
Abstract
Background
In England, although The National Institute of Health and Care Excellence recommends that patients’ religious beliefs should be incorporated into individual healthcare plans, these components are often neglected in diabetes management care plans. A literature review identified a paucity of research regarding how the spirituality of British people may influence their approach to their self-management of type 2 diabetes (T2D).
Aims
To explore how the spirituality of a small group of adults with T2D, living in England, influenced their coping strategies and self-management of diet and exercise.
Methods
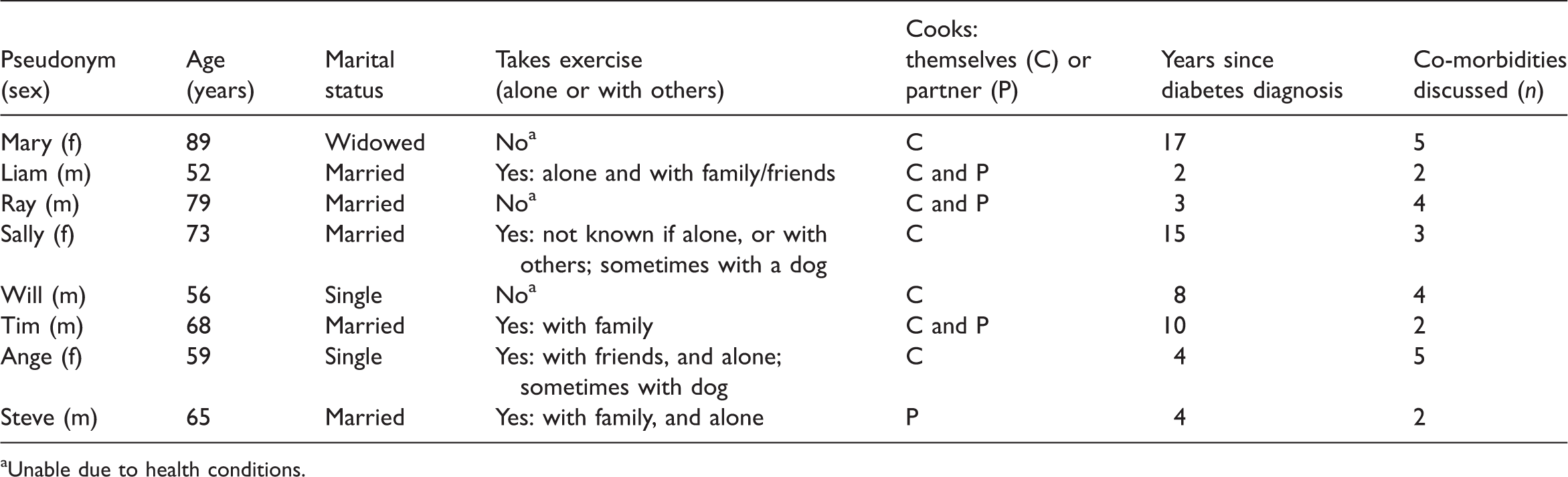
Biographic Narrative Interpretive Method of two interviews per participant and thematic analysis for data interrogation (n = 8). Data as glycated haemoglobin, living situation, age, length of time since T2D diagnosis, body mass index and diabetic medicines contextualised the interview data.
Results
Participants’ spirituality, health beliefs, coping and sense of responsibility for T2D self-management overlapped in complex layers. Three themes were generated: (a) spirituality influences expectations in life; (b) beliefs influence coping styles of diabetes self-management; and (c) responsibility influences diabetes self-management. A model was created to assist nurses in addressing these components.
Conclusion
Nurses should consider how patients’ self-management of T2D may be influenced by their spirituality, health beliefs, coping and sense of responsibility.
Introduction
Research analysing how the self-management of people with type 2 diabetes (T2D) is influenced by their spirituality has predominantly focused on African Americans, with a paucity of research involving British participants (Duke and Wigley, 2016). British people are citizens of the United Kingdom (UK) of Great Britain and Northern Ireland, the British Overseas Territories, and the Crown dependencies. The aim of this study was to explore how the spirituality of eight adults with T2D, who live in England (one of the countries of the UK) influenced their coping and self-management of T2D. A model is given for nurses to consider how the self-management of patients with T2D may be influenced by their spirituality, coping and responsibility.
Background
Type 2 Diabetes (T2D)
T2D is a lifelong condition involving the body’s inefficient use of insulin, where rising blood glucose levels can damage the body. Complications of poorly controlled diabetes may result in fatal and non-fatal strokes (Chen et al., 2016) and kidney disease (Diabetes.co.uk, 2017). In addition, sexual dysfunction (Malavige et al., 2009), reduced life expectancy (Leal et al., 2009) and painful nerve damage in the feet may occur, which can lead to lower limb and toe amputations (Barker, 2015). Diabetes can cause reduced vision and blindness and is the leading cause of blindness of people of working age in the UK (Liew et al., 2014). Depression in T2D is common and is associated with poorer self-management of T2D (Katon, 2008). In summary, T2D needs to be managed well to prevent the complications of T2D occurring.
Globally there are 422 million people with T2D with the prevalence doubling since 1980 to be 8.5% of the global adult population in 2017 (World Health Organization (WHO), 2018). The WHO (2016) projects by 2030 it will be the seventh leading mortality cause. In the UK, healthcare is managed by the National Health Service (NHS), and clinical care in England is directed by the National Institute for Health and Care Excellence (NICE; www.nice.org.uk) with treatment and prescription medication being provided at no cost to those with diabetes.
