
Abstract
Preclinical studies show that vortioxetine displays a robust analgesic activity in models of neuropathic pain. Here, we compared the effect of a 2-week treatment with vortioxetine, duloxetine, amitriptyline, fluoxetine, and paroxetine (all injected i.p. at the daily dose of 10 mg/kg) on mechanical and thermal pain thresholds, risk-taking behaviour and depressive-like behaviour in the streptozotocin (STZ) mouse model of painful diabetic neuropathy. Vortioxetine, duloxetine and amitriptyline reduced mechanical pain in diabetic mice, with vortioxetine displaying the greatest efficacy. In contrast, paroxetine and fluoxetine were inactive. Vortioxetine, duloxetine, amitriptyline and paroxetine were also effective in enhancing thermal pain thresholds in diabetic mice. Induction of diabetes did not affect risk-taking behaviour in the light-dark box test but enhanced depressive-like behaviour in the tail suspension test. All antidepressants, with the exception of amitriptyline, reversed depressive-like behaviour, whereas paroxetine unexpectedly reduced risk-taking behaviour in diabetic mice. We conclude that vortioxetine may offer therapeutic value for alleviating pain in diabetic neuropathy, particularly in patients with comorbid depression.
Introduction
Antidepressants that inhibit both serotonin and noradrenaline reuptake, for example, amitriptyline, duloxetine and venlafaxine, are first-line drugs in the treatment of neuropathic pain1–4 and they are widely used in the treatment of comorbid pain and depression. 5 The high rate of drug resistance and the cardiovascular adverse effects of serotonin/noradrenaline reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs) 6 makes the use of these drugs in the treatment of neuropathic pain suboptimal, and encourages the search for novel therapeutic targets or the repositioning of drugs that are already marketed for the treatment of depression and are not indicated for neuropathic pain.
One of the reasons why selective serotonin reuptake inhibitors (SSRIs) show low efficacy in the treatment of neuropathic pain is that serotonin becomes hyperalgesic in chronic pain. Selective serotonin depletion in rostral ventromedial medulla (RVM) neurons projecting to the spinal cord induced analgesia in rats with neuropathic and inflammatory pain, without altering pain thresholds in healthy controls. 7 The hyperalgesic action of serotonin in chronic pain may result from a hyperactive state of serotonergic neurons caused by the epigenetic silencing of inhibitory interneurons in the RVM raphe nuclei. 8 The pain enhancing action of serotonin is largely mediated by the activation of 5-HT3 receptors in the spinal cord.9–14 Accordingly, pharmacological blockade of 5-HT3 receptors alleviates neuropathic pain in rodents and humans.10,15
Vortioxetine is a multimodal antidepressant, which displays high potency as a 5-HT3 receptor antagonist. 16 In addition, vortioxetine inhibits the high affinity serotonin transporter and behaves as a full agonist of 5-HT1A receptors, a partial agonist of 5-HT1B receptors and an antagonist of 5-HT1D and 5-HT7 receptors.17,18 Vortioxetine is a first-line drug in the treatment of depression, 19 but has no clinical indication for the treatment of neuropathic pain. We found that a 3-week treatment with vortioxetine caused robust analgesia in the chronic constriction injury (CCI) model of neuropathic pain in mice. 20 This original observation was followed by an increasing number of preclinical studies showing the analgesic activity of vortioxetine in preclinical models of chemotherapy-induced neuropathy, 21 painful diabetic neuropathy 22 and fibromyalgia. 23 Data on the effect of vortioxetine in models of inflammatory pain are controversial. Vortioxetine did not change pain thresholds in the complete Freund adjuvant (CFA) model of chronic inflammatory pain, 20 but reduced nocifensive behaviour in the orofacial formalin and acetic acid-writhing tests in mice and mechanical hyperalgesia in the carrageenan model of inflammation in rats. 24
