
Abstract
Background
The rising rate of workplace violence in hospitals is a serious concern. While leading organisations recommend implementing interventions to address workplace violence, little is known about the workplace violence relationship between patients and visitors, and how it affects nurses’ emotional exhaustion and their perceptions of patient safety.
Aims
The study’s purpose was to understand the status of workplace violence in hospitals and the relationships between nurses’ experiences of workplace violence, emotional exhaustion, and perceptions of patient safety.
Methods
This cross-sectional analysis used data from a survey conducted at a large academic medical centre using the Agency for Healthcare Research and Quality Hospital Survey on Patient Safety Culture plus additional measures of workplace violence and emotional exhaustion.
Results
Nurses reported more occurrences of verbal violence than physical violence. Nurses’ experiences of workplace violence negatively affect nurses’ emotional exhaustion and patient-safety perceptions. Moreover, nurses’ emotional exhaustion mediated the relationship between verbal abuse and patient-safety perceptions.
Conclusions
Interventions to reduce nurses’ emotional exhaustion and strengthen resilience can mitigate the negative effects of verbal abuse and to some extent the effects of physical violence.
Introduction
Incidents of patient or visitor violence directed at healthcare workers are increasing. The US Bureau of Labor Statistics shows there was a 110% increase in workplace violence for healthcare workers between 2005 and 2014 with nurses and nurse aides experiencing this more than other professional groups (US Department of Labor, n.d.; Phillips, 2016).
Workplace violence is defined as ‘violent acts, including physical assaults and threats of assault, directed toward persons at work or on duty’ (National Institute for Occupational Safety and Health (NIOSH), 1996, para. 3). The US Department of Labor (n.d.) defines assault as ‘to attack someone physically or verbally, causing bodily or emotional injury, pain, and/or distress. This might involve the use of a weapon, and includes actions such as hitting, punching, pushing, poking, or kicking' (US Department of Labor, (n.d.) Workplace Violence Program-Appendices, para. 2).
The American Psychiatric Nurses Association (APNA) (Allen et al., 2019) indicates that nurses are exposed to two different sources of workplace violence: physical aggression, or specific actions by patients or family members toward nurses that are intended to inflict pain, bodily harm, or death; and verbal aggression, or verbal hostility, statements, or invectives expressed by patients or family members towards nurses that are intended to inflict psychological harm through humiliation, devaluation/degradation, or threats. According to the American Nurses Association (2014), 21% of nurses and nursing students have experienced physical assault and over 50% have experienced verbal assault. While the frequency of workplace violence is high, the experience of workplace violence is under reported, particularly physical assault that does not result in injury or verbal assault (American Nurses Association, 2019; Arnetz et al., 2015).
Multiple regulatory and professional groups are recommending interventions to reduce the incidence of violence. For example, The Joint Commission (2010), a non-profit organisation that accredits US healthcare organisations and programmes, recommends gathering, reporting and analysing data, providing support for affected staff and thoroughly reviewing events to understand and develop initiatives to reduce incidents. The American Organization of Nurse Executives (2014) has prepared a toolkit, Mitigating Violence in the Workplace, which integrates Joint Commission and other recommendations, including policy, training and addressing the ‘acceptance’ of violence in the workplace (The Joint Commission, n.d.). The Occupational Safety and Health Administration (2016) reflects the same recommendations and adds a proactive risk assessment to avoid incidences of violence, and the Nursing Executive Center Advisory Board recommends a faster response to workplace violence events when they occur (Boston-Fleischhauer et al., 2019).
Previous studies have demonstrated that workplace violence negatively impacts nurses and patient-care delivery. Experiences of workplace violence have been reported to increase nurses’ stress levels (NIOSH, 1996), burnout (Liu et al., 2019; Rees et al., 2018), and fear or insecurity in the workplace (Najafi et al., 2018). Workplace violence has also been associated with nurse absenteeism, job dissatisfaction, intent to leave their job or career, as well as post-traumatic stress symptoms (Rosenthal et al., 2018). These negative effects on nurses also impact nurses’ work and quality of patient care, as workplace violence has been reported to reduce nurses’ productivity (Kowalenko et al., 2013) and increase the potential for medical errors or adverse events (McNamara, 2010).
Despite the findings of prior studies, practical interventions to mitigate workplace violence are still lacking. Additionally, little is known about how the experience of workplace violence affects perceptions of patient safety and how different types of workplace violence impact nurses’ emotional exhaustion and potentially patient outcomes.
