
Abstract
Background
Registered nurses are ‘critical’ to population health, international responses to emergencies, epidemics and disasters. Retention of registered nurses (RNs) is an international nursing priority. In England, RNs are encouraged to be involved in improving healthcare services. This benefits quality of care, operational and financial performance. However, RN involvement in improvement may reduce RN retention. It is important to understand this relationship when developing effective RN retention strategies.
Aim
The purpose of this research is to describe possible relationships between RN involvement in improving healthcare services and RN retention, using published 2018 data for National Health Service (NHS) Trusts in England.
Methods
The relationship between RN involvement in improving healthcare services and RN retention was explored using a correlational design, involving secondary data from the annual NHS Staff Survey and Model Hospital.
Results
In mental health NHS Trusts in England, a statistically significant, positive correlation of 0.24 was found between RN ‘ab(ility) to make suggestions for improvement’ and RN retention. In mental health NHS Trusts, a statistically significant correlation of 0.278 was found between RNs ‘making improvements happen’ and RN retention. In acute NHS Trusts in England, a statistically significant, negative correlation of −0.15 was identified between RNs ‘mak(ing) improvements happen’ and RN retention.
Conclusions
The findings suggest that RN retention factors in mental health and acute NHS Trusts differ from community and specialist NHS Trusts in England. This is an important consideration for national RN retention programmes as a single approach to RN retention may not be effective across all healthcare settings.
Keywords
Introduction
The World Health Organisation (WHO) predicts a shortfall of 5.7 million registered nurses (RNs) worldwide by 2030 (WHO, 2020). RN retention is a priority internationally and for the United Kingdom’s (UK) National Health Service (NHS) (National Audit Office, 2020). Over 26 thousand RNs left NHS organisations in the year May 2017–June 2018 (NHS Digital, 2019). RN retention is influenced by many factors. Involving RNs in improvement offers exposure to inclusion, teamwork and improvement of the quality of patient care, which have been shown to positively influence retention. Jones et al. (2015) recommended that newly qualified RNs be involved in improvement projects to increase RN retention. This study identified that newly qualified RNs experienced job satisfaction from feeling valued, having development opportunities and a clear career structure. Being involved in improvement can lead to a sense of feeling valued and professional development, both of which were identified as retention factors (Jones et al., 2015). NHS policy (Department of Health, 2015) and nursing regulation (NMC, 2018) advocate the involvement of RNs in improvement to achieve high quality care and effective use of resources. However, there is limited understanding regarding how this involvement influences RN retention. This paper responds to this gap in knowledge and reports original research which analyses published data and describes the relationship between RN involvement in improving healthcare services and RN retention in England.
Literature review
An international literature search identified that RN retention is influenced by working environment, organisational culture and demographic characteristics. RN retention factors included strong nurse-physician relationships, an inclusive managerial style and development opportunities (Van den Heede et al., 2013). Perceived quality of care influenced RN retention (Van den Heede et al., 2013). Newman and Maylor (2002) noted that poor patient satisfaction negatively influenced retention and Wu et al. (2019) identified that satisfaction from helping patients recover was positively associated with an intention to stay in the profession. Koppel et al. (2017) increased RN retention by providing growth opportunities and support for RNs who were considering resignation, though figures are not provided. Karlsson et al. (2019) noted that a ‘chance for renewal’ (Karlsson et al., 2019: 1359) through learning new skills, positively influenced RN intention to stay with an employer.
RNs left an organisation due to concern over staffing levels, salary, issues with their own health or other family members’ needs (Estryn-Behar et al., 2010). Sellgren et al. (2009) identified that RN turnover was lower in smaller units, outpatients and day care, and Dieleman et al. (2011) identified how RN retention in rural areas, worldwide, could be improved, although why RN retention was difficult in rural areas was not explored. RN ‘stayers’ had a mean age of 2 years older than ‘leavers’ and had been employed with an organisation for a mean of 2 years less than the ‘leavers’ (Estryn-Behar et al., 2010: 168). Perhaps due to the complicated nature of retention, RN retention appeared to be highest when more than one retention strategy is used (Lartey et al., 2014: 1027).
RN involvement in improvement provides an opportunity for interprofessional teamwork with the shared goal of using information to focus on patient care and measure improvement results (Eriksson et al., 2016). Involvement in improvement is also a learning experience and facilitates development of trust and understanding between professional groups (Eriksson et al., 2016). Organisational context is highlighted by Dixon-Woods (2019) as important for any improvement initiative to be successful, with ‘professional coalitions of the willing’ being more influential than a ‘top down’ approach to improvement (Dixon Woods, 2019: 2). It is clear that there is some overlap between RN retention factors and the opportunities provided by involvement in improvement.
Published literature uses the terms ‘retention, turnover and intention to leave’ with no consistent term for ‘retention’ being used, which made interpretation of the papers complex. Several studies associated RN involvement in improvement with increased RN retention. Shared decision making, recognition and staff engagement by inclusive leaders were associated with increased RN retention (Karlsson et al., 2019; Harrison and Zavotsky, 2018; Koppel et al., 2017; Rondeau and Wagar, 2016; Sawasky and Enns (2012)). Murff and Defer (2010) reduced RN turnover by 5% during a local improvement project. Boettcher et al. (2019) reduced new RN turnover by 33% using Lean to re-design RN education and mentorship. Research by Karsh et al. (2005) identified a statistically significant negative correlation (r = −0.33, p < 0.05) between ‘organisation quality improvement environment and turnover intention’ in care homes (Karsh et al. 2005: 1268).
