
Abstract
Fabry disease (FD) is a progressive, X-linked inherited disorder of glycosphingolipid metabolism due to deficient or absent lysosomal α-galactosidase A (α-Gal A) activity which results in progressive accumulation of globotriaosylceramide (Gb3) and related metabolites. One prominent feature of Fabry disease is neuropathic pain. Accumulation of Gb3 has been documented in dorsal root ganglia (DRG) as well as other neurons, and has lately been associated with the mechanism of pain though the pathophysiology is still unclear. Small fiber (SF) neuropathy in FD differs from other entities in several aspects related to the perception of pain, alteration of fibers as well as drug therapies used in the practice with patients, with therapies far from satisfying. In order to develop better treatments, more information on the underlying mechanisms of pain is needed. Research in neuropathy has gained momentum from the development of preclinical models where different aspects of pain can be modelled and further analyzed. This review aims at describing the different in vitro and FD animal models that have been used so far, as well as some of the insights gained from their use. We focus especially in recent findings associated with ion channel alterations -that apart from the vascular alterations-, could provide targets for improved therapies in pain.
Methods and aim
The articles included in this review were searched at the PubMed database. We aimed at detecting articles describing the use of preclinical models for the study of pain in FD to give an overview of the models available, and the information obtained from each, particularly concerning ion channels. To organize it, we structured the information in tables (dividing cell models from animal ones, Tables 1 and 2), and additional ones with information on specific channels, and parameters obtained for pain on tests performed (Tables 3 and 4). This work describes FD in relation to pain, and describes the tables to assess and compare the information on preclinical models between different publications, the advantages and limitations, and how the different studies aim at resembling some of the tests performed on patients.
Overview of preclinical in vitro models in FD.

Overview of FD animal models.
Overview of Ion channels associated with FD.

Overview of behavioral tests in rodent models of FD.

An overview of Fabry disease
Fabry disease (OMIM 301500) is a very rare disorder. The prevalence of FD was previously estimated to be between 1:40 000 and 170 000, however, pilot newborn screening studies showed a higher prevalence of 1 in 3600. 1 FD belongs to the group of lysosomal storage disorders, i.e., inborn errors of metabolism characterized by the accumulation of undegraded macromolecules in lysosomes due to a deficiency of one of the lysosomal enzymes. In Fabry disease, there is a deficient or decreased activity of the enzyme α-galactosidase-A (AGAL-A; EC 3.2.1.22; abbreviated α-Gal A), as a result of a mutation in the GLA gene located on the X-chromosome (Xq22.1). 2 A large number of mutations have been reported so far. A tool constructed to help in this classification is the fabry-database.org that aims at covering all possible amino-acid mutations, updated manually as soon as enough data become available 3 FD is classified from early-onset severe ‘classic’ form to atypical, late-onset mild ‘variant’. 4 Decreased or absent activity of α-Gal A leads to the accumulation of glycosphingolipids, mainly globotriaosylceramide (Gb3), in lysosomes of various cell types: endothelial and vascular smooth muscle cells, cardiomyocytes, kidney cells 5 and sensory and autonomic ganglia of the peripheral nervous system.6,7 In addition, the deacylated form of Gb3, globotriaosylsphingosine (LysoGb3), is dramatically increased in plasma of “classically” affected male Fabry patients and plasma and tissues of Fabry mice. 8 Also, gender differences have been referred to in relation to pain in FD, and while the traditional view assumed females as carriers (ie, asymptomatic or mildly symptomatic), a more recent position suggests that the onset of Fabry disease symptoms in females may be comparable with that of males. 9
Neuropathic pain, defined as that arising from a lesion or disease of the spinal cord and/or brain 10 is a key feature of the disease. 11 In this review, we will focus on the preclinical models, behavioral tests, and ion channel alterations that have been described in relation to pain in FD.
