
Abstract
Background
Nurses have a rich history in performing their duty both domestically and internationally in response to a disaster. Comprising the largest proportion of the healthcare workforce, nurses possess a unique opportunity to inform disaster planning and management. With the ongoing threat from COVID-19 and continuing conflict, humanitarian aid needs, epidemics and natural disasters; the capacity of nurses to continue to respond in times of global need is unparalleled.
Aims
The aim of this paper is to explore the developments in the field of disaster nursing. Mapping key changes in policy, practice and outcomes.
Methods
A qualitative interpretive historical review was conducted to examine core developments in the history of disaster nursing, examining key organisations (e.g. World Health Organization, International Council of Nurses), national and international policies and historical accounts.
Results
29 articles were analysed, and politics, strategic perspectives and nursing identity (‘sense of duty’ and roles) emerged from the literature. The influence of professionalisation and public health/health promotion emerged next. A total of 10 articles refer to disaster nursing specifically, of which 4 of these are reports/policy.
Conclusions
Nurses have spent centuries building the trust and legitimacy of the profession. Disaster nursing goes beyond the expectations of a registered nurse. The responsibilities of a disaster nurse encompass wider community health promotion, critical decision-making beyond the individual patient, resilience and ethical challenges. Whilst significant advancements have emerged in the last 30 years, further research, and representation of the profession at a strategic and political level could enhance the effectiveness of nurses’ roles in the 4 phases of disaster response: mitigation, preparation, response and recovery.
Keywords
Introduction
Nurses have a rich history in performing their duty both domestically and internationally in response to a disaster; be that natural or human-initiated. Yet, the role nurses play in the phases of disaster response had not been formally recognised until the publication of the International Council of Nurses (ICN) Disaster Nursing Competencies Framework (2009). Comprising the largest proportion of the healthcare workforce, and are often frontline, nurses possess a unique opportunity to inform disaster planning and management both operationally and strategically (ICN, 2009; Pourvakhshoori et al., 2017). Historically, nurses practising in these austere environments have not been referred to as disaster nurses. Instead, nurses have been identified with a specific skillset including creative problem-solving skills, resource management, clinical capabilities and communication skills, that complement disaster response (Pourvakhshoori et al., 2017).
In 2020, the World Health Organization (WHO) Year of the Nurse, the COVID-19 pandemic reminded the world of the crucial role nurses play in supporting the delivery of healthcare to communities. The focus of the historical review is to explore the developments in the field of disaster nursing. Using the widely adopted 4 phases of disaster management of mitigation, preparedness, response and recovery (Sawalha, 2020), the history of nursing and its relationship with context and time will be examined; exploring the literatures’ relationship to key trends in policy development. This is not a review of disaster management, rather an abstract review of the history of the specialty – a summary of specific key examples in the progression of disaster nursing throughout history.
Background
The United Nations Office for Disaster Risk Reduction (UNDRR) define disasters as natural (geophysical, hydrological, climatological, meteorological or biological) or human-initiated (armed conflict, famine, environmental degradation, chemical or radiological events) (UNDRR, 2020). This can be in the form of an earthquake, volcano, tsunami, drought, cyclone, disease epidemic/pandemic, as well as conflict and biological warfare. Additionally, a disaster can occur immediately (e.g. earthquake) or progress slowly with a larger public health focus (e.g. epidemic such as Ebola). These natural or human-initiated hazards become a disaster when they affect a vulnerable community or society that has an insufficient capacity to prepare and respond effectively to mitigate the impact of the hazard(s) or displaced populations (UNDRR, 2020).
Disaster management in some form has been in existence as long as humans have (Ripoll Gallardo et al., 2015). It is human nature to care for the ill and dying. Early records of disaster management and battlefield trauma reach back to the Napoleonic era. Where the concept of triage was developed by Baron Dominique Jean Larrey in the 1790s (Surgeon in Chief to Napoleon’s Imperial Guard) when he changed the approach to field casualty care to commence prior to the end of the battle (Edwards, 2013). The assignment of degrees of urgency and order of treatment to the large number of casualties resulted in increased survival and enabled more soldiers to return to battle, increasing the force capacity (Edwards, 2013). The concept of disaster medicine and nursing, however, did not begin to appear until the arrival of modern medicine at the turn of the 20th Century alongside the industrial revolution (Suner, 2015; Stehrenberger and Goltermann, 2014). Prior to this, it could be argued that disaster medicine lay in its military roots.