In contrast to the findings regarding a positive relationship between RN involvement in improvement and RN retention, McGuire and Kennerly (2006) identified that RN retention was statistically significantly negatively correlated (r = −0.111, p < 0.01) with ‘intellectual stimulation’ (McGuire and Kennerly, 2006: 184). These unexpected findings were not fully explored by the authors. In addition, Rutherford et al. (2009) and Brunges and Foley-Brinza (2014) showed that RN retention changed during the course of an improvement project. Rutherford et al. (2009) demonstrated an initial reduction in RN retention which then increased over 4 years, while Brunges and Foley-Brinza (2014) experienced a reduced RN retention which later increased over 3 years. These findings warrant further investigation.
To summarise, the majority of international studies identified a positive relationship between RN involvement in improvement and RN retention. The studies which identified a negative (or changing) relationship between RN involvement in improvement and RN retention were set in the United States. NHS policy encourages the involvement of NHS staff in improving services (Department of Health, 2015), which makes understanding the relationship between the two variables, important. The research outlined in this paper, aims to describe this relationship and contributes important new information to the topic.
Methodology
The aim of this research was to investigate possible relationships between RN involvement in improving healthcare services and RN retention in England. Information regarding NHS staff experience including involvement in improvement is publicly available from the annual NHS Staff Survey (NHS England, 2018a). The actual number of staff leaving individual NHS organisations is recorded by NHS Trusts in the NHS Electronic Staff Record (ESR) and NHS Improvement publish these data on the Model Hospital (NHS Improvement, 2019). The Model Hospital is a ‘free digital tool (which) enables Trusts to compare their productivity and identify opportunities to improve’ (NHS Improvement, 2019).
Research design
Summary of RN respondents to NHS Staff Survey 2018.
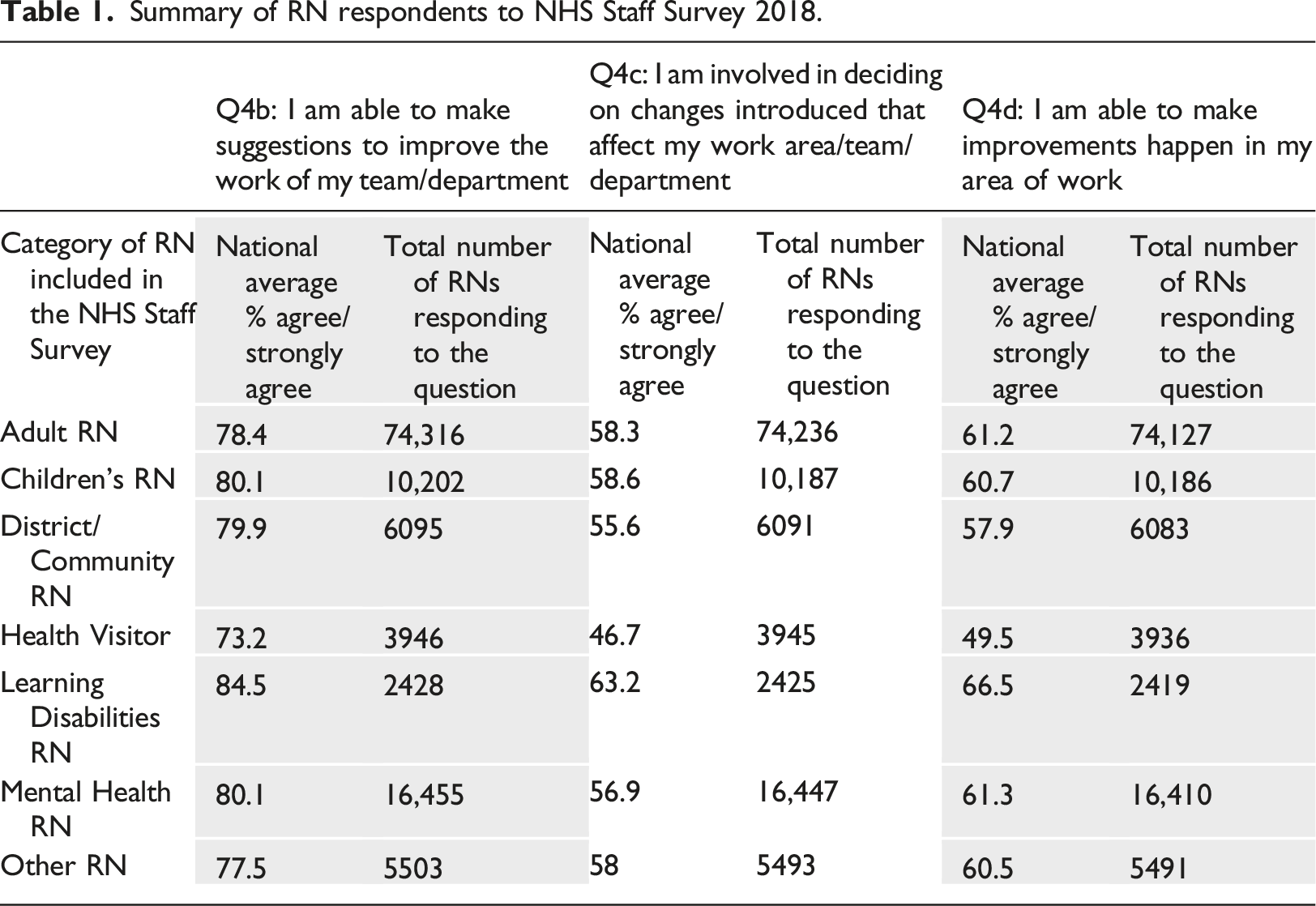
It was noted that Health Visitors consistently reported the lowest ‘agree/strongly agree’ to NHS Staff Survey questions 4b-4d. Learning Disabilities RNs consistently reported the highest ‘agree/strongly agree’ to NHS Staff Survey questions related to involvement in improvement. RNs who classified themselves as more than one type of RN, were allocated by NHS England into the category ‘other’ (NHS England, 2018b: 5).
