participants reported that working during COVID-19 had a negative influence on their mental health. The participants were made aware of the survey findings from the larger project during the interview.
Fears for their families
Participants responded by revealing their mental health struggles and confirming that their mental health was adversely affected by the pandemic. A participant reported that his role as a leader in his family contributed to mental health challenges: Because when the hospital shut down, you know elective surgery stopped, we lost a lot of business. We were unsure of our future. So being the head of a family and being the breadwinner of a family with a child, you start to get overwhelmed (P1).
This participant felt additional burden from COVID-19, relative to his self-concept of being the head of his family. He perceived that his role conveyed additional responsibility and struggled to manage the stress. Other participants also associated their mental health difficulties with their roles as a father.
I was reading stories of nurses and doctors who would go home asymptomatic or mildly symptomatic and family members would find them dead. And it turned out to be a pulmonary embolism, or a heart attack or stroke. And there was that fear that I would go to sleep and not wake up and or my wife would have to come over here and find me. So, that anxiety, man I was, I can’t even describe it. I’ve never experienced anxiety before, not to that level but I’m fearing of not waking up and leaving your kids without a father (P3).
This participant saw the potential consequences of COVID-19 relative to his children and wife, not only himself. He was also fearful about the experiences his wife may have as a lone parent if he became ill. Participants also found that COVID-19 changed their family relationships, which limited their social support.
So it’s definitely changed how I live my life. My wife and I, we hug, but on a very real level, I haven’t kissed my wife in like four or five months. Because of that fear and that’s really difficult for us, but it’s like, what’s the alternative? Like what if she were to get sick, could you live with yourself? (P3).
This participant feared the outcomes for his family because of his work as a nurse during the pandemic. The mental health challenges among these participants were associated with their roles as fathers and husbands, and how the pandemic could affect their family life. Even when participants were away from work, they were fearful for their families, and found it difficult to escape from the anxiety.
Regulating emotional displays
Other participants reported that their emotional displays were influenced by working during COVID-19. Participants felt they had to present a calm affect, even if that did not reflect their true feelings. When asked if he had noticed an impact on his mental health, this participant stated: I think it’s a real balancing act, to not freak out even as we hear [more about COVID-19]. And sometimes, the bad news piled on bad news becomes a lot. At my lowest points I just ride it out, and then get back up (P4).
This participant felt that he had to maintain calm emotions and continue working. These experiences were difficult for participants. With the additional COVID-19 workload and responsibilities, male nurse participants were under stress pertaining to catching the virus, taking care of themselves and caring for their families.
In contrast, another participant did not identify a gendered element when asked if gender made a difference in his experiences.
Everyone shared the same concern. I wouldn’t say that there were males that were more afraid [of COVID-19] (P5).
This participant characterised the pandemic as being a negative influence on everyone’s mental health and that the context, rather than gender, was a dominant factor.
Theme 3: Providing emotional support
In the context of a changing workload and the emotional impact of these changes, participants reported that they had to provide additional emotional support for patients and their families, students and colleagues. Participants did not report that providing support itself was difficult from a gendered lens.
Support for patients, students and families
Male nurses described increased incidences of having to provide emotional or spiritual care to patients. However, participants did not report their gender as a factor in their experiences of providing emotional support. When asked if the additional support needs were difficult to manage as a male nurse, a participant responded no, because he engaged with patients and families often: Patients no, I don’t think so. Not for patients, partly because I’m probably one of the people that spend more time with talking to patients and families about their concerns (P2).
This participant did not identify gender as a barrier as he regularly provided emotional support to patients and staff. The additional emotional support he provided during COVID-19 was an extension of his usual practice and was not unduly stressful.
The male nurses spoke about how they made extra efforts to provide emotional support for patients and their families during the pandemic. Participants worked to connect with families, recognising the challenges of being away from a loved one: It was a more critical ICU so most of our patients were intubated. So, we were having to deal with more with the family and trying to comfort them, and have a lot more communication, because they weren’t allowed in the facility whatsoever. So, we were the only point of contact, their point of reference. So, they talk to us. We did use our own personal devices to do Zoom meetings, FaceTime, Google duo was another one that we used a couple of times. Whatever system we could use to do that. We would use our personal devices. Sometimes our patients would have their devices with them and we’d be able to use those if they weren’t locked. (P6).
This participant overcame barriers to connecting with patients’ families by using technology. This effort allowed families to see their loved one, despite the restrictions in place. It required extra work on behalf of the male nurses to create these connections, and their use of personal devices shows their willingness to provide emotional support for patients and families.
Support for other staff
Male nurses were also called upon to provide emotional support for colleagues and receive emotional support in turn. Participants noted that with increased workloads, other nurses required extra support with personal emotions and carrying out their responsibilities. Participants described strategies that included acknowledging that everyone was under extra stress, giving each other space when needed, and asking colleagues if they needed help: So I think we’ve all cut each other a little more slack, everybody’s under a lot more stress than they used to be. So when somebody’s off, when you have a co-worker who comes in, you can just tell they’re not having a good day. We’ve always been supportive, but I think we’re also learning to give each other space when we sense that they’re not having a good day. And then typically we will get them one on one or we pull them into the supply room or the med room, we’ll say, ‘Hey, are you okay?’ And I think everybody in our department has somebody on the staff that they feel comfortable to completely open up to (P3).
