
Abstract
Complex regional pain syndrome (CRPS) is a highly enigmatic syndrome typically developing after injury or surgery to a limb. Severe pain and disability are common among those with chronic forms of this condition. Accumulating evidence suggests that CRPS may involve both autoinflammatory and autoimmune components. In this review article, evidence for dysfunction of both the innate and adaptive immune systems in CRPS is presented. Findings from human studies in which cytokines and other inflammatory mediators were measured in the skin of affected limbs are discussed. Additional results from studies of mediator levels in animal models are evaluated in this context. Similarly, the evidence from human, animal, and translational studies of the production of autoantibodies and the potential targets of those antibodies is reviewed. Compelling evidence of autoinflammation in skin and muscle of the affected limb has been collected from CRPS patients and laboratory animals. Cytokines including IL-1β, IL-6, TNFα, and others are reliably identified during the acute phases of the syndrome. More recently, autoimmune contributions have been suggested by the discovery of self-directed pain-promoting IgG and IgM antibodies in CRPS patients and model animals. Both the autoimmune and the autoinflammatory components of CRPS appear to be regulated by neuropeptide-containing peripheral nerve fibers and the sympathetic nervous system. While CRPS displays a complex neuroimmunological pathogenesis, therapeutic interventions could be designed targeting autoinflammation, autoimmunity, or the neural support for these phenomena.
Keywords
Introduction
Complex regional pain syndrome (CRPS) usually develops after limb injury followed by immobilization. 1 It presents with a disparate array of nociceptive, vascular, and autonomic changes that exceed the expected clinical course of the inciting injury in both magnitude and duration, frequently resulting in significant functional impairment and disability. Additionally, trophic changes consisting of acutely hypertrophic and later atrophic skin may be seen along with changes in nail texture and hair growth. Osteopenia is sometimes observed on radiographic studies. The population incidence of CRPS is approximately 26 per 100,000 person-years, though the incidence is much higher in specific settings. 2 For example, prospective clinical studies report a 31% incidence of CRPS after distal tibia fracture and an average 18.8% (1047 patients, range: 1%–37%) incidence of CRPS after distal radius fracture. 3 Additional sources of limb injury linked to CRPS include hand and foot surgery, sports-related trauma, and injuries suffered on the job. Traditionally, CRPS is divided into Type I and Type II with the latter less common variety involving a verifiable nerve lesion.
Patients with CRPS typically progress from an acute stage in which the affected limb is painful, warm, and edematous to a chronic stage in which warmth and edema resolve but the pain remains. 4 Quantitative sensory testing of both CRPS I and II patients has revealed high rates of thermal and mechanical hyperalgesia and slightly lower rates of cold and mechanical allodynia. 5 CRPS symptoms gradually improve over the first year after injury in some patients, but persistent CRPS is a serious problem resulting in severe pain, weakness, contractures, and bone loss. 6 Even with this improvement, however, the majority (∼75%) continue to meet the commonly used Budapest criteria for diagnosis. 7 Over 80% of chronic CRPS patients are severely disabled. 8 Treatment strategies are most often symptomatic and focus on rehabilitation; no currently available treatment is disease modifying. Moreover, there is considerable uncertainty as to whether any treatment for CRPS is reliably effective. 9
The fundamental obstacle to the rational design of therapies to prevent or treat CRPS is our lack of understanding of the syndrome’s underlying mechanisms. Indeed, the diverse and temporally evolving range of manifestations of the syndrome makes studies in humans and animal models difficult to execute and interpret. To this point, theories based on the dysfunction of a specific type of tissue, alterations in a single signaling pathway, or change in abundance of a single specific biochemical mediator have failed to explain the complexity of aptly named “Complex” regional pain syndrome. It is notable in this regard that a growing number of enigmatic multisystem syndromes and diseases are now believed to be the result of deranged immune system function. We hypothesize that CRPS may have a similar basis. Furthermore, dysfunctional neuroimmune interactions are likely responsible for initiating and perpetuating CRPS.