The study’s purpose was to understand the current status of workplace violence in hospitals and the relationships between patient and visitor workplace violence, nurses’ emotional exhaustion and patient safety with the goal of contributing to the development of interventions to mitigate the impact of workplace violence in the future. Our research questions were: (a) what are the characteristics of workplace violence, including the extent of under reporting violence?; (b) what are the relationships between nurses’ workplace violence experience, emotional exhaustion, and patient safety?; and (c) how do nurses’ experiences of workplace violence affect perceptions of emotional exhaustion and potential effects on patient outcomes? In particular, we were interested in understanding if nurses’ perceptions of emotional exhaustion mediated the relationship between workplace violence and patient safety.
Methods
Study design, participants and measures
This study used a cross-sectional analysis to examine data from the Agency for Healthcare Research and Quality Hospital Survey on Patient Safety Culture (HSOPS) (Sorra and Nieva, 2004) collected from hospital staff in 2017 at a large academic medical centre in south-eastern USA. In the 2017 survey, seven additional items were added to assess workplace violence and emotional exhaustion. This anonymous survey was designed to protect individual respondents. All data were de-identified through the use of codes assigned for individual responses. A total of 3601 hospital staff completed the survey. Only nurse responses (n = 1781) were used for this analysis. The nurse response rate was approximately 60%.
Workplace violence
Three items were developed to assess the frequency of workplace violence. Because no survey existed at the time to measure the frequency of workplace violence, specific workplace violence survey items were developed by conducting a thorough review of the literature on workplace violence, soliciting expert opinions and feedback, and pilot-testing for item clarity.
Our survey included items related to physical violence and verbal abuse, with examples provided for each. Our survey’s focus was limited to patient and visitor-initiated violence, as this is the most common type of workplace violence in healthcare settings (Phillips, 2016). A three-month recall period and response ranges were selected based on expert opinion (T Famolaro 2017, personal communication, 13 October). Additional expert opinion advised the inclusion of the phrase ‘regardless of the patient’s mental status or medical history’ because all types of workplace violence are often disregarded and under reported (C.N. Burchill 2017, personal communication, 11 October). Finally, the items developed were pilot-tested with 20 different nurses from three different areas where workplace violence often occurs (emergency department, psychiatry and medicine units). Minor wording changes were made based on nurses’ preferences for clarity.
The final three items included in our survey were as follows: regardless of the patient’s mental status or medical history, in the past three months, how many times have you experienced: (a) physical violence (e.g. hit, grabbed, bitten, scratched) from a patient?; (b) verbal abuse (e.g. insults, threats, screaming, cursing at you) from a patient?; and (c) verbal abuse (e.g. insults, threats, screaming, cursing at you) from a visitor (non-patient)? All items were measured using a 4-point scale, ranging from 0 = none, 1 = 1–5 times, 2 = 6–10 times, and 3 = 11 or more times.
Emotional exhaustion
Emotional exhaustion was measured using four items from the nine-item emotional exhaustion subscale from the Maslach Burnout Inventory (MBI) (Maslach and Jackson, 1981). There is general evidence supporting the use of the 9-item MBI emotional exhaustion subscale to measure emotional exhaustion in healthcare workers (Cain et al., 2017), as well as for using the four items used here (Sexton et al., 2014), and even using a single item from the subscale (West et al., 2012). We chose to use four items from the MBI to adequately capture aspects of emotional exhaustion, while also trying not to overburden survey respondents.
The four items used were as follows: (a) I feel fatigued when I get up in the morning and have to face another day on the job; (b) I feel burned out from my work; (c) I feel frustrated by my job; and (d) I feel I am working too hard on my job. These items were scored on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). A scale mean of four survey items was used for analysis, with a higher score indicating higher levels of emotional exhaustion. Cronbach’s alpha coefficients were 0.89 in this study and 0.84 in the study by Sexton et al. (2014).
Patient safety
This study used the HSOPS composite score of the Overall Perceptions of Safety to measure nurses’ perceptions of patient safety. The four items included in this composite are: (a) patient safety is never sacrificed to get more work done; (b) our procedures and systems are good at preventing errors from happening; (c) it is just by chance that more serious mistakes don’t happen around here; and d) we have patient safety problems on this unit. Items were scored using a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), and a scale mean of four items was used for analysis. Negatively worded items were reversed-scored so that higher scores indicated more positive perceptions of patient safety.