Pain in Fabry disease (FD)
Pain is one of the earliest clinical symptoms in Fabry disease (FD) reported by children and young adults, and even though some improvement may be obtained through enzyme replacement therapy (ERT), pain may still be present and require the use of adjunctive medication. 12 Two types of pain are generally described in FD: the episodic painful crises, also known as ‘‘Fabry crises,’’ characterized by agonizing burning pain starting in the extremities and radiating centripetally that may be precipitated by fever, exercise, fatigue, stress, or rapid temperature changes; and the second type is chronic pain characterized by burning and shooting pain in the hands or feet. 13 The definition of the type of pain is highly relevant to classify and decide on the therapeutic approach (see Politei et al. 12 and Schuller et al. 4 for pain treatment). Üçeyler et al. classified FD pain more precisely into 4 types: evoked pain, pain attacks, permanent pain, and pain crises as reported by patients. 14
Pain in FD is assumed to be mainly neuropathic and involving the small fibers (SF) as patients have a predominantly length-dependent reduction in the density of small, thinly myelinated Aδ, and unmyelinated C-fibers. Fiber hypofunction with a preference for Aδ fibers is unique when compared with other small fiber neuropathies, as in diabetes, amyloidosis, and other diseases known to cause small fiber neuropathy. In the latter, C fibers and Aδ fibers are equally affected. 11 Studies have shown accumulation of glycolipids and loss of cell bodies in dorsal root ganglia. 11 General recognized mechanisms for neuropathic pain in Fabry disease are the patterns of spontaneous pain (shooting and burning) that indicate increased excitability of axons; degeneration of C-fibers and exaggeration of pain due to heat, that suggests peripheral sensitization; and burning pain after cold exposure that supports the nociceptive disinhibition by degeneration of Aδ fibers, 15 i.e., reduction of the effects of the descending inhibitory pathway. 16 Impairment of small fiber conduction increases heat and cold pain perception. In general, spontaneous types of pain in patients with FD may be explained by hyperexcitability of peripheral nociceptive neurons. 17 Other mechanisms that may be responsible for pain in patients with FD include spontaneous ectopic firing, altered pain modulation, or central nervous system sensitization. 12 Repeated bouts of peripheral neuropathic pain may sensitize the central neural pain matrix, such that all pain in the body becomes amplified. 12 Additionally, an inflammatory component in FD pain has been suggested by several reports 18 as well as the contribution of the endothelium in pain pathogenesis mechanisms. 19
Preclinical models of neuropathic pain in FD
Different in vitro cell cultures and preclinical animal models have been used in the field of pain. We will give a summary of models available and used in the field of FD in in vitro cell models (Table 1) and animal models (Table 2) in general, to continue on the ones that have been predominantly used in pain in FD, described in detail (Tables 3 and 4).
The development of in vitro models may contribute to the discovery of promising drug targets that can be tested in future clinical trials. In addition, in vitro testing can reduce the duration and costs of translation to clinical trials by helping to identify the mechanism of action together with any associated risks. 20 The development of in vitro human disease models hinges on the availability of tissue- and organ-specific cell types that accurately recapitulate disease phenotypes. To date, most tissue engineering strategies rely on established cell lines (often transformed cell lines) or primary cells derived from patients. Human-induced pluripotent stem cells (iPSCs), which are derived from somatic cells by overexpression of a few transcription factors, can be generated from patients with or without a specific disease, and the resulting pluripotent cells can self-renew indefinitely or be differentiated into other specialized cells. Human iPSCs potentially offer an unlimited supply of cells for tissue engineering, therapeutic discovery, and modeling of diseases that affect almost all human tissues or organs. 21 This is particularly interesting to understand the underlying disease mechanism and provide a cellular and molecular platform for developing novel treatment strategies. 22
In vitro cell models (Table 1), initially, used cells obtained from FD patients especially of target organs in FD: endothelial cells23–27,29 kidney cells48–50,52–54 to determine glycosphingolipids accumulation and α-Gal A activity, and obtain lines for further research. Fibroblast32,34 and bone marrow cells30,31 were subjected to different techniques to incorporate an α-Gal A for enzyme expression, as well as for the analysis of different mutations present in FD patients. These cultures are also amenable to analyze the response to treatment, as illustrated with the use of DGJ33,39,40 (an α-Gal A inhibitor which at submolar concentrations works as a chaperone for the enzyme), or to test inhibitors of glucosylceramide synthase (lucerastat) 36 an approach based not on the replacement of the defective glycosidase, but rather on the inhibition of an earlier step in the synthesis of the accumulating glycosphingolipid. 63
Different established cell lines have also been used to analyze α-Gal A properties of mutant variants24,41 as well as the mechanisms of action of glycosphingolipids accumulation.27,46,47 Cell lines have also contributed to the development of improved enzymes.42,43,51 Reprogramming technology is being applied to derive patient-specific iPSCs lines, which carry identical genetic information as their patient donor cells. The field of FD research has also benefited from the advent of iPSCs55–58 and the CRISPR/CAS9-mediated genome engineering technology.59,60 This technique facilitates site-specific DNA deletions, insertions, inversions, and replacements and thus shows therapeutic potential, and is an invaluable tool in establishing the causal relationship between genes and stem cell behavior. 64
However, as the pain experience results from integrated pathways, all the way from sensory transduction in the periphery to perception in the brain, it is critical to study the system with each level of processing intact. 65 The use of intact animals enables the researcher to precisely manipulate physiological and pharmacological variables that allow examination of a pathway or circuit. 66
Flies have contributed greatly to the field of genetic screening in association with pain. Transient Receptor Potential (TRP) channels were first identified phenotypically in flies and cloned in that organism. Acute nociception can be assessed in flies since the somatosensory system displays properties of sensitization. The model shows also a neuropathic-like state after an injury that involves permanent central disinhibition, as a model to analyze possible aspects of chronic neuropathy. 65 Worm and fish have been particularly instrumental for possessing a neural circuitry capable of nociception, behavioral avoidance, and signal modulation. Overexpression of gain-of-function mutations of NaV1.7 in zebrafish sensory neurons led to decreased small fiber density and increased sensitivity to temperature changes 67 recapitulating hallmarks of small fiber neuropathy in patients.