Data collection
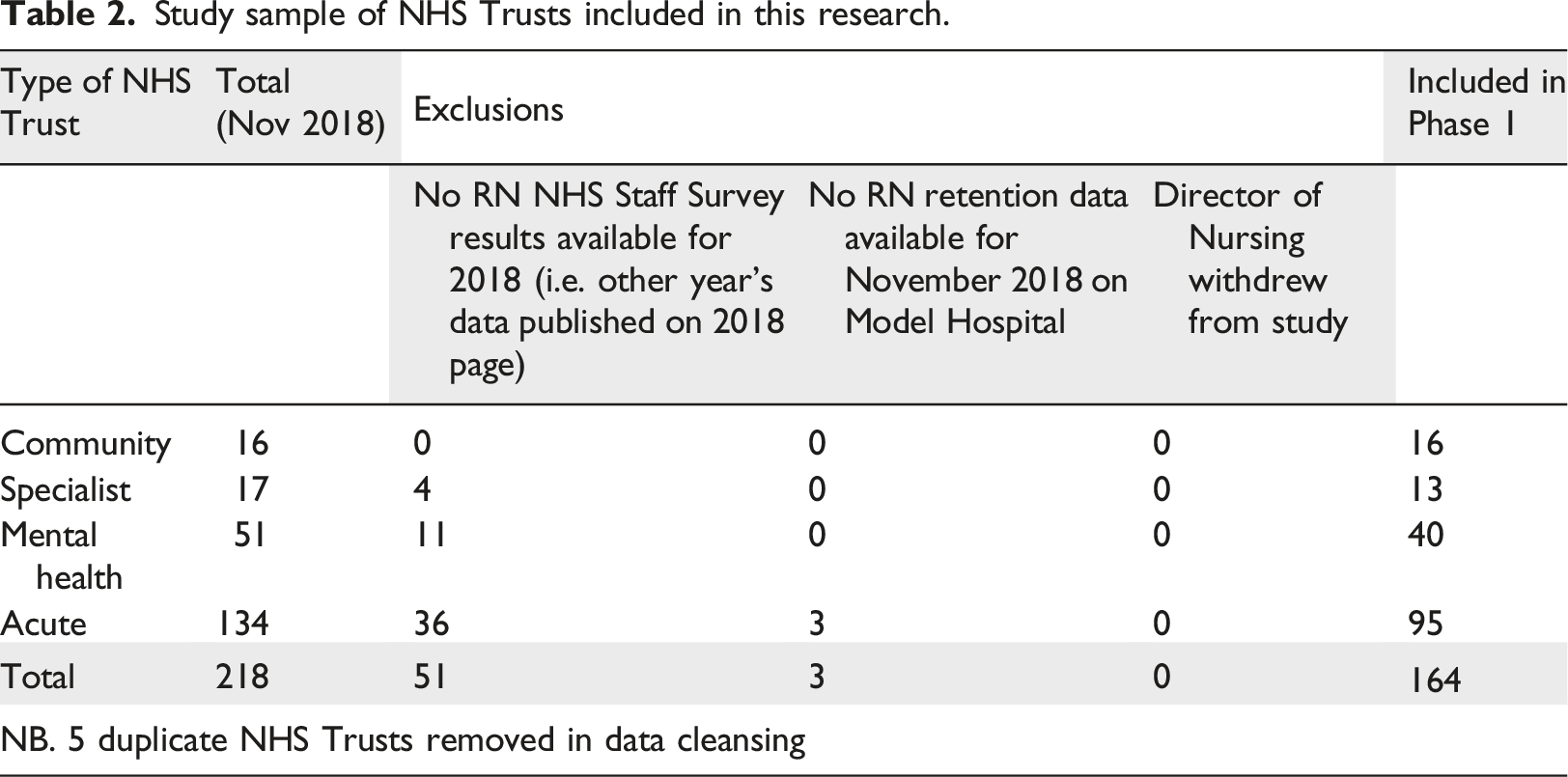
Study sample of NHS Trusts included in this research.
Involvement in improvement
The mandatory 2018 NHS Staff Survey core questionnaire included the following questions related to involvement in improving healthcare services.
Q4b: I am able to make suggestions to improve the work of my team/ department.
Q4c: I am involved in deciding on changes introduced that affect my work area/ team/ department.
Q4d: I am able to make improvements happen in my area of work.
Q4b and Q4c relate to the process of testing changes to NHS services and Q4d relates to successful results from improvement. NHS England collates individual responses of ‘agree/strongly agree’ to each NHS Staff Survey question and published as a percentage for each staff group every NHS Trust in England (NHS England, 2018a). Cronbach’s alpha was 0.793, confirming that the three questions were interrelated. Analysis was undertaken regarding the correlation between Q4b, Q4c, Q4d and RN retention to assess whether individual aspects of the process of involvement in improvement was influential.
It was noted that RNs employed by acute and specialist NHS Trusts tended to be from three types/fields of nursing (adult, children and ‘other’ types of RN). RNs employed by community and mental health NHS Trusts, tended to be from six types/fields of nursing (adult, children, mental health, learning disabilities fields, district nurses and health visitors).
RN retention
Retention rate for ‘nurses and health visitors’ is provided on Model Hospital for each NHS Trust using data from ESR (NHS Improvement, 2019), though the method for this calculation is not explained.
Data analysis
Descriptive statistical analysis was conducted for each type of NHS Trust using IBM SPSS v26, with simple scatterplots and linear trendlines created using Microsoft Excel. Microsoft Excel applied a linear trendline to the scatterplots using the ‘least squares fit for a line’ (Microsoft Corporation, 2020). A Shapiro-Wilk test of normality showed that data were not normally distributed (p < 0.05) with the need to use a non-parametric test to calculate the correlation coefficient. RN retention data for community, mental health and acute Trusts had a negative skew, which may have been due to a national focus on improving RN retention. Specialist Trust data had a negative skew for Q4b, Q4c and the composite score. IBM SPSS v 26’s Kendall’s tau was used as the sample sizes were small and there were visual outliers (Field, 2018). Outliers were included in the data analysis. Kendall does not provide effect size measures for these correlation coefficients (Kendall, 1938).