Despite the progression of civilian disaster management and medicine, the military still have a crucial role to fulfil in disaster response in modern practice (Stehrenberger and Goltermann, 2014; Suner, 2015). The military have the unique ability to mobilise thousands of personnel, specialist equipment and critical supplies at short notice to enable rapid response to an international disaster or crisis (Suner, 2015). This is a pivotal role to play, however, can pose equally challenging aspects to host countries and militaries alike with the need for mass coordination of assets and effort (Garfield et al., 2003; ICN, 2009; Suner, 2015). Following the formation of the United Nations (UN) in 1945, international humanitarian aid provision increased and non-government organisations (NGOs) began to form in response to this. NGOs were able to venture beyond politically sensitive borders and continue to provide essential care to vulnerable populations (Wall, 2015).
Disaster management and disaster response have traditionally been reactive – deploying into an affected region in the aftermath of a disaster. In the last two decades, this has progressed to focus more on prevention, planning and risk reduction – this is aligned to the Hyogo Framework (2005–2015) and more recently the Sendai Framework (2015–2030) – designed to provide a strategy for disaster risk reduction endorsed by the World Health Assembly (WHA), UN and WHO. This is based on a widely adopted disaster management continuum involving 4 phases – mitigation, preparedness, response and recovery (Sawalha, 2020). The four phases have been contested in the literature to consider their dynamic and integrated, rather than linear processes (Sawalha, 2020). Additionally, further phases have been documented to include prevention, rehabilitation, reconstruction and emergency intervention (Sawalha, 2020). Despite this, the use of the four-phase cyclical approach is the most consistent throughout the literature and disaster organisations (e.g. ICN, WHO and UN) in disaster response.
Prior to the registration and professionalisation of nursing at the turn of the 20th century, religious orders trained ‘nurses’ and cared for the ill (Hunt, 2017). The increasing role of women in society with rising awareness of status and rights, facilitated the evolution of nursing into the respected modern-day profession it is now known as (Hunt, 2017). Nursing was traditionally a caring role – hygiene, wound care, nutrition and elimination (Beck, 2010). Modern nurses are also required to do this, plus critically assess, implement and evaluate care (Nursing and Midwifery Council [NMC], 2018). The increased demand on the healthcare system paralleled traditional disaster response challenges, whereby facilities, staff and resources were overwhelmed globally (Nowell et al., 2021). The response to the pandemic demonstrated the ability of any nurse to rise to the challenge of responding to a disaster within a community or wider population, irrespective of their specialty (Nowell et al., 2021).
The progression of the concept of disaster nursing has occurred throughout history in parallel to the developments made in the professionalisation of nursing itself (Hunt, 2017; Pourvakhshoori et al., 2017). Although specific references to the term ‘disaster nurse’ are absent, the scope of practice and roles fulfilled throughout history indicate a different narrative (Kerfoot, 2019). Appreciating the history of nursing requires critical thinking – to navigate through the conflicting recollections of a profession fraught with identity crisis, political discourse and battles for equality and recognition of its value in healthcare (Hunt, 2017). Nursing has fought hard to gain the respect and professional stature of modern practice. Explorations of the history of nursing reveal the multi-dimensional role that is to ‘nurse’ and how this influenced the development of a disaster specialty.
Method
Study design
Using a qualitative interpretive approach, an historical review was conducted. This approach considers the impact of the researcher on the analysis, as well as the relationships formed between sources and subsequent themes (Smythe and Spence, 2012). Smythe and Spence (2012) argue that history is interwoven inseparably with our culture, experiences, language and traditions. Alternatively, a narrative review is useful for considering an overview of a topic of interest, however, due to the ambiguity of nursing in disasters throughout history, a deeper understanding of the problem requires an interpretive approach. A hermeneutic approach was chosen to enable contextualisation of the relationship of the nursing profession and disasters, to enable interpretation of these parallel developments in order to develop an holistic understanding (Gadamer, 1989; Heidegger, 1962). By comparing these relationships, considering the impact of language throughout history, a deeper understanding of disaster nursing was possible.