In England, most diabetes is managed by primary care nurses within GP (General Practitioners, i.e. primary care doctor) practices (Diabetes UK, 2018c). Diabetic people are advised to maintain a healthy weight and consume a healthy diet to prevent diabetic complications (NICE, 2019a). Diabetic people should exercise as part of their self-management (NICE, 2019b). In the UK, ‘regular exercise’ involves completing 150 minutes of aerobic activity a week (NHS, 2017). The NHS offers ‘exercise on prescription’ (NICE, 2019b) enabling nurses to refer people with T2D for low-cost exercise classes/gym. When planning diabetic care, nurses should incorporate patients’ religious/spiritual beliefs into individual healthcare plans (NHS, 2020), but many nurses lack confidence in addressing these (Duke and Wigley, 2016).
Clinicians advise patients how to self-manage their T2D, and this includes attention to diet, taking exercise, checking their feet (reporting any signs of skin damage) and taking prescribed medicines (NICE, 2019a). Although clinicians support patients, it is the patients who bear the day-to-day burden of diabetic self-management. This study explored if participants’ spirituality influenced their approach to diet and exercise.
Spirituality
The terms ‘spirituality’ and ‘religion’ lack scholarly definitions across academic disciplines, with Paley (2008) critical of poor analysis of spirituality within nursing. To this end, Puchalski et al. (2014) detail conferences where experts from clinical research, ethics, law and other disciplines considered a definition of spirituality alongside healthcare standards and policy. In this study the terms ‘spirituality’ and ‘religion’ are given definitions, influenced by literature from nursing, theology, psychiatry and sociology: spiritual and religious or spiritual but not religious (SBNR).
Literature reviews
This research spanned three years, involving three literature searches. Searches used controlled vocabulary, ‘suggested search term’ and truncation of peer-reviewed, full-text articles in English. The Boolean operator ‘AND’ connected the various search terms for T2D with the term ‘spirituality’. Controlled vocabulary, ‘suggested search term’ and truncation enabled variations of words, for example ‘spirit*’. In the 2014 search, 57 papers were accessed, and 21 were excluded that were not relevant to this study. Following the reading of each abstract, 37 papers were considered relevant, and 13 were considered key papers; the search was published in 2016 (Duke and Wigley, 2016). On 16 August 2019 the search was repeated: after reading every abstract, 71 sources were accessed, with 25 papers excluded, and from the two reviews in 2014 and 2019, 15 papers were considered as key. The literature showed that the self-management of T2D included: attention to diet and exercise; taking medicines for T2D; complementary alternative medicine and practices (CAMP) that may affect participants’ diet; CAMP influencing medicine-taking.
This study chose to focus on the diet and exercise of T2D. Following collection and analysis of interview data in 2019, it was evident that participants used ‘religious coping’ (RC) to manage T2D. Therefore, a third search was undertaken on 10 April 2019 using the same databases to identify literature regarding ‘RC’ and T2D’ with Boolean operator ‘AND’. Forty-eight articles were read, 26 articles excluded and 13 papers considered key.
The searches identified that psychological components, social aspects, ethnicity and gender influenced the spirituality/religiosity of people’s self-management and coping of T2D. Individuals’ dispositions influenced dynamic coping styles and together these factors influenced individuals’ self-management of diet, exercise, adherence to medicines and CAMP – traditional/folk medicines, spiritual/alternative healers, plants/herbs/nutritional supplements, acupuncture, massage or hypnosis. In America, CAMP are commonly used because they are cheaper than prescribed medicines (Jones et al., 2006). American healthcare is funded by employers, individual insurance or the government (Rosenthal 2013), where patients/organisations are billed for individual services, medication or doctor’s visits.
Most research was with African Americans, with a paucity of evidence involving British people. This research explored how the spirituality of eight adults with T2D, living in England, influenced their coping and self-management of their condition in relation to their diet and exercise. As theoretical frameworks assist with structure, certain models were considered for this research (Koenig 2012; Polzer and Miles 2007), but were decided against to avoid ‘forcing’ the data of this exploratory study into a rigid framework.
Results
Participants' spirituality, health beliefs, coping and sense of responsibility for T2D self-management overlapped in complex layers. Three themes were generated: (a) spirituality influences expectations in life; (b) beliefs influence coping styles of diabetes self-management; and (c) responsibility influences diabetes self-management. A model was developed to assist nurses in addressing these components.
The study
Aims
It was not theorised that participants living in England would have the same spirituality or coping strategies as those in America, rather the study sought to explore how the spirituality of a group of people with T2D, living in England, might influence their coping and self-management of their condition. The objectives were to: recruit participants with T2D who were living in England; explore their self-management of T2D; explore their spiritual beliefs and practices (i.e. their spirituality); explore how participants’ spirituality influenced their coping with T2D; explore how participants’ spirituality influenced the self-management behaviours of following a healthy diet and taking exercise.
Design
The constructivist paradigm posits that knowledge is socially constructed, and people develop multiple meanings about themselves and the world (Creswell, 2007). The Biographic Narrative Interpretive Method (BNIM) (Wengraf, 2001) interviews aim to reveal conscious and sub-conscious meanings springing from participants’ cultural, societal and individual beliefs. The BNIM can be used for data collection and analysis or data collection alone. The BNIM was used for its unique interview technique for data collection, and data interrogation underwent six-phase thematic analysis (Braun and Clarke, 2006). Contextual data from participants’ clinic records included glycated haemoglobin (HbA1c) over the preceding 2 years, living situation, age, length of time since T2D diagnosis, body mass index (BMI) and medicines for T2D.