Review
Autoinflammatory and autoimmune processes
Two types of immune system dysfunction are increasingly recognized for their contributions to a broad variety of disease states, autoinflammation and autoimmunity. As the “auto” prefix implies, both these processes involve immune activity against self though through distinct mechanisms. In autoinflammation, the innate immune system is directly responsible for tissue inflammation; in autoimmunity, the innate immune system activates the adaptive immune system against self. 10 Both sets of processes potentially affect the physiology of multiple systems including the neurological, musculoskeletal, vascular, and integumentary systems, all systems being involved in CRPS. The disease states currently recognized to be supported by autoinflammation and autoimmunity are highly diverse.10,11 Autoinflammation and autoimmunity were once thought of as mutually exclusive conditions, though it is now appreciated that diseases such as recurrent pericarditis, psoriasis, and ankylosing spondylitis have mixed autoimmunologic etiologies.12–14 Both autoinflammation and autoimmunity can support inflammation in the absence of infection, a sign of CRPS recognized from the time of Paul Sudeck’s descriptions of the syndrome more than 100 years ago. 15 While autoinflammation and autoimmunity are known components of several conditions and diseases involving painful symptoms, the specific roles of these phenomena as pain mechanisms are less well recognized.
Autoinflammation
Autoinflammatory conditions are currently recognized as “clinical disorders marked by abnormally increased inflammation, mediated predominantly by the cells and molecules of the innate immune system, with a significant host predisposition.” 16 These conditions are characterized by episodic or continuous inflammation commonly manifest as joint swelling, myalgias, and rashes. Pain is frequently experienced in the setting of autoinflammation and has been reported to occur in skin, joints, muscle, and viscera (Table 1). Both monogenic (Mendelian) and highly complex polygenic conditions may be considered autoinflammatory.10,14,16,17 Although many of the currently recognized autoinflammatory diseases are rare, several common pain-related conditions involve autoinflammatory processes including osteoarthritis and gout. 18
Diseases associated with autoinflammation.

Genes and corresponding proteins, where known, are included in this table.
TNF: tumor necrosis factor; NA: not applicable.
The basis for these conditions is dysfunction of the innate immune system, though specific conditions may involve different pathways. The innate immune system is that branch of immunity involving both humoral and cellular response elements nonselective for specific threats or antigens. This type of immunity provides an immediate defense against invading organisms, and the cellular components include dendritic cells such as the skin’s Langerhans cells, mast cells, and others. Pattern recognition receptors expressed on these cell types and involved in the innate immune response include Toll-like receptors, NOD and NALP receptors, RIG-I receptors, and several others.19,20 When these receptors and cells are activated, the involved cells produce cytokines, complement fragments, prostaglandins, bradykinin, and other pro-inflammatory and pronociceptive mediators. The activation of inflammasomes, multiprotein complexes that facilitate the maturation and subsequent secretion of inflammatory cytokines, 21 is common to many innate immune pathways resulting in the production of IL-1β and IL-18. The IL-1β produced by inflammasome activation in autoinflammatory disorders is thought to be a key mediator underlying painful symptoms.22–25
The complement system can be activated by multiple pathways including ones that are a part of the innate system of immunity generating complement split products.26,27 Anaphylatoxin split products including C3a and C5a both intensify inflammation and can contribute to pain directly through interactions with their respective receptors on neurons or indirectly by stimulating the production of cytokines and neurotrophins in the surrounding tissue.28–30 In addition, the membrane attack complex C5b-9 (MAC) formed by complement system activation can lead to nerve damage and Wallerian degeneration. 31 Recently, it was suggested that sublytic concentrations of MAC help to regulate acute and chronic inflammation through the activation of ERK1 and other intracellular signaling pathways in neurons and additional cell types.32,33
Autoinflammation and CRPS (cytokine production)
Observations made in CRPS patients, as well as the results of experiments using animal models, support the notion that autoinflammation contributes to multiple manifestations of CRPS. Early stage CRPS patients often exhibit the classical signs of acute inflammation including rubor (erythema), tumor (swelling and edema), calor (warmth), dolor (pain), and loss of function. Indeed, acute CRPS can be mistaken for infection, compartment syndrome, and other conditions involving acute inflammation. As reviewed above, autoinflammatory conditions have as their hallmark the generation of inflammation-related immune molecules including cytokines and complement fragments, the accumulation of innate immune cells such as mast cells, and the activation of dendritic cells in the absence of a foreign pathogen. All of these occur in CRPS.