Results
Descriptive data analysis of RN involvement in improvement and RN retention.
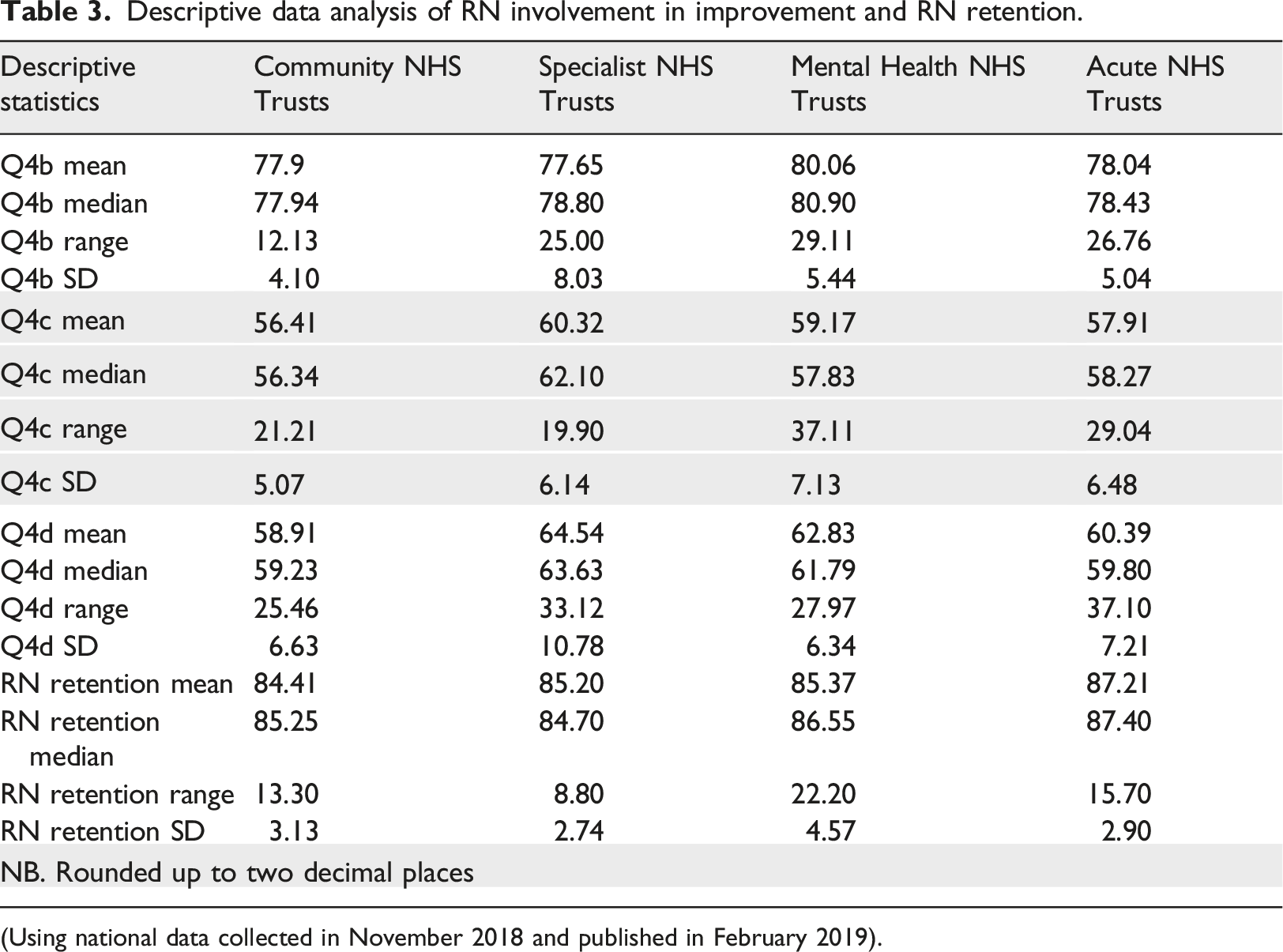
(Using national data collected in November 2018 and published in February 2019).