This participant highlighted the importance of looking out for other colleagues, checking in with others, and not minding colleagues’ behaviours if they were upset. The participants discussed how this approach was applicable to everyone who was working in the same context and did not differ among colleagues based on gender. A participant acted as a role model to encourage cooperation and support: So on a personal point of view, I have taken it very, very positively because if I don’t take it very positively then it is going to hinder most of my staff. That’s why I’m telling you, it’s a very difficult situation because as much as it is difficult, you have to show your members of staff that, yes, it is difficult, but we have to work around it (P9).
This participant felt a sense of obligation to his colleagues to support them through difficult changes. Participants identified this support as a collective responsibility, rather than a gendered issue.
Theme 4: Personal coping strategies of male nurses
Participants noted that their work changes and stresses led to various coping mechanisms. These strategies included talking more with coworkers, to taking on new hobbies, and hosting socially distanced gatherings after shifts. Some participants noted the colleagues were more talkative than previously. Others described talking to their neighbours and family through backyards and video chat, relying on support from churches, and taking on new hobbies. Participants also used alcohol as an entry point to debrief their experiences: It was a lot of venting sessions. All the bars and everything closed down here so we actually, a few mornings, being third shift, we get off, we clock out at 7:30 in the morning. One guy started it. He had a case of beer in the back of his truck that was cold. It was still cold outside so it stayed cold all night. We just went out to the parking lot and sat around, and we had a few cold beers and we’re just destressing. Because we had no other real outlet (P6).
This participant reported that he continued these sessions, bringing in beer to have in the parking lot after work for colleagues. The beers created an opportunity for colleagues to debrief informally and offer each other emotional support.
Other participants noted that alcohol was a factor in their coping strategies as well. This participant reported how he became more interested in gardening, after recognising that alcohol was not a positive coping strategy for himself: I’ll tell you (laughs) if you asked me 20 years ago I’d say you’re crazy but I found gardening, of all things [. . .] There’s this cathartic aspect of growing something and bringing life and whatever. All that touchy feely stuff, but it really has. It beats the alternative. About a month after I came back, I don’t drink at all but I started, I was drinking a little bit more than I normally do. And then I was like, well I can really see how you can become an alcoholic really quick. You get that numb feeling. I said this is a little too real for me, so I ended up getting rid of everything, all the alcohol in the house. And poured it into gardening and I’ve been fine since. Yeah, just trying to find a more positive outlet (P3).
This participant was quick to caveat the benefits of gardening as ‘touchy feely stuff’ but reported the personal value of coping strategies that did not involve alcohol. This finding suggests that participants had preconceptions about some coping strategies, but also recognised the need to have dedicated activities to manage their COVID-19 stresses.
Discussion
Our aim in conducting this study was to explore male nurses’ experiences during COVID-19 including their mental health and experiences of providing emotional support. While participants reported increased workloads and negative mental health outcomes, these were attributed to the pandemic rather than their gender. Providing emotional support for patients, students, families and colleagues was not described as a difficult part of their male nurse’s work.
Participants in this study reported similar COVID-19 related changes to their work as those described in other studies. Increased workload and PPE use have been found challenging for nurses in most areas (Liu et al., 2020). According to Mo et al. (2020), extensive patient care and additional hours were found to be a stressor among nurses working in the pandemic and resulted in increased anxiety. Male nurses are negatively impacted by increased workload and inadequate support (Xian et al., 2020), which has been demonstrated widely among general nursing populations as well. The findings of this study reinforce the challenges created for nurses by the pandemic.
Male nurse participants in this study reported negative impacts on their mental health, due to COVID-19, which is consistent with other studies (Arcadi et al., 2021; Chen et al., 2020; Labrague and De los Santos, 2020; Shen et al., 2020). The current study contributes insight into the gendered elements of this anxiety that affected some male nurses. Participants reported that their role as a breadwinner increased their concern for their families during COVID-19. The breadwinner narrative remains central to social narratives of masculinity (Abrahamsen, 2004; Lindsay et al., 2009). However, this dynamic is changing in Western countries, with both partners having a role in breadwinning, domestic and childcare labour (Abrahamsen, 2004; Lindsay et al., 2009).
Similar concerns about being a breadwinner have been described in other studies. Male nurses reported that a reason for leaving nursing was that a nurse’s salary was insufficient for them to meet the social expectation of being a breadwinner for their families (Kluczyńska, 2017; Zhang and Tu, 2020). Sasa (2019) identified the expectations of being a breadwinner and leader of a family as antecedents of the concept of a male nurse as a distinct entity. These views were reflected in some comments from participants in the current study. However, participants in the current study explained their breadwinner role in a way that reflected both practicality and genuine concern for their children and partners. The findings of this study differ from other accounts because participants reported the difficulty with their mental health was not heavily gendered, but instead reflected a reasonable response to their pandemic context.