Elevations in skin cytokine levels including TNFα, IL-1β, IL-6, and others have been demonstrated in human volunteers and patients after minor mechanical trauma, 34 fracture, 35 burns, 36 and surgery. 37 Using immunohistochemical analysis and immunoassays of skin suction blister fluid, elevated skin cytokine levels have been documented in CRPS patients at various stages of the syndrome as well. For example, suction blister fluid from CRPS patients was found to contain elevated levels of IL-6, TNFα, and ET-1,38,39 though these levels did not correlate strongly with the stage of the syndrome. 40 Immunohistochemical studies demonstrated that keratinocytes in the skin ipsilateral to CRPS symptoms express higher levels of IL-6 and TNFα than the skin of the contralateral limb. 41 Similar studies have been performed on serum from CRPS and control patients showing higher levels of cytokines such as IL-6 and TNFα along with lower levels of anti-inflammatory cytokines such as IL-10.42,43 Local TNFα activity may correlate with mechanical allodynia in CRPS patients. 44 Imaging studies indicate that TNFα accumulates in the joints and other tissues of CRPS limbs during the acute phase of the syndrome, 45 and biologic anti-TNFα agents have shown some promise in the treatment of CRPS.46–49
The mechanisms by which cytokine levels increase and support the varied manifestations of CRPS have been studied extensively in animal models. Using the well-validated rodent tibia fracture/cast immobilization model, it has been shown that skin and, to a lesser extent, muscle levels of IL-1β, IL-6, and TNFα are elevated.50–54 Although better investigated in animal models than in humans, the pain-related neurotrophin nerve growth factor (NGF) also appears to be strongly elevated in the skin of these model animals. 55 Furthermore, both small molecule and biologic therapies targeting NGF and cytokine signaling reduced the allodynia, hindpaw unweighting, and some of the vascular and autonomic CRPS-like features demonstrated in the model animals in these studies. Similar to the findings in humans, the keratinocyte layer was found to be responsible for generating most of the involved mediators,41,56 though again deeper tissues such as muscle do seem to generate pain-related cytokines. 50 Mitogen-activated protein kinase (MAPK) activation within keratinocytes was functionally linked to the enhanced cytokine production. 56 Additional studies on CRPS model animals demonstrated the activation of inflammasomes in keratinocytes as a required step in the production of IL-1β in the tibial fracture/cast model consistent with established autoinflammatory pathways. 52
A striking feature of these observations was the requirement for intact neuropeptide and sympathetic nervous system signaling. Blockade of the substance P (SP) NK1 receptor using the selective antagonist LY303870 was observed to block nociceptive and vascular CRPS-like changes in models of both CRPS Type I (fracture/cast) and CRPS Type II (sciatic transection).57,58 Subsequent studies using neuropeptide signaling-deficient animals showed that SP and calcitonin gene-related peptide (CGRP) signaling through efferent peptidergic neurons is required for enhanced levels of IL-1β, TNFα, and NGF. 59 The production of these mediators by keratinocytes is reliant upon neuropeptide-mediated activation of ERK1/2 and JNK MAPK signaling pathways. 56 Clinical evidence exists for exaggerated SP signaling in CRPS; the application of exogenous SP in CRPS patient limbs shows increased SP-induced plasma protein extravasation in both affected and unaffected limbs of patients. 60
The mechanism for upregulation of SP and CGRP signaling after fracture has not been fully elucidated, but oxidative stress may be involved. Several lines of evidence from human studies suggest oxidative stress in the limbs of patients with CRPS.61–63 Nociceptive sensitization and elevated markers of oxidative stress have been noted in the limbs of laboratory animals used with either the ischemia-reperfusion or the tibial fracture model of CRPS, changes that can be reduced by the administration of antioxidant drugs like N-acetyl cysteine and vitamin C.50,64 Using the tibial fracture model, it was observed that oxidative stress caused the upregulation of SP and CGRP that in turn were critical for the production of inflammatory cytokines (IL-6) and the pain-related neurotrophin NGF. 50
While the most extensive data regarding inflammation and cytokine production in CRPS pertain to skin, muscle, and joints, elevations in cytokine production in spinal cord tissue have been noted as well after fracture and cast immobilization. Specifically, elevations in IL-6 and CCL2, cytokines often associated with activated glia, were identified in spinal cord tissue ipsilateral to tibial fracture in rats one and four weeks after injury. 65 Similar to the results in skin, c-fiber activity was shown to underlie microglial activation and cytokine production, and the NK1 receptor antagonist LY303870 blocked the glial and cytokine changes.
