
Abstract
Keywords
Introduction
People with learning disabilities and autistic adults are at a significantly increased risk of premature mortality. In England alone, an estimated 1.3 million people have learning disabilities, and 1.2 million are autistic adults (UCL, 2023). Similar disparities have been reported globally, including in Europe, North America, and Australasia (REFS) According to the NHS Learning Disability Mortality Review Programme (LeDeR) (NHS, 2019), individuals with a learning disability die on average 22 years earlier than the general population. Both the LeDeR programme annual report 2023 (King’s College London, 2023) and the NHS Long Term Plan (NHS, 2024) emphasise the urgent need to improve the health and wellbeing of people with a learning disability and autistic adults, aiming for happier, healthier, and longer lives. This health disparity is partly due to barriers to accessing healthcare support (Allerton and Emerson, 2012; Hodgson et al., 2025). Adults lacking the capacity or capability to attend appointments often miss critical diagnoses and treatments, a concern highlighted in multiple Serious Case Reviews, Domestic Homicide Reviews, and Safeguarding Adult Reviews (Berry, 2022; Norfolk Safeguarding Adults Board, 2021; Preston-Shoot, 2020).highlighted in multiple Serious Case Reviews, Domestic Homicide Reviews, and Safeguarding Adult Reviews (Berry, 2022; Norfolk Safeguarding Adults Board, 2021; Preston-Shoot, 2020).
While learning disabilities and autism are distinct conditions with unique challenges, there is significant overlap in the experiences of individuals within both groups. It is believed 1 in 3 autistic people (up to 40% in adults autistic adults) also have learning disabilities (Autistica, 2024), which affects how they navigate healthcare and face systemic barriers to accessing support. Addressing these groups together allows for a more comprehensive understanding of how healthcare systems fail to accommodate neurodivergent individuals as a whole, particularly when it comes to communication, sensory sensitivities, and dependence on caregivers. Evidence shows that people with a learning disability and autistic adults are more likely to miss healthcare appointments than the general population (Chapman et al., 2018). While some may choose not to attend, others depend on family or care providers to support their attendance. Generally, in general practice alone, 15.4 million appointments are missed annually in England, costing the NHS £216 million (NHS England, 2019; NHS England, 2023c). Notably, less than three-quarters of people with a learning disability attended their annual health check in 2020-21 (there are plausible grounds for caution in interpretation as this data was collected during the Coronavirus outbreak) (NHS Digital, 2022), leading to possible gaps in preventative healthcare screening. General practice policies exacerbate this issue with patients removed from practice registers after as few as three missed appointments in England (Daily Gazette Standard Essex County, 2018; First 4 Health Group; Horizon Healthcare Derby). However, it is important to consider that the 2021-22 period was uniquely impacted by the COVID-19 pandemic, which may have affected both attendance reporting and actual attendance in healthcare settings and the issue of the challenges faced of reporting actual attendance figures, such as inconsistent recording of attendance (Carey et al., 2017).
Research has identified various barriers that people with a learning disability and autistic adults face in attending appointments such as communication and socio-relational issues (Van Schrojenstein and Valk, 2005). Aggregating and synthesising existing literature is essential to identify the most common and critical obstacles. Additionally, primary care settings are often unwelcoming to autistic adults due to unpredictable environments, sensory overload, and communication difficulties. Many struggle with crowded waiting rooms or the uncertainty of appointments. Adjustments such as quieter waiting areas or clearer communication can improve experiences, but these are inconsistently applied, leading to delayed diagnoses and treatment (Mason et al., 2022; NHS England, 2023b). Similarly, people with learning disabilities face diagnostic overshadowing, where health issues are misattributed to their disability. Despite NHS guidelines calling for reasonable adjustments, they remain inconsistently implemented across primary care, exacerbating health disparities (NHS England, 2023b).