Questions asked of the literature centred on challenging the authors’ perspectives of disaster nursing and if the literature altered these perspectives: • How is disaster nursing described and understood by the authors of the papers? • What is the nursing focus described – such as, goals for practice? • Is there agreement among authors or are there issues to be challenged? • What are the emerging themes, and do they fit in the 4 phases of the framework? If so, how? • Are there findings that do not fit in the framework?
Gadamer (1989) states that a person’s past, present and future influence interpretation, and our understanding; that is, we cannot consciously or unconsciously deny our historicity (Smythe and Spence, 2012). This approach recognises the limitations of a detached observer. That dialectical use of question and answer develops a critical understanding of the literature (Smythe and Spence, 2012).
Data collection
Primary sources were obtained as ‘first-hand accounts’ of experience and were published in contemporary journals (Given, 2008). Secondary data sources were publications that analysed or interpreted the original historical phenomenon (Given, 2008). The following databases were used: CINAHL, Medline, EBSCO, Psych INFO, Cochrane Library and SocINDEX. The ambiguity of nurses and their roles throughout history led to a broad search strategy.
Inclusion criteria
• English language • Publications 1780 – current • Notable figures of nursing that focus on disaster nursing • Articles reporting developments in the nursing profession in disaster management in its broad historical context
Exclusion criteria
• Book reviews • Course implementation papers (education focus) that lacked developmental/historical focus • Memorials
The following search terms and MESH headings were used: disaster* OR humanitarian* OR war AND nurse* OR nursing AND history OR historic* OR development. MESH headings were also used for the relevant databases: (MH ‘Disasters+’) and (MH ‘History of Nursing’).
The analysis was conducted applying the following principles: • Type of text • Authenticity of the source • Generation of themes through a process of questioning the texts, interpreting and examining theparts (themes) and their relationship with the whole (historical context and the current stages of disaster management)
Personal reflexivity
To understand how the authors’ personal subjectivity might have influenced the research exploration of the history of the concept of disaster nursing was necessary. It was important to acknowledge the ‘historically effected consciousness’ (Gadamer, 1989); that is, the effect experiences have on analysis. As a former military nurse, and disaster responder, the first author sympathised with the role of the nurse in a war or humanitarian crisis. The experiences of the co-authors were different and collectively brought shared perspectives in critical care and public health. More specifically, the authors were acutely aware of the challenges faced in providing care to a community when there is loss of logistics, necessities and the comforts of Western medicine. As a champion of the value nurses have in community health and disaster response, it cannot be denied that the authors felt passionate about the contribution of nurses to this field of practice. Gadamer (1989) argues that no individual is impartial to the influence of experience on their view of the world. In order to maintain the focus of the research, a conscious effort was made to focus on the evidence and evolving understanding of the history of the nursing profession in disasters through rigorous questioning of the data.