The autonomic nervous system may also control the production of inflammatory mediators in CRPS. For example, studies using chemical sympathectomy suggested that the sympathetic nervous system is responsible primarily for IL-6 upregulation after fracture and cast immobilization, and that this sympathetically supported IL-6 production is required for the full manifestation of CRPS-like symptoms. 66 Further investigation demonstrated that β2 adrenergic receptors are particularly important to IL-6 upregulation. The parasympathetic nervous system, on the other hand, has been much less well explored in relation of CRPS. The well-demonstrated roles of cholinergic stimulation, particularly through the vagus nerve, suggest that inadequate parasympathetic tone might contribute to the excessive production of inflammatory mediators as may be the case in rheumatoid arthritis. 67
Autoinflammation and CRPS (immune cell contributions)
Additional cellular immune system components including mast cells and Langerhans dendritic cells, which contribute to both innate and adaptive immunity, may contribute to CRPS. Evidence for mast cell involvement comes from skin blister fluid studies in which the mast-cell marker protein tryptase was found to be elevated in the CRPS affected versus contralateral limbs of patients. 68 Complementary data using skin biopsies from the ipsilateral versus contralateral skin of CRPS patients showed an accumulation of mast cells ipsilateral to the CRPS symptoms, particularly in subjects with relatively acute disease. 41 Patients with very chronic CRPS failed to show such differences in mast cell abundance. 69 Mast cell migration and degranulation is influenced by SP signaling in humans, and such signaling could be involved in the accumulation of mast cells in the limbs of CRPS patients.70,71 In humans, the contribution of mast cells to CRPS pain has not been established directly, though pain is a prominent feature of mastocytosis, a disease in which abnormally large numbers of mast cells accumulate. 72 Additionally, mast cells are contributors to neurogenic inflammation, a well-described component of CRPS. 73
Extensive investigation of mast cell function has been undertaken using animal models. Mast cell accumulation and degranulation in the dermis has been observed after tibial fracture and cast immobilization in rats. 74 The accumulation and degranulation of these cells controls nociceptive sensitization in this model of CRPS. Further investigation showed that the degranulation of the dermal mast cells was dependent upon SP signaling through the NK1 receptor consistent with established human physiology governing mast cell degranulation. In fact, SP-containing nerve fibers were found to be in close proximity to the infiltrating mast cells. Mast cells release a wide range of mediators capable of supporting nociception, though the specific nociceptive pathways have not been defined in clinical CRPS or animal models.