Our findings about male nurse emotional support differ strongly from many studies, where male nurses have been described as struggling with patient interaction. The responses of participants differed from published examples of men avoiding emotional support in favour of other elements of nursing work. These experiences included male nurses who worked in the intensive care unit, who spoke at length about the importance of emotional support in addition to biomedical care. Male nurses have been reported as responding to patients’ emotions at work with a strong consciousness of gender in their roles (Yada et al., 2014). One study reported that most male nurses in their sample did not really want to be nurses, and preferred working in critical care settings with more technology to avoid patient interactions (Zhang and Tu, 2020). Other studies report a male nurse preference for tasks and roles away from the bedside, where less emotional support is expected (Abrahamsen, 2004; Kluczyńska, 2017; Matthews, 2001; Saleh et al., 2020). Male student nurses reported that they aspired to work in critical care settings, with less interpersonal contact (Mohamed and Mohamed, 2015). These studies may be related to social and organisational expectations of emotional labour, which influence how employees present their emotions during their work (Hochschild, 1983; Smith, 1992). These studies suggest male nurses preferred to avoid providing emotional support as part of their work.
In contrast, the participants in the current study actively engaged with emotional support for patients and others and went to great lengths to provide this support. They did not describe emotional support as gendered or difficult, even when asked directly. There were other studies that supported our findings, including reports that male nurses do provide emotional support with patients (Younas and Sundus, 2018). It is also notable that performances of emotions and masculinity are influenced by the environment (Ridge et al., 2011). It may be that some healthcare environments are more conducive than others for male nurses to provide emotional support. These findings indicate that experiences of emotional support are more nuanced for male nurses than some studies suggest.
There is evidence to indicate that men may express stress and anxiety differently than women (Ridge et al., 2011). While men and women tend to experience mental health concerns at similar rates, women are more likely to verbalise that they experience these issues (Ridge et al., 2011). These differences include an increased use of alcohol among men to cope with distress (Ridge et al., 2011). Psychological support has been an important part of the pandemic response in case studies (Bernstein et al., 2021; Huang et al., 2020). People offering psychological support can be prompted to consider gender during their assessment of apparent distress. We did not identify reports of male nurses using different coping strategies to respond to workplace stress, as nurses reported similar activities to manage at work as in the current study (Akbar et al., 2016). When suggesting coping strategies, organisations could recommend activities that avoid alcohol and optimise opportunities for collegial support.
Limitations
The findings of this study are limited by several factors. There may be variation in the participant experiences due to the phase of the pandemic when they were interviewed or the severity of the pandemic in their area. We conducted a single interview with each participant and the findings of this study may have been different if we had spoken with participants at different points during their pandemic work. There were also only three countries represented in the sample, so it may be that male nurses in other areas experienced COVID-19 in ways that are not accounted for in this study. As the pandemic progresses, we recommend that this study be repeated or expanded upon, with a larger, more diverse sample. Male nurses from other roles could also be included to reflect upon their experiences across nursing roles.
Implications
Male nurses reported difficulty with their mental health during the pandemic, although this finding was attributed by participants to the pandemic context, rather than gendered factors. Participants readily provided additional emotional support to patients, students, families and colleagues. While participants acknowledged the challenges of COVID-19, they did not associate undue burden with supporting patients. Nurses and professional organisations can respond by recognising the skill of male nurses in providing emotional support for patients.
We found that male nurses’ experiences of providing support did not always match other accounts in the literature. Nurse leaders can create interventions to support all nurses, responding to the COVID-19 context rather than gender. An important next step for this field is to create and evaluate intervention studies, to determine if a broad suite of programmes is adequate for all staff. There are opportunities to facilitate nurses’ support for each other and there are opportunities to enact personal coping strategies. To support nurses during the pandemic, nurse leaders are encouraged to recommend activities that avoid alcohol and provide opportunities for nurses to connect and discuss their experiences.
Conclusion
Male nurses’ mental health was negatively impacted by the changes to their work during COVID-19. However, they have made extra effort to support patients, students, families and colleagues during the pandemic. Male nurses reported that their experiences were heavily influenced by the context of the pandemic, rather than gendered considerations. Nurse leaders are encouraged to offer supports to all nurses for their mental health, provision of emotional support and use of personal coping strategies. The findings of this study challenge dominant narratives in the literature about male nurses and emotional support and merit consideration during interventions for nurses.
Key points for policy, practice and/or research
Male nurses went out of their way to provide emotional support to patients, students, families and colleagues during COVID-19, contrary to evidence that suggests male nurses avoid this work.
Male nurses struggled with their mental health during the pandemic, including fear for their families. They reported regulating their emotional displays to support others.
Organisations can support the mental health of all nurses, recognising that male and female nurses with mental health difficulties may present differently.
Footnotes
Acknowledgements
The authors would like to thank the participants in this study, and Swati Dhingra and Lorelli Nowell for their support during the project.
Data availability statement
Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data is not available.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jennifer Jackson is a member of the International Advisory Board for the Journal of Research in Nursing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by University of Calgary, Faculty of Nursing, Research start-up funding.
Ethical approval
Ethical approval for this study was granted by the University of Calgary Research Ethics Board, REB20-0633.