Sampling strategy and method
The BNIM utilises small sample sizes (Wengraf, 2001). A purposeful sample of eight adults was recruited from seven GP practices through recruitment posters. Patients called/emailed if they were interested in the study and were sent relevant information. When eight adults had been recruited, recruitment ceased. Patients were sent Participant Information Sheets and Consent Forms to complete prior to interview, that advised contextual data would be obtained from their medical records. Inclusion criteria were > 18 years, could speak English and have had T2D > 6 months. Participants who were newly diagnosed with T2D were not chosen since they could still be in the phase of shock or denial (Peel et al., 2004), and not able to tell how they cope with the day-to-day management of their condition.
A pilot interview confirmed that two interviews per participant would be required. In 2016–2018, 16 interviews were conducted in either participants’ homes/university premises. In the BNIM method, the interview style allows participants to talk for as long as they wish with no interruptions from the interviewer. In the first interview, participants were asked to tell their story of living with diabetes; interviews lasted 50–170 minutes. As is recommended in the BNIM method, the second interviews mostly occurred one month later, asking about diet, exercise, spiritual practices and what gave them strength to cope, lasting 40–90 minutes.
Rigour
Lincoln and Guba (1985) developed criteria to verify the trustworthiness of qualitative inquiry: credibility, transferability, dependability and confirmability. Credibility was addressed by following the research process systematically; prolonged engagement with the data; audit trails of memos, developing codes and themes; peer review; keeping a reflexive journal detailing developing thoughts and theme creation, and member checking occurred – in which participants expressed resonance with the codes/themes. Transferability was assisted by a definition of spirituality and details of the English healthcare system. Dependability and confirmability were established through all these processes and the findings were not at odds with literature review results. The author acknowledges biases of being non-diabetic, white, middle-aged, female, a nurse and a Christian. These biases could not be eliminated, rather they were reflected upon deeply in a reflexive journal to prevent them influencing data interrogation.
Data analysis