Analysis also included simple scatterplots (Figures 1–4) with the trendline highlighted and outliers marked with a grey circle. These data demonstrated a difference between type of NHS Trust. Simple scatterplots for community NHS Trusts. Simple scatterplots for specialist NHS Trusts. Simple scatterplots for mental health community NHS Trusts. Simple scatterplots for acute NHS Trust.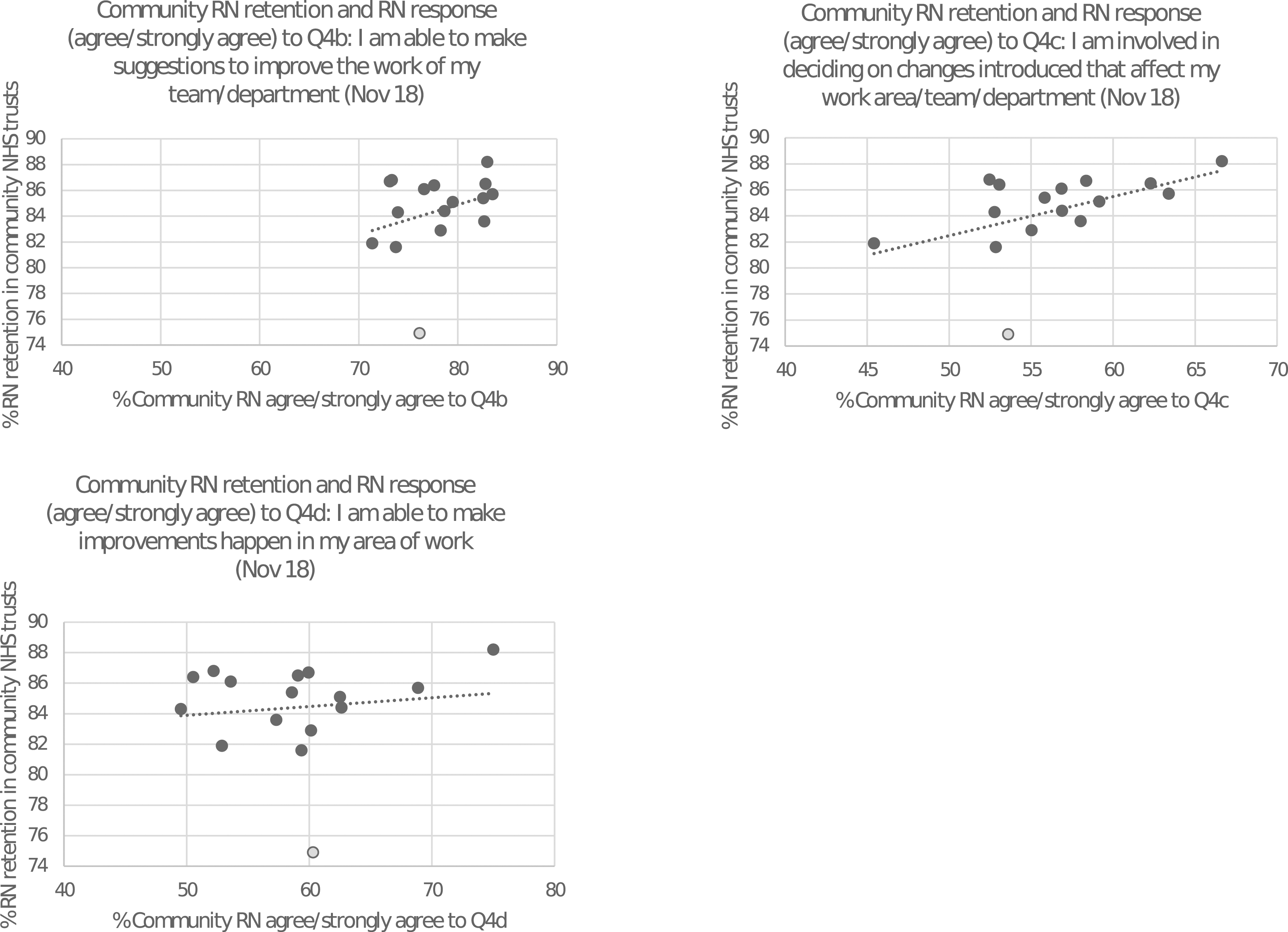
RN Involvement in improvement and RN retention (using Kendall’s tau).
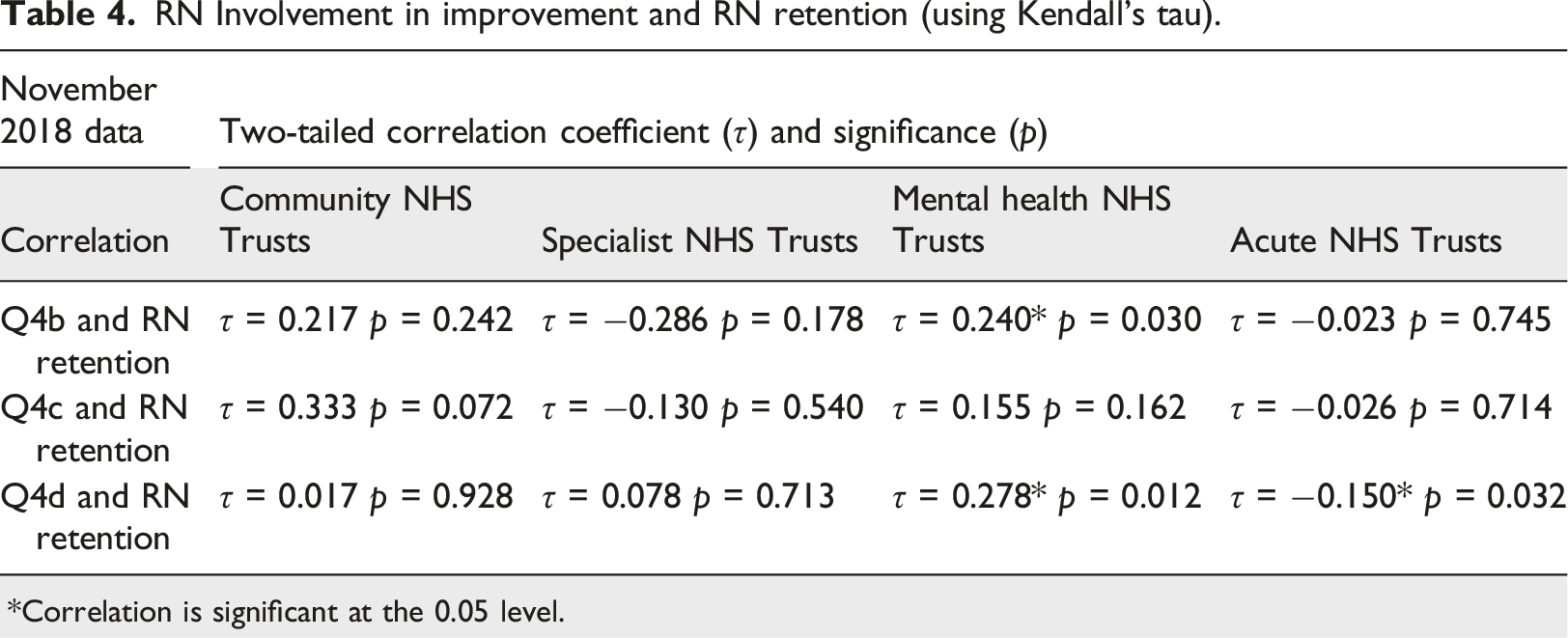
*Correlation is significant at the 0.05 level.