Data analysis
Analyses were conducted using IBM SPSS statistics version 26.0 (IBM Corp, 2019). Descriptive analyses and bivariate Pearson correlations were performed to describe the sample characteristics and main study variables. Multiple linear regression analysis was used to explore the relationships among nurses’ perceptions of workplace violence, emotional exhaustion and patient safety, adjusting for nurse characteristics: unit type, work hours per week, years of experience as a registered nurse and years of experience in the current work area. We used Model 4 of Hayes’s (2017) PROCESS macro and Bootstrap method to examine the mediating effect of nurses’ emotional exhaustion in the relationship between workplace violence experience and patient safety.
To estimate the extent of under-reporting workplace violence, we compared the workplace violence incidence rate from the HSOPS data to the incidence rate from two existing sources of hospital data: employee incident reports (EIR) and hospital police reports (HPR). These data were obtained from the organisation’s occupational health department, which gathers and maintains data on encounters and some health-related details when staff seek care for workplace-violence-related injuries. Hospital police reports are also created each time hospital police or security are called to assist during a workplace violence event. Therefore, we used EIR and HPR data to verify the incident rates reported in the HSOPS. Because neither the EIR nor the HPR datasets identified individuals completing a report or the professional roles represented by those who were involved in incidents, this analysis included all individuals who responded to the HSOPS (n = 3601).