For data interrogation, the six phases of thematic analysis were used systematically (Braun and Clarke, 2006: 87) and assisted by memo-writing, code-book development audit trail, keeping a reflexive journal and peer reviews. In phase 1, ‘immersion’ in the data involved transcribing interviews verbatim, note-taking, creation of memos and repeated re-reading of the data. In phase 2, initial codes were generated for every piece of information across the entire data identifying specific characteristics and involved three cycles as salient features of the meaning of the data became evident. Data was managed using 'Nvivo12', a computer assisted qualitative data analysis software program (QRS International 2018). In phase 3, collated codes were placed into broad themes. Memos were written as analysis progressed, and all Codebooks were discussed via peer review. Phase 3 resulted in 18 ‘main codes’ and 91 ‘sub-codes’. During phases 4 and 5 all main codes were reviewed to consider how the data related to the research question, the key aspects within it, how they linked to other codes and the overall ‘story’ that is evident in the data. During phase 5, five ‘analysis maps’ were created resulting in three themes involving spirituality, coping and responsibility.
Ethical consideration
Written consent was obtained before interviews. Pseudonyms enabled participant anonymity. The study gained ethical approval from the university and the Health Research Authority in 2016.
Results
Description of participants
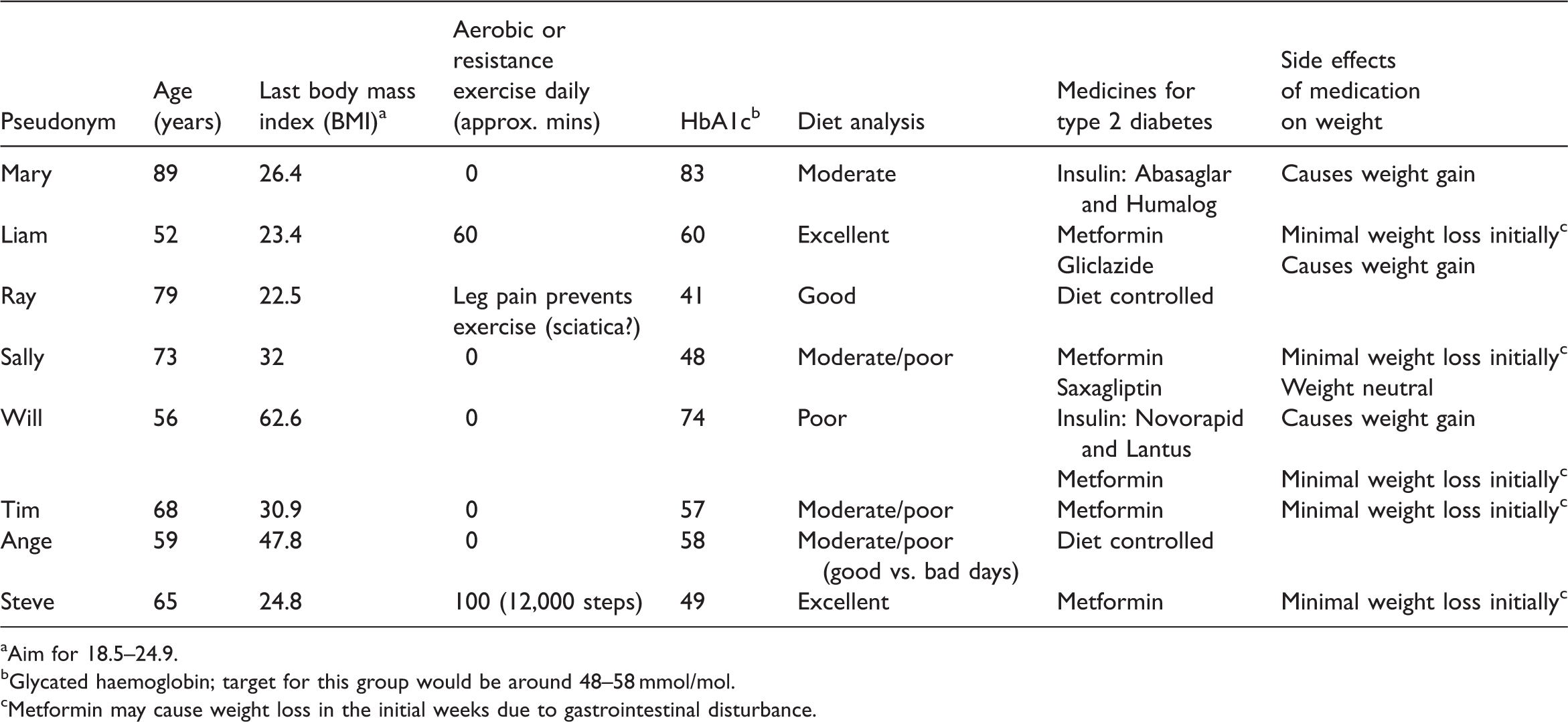
Participants lived in Hampshire, aged 52–89 years and the lived experience of T2D varied from 2 to 17 years. Tables 1 and 2, and Figure 1 show participants’ age, exercise, cooking practices and co-morbidities. Six participants self-identified as Christian: most as Church of England (i.e. Anglican) and one identified with the Salvation Army church; all were labelled as ‘spiritual and religious’. Two participants self-identified as not religious, but gave descriptions relating to the definition of spirituality used in this study and were identified as ‘spiritual but not religious’ (SBNR). Co-morbidities of participants. Description of participants’ age, exercise, cooking practices and co-morbidities. Unable due to health conditions. Participants’ contextual data compared with their diet and exercise. Aim for 18.5–24.9. Glycated haemoglobin; target for this group would be around 48–58 mmol/mol. Metformin may cause weight loss in the initial weeks due to gastrointestinal disturbance.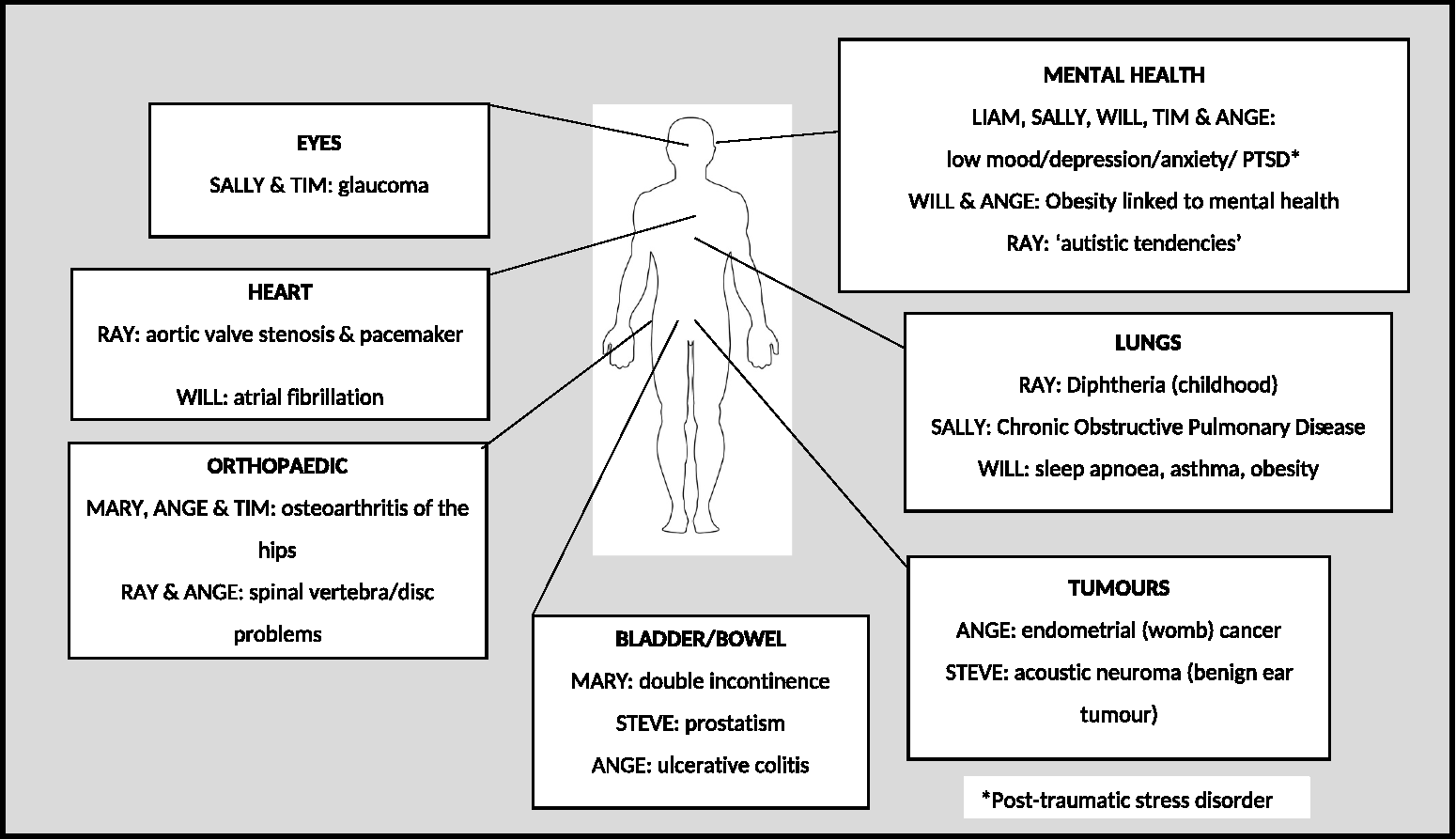
Three themes were created: (a) spirituality influences expectations in life; (b) beliefs influence coping styles in the self-management of T2D; (c) responsibility influences the self-management of T2D.