Also, the introduction of mutations on nematodes has helped in the analysis of pain mechanisms using the noxious heat response of the organism. 65
Since in humans, neuropathy commonly presents with a complex combination of different sensory signs and symptoms with the presence of multiple comorbidities, including anxiety, depression, and sleep disorders, these aspects are amenable for analysis using other animal models like mice, rats, and monkeys.
As far as preclinical animal models in FD are concerned, different models have been used (Table 2). The Drosophila model has been used in Gaucher disease, another lysosomal storage disease, with deficits of the lysosomal enzyme glucocerebrosidase. Flies generated by knocking the enzyme ortholog have been used to recapitulate the disease, and autophagosome deficits have been documented. 76 This model has not been used in FD so far.
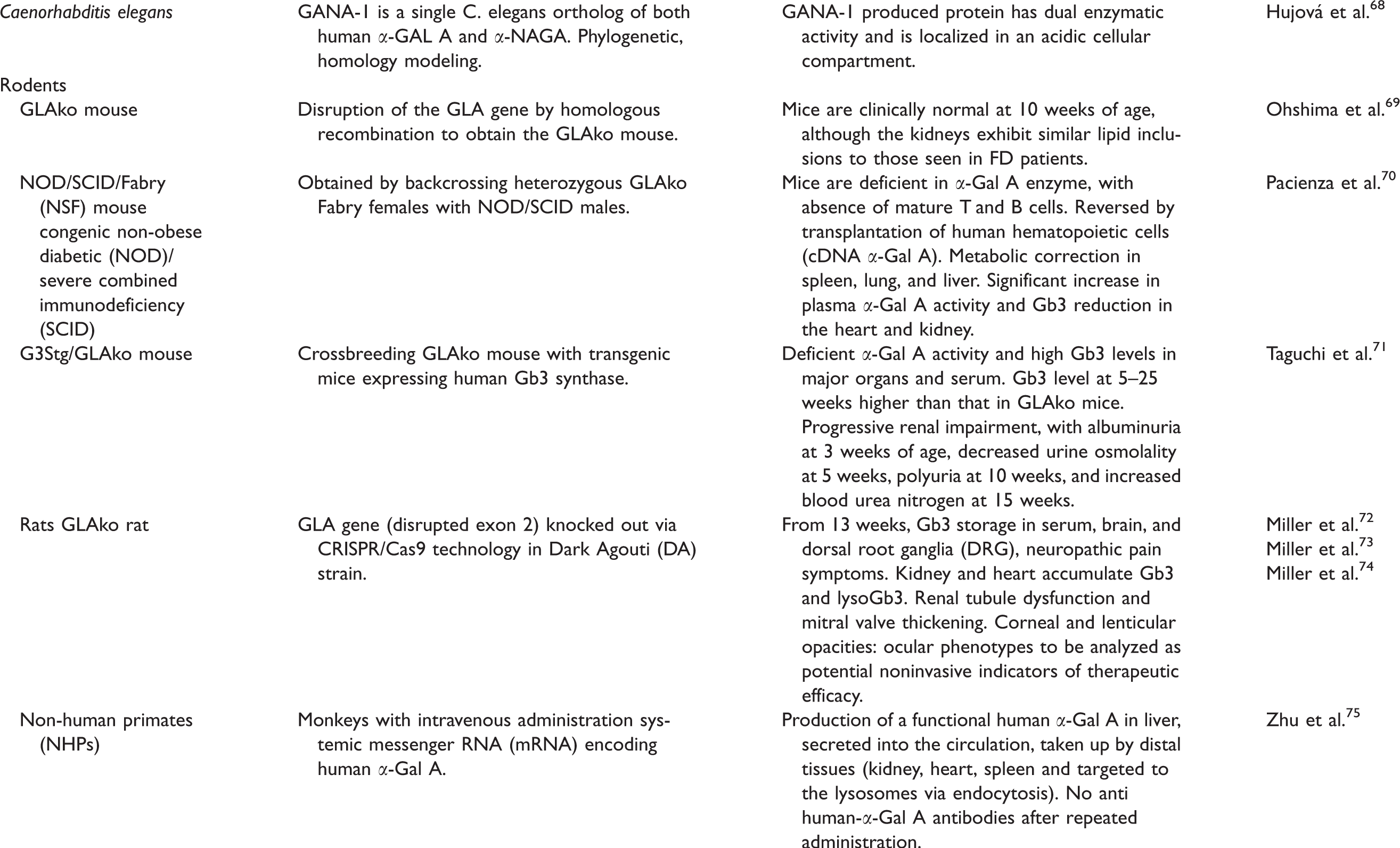
In FD, studies using C. elegans revealed a single gene with homology to both human genes (α-galactosidase and α-N-acetylgalactosaminidase), and further analysis of the protein product detected a pattern of distribution compatible with lysosomal compartments. 68
Different rodent models have also been developed. In 1997, disruption of the GLA gene by homologous recombination generated the GLAko mouse by Ohshima et al. 69 This mouse was crossed to other mice to generate a mouse line deficient in α-Gal A enzyme, with an absence of mature T and B cells to study transplantation of human hematopoietic cells expressing a cDNA for α-Gal A. 70 The GLAko mouse was also crossed to mice expressing human Gb3 synthase to obtain the G3Stg/GLAko. 71 This mouse generated higher amounts of Gb3 both in serum and the main target organs compared to the GLAko mouse and was thus proposed as phenotypically closer to classical FD. Recently, a GLAko rat model was generated using the CRISPR/CAS9 technology. 72 Non- human primates have also been used to test different therapies for the administration of systemic messenger RNA (mRNA) encoding human α-Gal A. 75
From human to animal pain
Peripheral neuropathy in patients with FD is mainly of the SF type and is associated with impaired temperature sensation, heat intolerance, and heat-induced pain, as well as abnormal cold detection threshold and thermal sensory limen at the upper and lower limb. 77 Patients refer thermal hyposensitivity and pain, with cold and warm perception reduced over time reflected by an increase in thermal perception threshold and paralleled by a loss of intraepidermal innervation, which is length-dependent. 78 Pain in FD patients has been assayed through different tests to examine fibers functionally and structurally with quantitative sensory testing (QST), and intraepidermal nerve fiber density (IENFD), via punch biopsies, respectively. QST measures sensory thresholds for pain, touch, vibration, and hot and cold temperature sensations. Commercially available devices range from hand-held tools to sophisticated computerized equipment with complicated testing algorithms, standardization of stimulation and recording procedures, and