Results
The search strategy generated a total of 2228 references; 10 additional references resulted from disaster policy searching and a further 22 from hand searching. After exclusion of duplicates, 1572 titles were identified for further screening. A total of 1429 titles and abstracts were removed according to the exclusion criteria. This resulted in 144 full-text articles; nine full-text articles could not be retrieved, and 106 did not meet the inclusion criteria, leaving 29 references for analysis (Figure 1). PRISMA 2009 Flow Diagram (Searched: July 2020): 144 Full-Text Articles; 9 Full-Text Articles Could Not Be Retrieved, and 106 Did Not Meet the Inclusion Criteria, Leaving 29 References for Full-Text Analysis.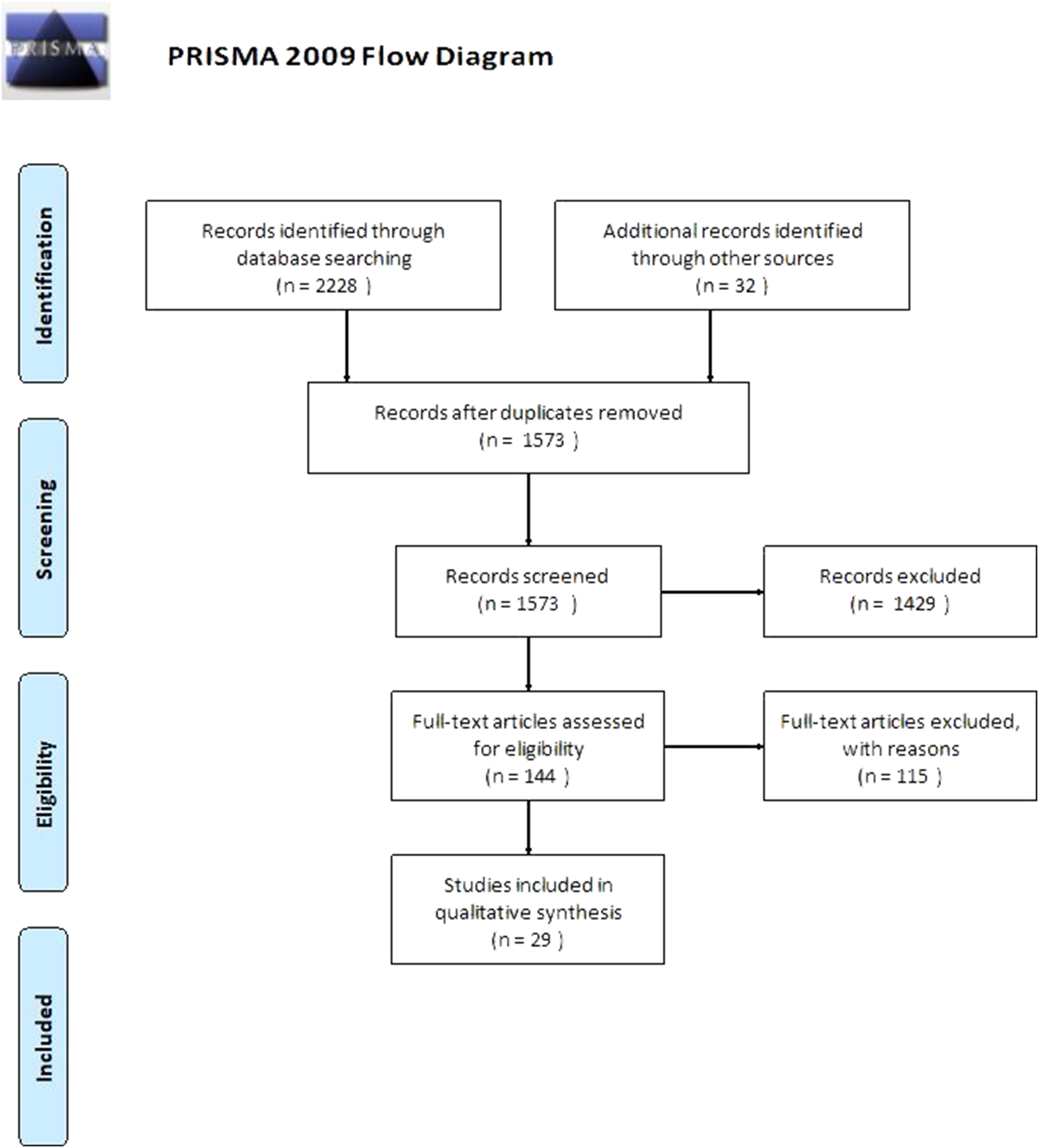