Spirituality influences expectations in life
Spirituality was significant in all participants’ lives through either family, friendships, nature and growing and/or cooking food. In addition, Christian participants found prayer, religious reading and church connections meaningful. Christians expressed core Christian beliefs, for instance Ray stated, ‘I’m a Christian and I believe in Jesus Christ and an afterlife’ and Will believed in ‘God the Father, God the Son and God the Holy Spirit’.
All Christians received ‘strength’, ‘comfort’, ‘love’ or ‘help’ from God enabling them to cope with life’s challenges. Attitude towards God varied: Mary had an ‘awe’ of God, Ange described God as her ‘best pal’ and Liam stated that Jesus is ‘the closest friend you’re ever likely to have’. Will however focused on his perceived omnipotence of God’s power in his life.
For most Christians, prayer involved communication between themselves and God, and increased their coping. Sally stated about T2D: ‘I just pray and ask God to help me and often if I’m feeling really down… I will take out my Bible and read a bit’.
All Christians spoke of God increasing their ability to cope with diabetes through prayer, reading the Bible or church, for instance Will stated God worked through ‘prayer and the scriptures’ to influence his ‘everyday thinking’. All Christians except Ray spoke of God ‘allowing’ events or ill health in their lives. Christians believed the causality of their T2D was a combination of ‘God allowing’ it, lifestyle choices and genetic factors. Liam experienced a spiritual crisis when despite prayer, God did not heal his T2D. He ‘came to terms’ with this through a spiritual encounter when he felt God say, ‘I can be with you, while you go through these things’. Ray talked about the ‘power of prayer’, and four participants believed that God had ‘a plan’ for their lives, including timing of their death. Ange believed God ‘mapped out’ her life, and Mary stated: ‘it’s not good fighting that [God’s will]… just go along with it and do your best’.
Beliefs influence coping styles in the self-management of T2D
Participants’ health beliefs, emotions, spirituality and other people influenced their coping strategies. Health beliefs included knowledge regarding causes, treatment and complications of T2D. Linking to Folkman’s (2013) coping theory, all participants appraised their diagnosis as a ‘loss’ of health, a ‘challenge’ to improve their health or a ‘threat’ to health. The SBNR participants were ‘thankful’ for their T2D diagnosis, seeing it as a ‘challenge’ to improve their health.
Participants used problem-based and emotion-based coping to improve diet, do exercise, reduce alcohol and take medicines. They attended T2D clinics and sought information from ‘Diabetes UK’ and diabetes research. Positive emotion-based coping included instrumental support, social support, positive cognitive reappraisal and ‘fighting’ negative thinking. Sally re-interpreted her diagnosis to turn ‘bad news’ to ‘good news’ by spurring her to lose weight. Family/friends support influenced mood positively, healthy dietary choices and exercise, for instance Will’s friends checked his medicine taking, Tim’s wife challenged unhealthy food choices, and Steve’s family sought healthy recipes. Participants expressed optimism and gratitude for clinical support, family, independence and instrumental support. Gratitude bolstered ability to cope with self-management; Will expressed the least gratitude and coped poorly with diabetes self-management, whereas Liam who was exceptionally disciplined in his self-management expressed the most gratitude. Negative emotion-based coping occurred with five out of eight participants who had or previously had experienced poor mental health, which linked to reduced exercise, increased alcohol, not taking prescribed medicines, a high carbohydrate diet, binge eating and obesity.
Participants’ co-morbidities influenced T2D self-management, for instance ulcerative colitis (requires low fibre diets), and breathlessness from heart/lung conditions reducing ability to exercise/mobilise (Figure 1).
Christians used religious coping (RC) to quit smoking and manage their health. Believing God to be benevolent influenced their view of God co-partnering with them. Mary stated ‘I mean people say, “Well why did He [God] let it happen?” Because God gave us willpower! And it’s your own willpower that dictates whether you cope or you don’t cope.’
Sally struggled with anxiety in self-managing T2D, prayed and sometimes would ‘get a verse’ from the Bible that would encourage her. Ange prayed before shopping ‘God help me again!’ and imagined God sitting on the supermarket freezer preventing her choosing unhealthy desserts. RC enabled most Christians to take responsibility for their diabetic self-management.
Responsibility influences the self-management of T2D
Except for Will, all participants believed in taking responsibility to eat healthily, exercise, monitor/adjust alcohol intake, monitor/manage blood sugars. Attitudes towards self-management appeared constant since diagnosis. Believing that diabetic complications could affect them motivated self-management: it’s your life, and you can do whatever you like with your life. But you’ve got to pay the consequences. (Tim) I’m shocked by people who don’t take responsibility for this problem… and I’m thinking, ‘Wow, what’s wrong with you?! It’s not the doctor who’s gonna lose their feet – it’s you. (Liam)
Some behaviours evidenced reduced responsibility (smoking and binge eating) but Sally swapped smoking to vaping, and Ange used BNIM interviews towards self-motivation. Will however appeared powerless to address his binge eating, leading to morbid obesity, shame and depression and asking, ‘What’s the point of my life?’