These studies laid the groundwork for the evaluation of the analgesic activity of vortioxetine in patients suffering from comorbid depression and pain. In two open-label studies, vortioxetine showed analgesic activity in patients suffering from burning mouth syndrome.25,26 In a multicentre, prospective, open label study, vortioxetine treatment induced analgesia in patients with major depressive disorder (MDD) associated with chronic pain. 27 Thus, the use of vortioxetine may expand the therapeutic options in the treatment of MDD and comorbid neuropathic pain. What is missing in preclinical studies is a head-to-head comparison between vortioxetine and other antidepressants in a model of neuropathic pain. The role of TCAs and SNRIs in pain treatment is well acknowledged in both preclinical and clinical studies, whereas vortioxetine has not yet clinical indications for the treatment of neuropathic pain. Moreover, there are no preclinical studies in which the different classes of antidepressants are compared. Here, we examined the effect of a 2-week treatment with vortioxetine, amitriptyline, duloxetine, fluoxetine and paroxetine on mechanical and thermal pain thresholds, and depression- and anxiety-like behaviour in the streptozotocin model of painful diabetic neuropathy, in which vortioxetine was reported to be effective. 22
Materials and methods
Induction of experimental diabetes in mice and drug treatments
We used two-month-old male C57Bl/6 mice (bred in the animal house of I.R.C.C.S. Neuromed) for the induction of diabetic neuropathy. Mice were kept under controlled conditions (T = 22°C; humidity = 40%) on a 12-h light-dark cycle with food and water ad libitum. Diabetes mellitus was induced by a single injection of streptozotocin (STZ; 200 mg/kg, intraperitoneal (i.p.), as described by Furman). 23 Blood glucose levels were measured with a glucometer (ACCU-CHEK Active, Roche), according to the manufacturer’s instructions. Mice with random blood glucose levels ≥ 250 mg/dl 13 days after STZ injection were considered as diabetic and used for the assessment of mechanical pain thresholds the following day. Age-matched, non-diabetic C57Bl/6 mice were used as controls. Randomized groups of 7/17 diabetic or non-diabetic mice were treated i.p. as follows: 14 days injections of saline, vortioxetine 10 mg/kg (provided by Lundbeck A/S, Denmark), fluoxetine hydrochloride 10 mg/kg #F132, paroxetine hydrochloride 10 mg/kg #PHR1804, amitriptyline hydrochloride 10 mg/kg #A8404 and duloxetine hydrochloride 10 mg/kg #PHR1865 were purchased by Merck (KGaA Darmstadt, Germany). The fixed dose of 10 mg/kg for the five drugs was selected on the basis of previous studies in models of neuropathic pain.20,28–30
Body weight and glucose levels
Body weight was measured at the beginning (day 0) and at the end of the experiment (14 days after diabetes induction), prior to the evaluation of glucose levels. We evaluated glucose levels at day 0 (before intraperitoneal injection of STZ or vehicle), at day 2 and at day 14 of the experiment, on blood drops obtained by tail tip puncture.
Blood glucose levels were measured with a glucometer according to the manufacturer’s instructions. Mice with random blood glucose levels ≥ 250 mg/dl 14 days after STZ injection were considered as diabetic and used for the assessment of mechanical pain thresholds.
Behavioural tests
The behavioural tests were carried out in a specific dark testing room, between 2 and 4 PM. All experiments were conducted in a blinded manner, with the researchers unaware of the treatment group assignments.
Pain testing/assessment of mechanical pain thresholds
Mechanical pain thresholds were quantified by measuring the hind paw withdrawal response to von Frey filament stimulation. In brief, mice were placed in a plexiglass box (20 cm high, 9 cm diameter) with a wire grid bottom through which the von Frey filaments (North Coast Medical, Inc., San Jose, CA; bending force range from 0.008 to 3.5 g) were applied by using a modified version of the up-down paradigm. The filaments were applied five times each, in order of increasing forces, and pressed perpendicularly to the plantar surface of the hind paw until they bent. The first filament that evoked at least three responses was assigned as the pain threshold in grams.
Pain testing/thermal assay
The hot plate test was used to measure thermal pain threshold. Mice were placed on a 50°C heated surface (Ugo Basile, Gemonio (VA), Italy); the time to the first sign of nociception, such as licking of the back paws or jumping, was recorded and the animal was immediately removed.
Light-dark box
Thirteen days after the induction of diabetes mice were tested for anxiety using the light-dark box test. The light-dark apparatus consisted of an acrylic box of 20 × 50 × 20 cm, divided into a dark compartment (one third) and an illuminated compartment (two thirds). The division between zones contained a door of 12 × 5 cm, which permitted the passage of the animal from the white to the black compartment. The test was carried out as previously described, 31 between 9:30 AM and 5:00 PM. Mice were placed inside the dark compartment facing away from the access door and were recorded for 10 min. The number of entries into the light compartment, the time spent in the light compartment, and the number of transitions between the compartments were recorded.