To calculate the frequency of workplace violence in the three-month recall period, the range scale of workplace violence was converted to the median such that 0 reflected no occurrences of violence during the period; occurrences of one to five times was converted to 3; occurrences of six to 10 times were converted to 8; and more than 11 occurrences were converted conservatively to 11. Incidence rates from HSOPS data, EIR and HPR were calculated by dividing the total number of incidents within the 90-day period by the total number of patient days within 90 days (or the total number of patient visits within 90 days for the emergency department), and multiplying this by 1000 so that the rates are presented in a standardised rate of incidents/1000 patient days (or per 1000 patient visits), in accordance with the recommendation of the APNA Council for Safe Environments (CES) (Allen et al., 2019).
Results
Sample characteristics
Nurse characteristics (n = 1781).
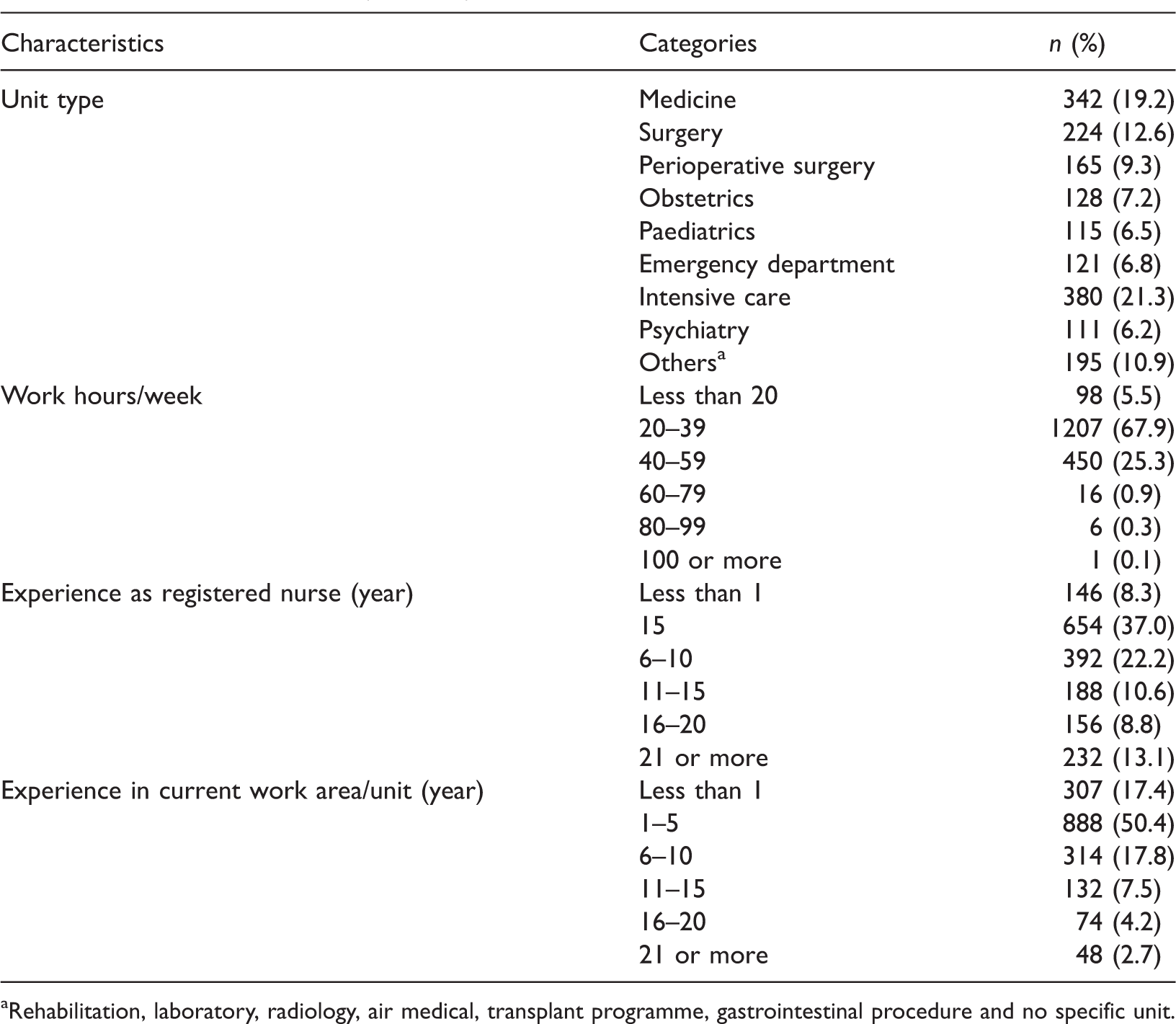
Rehabilitation, laboratory, radiology, air medical, transplant programme, gastrointestinal procedure and no specific unit.
Description and relationships of the major study variables
Descriptive statistics and correlations of the main variables.
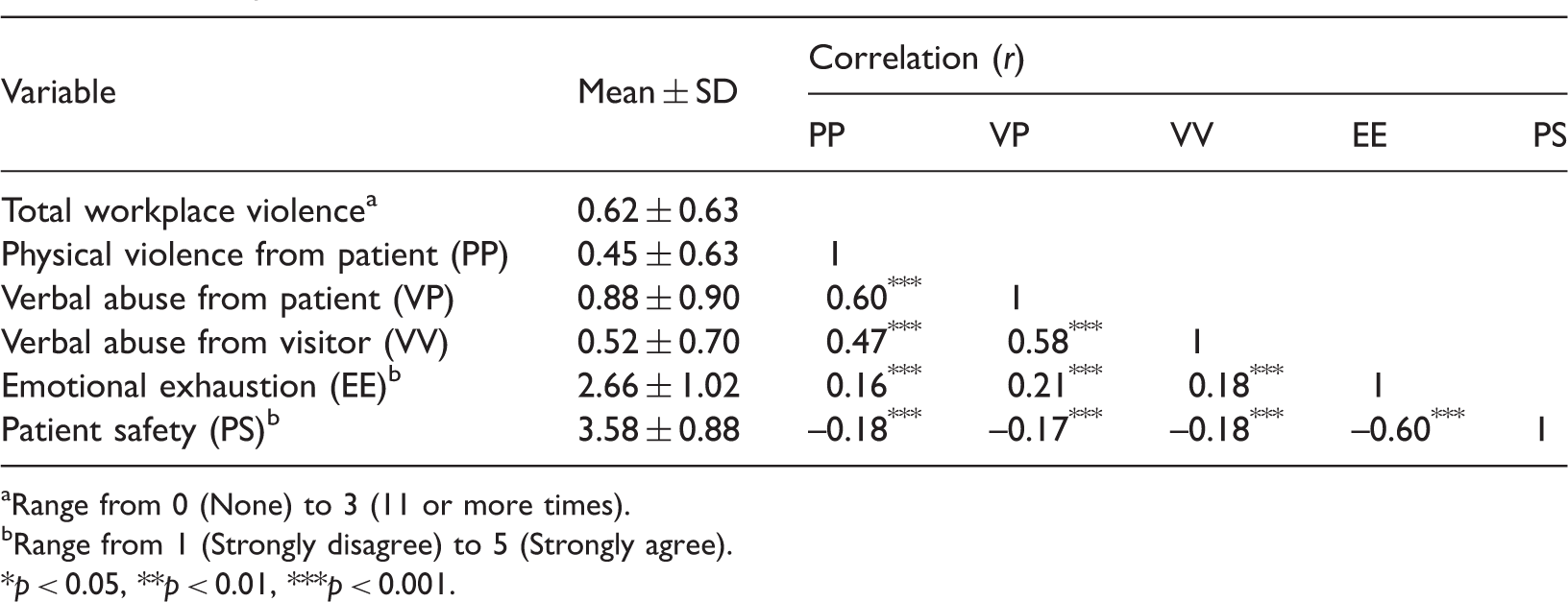
Range from 0 (None) to 3 (11 or more times).