comparisons with age- and gender-matched control values. With this technology, specific fiber functions can be assessed: Aδ-fibers with cold, cold-pain, and mechanical pain detection thresholds; C-fibers with heat and heat-pain detection thresholds; and large fiber (Aαβ-) functions with vibration detection thresholds; and mechanical detection thresholds with von Frey hairs. Elevated sensory thresholds correlate with sensory loss; lowered thresholds occur in allodynia and hyperalgesia. 79 Different parameters can be obtained: cold and heat detection thresholds (CDT, HDT); the ability to detect temperature changes (thermal sensory limen, TSL), as a read-out of small fiber function. Also, paradoxical heat sensation (PHS) (if the subject experiences cold as heat), and vibration detection threshold (VDT) can be analyzed. 80 In addition, examination of small fibers can be performed specifically by other methods: laser evoked potentials, microneurography, and pain-related evoked potential. 80 For further characterization of pain in FD, different studies have used questionnaires applied to other neuropathic pain conditions, to assess the intensity, and associated depressive symptoms. 14 Other characteristics such as localization, duration, and triggers of pain have been suggested as additional parameters to be assessed in FD as FD patients reveal a distinct pain phenotype. 14
The assessment of neuropathic pain in preclinical models is associated with significant challenges given the need for indirect behavioral readouts as a surrogate of the pain experience. To study the mechanisms of persistent pain, animal models of inflammatory hyperalgesia that mimic human clinical pain conditions have been developed by the injection of inflammatory agents into the rat or mouse hind paw. These models attempt to mimic human clinical conditions. The presence of pain in the inflammation models is inferred by an increased response to a noxious stimulus (hyperalgesia) or a nocifensive behavior in response to an innocuous stimulus normally not perceived as painful (allodynia). 81 As an example, the use of inflammatory pain models help discriminate an initial phase of “nociceptive behavior” (direct effect on nociceptors), or acute peripheral pain, from a second phase considered to reflect central sensitization, due to ongoing inflammation.82,83 These models in turn can be compared to other models of neuropathic pain used to simulate chronic pain states.16,84,85
For practical reasons, the most commonly assessed behavioral outcomes are reflex withdrawal thresholds evoked by thermal or mechanical stimuli (some of the tests used in FD preclinical animal models are shown in Figure 1 compared to tests carried out in patients). These tests have been useful as most animals develop marked levels of pain-like behavior to mechanical or thermal (hot or cold) stimulation; however, there are some concerns that such models neither fully mimic traumatic nerve injury, or reflect all aspects of nerve injury seen in the clinic. Nevertheless, these have given the opportunity of testing behavior as will be further described.