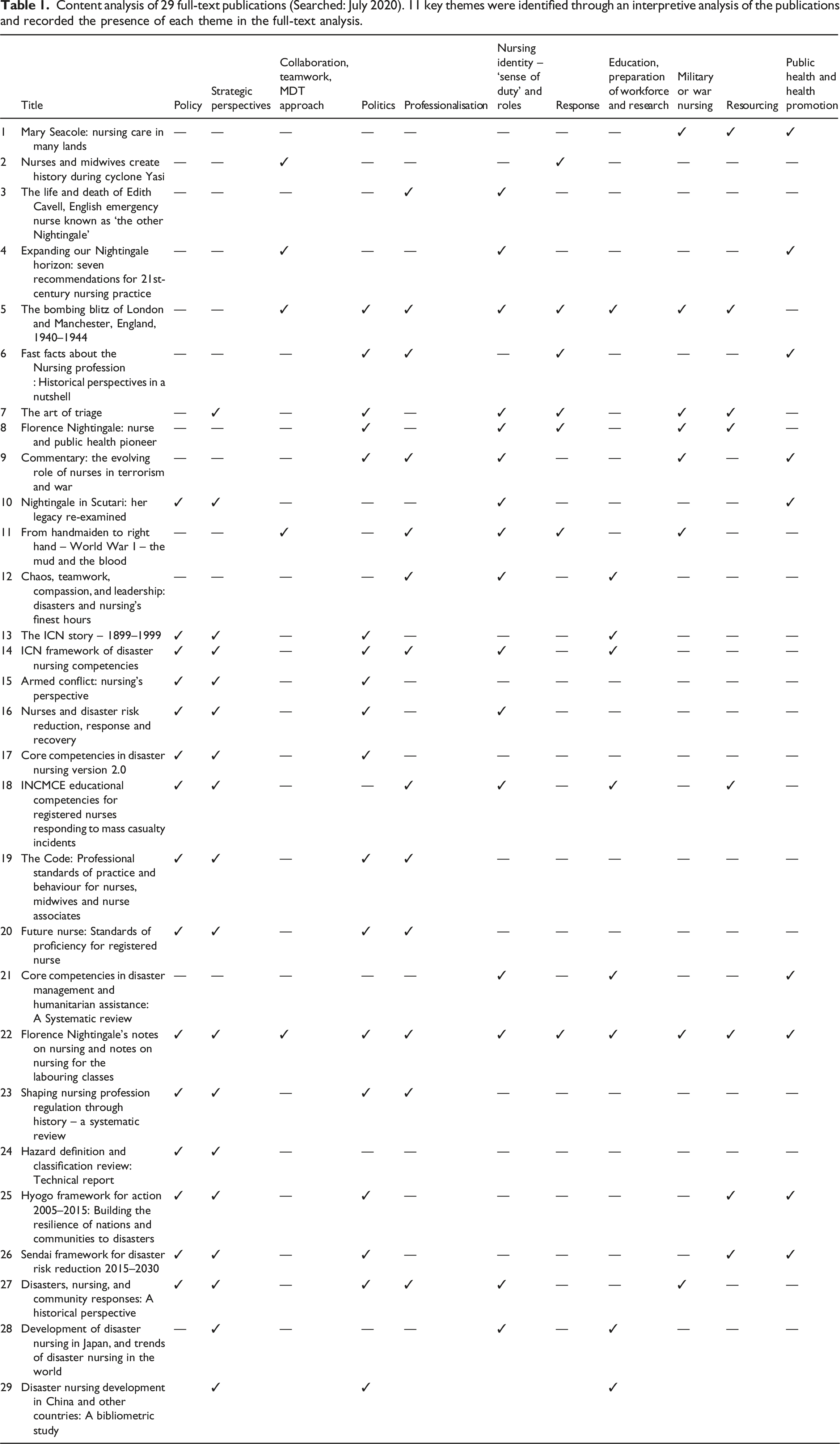
Of the results, three were systematic reviews /bibliometric studies (Ripoll Gallardo et al., 2015; Stievano et al., 2019; Zhang et al., 2018), nine peer reviewed (Anionwu, 2012; Arthur, 2006; Ellis, 2010; Gill and Gill, 2005; Holder, 2004; Kerfoot, 2019; Lynaugh and Brush, 1999; Wall, 2015; Yamamoto, 2013), five books or book chapters (Beck, 2010; Brooks, 2015; Hunt, 2017; Edwards, 2013; Skretkowicz, 2010), one news article (Queensland Nurses Union (QNU), 2011), one commentary (Garfield et al., 2003) and 10 policies /reports (ICN, 2009, 2012, 2019a, 2019b; International Nursing Coalition for Mass Casualty Education (INCMCE), 2003; Nursing and Midwifery Council, 2015; NMC, 2018; UN, 2005, 2015; UNDRR, 2020).