Range from 1 (Strongly disagree) to 5 (Strongly agree).
p < 0.05, **p < 0.01, ***p < 0.001.
The mediating effect of emotional exhaustion in the relationship between workplace violence and patient safety
Regression results and mediation analysis (n = 1781).
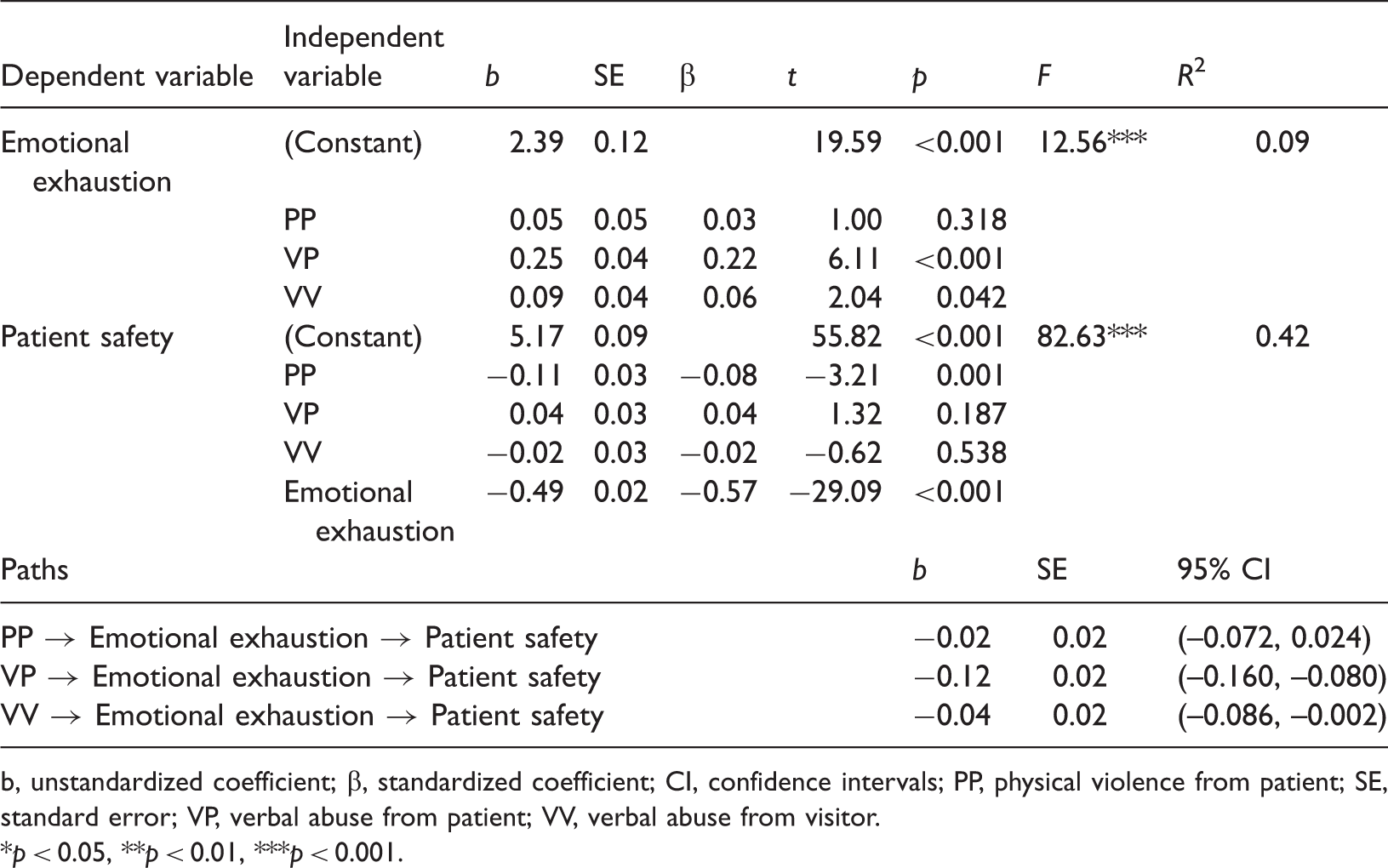
b, unstandardized coefficient; β, standardized coefficient; CI, confidence intervals; PP, physical violence from patient; SE, standard error; VP, verbal abuse from patient; VV, verbal abuse from visitor.
p < 0.05, **p < 0.01, ***p < 0.001.