Ion channels and pain in FD
Preclinical models have been instrumental in dissecting molecular mechanisms and pathways involved in FD and revealing the importance of different channels in pain.
The biophysical properties of ion channels can determine nociceptor responses to noxious stimuli and ultimately the level of nociception experienced. Ion channels, in particular sodium, calcium, and potassium channels, that regulate action potential and excitability of neurons via rapid, voltage-gated changes in ion permeability, have been proposed to hold a critical role in the transition from acute to chronic pain and contributing to neuropathic pain chronicization. 92 Sensitization and hyperexcitability of sensory neurons increase neurotransmission and excitotoxic signals.
Altered channel mRNA transcript levels, altered expression of the channel proteins, changes in their functional activity, in the cell bodies of sensory or CNS neurons, as well as alteration in channel trafficking in damaged nerves, seem to be key factors in pathological pain states.93–96 For example, the calcium channel accessory subunit α2δ1 is upregulated 20-fold in damaged peripheral neurons and is the site of action of the analgesic drugs gabapentin and pregabalin. 96 This subunit facilitates trafficking of CaV2.1 channels to the cell membrane, thus the analgesic action of gabapentin in patients with neuropathic pain could relate to the lowered calcium currents. 97 Additionally, acute effects of pregabalin, a related drug, has also been shown as reducing calcium currents.98,99
Biophysical properties of ion channels can determine nociceptor excitability, and hence abnormal channel function or expression that could lead to chronic or neuropathic pain. As an example, a central role of ion channels in chronic pain and diseases, such as epilepsy is underscored by the utility of similar drugs, such as carbamazepine, for both pathologies. 96
Many of these ion channels have also been investigated in the field of FD. As depicted in Table 3, Voltage-gated sodium channels (NaV1.7 and NaV1.8), Transient receptor potential (TRP) channels (TRPV1, TRPM8, TRPA1), voltage-gated calcium channels (VGCC); Potassium/sodium hyperpolarization-activated cyclic nucleotide-gated ion channel 2 (HCN2), voltage-gated potassium channels (KV), calcium-activated potassium channels (Kca1.1, Kca3.1), and the acid-sensing ion channels (ASIC1a) have been implicated in FD.