To address these barriers to accessibility, reasonable adjustments can be made. Reasonable adjustments are necessary to ensure individuals can access, enjoy, and complete their healthcare appointments. The Equality Act 2010 also mandates adjustments to prevent discrimination against disabled people, including those with learning disabilities and autism (legislation.gov.uk, 2024). Initiatives like the North East and Cumbria Learning Disability Network’s ‘Reasonable Adjustments Preventing Adult Not Brought’ work programme are examples of efforts being made to support access. This focuses on making practical changes in healthcare settings to ensure accessibility for people with a learning disability and autistic adults, minimising missed appointments and improving health outcomes. This includes development of a new code ‘adult not brought to appointment (ANB)’ as of July 2023 (Learning Disability Network, 2024).
Working with patients and public contributors the review team have explored the barriers and enablers they faced when accessing healthcare appointments in primary care. With this group a co-designed art piece (Figure 1) was created, capturing their experiences and where they felt adjustments could have been made. Artwork results.
The ANB code and strategy originated out of the North-East of England, developed and championed by a GP Clinical Lead and supported by the North East and Cumbria Learning Disability Network. The strategy and code for the North-East North Cumbria Integrated Care System originally aimed to identify and support adults who may need support attending healthcare appointments. However, this code has the potential for widescale roll-out and applicability beyond learning disabilities, such as adults with dementia. Traditionally, ’Did Not Attend (DNA)’ was often used when an appointment was missed by an adult. This code however does not fully capture why patients are not brought to appointments, particularly people with a learning disability and autistic adults who may require assistance to attend. The distinction between the original code and ANB is critical as it addresses gaps in service for individuals who depend on assistance to access healthcare, providing a foundation for more targeted and supportive healthcare delivery for populations with heightened vulnerability, such as those with learning disabilities and autism. Given the severe health inequalities faced by people with a learning disability and autistic adults, coupled with long NHS waiting lists, reducing the number of missed appointments is crucial. Listening to patients and the public who have autism or a learning disability there is a need to ensure change is supported and is grounded in evidence. Timely access to healthcare is vital for maintaining the health of these populations.
This scoping review aimed to explore the barriers and facilitators affecting the attendance of people with a learning disability and autistic adults at healthcare appointments. Furthermore, we aimed to meta-aggregate the synthesised findings using a social-ecological model (SEM) lens (Erickson et al., 2024). The SEM serves as a comprehensive framework for examining the diverse factors impacting healthcare accessibility at multiple levels. The SEM categorises influences on health behaviours across individual, interpersonal, organisational, and policy layers, highlighting how each level interrelates to shape healthcare experiences. This model is particularly suitable for understanding the healthcare barriers faced by people with learning disabilities and autism, as it encompasses individual needs, relationship dynamics, community support systems, organisational structures, and policy implications. (Garney et al., 2021). By synthesising evidence using the SEM model we hope this scoping review can be used alongside the ANB strategy and code to help further develop and implement the ANB strategy and inform potential reasonable adjustments that may be needed.
Methods
Design
This review followed the Joanna Briggs Institute (JBI) Scoping Review Network, Manual for Evidence Synthesis for the development of a review protocol, methods, and reporting (Aromataris et al., 2024). This review applied the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (Page et al., 2021).
Search strategy
The systematic search strategy was informed by the PEOS (population, exposure, outcome, and study design respectively) framework (University of Suffolk), where the population of interest was adults over the age of 18 with a learning disability or autistic adult over the age of 18 residing in the UK; the exposure was attendance or non-attendance to healthcare clinical appointments; the outcome was missed clinical appointments; and the study design was any primary empirical research design in which qualitative data was collected and could be explicitly separated from all other reported data. The search terms were developed through discussions within the review team, prior knowledge of policy, and pilot searches to identify relevant keywords and terms. For a full list of search terms please see Supplemental material file 1 (P- People with learning disabilities and autistic adults, E − non-attendance, O– Missed healthcare, S-open). Searches were initially run in March 2023 by MC and re-run in June 2024 by ET.