Secondly, we tested the effects of the three types of workplace violence and emotional exhaustion on patient safety, adjusting for nurse characteristics. The model was statistically significant (F = 82.63, p < 0.001) and accounted for approximately 42% of the variance in nurses’ perceptions of patient safety. Nurses who reported greater occurrences of physical violence from patients reported lower perceptions of patient safety (b = −0.11, p = 0.001), and nurses who reported higher levels of emotional exhaustion had lower perceptions of patient safety (b = −0.49, p < 0.001).
Based on the results of the regression, the bootstrapping approach was used to examine the mediating effect of emotional exhaustion in the relationship between each type of workplace violence and patient safety. Our results indicated that verbal abuse from patients and visitors had an indirect effect on patient safety through emotional exhaustion (b = −0.12, 95% confidence interval (CI) (–0.160, –0.080); b = −0.04, 95% CI (−0.086, −0.002)). However, physical violence from patients directly affected nurses’ perceptions of patient safety (see Figure 1). Therefore, our results suggest that all types of workplace violence negatively affect patient safety; especially verbal abuse from patients and visitors increases nurses’ emotional exhaustion, which in turn negatively affects patient safety.
Mediating effect of emotional exhaustion in the relationship between workplace violence and patient safety. b, unstandardized coefficient; CI, confidence intervals; *p < 0.05, **p < 0.01, ***p < 0.001.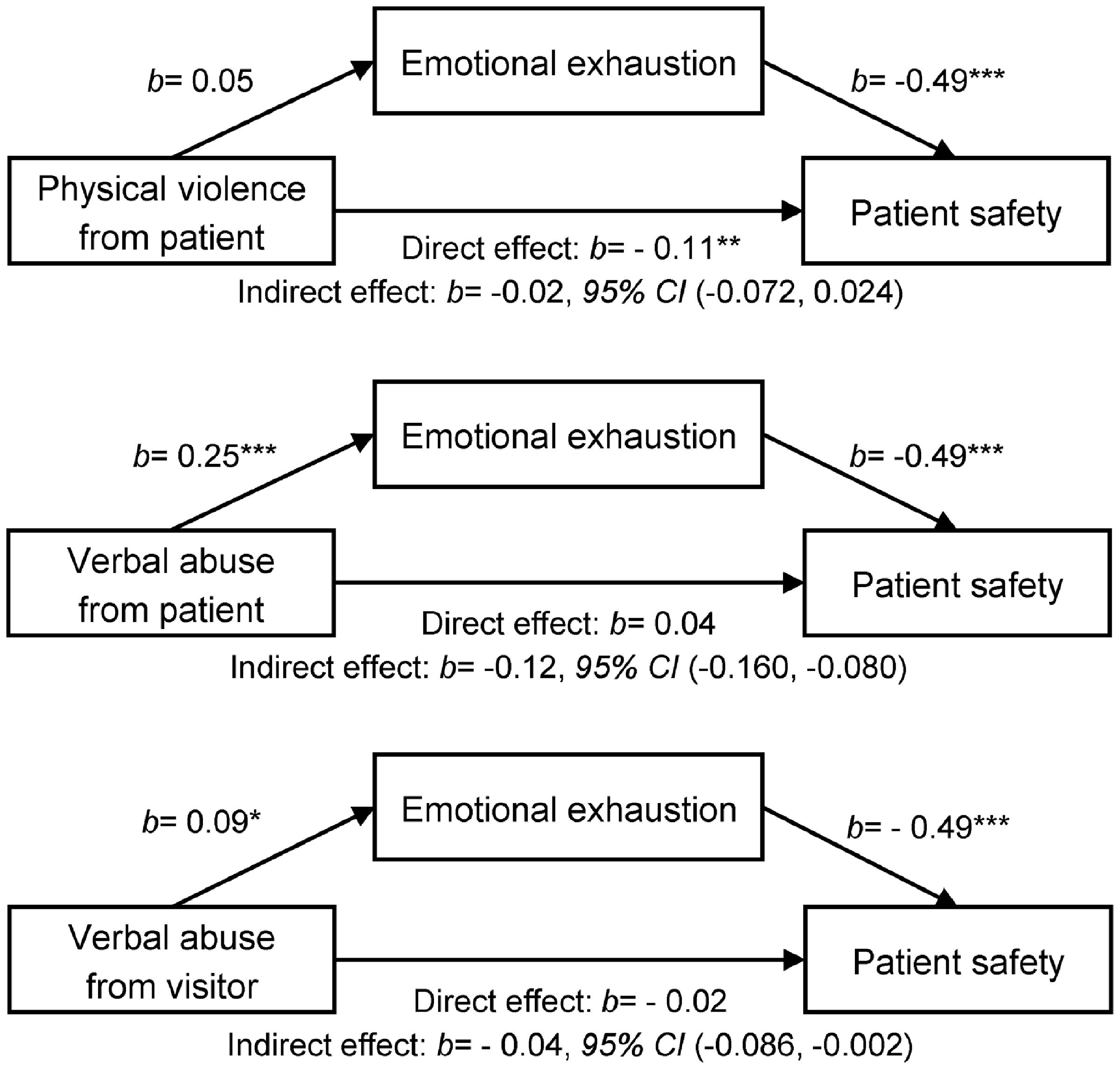
Under reporting workplace violence
Incidence rates of workplace violence: comparison of survey data and hospital data (n = 3601).