Even though few studies have been carried out using animal models and patients simultaneously, Namer et al. analyzed changes in ionic conductance of nociceptors in a small number of patients as well as in a GLAko model. The study described sensory abnormalities both in patients and in animals, and detected a decrease conductance of NaV and VGCC channels as well as activation of KV channels at more depolarized potentials. 108
Changes in protein levels, mRNA expression, and electrophysiological properties have been analyzed in relation to the accumulation of glycosphingolipids (Gb3 and LysoGb3) in FD. Hofmann et al. documented alteration of HCN2 and the sodium channel NaV1.7, in the GLAko (C57BL/6 backcrossed) mouse compared to control animals. 6 Even though other ion channels might also be involved, this demonstrated that increased amounts of Gb3 can lead to pathological, physiological, and behavioral signs of neuropathy. 109
Neuron hyperexcitability in DRGs soma has been analyzed in relation to Nav channels. Local anesthetics, block pain via nonselective inhibition of Nav channels in primary afferent nerve fibers of the somatosensory nervous system.110,111 These channels are responsible for the depolarizing phase of the action potential (for a detailed description of NaV channels in pain, see Bennett et al. 93 For instance, ablation of Nav1.7 and subsequent behavioral analysis has made it very clear that Nav1.7 is vital for acute pain sensation and also contributes to sensitization in a number of persistent pain models. 93 Loss of Nav1.7 function leads to congenital insensitivity to pain, whereas gain-of-function mutations in the SCN9A gene that encodes Nav1.7 cause painful neuropathies. 93 As described by Vicario et al., reduction of NaV1.8 channels in nociceptors has been associated with neuropathy, while ablation of NaV1.8 channels was associated with the development of mechanical allodynia and thermal hyperalgesia. 92 In a rat model of bone cancer pain, pharmacological blockade of Nav1.8 alleviated mechanical allodynia and thermal hyperalgesia. 112 Both channels were analyzed in association with FD6,100 (see Table 3). Namer et al. analyzed conduction velocities (CV) of C fibers in FD patients and a mouse GLAko model. They showed an increase in CV in FD compared to controls and related this result to heat hyposensitivity. Since CV depend on slow inactivation of voltage-gated sodium channels and intracellular sodium accumulation, these channels were analyzed. Tetrodotoxin-sensitive NaV currents decreased in GLAko DRGs, with a decrease in conductance that could contribute to the hyposensitivity in mice and FD patients to noxious stimuli 17 Consistent with this finding, Hofmann et al. determined a reduction of NaV1.7 currents in aged GLAko mice, as well as HEK cells in which α-Gal A had been silenced. 6 In addition, they show an increase in NaV1.8 protein levels in younger GLAko mice.
Transient receptor potential vanilloid 1 (TRPV1), known as the capsaicin receptor, is a ligand-gated ion channel. TRPV1 channels are activated by multiple pain stimuli such as acid, heat, capsaicin, protons, lipids, and spider toxins. Gene deletion and pharmacological studies have shown that TRPV1 channels have central roles in inflammatory and neuropathic pain. 113 Alteration in thermal perception was also studied in association with the TRPV1 channels in the GLAko mouse and related to heat hypersensitivity. Hofmann et al. analyzed these channels, and showed an increase in protein levels by immunofluorescence in DRG cultures of old GLAko mice. 6 Frontal paw skin as well as primary cultures of DRG neurons from Glako male mice also showed increased TRPV1 levels as shown by Lakoma et al.35,100
Transient receptor potential ankyrin 1 (TRPA1), known as a noxious cold-activated ion channel, is a nonselective cation channel mainly expressed in nociceptive primary afferent sensory neurons. TRPA1 channels contribute to transmitting harmful stimuli, whereas at central terminals in the spinal dorsal horn, these channels regulate excitatory synaptic transmission to interneurons in the spinal cord. 113 Mechanical sensitivity alterations were associated with TRPA1 channels in FD rats. 72
The TRPM8 channel is expressed by subsets of sensory neurons in the dorsal root and trigeminal ganglia and is activated by cold or ligands, such as menthol, that trigger cold sensation. In a rat model of neuropathic pain, mild cooling of the skin, peripheral or central application of icing produced marked analgesic effects, inhibiting sensitization of dorsal-horn neurons and facilitation of behavioral reflexes. 114 This channel was associated with a decreased sensitivity to cold stimulation in a GLAko mouse. 100
Activation of voltage-gated calcium channels increases neurotransmitter release and enhances excitatory synaptic transmission in the nociceptive circuits. 92 N- and P-type VGCCs are predominantly expressed in neuronal tissue in the brain, and influx through these channels is essential for depolarization-induced transmitter release. Antagonists for N- and P-type VGCCs showed antinociceptive effects in animal models of inflammation. 113 These channels have also been studied in FD –though not fully characterized- in animals injected with glycosphingolipids. 102 Namer et al. also showed decreased conductance of VGCCs both in high and low voltage-activated channels. 17
Hyperpolarizing activated cyclic nucleotide-gated (HCN) channels emerged as key players controlling and facilitating neuron excitability. The Na+/K+ inward current flowing during HCN opening, Ih, appears to contribute to spontaneous or ectopic firing in several tissues, including the central nervous system and peripheral ganglia and nerves. Evidence support the over-expression and/or gain of function of HCN in animal models of chronic, neuropathic pain. 115 Geevasinga et al. performed axonal excitability studies on the median motor and sensory nerves of FD patients and documented an upregulation of Ih which was suggested to be associated with the development of FD neuropathy and possibly neuropathic pain. 116 In turn, Hofmann et al. reported hyperpolarization-activated (Ih) current densities were reduced in DRG neurons from old GLAko mice. 6
KCa channels are major determinants of firing adaptation because they speed the repolarization of the action potential and generate the after-hyperpolarization of the plasma membrane. KCa currents are important modulators of inflammatory and neuropathic pain. They are downregulated by nerve injury and inflammation, which induces nociceptive neuron hyperexcitability, ectopic firing, and spontaneous pain. 117 These channels are altered in different in vitro FD models,37,103,105–107,118 especially analyzed in fibroblasts and altering different signaling pathways (see Table 3).