Community NHS Trusts
The simple scatterplots for community NHS Trusts are provided in Figure 1. The trendline showed a positive relationship between the two variables. RN retention was lowest in the outlier marked with a grey circle and this was the same NHS Trust (C2) for each scatterplot.
Table 4 shows that there were no statistically significant correlations between Q4b, Q4c, Q4d and RN retention in community NHS Trusts.
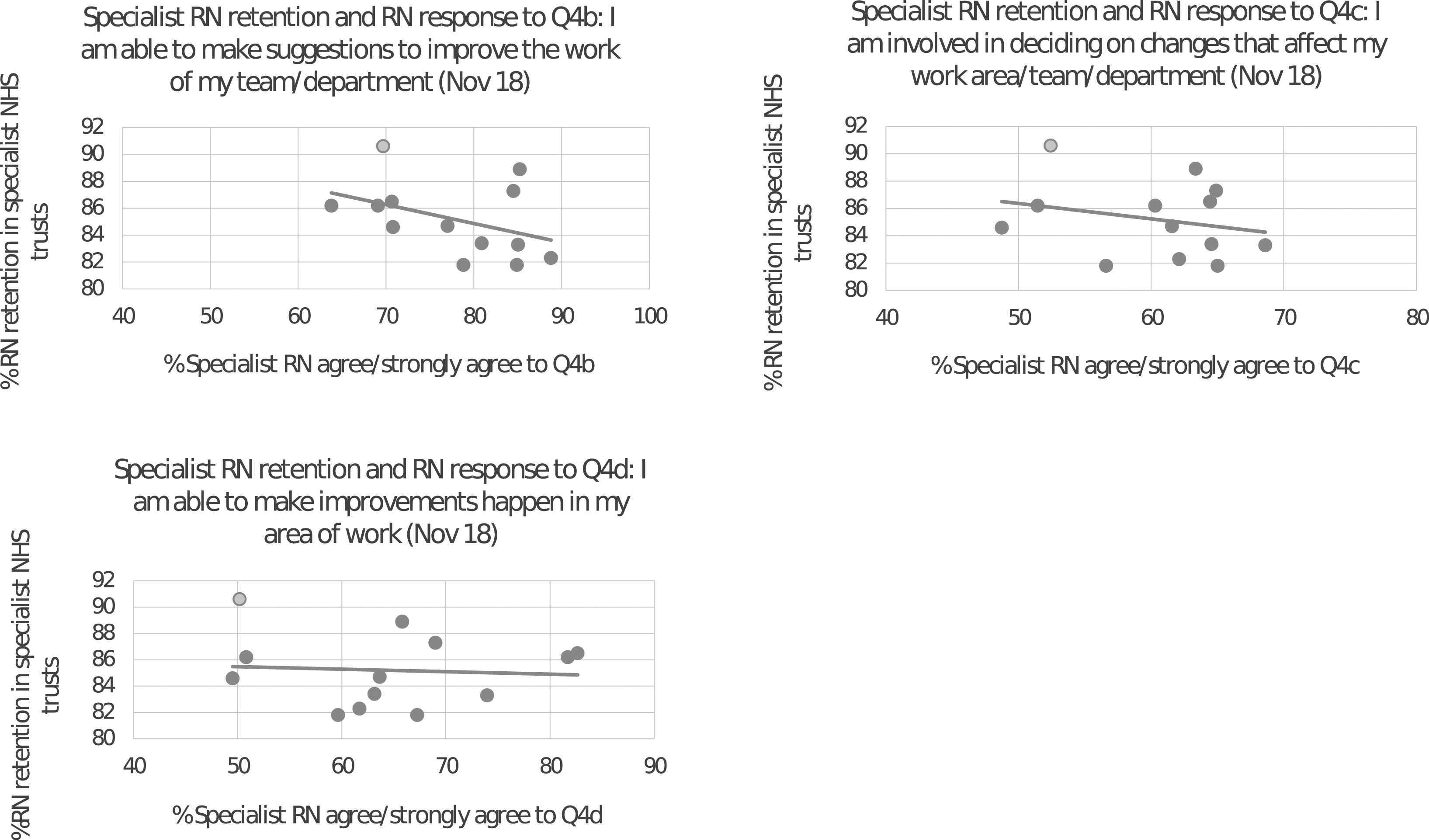
Specialist NHS Trusts
The simple scatterplots for specialist NHS Trusts are provided in Figure 2. The trendline showed a negative relationship between the two variables. RN retention was higher in the outlier marked with a grey circle and this was the same NHS Trust (S3) for each scatterplot.
Table 4 shows that there were no statistically significant correlations between Q4b, Q4c, Q4d and RN retention in specialist NHS Trusts.