Content analysis of 29 full-text publications (Searched: July 2020). 11 key themes were identified through an interpretive analysis of the publications and recorded the presence of each theme in the full-text analysis.
Discussion
The diversity of the role of nursing lends itself towards flexibility, adaptability and selflessness (Kerfoot, 2019). Nurses’ roles are multi-dimensional and are often key in managing infectious diseases, social support, medical care and recovery/rehabilitation (Kerfoot, 2019). Despite the phases of disaster management emerging from the literature in the 21st century, they were key principles of disaster risk reduction throughout history (Sawalha, 2020). The literature focuses strongly on the preparedness and response phases, with an emerging reference to the role of the nurse in mitigation and recovery in modern practice (Table 1). This aligns to the increasing emphasis on disaster risk reduction and prevention in the last 30 years (UN, 2005, 2015). Despite the more recent contestation of the four-phased disaster cycle, it is still the most widely adopted approach to disaster response.
Mitigation
Florence Nightingale, undoubtably revolutionised the profession, thrusting it into the 20th Century (Beck, 2010; Ellis, 2010; Gill and Gill, 2005). Her ‘Notes on Nursing: What it is and what it is not’ moulded the future of modern-day nursing (Skretkowicz, 2010). Nightingale adapted clinical practice aligned to scientific developments on sanitation, food and hygiene, ventilation and swift administration of medication and treatment (Gill and Gill, 2005). This resulted in significant improvements in communicable disease transmission and associated death rates (e.g. dysentery and cholera) in military hospitals (Gill and Gill, 2005). Nightingale was an early adopter of the principles of modern disaster risk reduction and championed the role of the nurse as critical in this environment (Gill and Gill, 2005). This led to increased political awareness of the nurse; however, it took a further 150 years to recognise the specialty of disaster nursing (ICN, 2009).
Historically, nurses’ role in the mitigation phase was at an operational level in healthcare provision. More recently, nurses have an increased presence and political voice in strategic planning and response. Additionally, increasing global focus on health promotion and prevention through community empowerment, resilience and structural changes (World Health Organization, 1986) has ideally positioned contemporary disaster nurses to contribute effectively to the earlier phases of disaster response (Jackson et al., 2017). Disaster management strategies are increasingly more focused on the mitigation and prevention phases of disaster response.
Preparedness
The International Nursing Coalition for Mass Casualty Education (INCMCE) published the first recorded ‘disaster’ related competencies for nurses responding to mass casualty incidents early in the 21st century (INCMCE, 2003). This triggered the conception and partnership with the ICN in the publication of the disaster nursing competencies (ICN, 2009). Since then, there has been an exponential growth in disaster nursing research which has been adopted into continuing professional development (CPD) and curriculum development globally (Yamamoto, 2013; Zhang et al., 2018). Interestingly, there are notable rises in disaster nursing research following a disaster that has increased displacement of populations or damages to that community (Molassiotis et al., 2020). Disaster nursing research is anecdotal though, with little external validity – often focused on case studies, curriculum design and competency measurements (Zhang et al., 2018). Wall (2015) has extensively researched the history of disaster nursing, with a focus on case-study analysis, and transitions of nursing practice with the findings recognising the value of nursing in disaster response, rather than chronology of the specialty developments.
Politics and strategy were interwoven clearly throughout history, from Florence Nightingale, to modern-day warfare (Garfield et al., 2003). Politics emerged in two ways – in professionalisation and complexities of the disaster itself (Holder, 2004; Stievano et al., 2019). The progression of registration and educational developments at the turn of the 20th Century aligned with modern medical advancements (Stievano et al., 2019). An example of this is the 1918 Spanish Flu. This forced the refocus onto public health and health promotion whereby scientific developments focussed on treatment and prevention and was evident through the conception of the first influenza vaccine that was trialled in soldiers in preparation for World War Two (Wallace, 2020). Nurses often exploited the context of war to advance the notoriety and advancement of the profession (Garfield et al., 2003). Strategic developments relied heavily on political support and despite history criticising the role of individuals in influencing the profession, these were necessary drivers of progression (Stievano et al., 2019).