The use of non-steroidal anti-inflammatory drugs (NSAIDs) in Fabry as a non-typical treatment for neuropathic pain has been referred to by Politei et al. as part of the recommended analgesic drugs for supportive treatment of acute pain in Fabry disease. 12 Interestingly, one effect that has been documented in the field of pain is that of NSAIDs on ASIC channels. NSAIDs are major drugs used in the treatment of inflammation and pain in a wide variety of disorders. 119 A thorough study by Volley et al. pointed to the fact that apart from the best-known mechanism of action of NSAIDs, i.e., the inhibition of prostaglandin synthesis secondary to their action on cyclooxygenases (COX), NSAIDs also act on other targets to counteract pain, such as ASIC channels. 120 In fact, they showed that NSAIDs modulated the channels in two ways: with a COX-independent, fast, and reversible direct inhibition of their activity (blocking the channel); and by preventing the large inflammation-induced increase in channel expression. 121 We have recently documented ASIC1a upregulation in an in vitro model of FD. 47 The increase in ASIC1a channels, protein as well as mRNA levels, was associated with the activation of the ERK kinase, a kinase involved in the pain pathway.122,123
Involvement of channelopathies in human pain conditions has been highlighted by evidence from analysis of pain phenotypes in transgenic animal models, and different behavior in animal models could be associated with particular ion channels as assessed by pharmacological tools (Table 3, underlined, and Table 4). The behavioral tests described in Figure 1 were used to assess the GLAko mouse and the GLAko rat. As previously mentioned, the GLAko mouse has been used backcrossed to different strains (the sv129 or the BL6).
The most frequently evaluated behavioral tests were those for thermal sensitivity to heat assessed by the hot plate and Hargreaves’s tests (Table 4) and mechanical sensitivity with Von Frey’s test.
Comparing the behavior obtained in the different tests, thermal sensitivity was assessed as hypoalgesia by Rodrigues et al. 124 and Bangari et al. 125 while as hyperalgesia by Lakomá et al. 100 in the GLAko mouse. Recently, Jabbarzadeh-Tabrizi et al. compared GLAko mice backcrossed to either strain (sv129 or BL6), and found hyposensitivity to heat in both with different temperature thresholds. 126 No differences in this parameter was found for the GLAko rat by Miller et al. 72 Üçeyler et al. 101 subclassified the GLAko mouse in young and old groups and showed heat hypersensitivity in the young group (until 3 months) and hyposensitivity in the old group (more than 9 months). In the case of cold sensitivity, the GLAko mouse-regardless of the strain it was backcrossed to, hyposensitivity has been documented, while the GLAko rat has shown no difference to the control counterparts.
Therefore, thermal sensitivity alterations in the GLAko mouse might be a helpful model reflecting some aspects of the alterations detected in FD patients. In fact, changes in warm and cold detection thresholds do not always correlate well with patient pain experience. 127
In the case of the mechanical tests using von Frey filaments, GLAko mice and rats show a decreased threshold to the mechanical force applied (see Table 4, and in bold letters).
The effect of sex has not been explored consistently by the different authors. Most of the studies analyzed the behavior of male animals or pooled the results of male and female animals. Üçeyler et al. 101 and Miller et al. 72 explored the effect of sex on behavior, finding no significant differences. These results contrast with the effect of sex observed in FD patients. 9 We believe that this difference observed between the animal models and FD patients warrants further studies on the effect of sex on pain behavior in FD animal models.