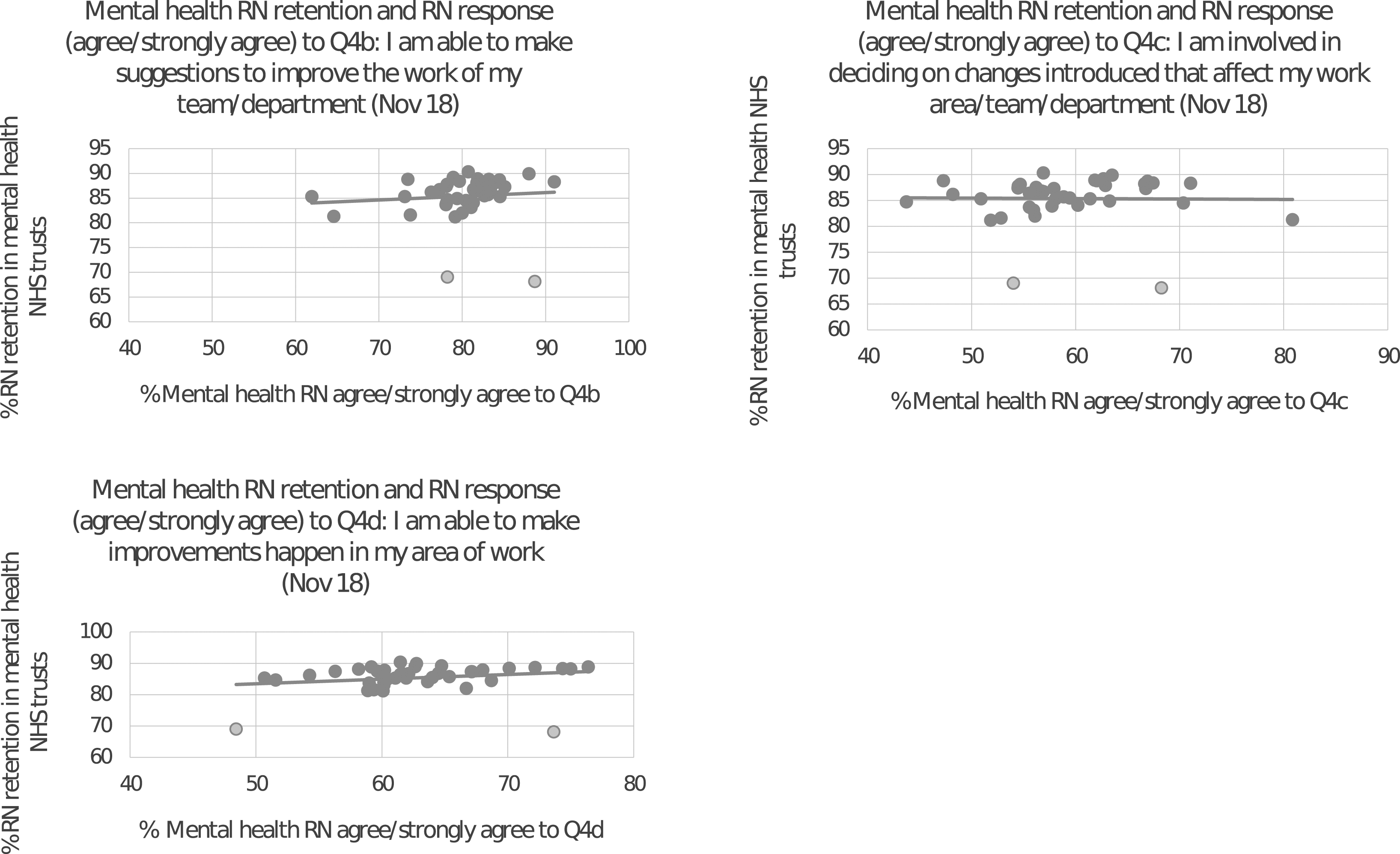
Mental health NHS Trusts
The simple scatterplots for mental health NHS Trusts are provided in Figure 3. The trendline showed a slightly positive relationship between the two variables. The outliers are marked with a grey circle. Outliers for each scatterplot were different. M38 was an outlier on all scatterplots. M10 was an outlier for Q4b and M14 was an outlier for Q4c, Q4d.
Table 4 shows that there was a positive correlation (
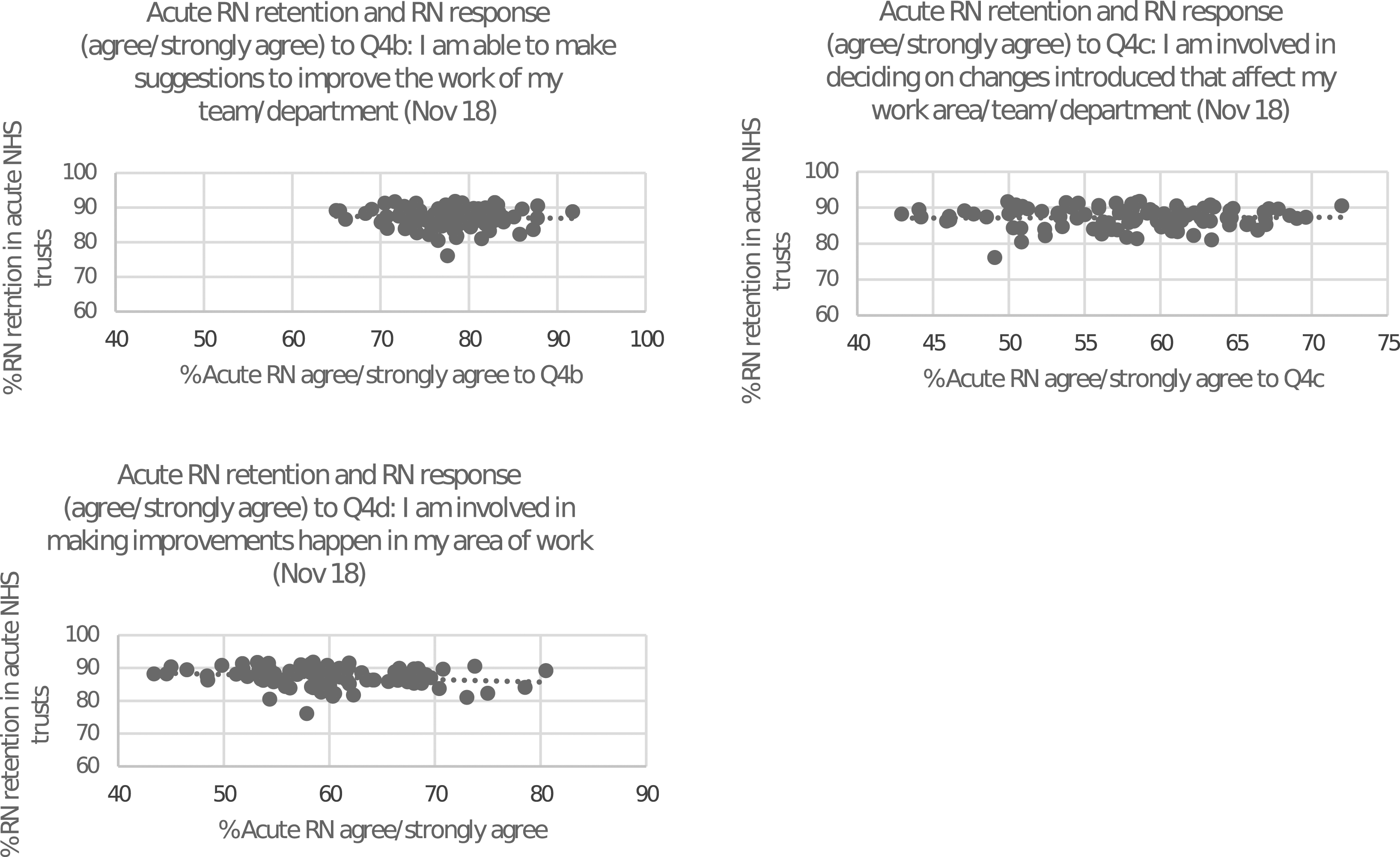
Acute NHS Trusts
The simple scatterplots for acute NHS Trusts are provided in Figure 4. The trendline showed a linear relationship between the two variables. There were no outliers.