Florence Nightingale’s post-war achievements in improving nurse education, practice standards and the voice of nurses in the political domain had a more profound impact on the development of the profession (Beck, 2010). Alternatively, Anionwu (2012) explored the race and logistical challenges faced by Mary Seacole – a stark contrast to Florence Nightingale’s relationship with politics. Additionally, Edith Cavell’s nursing care ultimately changed the course of World War One when she sacrificed her life to uphold the principles of nursing and the utilitarian approach in disaster nursing – the greatest good for the greatest number, and help for all (Arthur, 2006).
It was not until 2009, that the ICN published the first standards for disaster nurses – over a century after Nightingale’s practice (ICN, 2009). The ICN Framework of Disaster Nursing Competencies was developed in consultation with key nations and organisations to support a global consensus and has recently been updated in 2019 (ICN, 2019a). Various national expectations were in existence, but had no consistency or benchmark, particularly for countries that lacked a response strategy (ICN, 2019a; Ripoll Gallardo et al., 2015). This paved the way for disaster nursing research to begin to emerge.
The NMC updated ‘Future nurse: Standards of proficiency for registered nurses’ (2018) demonstrate its adoption of this with the inclusion of disaster terminology for the first time in history. Whilst it is not explicit in its description of disaster management itself, the inclusion of managing and prioritising care in reference to a major incident and global health patterns, sparks opportunity for inclusion in undergraduate education and the nursing profession for advancing disaster preparedness in the United Kingdom (UK) (NMC, 2018).
Response
The literature focused predominantly on the response phase as this is where the research and historical accounts laid (Table 1). Nursing in crisis and conflict was arguably first documented by Nightingale and Seacole during the Crimean War in the mid-19th Century. The Crimean War is considered a pivotal historical point in the nursing profession where Nightingale practised managing patients in appalling environments and field hospitals (Anionwu, 2012; Gill and Gill, 2005). The provision of nursing care by these two individuals, were to preserve the fighting force and improve care and outcomes under dire circumstances (Anionwu, 2012; Gill and Gill, 2005). The utilitarian approach (greatest good for the greatest number) to healthcare provision in a disaster, emphasises the need to consider a more strategic perspective in approaching nursing care (Brooks, 2015; Kerfoot, 2019). Nightingale was a notable example of this, examining the impact hygiene, ventilation and hydration had on the statistical outcomes of survivability (Ellis, 2010). Additionally, ethics are challenged by disaster situations; for example, traditional ethical frameworks are difficult to adopt in a disaster as that situation differs from the everyday (Komenská, 2016). Where rigorous ethical frameworks exist within registration bodies such as the NMC, a disaster can cause ethical frustration through the alteration to decision-making and provision of care (Komenská, 2016).
The literature frequently identified disaster nursing with a ‘sense of duty’ and multi-dimensional roles (Arthur, 2006; Brooks, 2015; Skretkowicz, 2010). And this was often used synonymously with resilience and adaptability (Arthur, 2006; Queensland Nurses Union (QNU), 2011).
Recovery
The rise of NGOs in the mid-19th Century such as the International Federation of Red Cross and Crescent Societies (IFRC) and International Committee of Red Cross (ICRC), saw the political nature of health and disasters raised strategically (Wall, 2015). This was a significant step in humanitarianism and refocusing disaster management away from its military roots – instead NGOs aimed to provide care to all, regardless of political position or identity (Wall, 2015). This was amid the political developments globally with the formation of the ICN in 1899, publication of the Treaty of Geneva in 1925 and formation of the UN in 1945 (Lynaugh and Brush, 1999). It was not until April 1948, that the WHO was formed as a single intergovernmental health organisation. Despite the ICN’s attempt to raise awareness of the refugee and disaster needs globally in the 1960s, it was not until many decades later that both national and international organisations were able to adopt this concept (Lynaugh and Brush, 1999; Ripoll Gallardo et al., 2015; Stievano et al., 2019). Continuation of the development of NGOs saw the conception of Médecins Sans Frontières (MSF) in 1968, and other private aid organisations, where emergency medical aid was provided amid conflict and major disasters (Wall, 2015) (Box 1).