Likewise, abundant Langerhans cells were identified in skin samples from some CRPS patients using immunohistochemical techniques,75,76 although a more definitive study involving primarily later stage patients found diminished Langerhans cell numbers in CRPS skin. 69 Interestingly, the migration of Langerhans cells in skin is regulated in part through α1 adrenergic receptor signaling, 77 and signaling through β adrenergic receptors controls cytokine release from these cells. 78 Aberrant adrenergic signaling is a key component of CRPS pathophysiology. 4 However, recent studies using the well-validated rodent tibial fracture/cast immobilization model of CRPS failed to demonstrate any effects of Langerhans cell depletion casting some doubt on this hypothesis or perhaps highlighting immunological differences between humans and mice. 76
Autoimmunity
Autoimmune conditions are ones in which the body produces an immune response against its own tissues. Autoimmunity involves the adaptive immune system, a system of cells and processes targeting specific antigens. Both B and T lymphocytes participate in adaptive immunity, and in many instances, this form of immunity involves the formation of antibodies released into the blood and other tissues to find their targets. An additional component of the complex biology governing adaptive immunity are dendritic or Langerhans cells. Langerhans cells are found in especially high numbers in the gut and skin where they are positioned to detect early the presence of foreign proteins on invading microorganisms. 79 Mentioned previously as participants in the innate system of immunity due to their ability to phagocytose invading organisms and to produce inflammatory mediators such as cytokines, these are also one type of antigen-presenting cell. Under certain conditions, Langerhans cells activate CD4+ helper T cells which in turn stimulate B cells to produce antibodies against the presented antigen. 80 Langerhans cells are capable of presenting self-antigens thus stimulating an adaptive immune response against intrinsic tissues. However, antigen presentation capability is not limited to Langerhans cells. 81
A wide variety of tissues can be the target of autoimmunity, and the list of diseases with autoimmune pathology is growing rapidly. In addition to classic autoimmune diseases such as rheumatoid arthritis, type-1 diabetes, Hashimoto’s thyroiditis, and myasthenia gravis, autoimmunity is now believed to play a role in several heart and lung diseases, narcolepsy, and certain forms of encephalitis.82–84 Many autoimmune conditions involve antibodies directed against components of the central or peripheral nervous systems, and some of these conditions involve pain as a primary symptom (Table 2). For example, Guillain–Barre syndrome (GBS) involves a polyneuropathy affecting both motor and sensory components of peripheral nerves.85,86 Autoantibodies have been identified in variable percentages of GBS patients against neurofascin, gliomedin, contactin, GM1 ganglioside, and several additional proteins.87,88 Recent evidence suggests that many cases of idiopathic small fiber neuropathy may be due to autoantibodies against these fibers. 89 Although rare, a pain syndrome caused by anti-voltage-gated potassium channel complex antibodies has been described. 90 Nearly 50% of patients with such antibodies had pain, and nearly one-third had pain as the only presenting symptom. In the case of paraneoplastic neuropathies, autoimmunity involving anti-Hu and anti-CV2/CRIMP5 antibodies has been linked to painful sensory changes. 91
Autoimmune diseases characterized by painful symptoms.
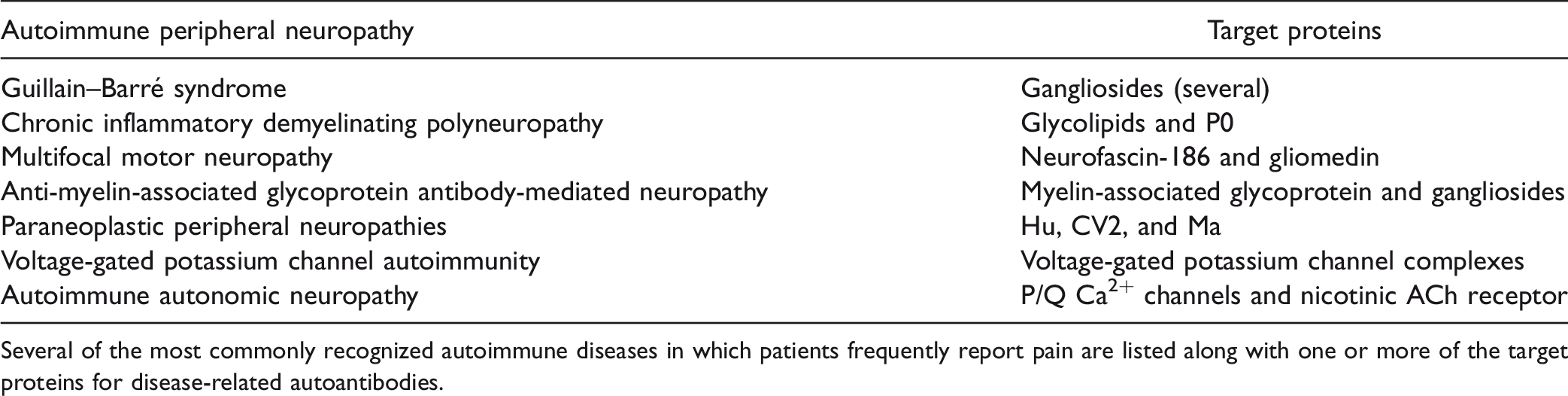
Several of the most commonly recognized autoimmune diseases in which patients frequently report pain are listed along with one or more of the target proteins for disease-related autoantibodies.