Diet
Post diagnosis five out of eight participants improved their diet, which was influenced by diabetic knowledge and family/friends. Ray and Tim believed their diagnosis was linked to their previous alcoholism, and monitored alcohol intake to recommended limits (NHS Choices, 2018). Only two out of eight participants aimed for high fibre/low carbohydrate diet and had 5 + /day of fruits/vegetables. Participants’ diet varied: every minute of every day I think about what I eat. (Liam, whose BMI is 23.4 and has an excellent diet) I don’t know how to be a thin person… I don’t take any notice of what I eat. (Will, whose BMI is 62.6 and has a very poor diet)
For six out of eight participants, moderate/poor diet was connected to insufficient nutritional knowledge, eating habits or depression/low mood. Those with moderate/poor diet had out-of-target range BMI and HbA1c, except for Sally whose HbA1c was within target range. It would be expected that Liam’s excellent diet and in-range BMI would result in a good HbA1c, but this was not evidenced. It may be Liam was mis-diagnosed and had ‘latent autoimmune diabetes of adulthood’ rather than T2D (Diabetes UK, 2019a). Mary’s out-of-range HbA1c is likely due to insufficient insulin doses.
Exercise
In this study, walking refers to walking outside, not around home. Promoters of exercise were motivation, free time and pleasant walking areas. Inhibitors were lack of motivation and co-morbidities impinging exercise. Attitudes towards exercise varied from focused intent to no interest. Minutes spent on exercise varied from 0 to100 minutes daily. The combination of exercise and diet resulted in BMIs ranging from 22.5 (active with a good diet) to a BMI of 62.6 (not active and poor diet) (Table 2).
Discussion
Spirituality and T2D
In this study, the spiritual practices used were similar to other research (Duke and Wigley, 2016), although participants did not use any CAMP. Consistent with other studies prayer was commonly used, but contrary to some studies participants did not forsake self-management believing prayer would heal their T2D as was found by Jones et al. (2006) and Polzer and Miles (2007).
Participants in this study talked about the private and personal importance of church. Christians were mostly Anglican, which does not appear to promote God as a healer (International Anglican Family Network, 2017).
Similar to other studies, participants found that God provided strength, support, guidance and resources to cope with diabetes (Jones et al., 2006; Namageyo-Funa et al., 2015; Polzer and Miles, 2007). According to Koenig (2008), religious beliefs and practices in the Christian worldview can provide a positive framework for individuals to interpret stressors. However, this is only likely if individuals believe God to be benevolent and responsive to individuals’ needs. This study found participants saw God as an enabler, assisting them to manage their T2D; or God as the authority figure determining their life, or considered God was benevolent. Polzer and Miles (2007) detailed some of these views with African Americans in the US who managed their diabetes via ‘a relationship with God’. With Group 1, participants believed that God helped them to perform good T2D self-management; self-management was emphasised rather than faith. In Group 2, participants believed that although God helped them with self-management, they were submissive to His will, and any positive outcomes attributed to God. In Group 3, participants believed that if they had enough faith, self-management was not necessary because God would heal them. Aspects of Group 1 and 2 were echoed in this study, but no participants abandoned self-management believing that God would heal them as in Group 3.
Beliefs and coping with self-management of T2D
In this study, participants’ beliefs influenced their coping strategies in T2D self-management. Health beliefs, spiritual beliefs and the spirituality of family/friends overlapped and promoted various coping strategies. Cultural factors sometimes overlapped with spiritual activities, such as sharing meals together and attending church together for special events, for example Christmas. Having friends/family with the same Christian beliefs bolstered some participants ability to cope.
Maladaptive coping included comfort and binge eating, which linked to depressive symptoms. Previous studies show that avoidant and negative emotion-based coping are less successful at controlling T2D (Garay-Sevilla et al. 2011; Peyrot et al. 1999), have been linked with depressive symptoms, reduced emotional well-being and poorer T2D control (Al-Amer et al., 2015). The systematic review by Abbott et al. (2018) found that binge eating and night eating syndrome resulted in a higher BMI, but no statistical difference with HbA1c. In the meta-analysis of social support and patient adherence to medical treatment by DiMatteo (2004), greater success was seen in married individuals than those unmarried, which contrasted with the study by Gallant et al. (2007) which found for those with arthritis/T2D/heart disease, more negative influences occurred from family rather than friends. In this study, the two participants who described pathological eating also had similar factors of depression, high BMI, were not married and found friends rather than family supportive.
In the study in the US, by Utz et al. (2006) involving African Americans, participants were ‘working hard’ to address diet, exercise and taking diabetic medicines. They used combinations of problem-based, emotion-based and religious-based coping for T2D self-management. With regards to active coping with T1D and T2D in Ireland, Collins et al. (2009) found coping related to values participants placed on health. Group 1 placed high value on their health and used active coping. Group 2 were passive, but followed advice from clinicians, and Group 3 placed low value on their health and took minimal responsibility for their diabetes. Most participants in the present study placed high value on their health, aiming for good diabetes self-management.
In this study, fear of diabetic complications motivated diet management and alcohol reduction. Gupta and Anandarajah (2014) found that self-management motivators in African Americans in the US included diabetic complication concerns, alongside desire to work/care for their family. The study of Romanian patients by Albai et al. (2017) regarding coping found that emotion-based coping followed by social support-based coping was more successful than problem-based coping for diabetes self-management. Emotion-based coping was the most successful for patients taking exercise and good blood glucose control. Those with complications were more likely to use problem-based and social support-based coping, but social support-based coping was associated with a significantly lower BMI. In this study, although exercise often was taken with family/friends, it did not link to lower BMI.