• 1859: Florence Nightingale’s ‘Notes on Nursing: What it is and what it is not’ published • 1863: Birth of the Red Cross movement • 1887: Ethel Gordon Fenwick founded Royal British Nurses Association (RBNA). • 1899 - 1909: ICN, the foundation years • 1916: The Royal College of Nursing (RCN) founded • 1919: The Nurses Registration Act (UK) passed • 1920: General Nursing Council (UK) formed • 1945: Formation of the United Nations (UN) • 1948: Formation of the World Health Organization, ; the ICN and WHO began collaboration • 1976: World Association of Disaster and Emergency Medicine (WADEM) established • 1994: International Classification for Nursing Practice (ICNP) – ICN • 2000: UN International Strategy for Disaster Risk Reduction (UNISDR) • 2003: International Nursing Coalition for Mass Casualty Education (INCMCE) published the competencies for registered nurses responding to mass casualty incidents • 2005–2015: Hyogo Framework for Action (UN) • 2008: World Society of Disaster Nurses (WSDN) established in response to increasing disasters and the nurse’s role in this globally • 2009: ICN disaster nursing competency framework • 2015-2030: The Sendai Framework for Disaster Risk Reduction (UN) • 2018: NMC future nurse: Standards of proficiency for registered nurses published • 2019: ICN disaster nursing competencies 2.0 publishedBox 1. Key historical milestones of disaster management, global health and disaster nursing listed chronologically.
Nurses are increasingly going beyond their clinical role – advancing into the political and strategic arena (Garfield et al., 2003; Wall, 2015). This aligns with all 4 phases of disaster management and further emphasises the significance of nursing practice on the outcomes of a disaster. Nurses’ multi-dimensional and adaptive capabilities lend themselves to a diverse profession capable of effecting change – for this to occur, nurses’ voices must be heard at a strategic level to cascade down to the clinical application (Wall, 2015). Their unique access to the population and ability to gauge awareness of the populations’ strengths and weaknesses, allow appropriate planning and support to promote recovery and mitigation in any disaster (ICN, 2009; 2019a). Disaster nursing requires resilience, adaptability and innovation to overcome challenges in logistics and healthcare provision (ICN, 2019a; Kerfoot, 2019; Wall, 2015).
Conclusion
Nurses have spent centuries building the trust and legitimacy of the profession (Garfield et al., 2003; Wall, 2015). The invisibility of nursing developed alongside other professions in response to need and the public recognition of disaster nursing did not eventuate until more recently. All nurses are disaster nurses and planners, and it is in times of disaster that we truly see the role of the nurse emerge (Wall, 2015). This was demonstrated repeatedly since the beginning of the COVID-19 pandemic, where ordinary nurses have embraced the challenges of disaster response and continued to adapt to provide the highest possible care to their communities (Mao et al., 2021). The value placed on nurses during disasters highlights the crucial roles we fulfil during challenging and often unimaginable circumstances. The core purpose of disaster nursing is to minimise the impact of the disaster on the patients or communities that nurses are entrusted to care for – to maximise their potential and minimise harm (ICN, 2019a; Wall, 2015). Disaster nursing goes beyond the expectations of a registered nurse – whereby clinical practice is considered phased and cyclical throughout the phases of disaster response (ICN, 2019a). The responsibilities of a disaster nurse encompass wider community health promotion, critical decision-making beyond the individual patient, resilience and ethical challenges (ICN, 2019a; Jackson et al., 2017; Wall, 2015). Whilst significant advancements have emerged in the last 30 years, further research, and representation of the profession at a strategic and political level could improve the mitigation, preparedness, response and recovery of any community.
Disaster nursing responsibilities go beyond the disaster; they encompass public health, health promotion and community resilience, critical decision-making and resourcefulness. Nurses are positioned to influence strategic and operational development of disaster nursing policy and procedures; to enhance awareness of the unique contribution of disaster nurses to global health promotion and disaster response. Further research in the field of disaster nursing is required to examine the influences of nurses strategically in policy development, strategic and operational response, preparation of workforce, education development in modern disaster nursing and role profiles within the four phases of disaster response.Key points for policy, practice and/or research
Footnotes
Declaration of conflicting interests
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics
Ethical permissions were not required for this paper. No human subjects were involved, and no primary data were collected.