Tail suspension test
Fourteen days after the induction of diabetes, mice were tested for depressive-like behaviour using the tail suspension test. On testing day, mice were moved to the testing room 1 h prior. Mice were suspended by the tail from a hook connected to a horizontal steel bar (the distance from floor was 20 cm) using adhesive tape, in a constant position three quarters of the distance from the base of the tail. To avoid injury, the animals were suspended by passing the suspension hook through the adhesive tape as close as possible to the tail (1–2 mm) to ensure that the animal hangs with its tail in a straight line. The mice were videotaped manually for 6 min and the parameter recorded was the immobility time (sec) in the last 4 min and the latency (sec) to immobility. 32
Western blot analysis
Western blot analysis was performed in the dorsal regions of the lumbar spinal cord dissected from diabetic or non-diabetic mice.
Tissue was homogenized on ice with RIPA buffer containing protease and phosphatase inhibitors cocktail tablet (Santa Cruz Biotechnology, Inc., Temecula, CA). Homogenates were centrifuged at 14,000 r/min for 10 min, and an aliquot was used for protein determinations. Equal amounts of proteins (20 µg) from supernatants were separated by 8/10% SDS polyacrylamide gel and transferred on Immuno PVDF membranes (Bio-Rad, Milan, Italy) for 7 min using Trans Blot Turbo System (Bio-Rad, Milan, Italy). Membranes were blocked overnight in blocking buffer (TBS, 0.05% Tween-20 and 5% non-fat dry milk) at 4°C. Membranes were incubated with the following primary antibody: anti-5HT3A receptors (1:2000, Sigma-Aldrich, Darmstadt, Germany).
Blots were incubated with corresponding secondary antibody. The blots were re-probed with anti-β-Actin monoclonal antibody (1:50,000 Sigma-Aldrich). Immunostaining was revealed by enhanced chemiluminescence luminosity (AmershamPharmacia Biotech, Arlington Height, IL) and images captured by ChemiDoc System (BioRad, Berkley, CA).
Statistical analysis
Statistical analysis was carried out by Student’s t-test for blood glucose levels and protein determinations, One-Way Analysis of Variance (ANOVA) or Two-Way ANOVA for repeated measures followed by Fisher’s LSD multiple comparisons test for nocifensive, anxiety-like and depressive-like behaviours. p values < 0.05 were considered significant. The Grubbs test was used for the identification of outlier values.
Results
For the induction of painful diabetic neuropathy, we injected mice with a single dose of STZ (200 mg/kg, i.p.). Measurements of blood glucose levels confirmed the induction of diabetes 14 days after STZ injection (Figure 1).
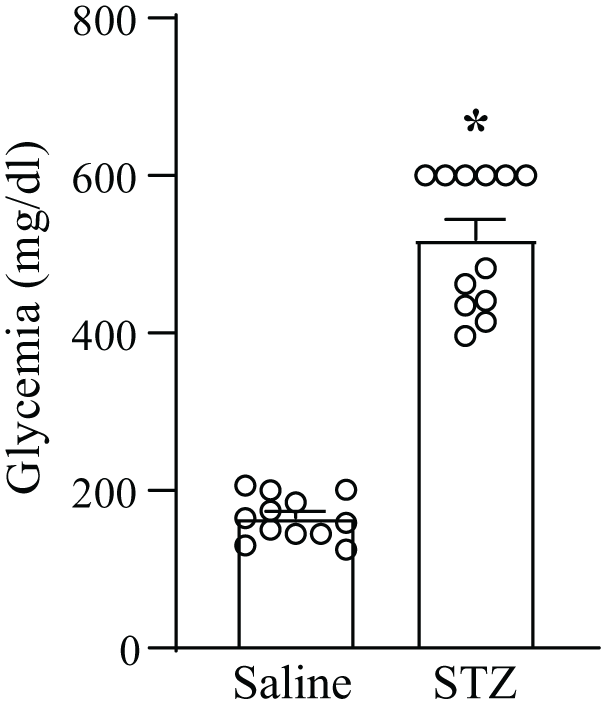
Blood glucose levels in mice injected i.p. with either saline or streptozotocin (STZ, 200 mg/kg). Values are means + S.E.M. of 12 mice per group *p < 0.05 (Student’s t test), t = 13.41.
In subgroups of mice, we measured protein levels of 5-HT3A receptors in the dorsal portion of the lumbar spinal cord. 5-HT3A receptor protein levels did not change 14 days after STZ injection (Figure 2).