As stated by Mogil et al., the entire existing preclinical pain literature may be male-biased as the subjects of experiments have overwhelmingly been male. 128 Sex differences in brain region activation in response to thermal and electrical stimuli have been reported. 129 Animal studies have demonstrated effects of estrogens on dendritic growth and synaptic density; shifts in estradiol levels that accompany the menstrual cycle affect patterns and levels of neuronal activity. 130 In the case of FD, variability of the phenotype in females could be contributed by X-chromosome inactivation (XCI), as well as highly skewed XCI favoring the expression of the mutant allele, and has been proposed as a mechanism to explain the occasional development of clinical symptoms. 131
FD patients report frequent symptoms of anxiety, and most FD patients experience episodic and chronic pain that limit their physical and everyday life activities. Their overall quality of life is reduced which induces depressive symptoms and impaired cognitive function (concentration and mental endurance). Hofmann et al. set out to explore whether these behaviors could be evidenced in animal models of FD. However, no significant differences were observed between GLAko mice and their control counterparts when anxiety, depression, and learning behavior were explored. 132
An important point to highlight, when using rodent animal models, is the fact that neuropathic models, sometimes used in FD, were initially developed in rats, so attention should be paid due to anatomical differences, as nerves are configured differently and the constriction of a lumbar spine nerve at one level might be different in either rat, mouse, or even in different strains. 133 Also, when considering the behavior of mouse models, there is an inherent limitation in the way the transgenic animal has been generated: most lines started with a gene knocked out in a strain stem cell line (normally the “129” strain) different from the blastocyst embryo stage where it is introduced to (normally the C57BL/6). 134 Controls will also differ according to the strain used for the backcrossing. This point was thoroughly described by Gerlai in 1996 134 who claimed how phenotypical abnormalities attributed to the null mutation in several molecular neurobiological studies could simply result from the effects of background genes. 135 Even if backcrossing for several generations is performed, as described by Gerlai, eliminating the confounding effects of background genes would be a considerable undertaking and not an optimal solution. 134 Thus, control strains used are very important and perhaps the reason why as Üçeyler et al. 101 described, there are different heat withdrawal latency times for different control animals used (of different strains and whether littermate is used), leading to conclude for a hyper or hyposensitivity accordingly 6 (see Table 4, in bold letters). These results are not surprising since Mogil et al. in 1999 tested a large number of inbred mouse strains for responses in a broad range of murine assays of nociception. The main result of the work being that genotype significantly affects performance in all of the nociceptive measures: behavioral traits have a significant heritable component in mice, and among the different strains, the C57BL/6 is one of the most sensitive and genetically distinct. 136
These factors have to be considered when interpreting results and verifying with proper controls, -that might be silencing RNA techniques or with pharmacological inhibitors- to confirm and discard the possibility that the result might be a consequence of a “hitchhiking donor gene confound” effect. 135
As shown in Table 2, the CRISPR/CAS9 technology offers also new possibilities of analyzing animals with a gene deletion without the mentioned problems. However, the experimenter might decide on a model according to how well it reflects features of pain as present in FD patients.
To sum up, the different models described can be used to recapitulate particular aspects of pain that reflect FD characteristics. This can help analyze mechanisms and potential therapeutic targets in pain in FD, as long as the experimenter bears in mind all the limitations of the models to confirm with the proper tools. In FD research, these tools are just starting to be used and can thus benefit greatly from all previous work done in the field of pain.
Final remarks
As discussed throughout this review, pain in FD shows differences from other SF neuropathies. The use of different preclinical models has been instrumental in dissecting different players involved in the mechanism of pain. In addition, most of the documented work in FD has focused on peripheral and spinal levels, while supraspinal structures should also be taken into account, especially since Gb3 accumulation has been also detected in different areas of the brain. 137
Another aspect that should be considered is the effect on kidney function and its contribution to pain which is not consistently analyzed.
Apart from ion channels, a significant portion of studies have also indicated a dysfunctional endothelial metabolism characteristic of sensory profiles in Fabry disease. This could indicate a dysfunctional release of endothelial nitric oxide (NO) underlying pathomechanisms in FD that may rather implicate a central disinhibition pain mechanism due to a reduced A-δ fiber input. 19
In addition, studies published over the last decade have elucidated the role of CNS resident glial cells in many aspects of pathological neuronal functioning, occurring in neuropathic pain, with phenomenon like cell-to-extracellular communication mediated by hemichannels and cell coupling (gap junctions-GJs). 92
A comprehensive revision of past studies, and a closer analysis on the similarities and differences between patients and animal models would help achieve translatability of preclinical models.
All these factors will have to be considered and thoroughly analyzed to aim at better therapies in FD pain.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grants PICT 2016-3642 from Agencia Nacional de Promoción Científica y Tecnológica (ANPCYT) and Grant 01/Q666 (20020130100666BA; Universidad de Buenos Aires Ciencia y Tecnología [UBACYT]) from University of Buenos Aires (to O.D.U.) and Investigator-Initiated Research grant (no. IIR-AR-002659) funded by Takeda Pharmaceuticals International AG Singapore Branch (to O.D.U).
ORCID iD
Carina Weissmann ![]() ">https://orcid.org/0000-0002-7196-5390
">https://orcid.org/0000-0002-7196-5390