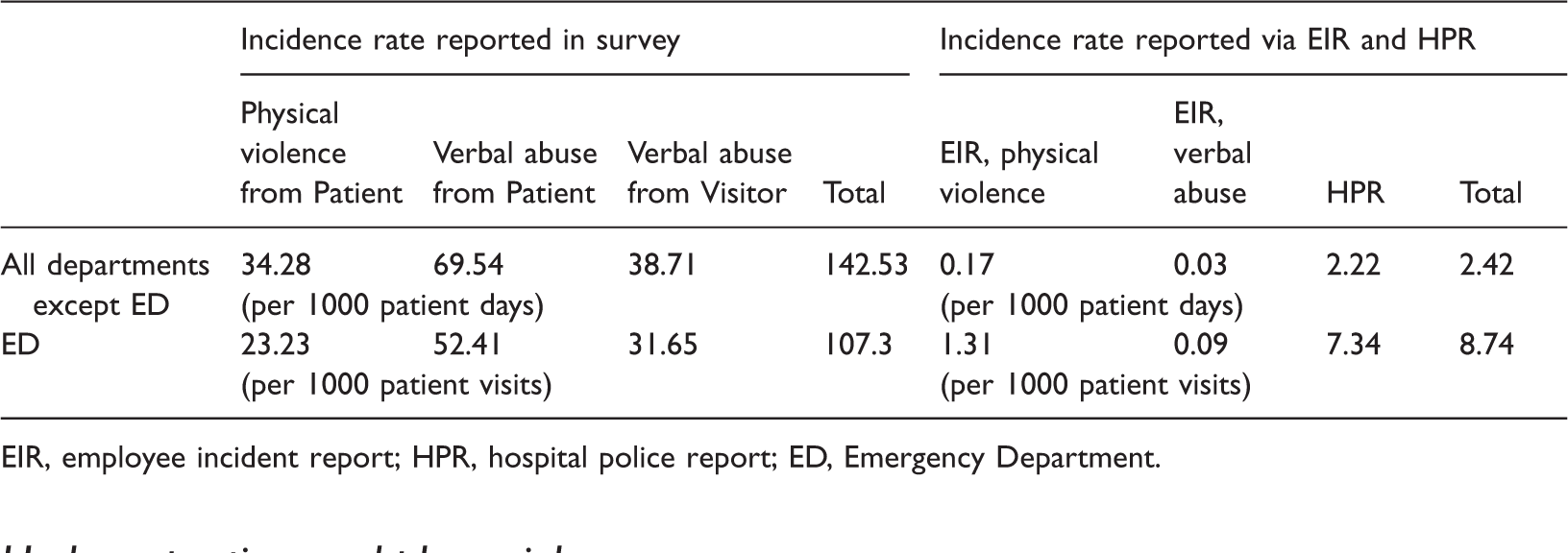
EIR, employee incident report; HPR, hospital police report; ED, Emergency Department.
Discussion
This study reveals several important findings. First, it confirms previous findings that workplace violence in the form of verbal abuse from patients occurs more frequently than patient physical violence (Pompeii et al., 2015). Our survey findings also indicate that visitor verbal abuse, presumably from patients’ friends and family, occurs more often than physical violence from patients but less often than verbal abuse from patients. In addition, this study shows that workplace violence is under reported via the hospital reporting system, and under reporting is more common in verbal abuse than physical violence, although verbal abuse occurs more frequently than physical violence.