In this study, RC was mostly associated with motivation towards diabetes self-management. The literature shows both positive and negative effects of RC on health (Stauner et al., 2016). The systematic review of quantitative research between 1872 and 2010 by Koenig (2012) analysed the effect of religion/spirituality on mental and physical health. Of the 3300 articles, 80% related to religion/spirituality and mental health. Positive effects are psychological, social and behavioural processes that influence health and coping, including positive emotions, a positive worldview and appraisal of chronic conditions in a way that makes them less distressing. Koenig (2012) found that the negative effects of religion/spirituality could include depression, anxiety, fear, rigid thinking, avoidance and delay in seeking medical advice, but overall RC was associated with greater well-being and improved coping with stress.
Responsibility and the self-management of T2D
Baumeister et al. (2018) posit that people are information-agents that can have socio-political values. In this study, most participants took responsibility for eating healthily, taking exercise, moderating alcohol and managing blood glucose, believing that taking responsibility assisted beleaguered NHS resources. According to Hibbard and Gilburt (2014) ‘patient activation’ is a concept referring to the engagement and self-management that people adopt for their own health, and are ‘activated’ towards better health outcomes. The King’s Fund (2017) asserts that British people value the NHS, with 65% believing individuals should be responsible for their health, with just 7% placing responsibility with the NHS. It may be that the British belief in protecting the NHS is a factor in promoting diabetes self-management.
Most participants expressed the importance of having diabetes knowledge. Research in the Netherlands found 83% of participants preferred education to occur in their regular primary care check-ups, and only 3% attended diabetes education programmes (DEP) (Gorter et al., 2010). Jager et al. (2019) found that the diets of ethnic minorities in the Netherlands were influenced by culture, self-efficacy and social support, showing the significance of care delivered by primary care nurses, who know patients well and offer tailored diabetes advice. The National Diabetes Audit shows that in 2016 in England and Wales, although 74.5% of patients were offered DEP, only 8.3% actually attended (NHS Digital, 2019). It may be British patients prefer DEP by primary nurses.
In this study, the spirituality of some participants increased self-efficacy regarding dietary planning, the type/quantity of food consumed. The quantitative systematic review by Koenig (2012) of religion/spirituality found 21 studies examining spirituality and diet, with 13 studies demonstrating a significant positive association between spirituality/religion and diet, and one study demonstrating a poorer diet. In this study, the SBNR participants’ family acted like the ‘diabetes police’, encouraging them to choose healthier foods, which was similar to other studies (Lundberg and Thrakul 2011; Samuel-Hodge et al. 2000).
This research found that promoters of exercise were motivation, free time and pleasant walking areas, and inhibitors were reduced motivation and co-morbidities impinging on exercise/mobility. Exercise was not strongly linked to spirituality. In their systematic review of T2D self-management in six European countries, Kousoulis et al. (2014) found consistent, multi-level approaches to long-term education were required to address changes to diet and exercise, and was often focused in primary care. In the systematic review of randomised control trials of exercise in T2D by Avery et al. (2012), specific interventions regarding exercise had positive outcomes and reduced HbA1c, with greater success for those using multiple behaviour change techniques. Currently in England, specific exercise interventions are not promoted in diabetes care.
Limitations
The aim of the study was to explore how spirituality may influence the self-management of T2D of eight adults living in England. As is usual in the BNIM, the sample size was small, and these findings cannot be generalised to people with T2D living in England or other parts of the UK. In this study, the participants were middle-aged to old in age; it may be that younger participants would have had different perspectives. Participants were mostly Christians; it is likely that findings would be different if participants were from other religious groups or spiritual beliefs. Participants were not asked about diabetic complications, and participants’ diabetes knowledge was not measured, but it is likely this was a factor in dietary choices.
Future research
Further research on how the spirituality of British people influences their T2D self-management could focus on other ethnicities (for instance, Black British, Welsh, British Asian) and other religious groups (for instance, Muslim, Sikh, Jewish people).
Implications for clinical practice
Due to the rapid rise in people with T2D, Diabetes UK (2019b) state that diabetes is ‘potentially the greatest health crisis facing our nation’, with joint partnerships such as NHS England, Public Health England (PHE) and Diabetes UK collaborating to address the rising incidence, management and complications of the condition (Gatineau et al. 2014; NHS England 2019a; PHE 2017). In the UK, people with diabetes should be referred to diabetes education classes, yet only 6% of newly T2D diagnosed people in the UK attend (Diabetes UK, 2019c). Although some localities have improved attendance (NHS Clinical Networks, 2018) it mostly rests on primary care to deliver patient-focused, culturally relevant advice regarding diet and exercise that incorporates patients’ lifestyle, values, beliefs and co-morbidities (NICE, 2019a). Primary care clinicians therefore need to understand how their patients’ spirituality and beliefs may influence their self-management of T2D. Clinicians should consider that the ability of patients to take responsibility for their T2D might be influenced by patients’ spirituality, health beliefs and coping because it directly affects their self-management of T2D and their diabetic outcomes. It is anticipated that publication of this study will inform clinicians, especially nurses, how the complex interwoven layers of spirituality, beliefs, coping and responsibility influence patients’ spirituality when planning their diabetes care. Nurses need to ensure a good rapport with patients before opening discussions on spirituality and be careful to ensure their own spiritual beliefs do not influence discussions. Within clinics nurses could explore how their patients’ spirituality links to negative/positive interpretation of stressors; spirituality influences their motivation towards diet/exercise/medicines use; co-morbidities may conflict with T2D management; sense of responsibility links with their spirituality to influence T2D self-management.