Streptozotocin (STZ)-induced diabetes did not cause changes in 5-HT receptors in the dorsal region of the lumbar spinal cord. Values are means + S.E.M. of four mice in the Saline group and five mice in the STZ group.
Control and diabetic mice were treated daily i.p. for 2 weeks with either saline, vortioxetine, duloxetine, fluoxetine, paroxetine or amitriptyline (all drugs at the dose of 10 mg/kg), starting 2 weeks following saline (in controls) or STZ injection. In control non-diabetic mice none of the antidepressants caused significant changes in mechanical pain thresholds after 2 weeks of treatment (Figure 3(a)). STZ injection largely reduced mechanical pain thresholds after 2 weeks, before treatment with either saline or antidepressant drugs. Means + S.E.M. of all ‘Pre’ values in control and STZ-injected mice (Figure 3(a) and 3(b)) are 1.17 + 0.04 and 0.17 + 0.016, respectively (n = 53 and 66 in controls and STZ-injected mice; p < 0.0001; Student’s t test). Treatments with vortioxetine, duloxetine or amitriptyline significantly enhanced pain thresholds, whereas treatments with saline, fluoxetine or paroxetine did not reduce mechanical pain (Figure 3(b)). Vortioxetine reduced mechanical pain to a greater extent than duloxetine and amitriptyline (Figure 3(c)).

Mechanical pain thresholds in control (a) or streptozotocin (STZ) (b) mice treated for 2 weeks with saline, vortioxetine (Vort), duloxetine (Dulox), paroxetine (Parox), fluoxetine (Fluox) or amitriptyline (Ami). Thresholds were measured 24 h before (Pre) and at the end (Post) of drug treatment. In (a), values are means + S.E.M. of 12 saline, 9 Vort, 7 Dulox, 9 Parox, 8 Fluox and 8 Ami mice per group. In (b) values are means + S.E.M. of 8 saline, 17 Vort, 11 Dulox, 10 Parox, 11 Fluox and 9 Ami mice per group. * p < 0.05 versus the respective ‘Pre’ values (Two-Way ANOVA for repeated measures + Fisher’s LSD multiple comparisons test); time factor (Post vs Pre): F(1,60) = 21.71; p < 0.0001; treatment factor: F(5,60) = 4.544; p = 0.0014; interaction: F(5,60) = 10.56; p < 0.0001. (c) Δ mechanical pain thresholds in STZ mice. *p < 0.05 versus saline, parox and fluox; #p < 0.05 versus saline and parox (One-Way ANOVA + Fisher’s LSD multiple comparisons test), F(5,60) = 10.56; p < 0.0001.
Thermal latencies were measured in non-diabetic mice treated with saline and in all groups of diabetic mice. Thermal latencies were significantly reduced in all groups of STZ-injected mice with respect to control mice treated with saline (Figure 4). In STZ-injected mice, treatments with vortioxetine, duloxetine or amitriptyline significantly increased thermal latencies with respect to mice treated with either saline or fluoxetine, which was the only antidepressant lacking an effect on thermal latencies. Treatment with paroxetine increased thermal thresholds with respect to treatment with saline, but not with fluoxetine (Figure 4).

Thermal pain thresholds in non-diabetic mice treated for 2 weeks with saline or streptozotocin (STZ) mice treated for 2 weeks with saline, vortioxetine (Vort), duloxetine (Dulox), paroxetine (Parox), fluoxetine (Fluox) or amitriptyline (Ami). Values are means + S.E.M. of 12 saline, 8 saline STZ, 17 Vort, 11 Dulox, 10 Parox, 11 Fluox and 9 Ami mice per group. p < 0.05 versus values obtained in non-diabetic mice treated with saline (*) or versus diabetic mice treated with saline or fluoxetine (#) (One-Way ANOVA + Fisher’s LSD multiple comparisons test), F(6,71) = 18.47; p < 0.001.
We assessed risk-taking (or anxiety-like) behaviour in control or diabetic mice using the light/dark box test, in which mice are considered more ‘anxious’ if they avoid the light compartment. In saline treated mice, STZ injection did not significantly change the total time spent in the light compartment and the latency to enter the light compartment of the light-dark box (Figure 5(a) and (b)). None of the treatments caused behavioural changes in the light-dark box test with the exception of paroxetine, which, unexpectedly, reduced risk-taking behaviour (i.e. increased anxiety-like behaviour; Figure 5(a) and (b)).