Autonomic changes tend to be less of a therapeutic focus when confronted with a patient suffering from CRPS, yet autonomic dysfunction is a component of this syndrome.43,92,93 It is notable then that several types of autoimmune autonomic neuropathies have been described, 94 and some degree of autonomic dysfunction, for example, cardiovascular reflex tests, heart rate variability, and sympathetic skin tests, has been found in rheumatoid arthritis, the archetypical painful autoimmune disease. 95
Autoimmunity and CRPS
Emerging evidence suggests that autoimmunity may contribute to CRPS. 96 A collection of observations made over the past decade suggest an autoimmune etiology for CRPS, thus helping to explain the seemingly unrelated nature of the syndrome’s signs and symptoms as well as difficulties in achieving adequate symptom control, remission, or cure using standard therapies. Exploration of CRPS-related autoimmunity began with the serendipitous observation of symptom improvement in CRPS patients treated with intravenous immunoglobulin for unrelated conditions. Later, a small randomized clinical trial using low-dose intravenous immunoglobulin provided positive results, 97 although a subsequent larger scale trial failed to reveal significant effects using this drug. 98 Plasma exchange therapy has also been shown effective in reducing pain in CRPS patients, 99 but larger trials are required to confirm these results.
The autoimmune hypothesis is bolstered by several additional sets of observations. First, it was demonstrated that a disproportionate number of patients had IgM and IgG profiles consistent with antecedent infections by chlamydia, parvovirus, and campylobacter.100,101 Cross-reactivity of antichlamydia and campylobacter antibodies with self-antigens explains some cases of autoimmune neuropathy.102,103 Second, experiments using immunohistochemical techniques and cytometric analysis identified sympathetic nervous system neurons as targets for autoantibodies from some CRPS patients with little evidence of such autoimmunity from patients with other types of peripheral neuropathy.101,104 Subsequent experiments using an in vitro beating cardiomyocyte preparation suggested that a majority of CRPS patients but not healthy controls have autoantibodies binding to and activating the M-2 muscarinic, β-2 adrenergic (β2-AR), or α-1 adrenergic receptors.105,106 Interestingly, other patients expressing anti-β2-AR autoantibodies display orthostatic hypotension and additional nonpain symptoms suggesting adrenergic receptor autoantibody expression alone may not be sufficient to cause CRPS. 107 Third, CD14+ monocytes are elevated in the blood of CRPS sufferers, and those cell counts correlate with allodynia severity. 108 Fourth, specific human leukocyte antigen (HLA) immune alleles are associated with CRPS.109–111 HLA-B62 and HLA-DQ8 have been associated with CRPS with fixed dystonia, while HLA-DQ8 alone was associated with CRPS without dystonia. Last, CRPS shows a 3–4:1 female:male predominance similar to the strong female predominance characterizing most autoimmune conditions.2,112
Animal models have been employed to pursue the hypothesis that autoimmunity contributes to the signs and symptoms of CRPS. Paradigms of passive transfer of immunoglobulins have been used to address the question of whether antibodies themselves are involved. For example, Goebel et al. injected purified IgG from CRPS patients intraperitoneally in control mice. Although nociceptive behaviors were not changed in these mice, the animals displayed both changes in rearing behavior and performance in a task involving balance and coordination perhaps consistent with the motor changes in CRPS patients. 