A model is provided to assist clinicians with considering these factors (Figure 2). Model showing how the self-management of type 2 diabetes (T2D) may be influenced by spirituality, health beliefs, coping and sense of responsibility.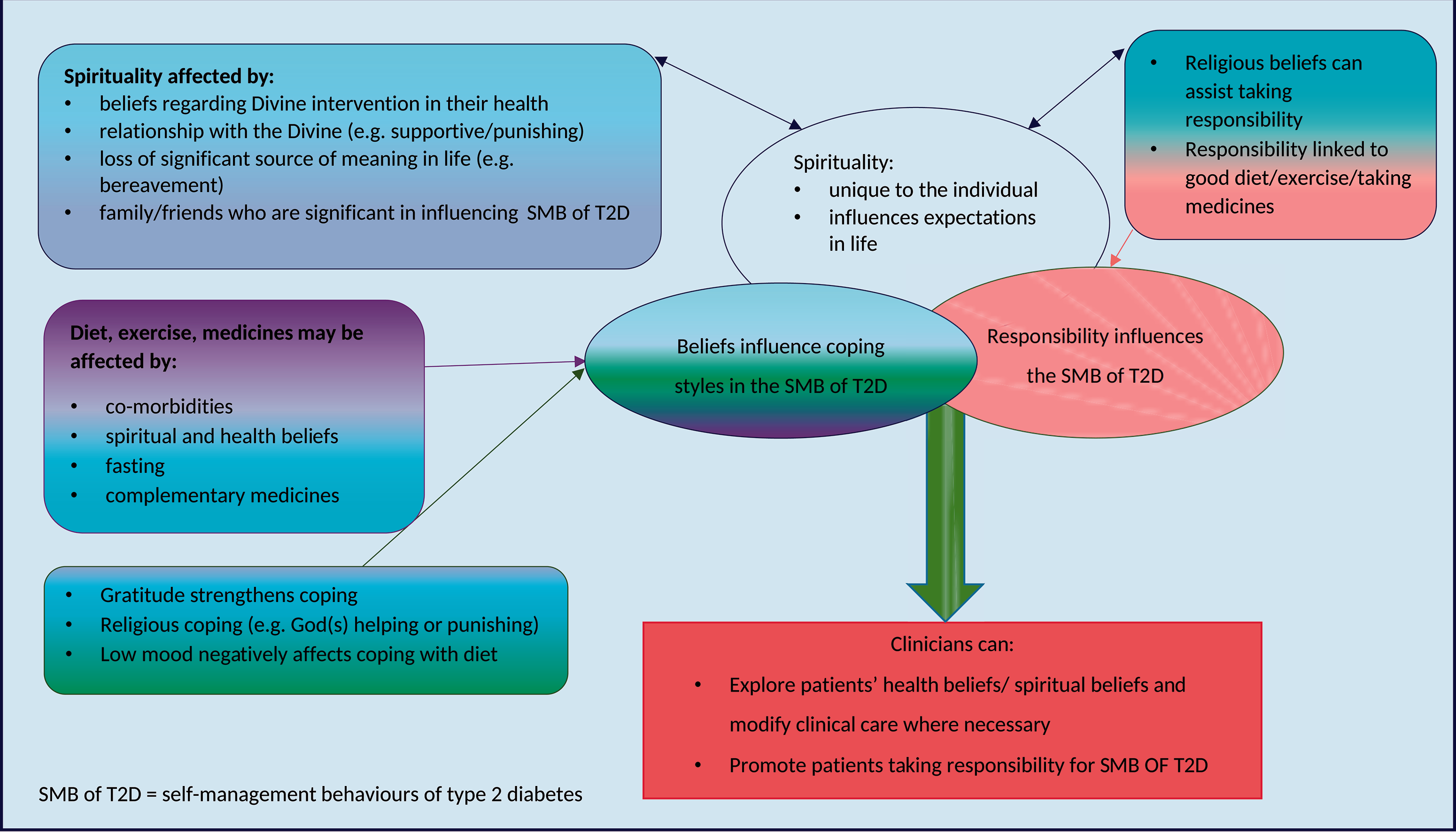
Conclusion
This study of eight British adults found that their spirituality, coping styles and responsibility overlapped in complex layers, and together influenced their self-management of T2D. For most Christian participants, their relationship with God particularly influenced their cognitive reappraisal of the stressors of their lives positively. Belief in a benevolent God provided benefits not found in human relationships. In addition to feeling loved and cared for, the belief that ‘God allowed’ challenges and was in control of the major events in their lives strengthened their coping. By interpreting stressors in life through the lens of their faith, most Christian participants were able to imbue positive meanings to difficult circumstances. The SBNR participants had a positive approach to life, appraised their T2D as a ‘challenge’ and found meaning in pursuing healthier lifestyles, providing for and enjoying their families.
Key points for policy, practice and/or research
Nurses should be aware that patients' spirituality may influence their self-management of T2D. Spirituality is a nebulous construct. People may be spiritual and religious, or spiritual and not religious. For Christians, their relationship with God may influence their cognitive reappraisal of the stressors of their lives positively or negatively, which may influence how they cope with self-management of T2D. Patients' spirituality, coping styles and responsibility is likely to overlap in complex layers, and together can influence their self-management of T2D.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
The study obtained ethical approval from the University of Southampton, and the Health Research Authority (UK) in 2016. Written informed consent was obtained from all of the participants, and verbal consent confirmed before each interview. Pseudonyms enabled participant anonymity. HRA ref: 16/NI/0089.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: scholarships/awards from the Royal College of Nursing Foundation Professional Bursary Scheme, the Florence Nightingale Foundation and The Barbers’ Company Clinical Nursing Scholarship.