Table 4 shows that there was a negative correlation (
Discussion
The aim of this research was to explore the relationship between RN involvement in improving healthcare services and RN retention in NHS Trusts in England, using 2018 data. The findings suggest that RN retention factors differ across types of NHS Trusts.
In mental health NHS Trusts, there was a statistically significant positive correlation between RN ‘ability to make suggestions to improve the work of teams/departments’ (NHSE, 2018a RN retention. In mental health NHS Trusts, there was also a statistically significant positive correlation between ‘mak(ing) improvements happen’ (NHSE, 2018a) and RN retention. The respondents from mental health NHS Trusts to the NHS Staff Survey in 2018, were from the same fields of nursing as community NHS Trusts. This suggests that the field/type of RN employed in mental health NHS Trusts may not be the contributing factor to the statistically significant results. The organisational culture in mental health NHS Trusts in England may support the retention factors of strong working relationships, development opportunities and satisfaction from delivering high quality care identified by Van den Heede et al. (2013) which also are integral to involvement in improvement (Eriksson et al., 2016). None of the published studies took place in mental health settings.
In acute NHS Trusts, there was a statistically significant negative correlation between RN ‘mak(ing) improvements happen’ (NHSE, 2018a) and RN retention. This finding could overshadow the positive benefits of involving RNs in improving healthcare services identified by Robinson and Gelling (2019). Directors of Nursing in acute NHS Trusts may be reluctant to encourage RNs to become involved in improving healthcare services if there is a risk that this may result in reduced RN retention.
These are important issues for nursing policy makers and local nursing leaders to understand. Further research to gain insight into how individual RNs view their experiences of being involved in improving healthcare services and whether those experiences influence the decision to stay with a current employer, is imperative.
There were limitations to using existing published data, including difficulty in data manipulation, necessitating development of the composite involvement in improvement score. Model Hospital relies on accurate recording of RNs who leave NHS Trust employment. The small sample sizes of each type of NHS Trust (as opposed to the number of RNs who took part), particularly specialist NHS Trusts, may have limited the ability to identify significant relationships between the variables. Individual RN level data are not provided by the NHS Staff Survey results (NHSE, 2018a).
Conclusion
This research involved an estimated 88,000 RNs who had been involved in improvement and were employed by 164 NHS Trusts in England. In mental health NHS Trusts in England, a statistically significant, positive correlation of 0.24 was found between RN ‘ab(ility) to make suggestions for improvement’ (NHSE, 2018a) and RN retention. In mental health NHS Trusts, a statistically significant correlation of 0.278 was found between RNs ‘making improvements happen’ (NHSE, 2018a) and RN retention. In acute NHS Trusts in England, a statistically significant, negative correlation of −0.15 was identified between RNs ‘mak(ing) improvements happen’ (NHSE, 2018a) and RN retention.
It is not possible to ascertain whether these differences were due to type/field of RN, the teams in which RNs worked, organisation’s culture, patient or service user differences.
It is recommended that an in-depth qualitative study is under-taken to understand what ‘involvement in improvement’ means to RNs and the relationship between RN involvement and RN improvement from the perspectives of RNs working in mental health and acute NHS Ttrusts in England. Understanding whether the experience of being involved in improvement influences RNs’ intention to stay with their employer, is vital to influence nursing practice, national nursing retention policy and local nursing strategy. In addition, comparison of the findings from this research (using 2018 data) with data from 2020, would facilitate understanding the impact of Covid-19 on RN involvement in improvement and RN retention.
Policy: A single national RN retention programme may not be appropriate across all types of healthcare organisation. Practice: There may be a positive personal impact for RNs who leave an organisation and their improvement skills may benefit patients and staff in a new organisation. Research: Existing published data provides accessible information for research.Key points for policy, practice and/or research
Footnotes
Acknowledgements
Thanks to Dr Ruth May, Chief Nursing Officer for England, Professor Mark Radford, Chief Nurse for Health Education England/ Deputy Chief Nursing Officer and Sue Tranka, Deputy Chief Nursing Officer, for their support.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jane Robinson is employed by NHS England and NHS Improvement.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NHS England and NHS Improvement provided 50% funding for this research.
Ethical approval
This research had ethical approval from Anglia Ruskin University’s Ethics Committee (NM-SREP-10-001) was approved on 18 October 2019.