113 A follow-up study involved the administration of CRPS or control patient IgG to mice in which hindpaw incision had been made mimicking the trauma normally preceding the development of CRPS. In this model, both mechanical hyperalgesia and edema were enhanced by the CRPS patient IgG. In addition, the CRPS IgG increased wound area SP levels. 114 Separate experiments employed the well-characterized tibial fracture/cast immobilization model of CRPS in which to study autoimmune contributions. In CRPS model mice in which CD20+ B cells had been depleted using a biologic agent, the manifestation of allodynia, postural unweighting, and vascular changes were all attenuated. The results were nearly identical when the same measurements were made in the muMT mice that do not produce mature B cells. 115 More recent autoantigen discovery experiments identified several potential autoantigenic proteins, and one protein, keratin 16, seemed to be reactive with both murine CRPS model IgM and IgM antibodies from CRPS patients. 116 The passive transfer of IgM but not IgG antibodies purified from CRPS model wild-type mice reconstituted nociceptive sensitization in CRPS model muMT mice. 117 It is not clear whether CRPS-related IgM autoantibodies lead to pain via a direct interaction with their targets, or whether the deposition of antibodies promotes subsequent responses such as the activation of complement.
Additional experiments showed that knockdown of B cells did not affect postfracture increases in skin cytokine levels, though the deposition of complement fragments in peripheral tissues was diminished. 115 The complement cascade is activated through the classical pathway by antibodies bound to tissue antigens. With regard to complement activation, IgM class antibodies are particularly efficient. 118 This activation produces C5a, a nociceptive mediator we have shown to support allodynia through the activation of C5a receptors on sensory neurons.28,30 C5a also causes the migration and degranulation of mast cells in skin that we and others have linked to pain in CRPS patients and in the fracture/cast model.41,74 Separately, complement activation leads to the formation of MAC complexes thus damaging peripheral nerves.119,120 In fact, cutaneous neurite loss has been reported in CRPS patients, 121 and we have shown skin and sciatic nerve MAC levels to be increased in B cell-dependent fashion in the mouse tibial fracture CRPS model. 115
The vexing question of regional symptoms
One of the principal characteristics of CRPS is that in the majority of cases a single limb is involved, although spread, most often to the contralateral limb, is sometimes seen. 122 How are symptoms limited to a single limb if contributing autoimmune antibodies are present in serum? We are only beginning to understand how regional autoimmunity might function, but it is notable that in the mouse fracture/cast immobilization model we found deposits of immunoglobulins in the skin and sciatic nerves ipsilateral but not contralateral to the fractures. 115 Furthermore, in both humans as well as animal models, Langerhans cell accumulation was greater in the skin of the affected compared to the contralateral limbs75,76 although, as mentioned above, the analysis of skin from patients with longstanding CRPS (years) did not show such changes. 69 In the setting of CRPS, new antigens (neoantigens) could be regionally expressed, posttranslational modifications of existing proteins might render them immunogenic such as by citrullination or carbamylation, the compartmentalization of proteins might be altered or the target antigens might lose their “immune privileged” status in the setting of CRPS by virtue of a change in a tissue barrier. Each has been posited as an explanation for autoimmunity in other disease states, though none of these mechanisms have been conclusively demonstrated to occur in CRPS.