Anxiety-like behaviour in control and streptozotocin (STZ) mice. The time spent in the light compartment of the light-dark box is shown in (a). Latencies to enter the light compartment for the first time are shown in (b). Values are mean + S.E.M. of 16 saline, 9 Vortioxetine, 7 Duloxetine, 9 Paroxetine, 8 Fluoxetine and 8 Amitriptyline mice per group for control mice and 10 saline, 14 Vortioxetine, 16 Duloxetine, 12 Paroxetine, 11 Fluoxetine and 7 Amitriptyline mice per group for STZ mice. In the evaluation of latency one value of the STZ groups treated with saline was identified as outlier by the Grubbs test and was removed from the analysis. *p < 0.05 versus the respective control (Two-Way ANOVA + Fisher’s LSD test). In (a), control versus STZ: F(1,115) = 25.22; p < 0.0001; treatment factor: F(5,115) = 1.435; p = 0.2168; interaction: F(5,115) = 2.522; p = 0.0332. In (b), control versus STZ: F(1,114) = 5.967; p = 0.163; treatment: F(5,114) = 2.655; p = 0.0262; interaction: F(5,114) = 2.441; p = 0.0384.
Finally, we measured the immobility time in the tail suspension test to assess depression-like behaviour. STZ injection in saline-treated mice significantly enhanced the immobility time with respect to control mice treated with saline (i.e. STZ induced depressive-like behaviour). This effect was abolished by all antidepressants except amitriptyline (Figure 6).

Depressive-like behaviour in control and streptozotocin (STZ) mice. Values are mean + S.E.M. of 16 saline, 9 Vortioxetine, 7 Duloxetine, 8 Paroxetine, 8 Fluoxetine and 8 Amitriptyline mice per group for control mice and 12 saline, 12 Vortioxetine, 15 Duloxetine, 9 Paroxetine, 10 Fluoxetine and 8 Amitriptyline mice per group for STZ mice. p < 0.05 versus the respective control (*) or versus STZ/saline (#) (Two-Way ANOVA + Fisher’s LSD test). Control versus STZ: F(1,109) = 5.255; p = 0.238; treatment factor: F(5,109) = 3.316; p = 0.0079; interaction: F(5,109) = 3.045; p = 0.0130.
Discussion
Diabetes mellitus (DM) is an endocrine disorder characterized by either the lack of insulin (in type-1 DM) or the development of insulin resistance (in type-2 DM). This leads to increases in blood glucose levels, abnormalities in fat and protein metabolism and a series of long-term complications, which severely compromise the quality of life of DM patients.
Diabetic polyneuropathy, one of the most common complications of both type-1 and -2 DM, is characterized by a length-dependent damage of peripheral nerves, and alterations of limb sensations and pain, and often persists in spite of a good control of blood glucose levels.33,34 Depression is frequently associated with diabetic neuropathy, and the severity of depressive symptoms is directly related to pain intensity.35–37
For this reason, antidepressant drugs that are known to reduce neuropathic pain, such as amitriptyline and duloxetine, are first-line drugs in the treatment of diabetic neuropathy, 2 particularly in patients with comorbid depression. In contrast, SSRIs, such as fluoxetine and paroxetine, show level A/B rating for inefficacy or discrepant results in diabetic neuropathy. 2 However, SNRIs, including duloxetine, and amitriptyline may increase the risk for hypertriglyceridemia and metabolic syndrome, 38 which play a key role in the pathophysiology of diabetic neuropathy, and this limits the therapeutic use of these antidepressants. Vortioxetine might be considered a valuable option in the treatment of diabetic neuropathy and comorbid depression because this drug has consistently shown analgesic activity in animal models of neuropathic pain, including the STZ model of diabetes (see Introduction and References therein). Vortioxetine is widely used in the treatment of major depressive disorder with a remarkable effect on cognitive symptoms, anhedonia, and emotional blunting, and excellent profile of safety and tolerability and lack of pharmacokinetic drug-drug interactions.19,39
Here, we compared vortioxetine with duloxetine, amitriptyline and the two SSRIs, fluoxetine and paroxetine, on pain thresholds and depressive-like and anxiety-like behaviour in the STZ model of painful diabetic neuropathy. We confirmed previous findings 22 showing that vortioxetine treatment caused analgesia in diabetic mice measuring both mechanical and thermal pain thresholds. Interestingly, vortioxetine enhanced mechanical thresholds in diabetic mice to a greater extent than duloxetine and amitriptyline (see Figure 3(c)), although the three drugs equally enhanced thermal pain thresholds. This suggests that the potent 5-HT3 receptor blockade by vortioxetine has a stronger impact on mechanical thresholds, or, alternatively, that