Under reporting of workplace violence underestimates the severity of the problem and provides limited information about real situations. Accurate reporting is essential to understand the workplace violence problem and to develop effective interventions (Arnetz et al., 2015). In our study, all types of workplace violence were significantly related to nurses’ perceptions of emotional exhaustion and patient safety, and frequent verbal abuse was a strong predictor of nurses’ perception of emotional exhaustion. National groups have recommended that interventions be designed to reduce physical violence, but there is limited focus on addressing verbal violence in the workplace. Verbal violence has been associated with invisible psychological trauma that can have a cascade of negative effects on an individual’s life and ability to provide quality care (Beattie et al., 2018). Hospital administrators need to focus more on improving their reporting systems and developing robust prevention and intervention strategies for verbal abuse as well as physical violence.
Most importantly, our findings indicate that emotional exhaustion mediates the relationship between verbal abuse from both patients and visitors and patient safety. Previous literature suggests that emotional exhaustion, or burnout, is the opposite of resilience, a concept that reflects one’s ability to ‘bounce back’ from feelings of burnout (Hart et al., 2014). Strategies to enhance resilience at the individual and organisational levels are promoted as tools to combat burnout (Advisory Board, 2018). Considering emotional exhaustion along a continuum ranging from emotional exhaustion (or burnout) to resilience is helpful to interpret study findings. That is, resilient nurses may be less affected by verbal assaults from patients and visitors such that verbal abuse does not affect their perceptions of patient safety. However, nurses with low resilience, or those who are emotionally exhausted, may be confronted with repeated attacks of verbal abuse such that their perceptions of patient safety are compromised. Therefore, interventions designed to strengthen nurses’ resilience, such as mindfulness, empowerment and team support (Wei et al., 2019; The Joint Commission, 2019) are needed to mitigate the potentially devastating effects of nurses’ frequent exposure to verbal abuse and, to some extent, physical violence.
In addition, future research should focus on further testing of the mediating role of emotional exhaustion in the relationship between workplace violence and patient safety. Such an examination could highlight the importance of emotional exhaustion in understanding the overall impact of workplace violence on staff and patient safety. Other factors that mediate or moderate these relationships should also be investigated to provide a more comprehensive approach to developing targeted workplace violence intervention strategies.
Several limitations are worth noting. First, we used a partial subscale of the MBI. Although not ideal, this approach was supported in the literature and was previously used in samples of healthcare workers. Second, to our knowledge, there were no other measures of workplace violence available in the literature at the time of this study. This required our study team to develop and pilot test the workplace violence items for use in this study. Although no extensive psychometric testing was performed on these items, the items were developed specifically for this study, based on an extensive review of the literature, reviewed by field experts, and pilot tested in a small sample of nurses. Lastly, there is a possibility of duplicate reporting between the EIR and HPR. Unfortunately, we could not identify duplicates because data contained in the two reporting systems cannot be linked. Modifications to one or both systems may be needed to address this issue. For example, a specific data element could be included in each system that facilitates the linking of incident rates reported via each separate system. Future research should attempt to account for such duplicate reporting limitations to capture the precise incidence of workplace violence.
Conclusions
Workplace violence in the form of verbal abuse occurs more frequently than physical violence. Nurses’ emotional exhaustion mediated the relationship between verbal abuse and perceptions of patient safety. Although workplace violence in hospitals and healthcare settings cannot completely be eliminated, interventions are needed to mitigate the impact of violence alongside interventions to reduce its incidence. Our findings may suggest that improving hospital incident reporting systems and strengthening nurses’ resilience as a buffer against emotional exhaustion can be effective strategies to minimise the potential threat of workplace violence to patient safety.
Key points for policy, practice and/or research
Workplace violence in the form of verbal abuse from patients and visitors occurs more frequently than physical violence from patients. Workplace violence is under reported via the hospital reporting system, and under reporting is more common in verbal abuse than physical violence despite nurses’ experiences of frequent verbal abuse from patients or visitors reported in our survey. Verbal abuse from patients and visitors increases nurses’ emotional exhaustion, which has a negative effect on patient safety. Strengthening nurses’ resilience as a buffer against emotional exhaustion can be an effective strategy to mitigate the impact of workplace violence on patient safety.
Footnotes
Acknowledgements
We thank Ms Theresa Famolaro (MPS, MS, MBA, Senior Study Director, Westat, Center for Healthcare Delivery Research and Evaluation) and Dr Christian N. Burchill (PhD, RN, CEN, Nurse scientist for Cleveland Clinic’s Office of Nursing Research and Innovation) for assistance in developing the workplace violence survey items.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics
The study was approved by the organization’s Institutional Review Board (No.18-1993) and the shared governance nursing research council.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.