Neural control of autoimmune mechanisms in CRPS
An intriguing possibility is that regional changes in peptidergic and sympathetic function in the affected limbs could be supporting autoimmune-related changes similar to how these systems support changes in innate immune function as previously discussed. Neural control of adaptive immunity is a novel concept, but one for which evidence is beginning to accumulate. Using the fracture/cast mouse model of CRPS, it was shown that the accumulation of immunoglobulins in the skin ipsilateral to injury was dependent on NK1 receptor signaling. Likewise, the sera of CRPS model mice in which the SP coding tac1 gene had been deleted was not capable of reconstituting nociceptive sensitization in muMT fracture/cast model mice, and the tac1−/− mice did not display IgM accumulation in skin, peripheral nerves, or spinal cord tissue after fracture as was observed in the wild-type mice. The results were similar for mice in which CGRP signaling was disrupted. 76 Interestingly, SP signaling has been implicated in the disruption of immune privilege in autoimmune diseases of the CNS and in regionally localized conditions like alopecia areata.123,124 Furthermore, it was observed that the enhanced postfracture expression of one confirmed autoantigen, Krt16, was dependent on intact SP and CGRP signaling. 76
Loss of immune privilege of the CNS including the spinal cord and higher centers is particularly intriguing. Most studies to this point have examined autoimmune responses against peripheral nerves and other tissues, but IgM antibodies are found in spinal cord tissue in the rodent fracture model. 76 Pain and other consequences might result from interactions of autoantibodies with specific CNS targets, for example, ion channels, cell surface receptors, or might modulate nociception through the fixation of complement. Elevated spinal levels of C5a in nerve injury models have been linked to nociceptive sensitization. 125
Dysfunction of the sympathetic nervous system has been observed in some CRPS patients, and the older name for the syndrome “Reflex Sympathetic Dystrophy” highlighted this association. Furthermore, it has been reported that sympathectomy can reduce the inflammation and pain associated with the classic autoimmune condition rheumatoid arthritis.126,127 In animal models of rheumatoid arthritis, sympathetic signaling through β2-AR on B cells is responsible for stimulating autoantibody production particularly in the acute phases of the condition.128,129 The precise mechanisms for these effects are unclear, though both B cell and Langerhans cell activity can be regulated by norepinephrine through the activation of α and β adrenergic receptors.78,130 Thus, regionally activated neuroimmune networks involving peptidergic, sympathetic, or both systems may play a role in the autoimmune manifestations of CRPS.
Conclusions
CRPS is an enigmatic syndrome for which no convincingly effective treatments exist. One of the most confounding aspects of the syndrome has been the disparate mix of manifestations involving multiple tissues thereby defying the identification of a clear unifying etiology. Recent evidence suggests that the interrelated phenomena of autoinflammation and autoimmunity may be the basis for this syndrome. Dysfunction of neuropeptide-containing afferent neurons and sympathetic fibers may support the inflammation and autoimmune phenomena, at least in CRPS Type I where no clear nerve lesion is present. Much less information is available regarding mechanistic overlap with CRPS Type II, although nueropeptide dysregulation seems to be involved.
131
In Figure 1, a summary of the interactions of neuropeptidergic and sympathetic transmitters with key cells participating in CRPS-related autoimmunity and autoinflammation is presented. An attractive aspect of this hypothesis is that a number of new therapeutic approaches could be considered to combat autoinflammation and autoimmunity. For example, biologic anti-cytokine agents (TNFα, IL-1β, IL-6, etc.) are available and could be tested in clinical populations. Likewise, agents targeting components of the adaptive immune system such as rituximab (anti-CD20) or calcineurin inhibitors might be tested. Peptidergic and sympathetic signaling blockers may reduce both autoinflammatory and autoimmune responses. One challenge, however, will be to weigh the potential benefits of these powerful immunological agents against susceptibility to infection and certain forms of cancer, problems currently faced by patients taking these drugs to relieve rheumatological conditions. Still, for patients not improving with more conservative therapies or time, immunomodulatory agents might at some point become viable options for reducing the pain, disability, and other consequences of CRPS.
A neuroinflammatory model of Complex Regional Pain Syndrome. Data from patients and laboratory models suggest both neuropeptides and autonomic nervous system activity contribute to the pathogenesis of CRPS. Antigen-presenting cells, epithelial cells and mast cells may all be contributing components. NE: norepinephrine; SP: Substance P; β2: β2 adrenergic receptor.
Footnotes
Author Contributions
JDC conceived, outlined, and wrote substantial portions of the manuscript. VLT and MT provided discussion and feedback on the manuscript’s goals, read the manuscript, and provided text, references, and comments. WSK provided extensive comments, text, and revisions of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Department of Veteran Affairs I01RX001475 and NIH NS072143 and NS094438.