the three drugs caused a ceiling effect on thermal pain. Neither fluoxetine nor paroxetine had any effect on mechanical pain, suggesting that drugs that enhance synaptic serotonin levels without interacting with serotonin receptors (with the exception of 5-HT2C receptors for fluoxetine) have no effect on chronic pain. This is consistent with the evidence that chronic pain is associated with functional changes in serotonergic neurons projecting to the spinal cord, which contribute to nociceptive sensitization reducing pain thresholds.7,8 Unexpectedly, however, paroxetine enhanced thermal pain thresholds in diabetic mice, albeit to a lesser extent than vortioxetine, duloxetine or amitriptyline. We have no explanation for the differential effect of fluoxetine and paroxetine on thermal pain in diabetic mice because both drugs display a great potency as inhibitors of serotonin transporter. Paroxetine also acts as a muscarinic cholinergic receptor antagonist at high doses, but it is unlikely that this mechanism might have contributed to the effect of paroxetine on thermal pain because it is the activation of muscarinic receptors that causes analgesia.40–42
Data obtained with the light-dark box and tail suspension test showed that diabetic mice displayed depressive-like behaviour but no changes in risk-taking (or anxiety-like) behaviour. We were surprised to find that chronic treatment with paroxetine reduced risk-taking behaviour in STZ mice because paroxetine is indicated for the treatment of anxiety in humans. 43 Treatments with all antidepressants reversed the increase in depressive-like behaviour in diabetic mice, with the exception of amitriptyline. This was also surprising in light of the robust antidepressant effect displayed by amitriptyline in rodents. 44 It is possible that neuroadaptive mechanisms associated with diabetes alter behavioural responses to classical anxiolytic and antidepressant drugs, such as paroxetine and amitriptyline. For example, it has been shown that a single injection of fluoxetine is less effective in reducing the immobility time in the forced swim test in diabetic mice because the component mediated by 5-HT1A receptors in the antidepressant activity of acute fluoxetine treatment is lost in diabetic mice. 45 The identification of the neuroadaptive mechanisms underlying the paradoxical anxiolytic effect of paroxetine and the lack of antidepressant-like effect of amitriptyline in diabetic mice awaits further investigation.
In conclusion, our findings support the analgesic activity of vortioxetine in the STZ model of painful diabetic neuropathy, an effect that may involve more than one mechanism. 5-HT3 receptor levels in the spinal were unchanged in diabetic mice, and vortioxetine-induced analgesia might be consequent to 5-HT3 receptor blockade. However, vortioxetine also behaves as a full agonist of 5-HT1A receptor, a partial agonist of 5-HT1B receptors, and antagonist of 5-HT1D and 5-HT7 receptor and a SERT inhibitor (see Introduction and References therein). All these targets might contribute to the overall analgesic action of vortioxetine. It will be important to examine whether and in which direction induction of diabetes with STZ influences the expression of the vortioxetine targets in different stations of the pain neuraxis.
Vortioxetine may be a valuable drug in the treatment of diabetic neuropathy and comorbid depression owing to its combined antidepressant and analgesic activity. Diabetes is associated with both cognitive dysfunction and depression as a result of cerebral microvascular complications. 46 This may reinforce the choice of vortioxetine in the treatment of diabetes and comorbid depression patients because the drug shows superiority with respect to all other antidepressants in improving cognitive functions.19,47 In addition, vortioxetine displays an excellent profile of cardiovascular safety, and causes no changes in body weight or sexual dysfunction. 19 As opposed to fluoxetine, paroxetine and duloxetine, vortioxetine is not an inhibitor of CYP2D6 or other isoforms of cytochrome-P450, 48 and, therefore, lacks pharmacokinetic interactions with other drugs used in the treatment of diabetic neuropathy. It is the right time to investigate the efficacy of vortioxetine in patients affected by diabetic neuropathy.
Footnotes
Data availability
All data included in this work will be deposited in a publicly accessible repository.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The independent initiated study was conducted with a partial financial support of Lundbeck Italy.
Ethical considerations
All procedures were approved by Italian Ministry of Health (923/2023-PR).