The following ten electronic databases were searched: SCOPUS, MEDLINE, Allied and Complementary Medicine Database (AMED), CINAHL Complete, CINAHL Ultimate, APA PsycArticles, APA PsycInfo, Dentistry and Oral Sciences Source, SPORTDiscus, and Psychology and Behavioral Sciences Collection. Searches were restricted to UK-based studies and published in English to ensure relevancy and applicability to UK health policy and practice. Hand and citation searches of included studies were conducted using Google Scholar.
Studies were included if they post-2005, involved a UK-based population of adults with a learning disability, autistic adults, carers (paid or unpaid), or health care professionals (HCP), aged 18 years or older. Included studies also need to have a qualitative component (of any data collection method) which identified the lived experiences of clinical appointment accessibility. If primary qualitative data was presented with quantitative data or with those not in the target population, included studies needed to present a clear separation of data between populations.
Focusing on the UK allowed the review to examine accessibility within the context of the UK healthcare system, which has unique policies, structures, and care pathways that may not be directly comparable to those in other countries. Additionally, papers from 2005 onwards were selected to ensure that the findings reflected more current practices, policies, and healthcare experiences, particularly considering significant changes in healthcare provision and disability rights after this period.
Study selection
All results were uploaded and managed using Rayyan. This tool was used to establish any duplicates in the results which were screened by three reviewers (KK, EE, ET) for accuracy and removed where appropriate. Following deduplication from the original and updated searches, stage 1 (title and abstract screening) was completed by five reviewers (EE, KK, ET, ELG, MC), working independently on 100% of the included studies, using the inclusion criteria. Any disagreements were resolved with a discussion with a third reviewer (JH). All studies retained following stage 1, were then screened as full-text articles by the same reviewers (EE, KK, ET, ELG, MC) under the same conditions. Disagreements were resolved by the same third reviewer (JH). All decisions made at stage 2, were recorded and presented in the PRISMA diagram.
Data extraction
A data extraction form was developed within Microsoft Excel to capture: participant characteristics (including if they were a person, carer, or healthcare professional and their experience of learning disabilities or autism), location and region, aims, design, data collection, analysis method, qualitative data, and data relevant to assessment of methodological quality. The data extraction form was piloted by one reviewer (MC). Study characteristics data were subsequently extracted by two reviewers (MC, ET) and verified for accuracy by a second reviewer (ELG, ES, JB, JH). Any discrepancies in data extraction were resolved through discussion.
Data synthesis
Data was synthesised following the methods of meta-aggregation as outlined by the JBI manual (Aromataris et al., 2024) and Microsoft Excel used to extract findings. Meta-aggregation follows five broad steps including:
Step 1 – Data extraction. Data are extracted from the findings section and coded to include all themes, topics, relationships, and results reported. Extracted data are verbatim of the presented text including the authors presentation summary and illustrative quotes (where available).
Step 2 – Data assessment. All extracted data are then assessed as either ‘unequivocal’ (‘findings accompanied by an illustration that is beyond reasonable doubt and; therefore not open to challenge’), ‘credible’(‘findings accompanied by an illustration lacking clear association with it and therefore open to challenge’), or ‘not supported’ (‘findings are not supported by the data’) based on the evidence available to support the narrative. Data were extracted by two reviewers (MC, ET) and checked for accuracy by a second (ELG, JB).
Step 3 – Categorisation of similar data. Data are arranged into categories of ‘similar data’ (data of a comparable narrative). Categories of similar data are developed based on the narrative presented within the study and does not involve the reviewer’s re-interpretation of the primary data reported. For this review, the socioecological model (SEM) was applied to provide a framework to the categorisation of similar data (Khan et al., 2021). The application of the SEM provided support to organise the narrative presented, explore the different levels of accessibility, and the context within which experiences of clinical appointments are categorised. All extracted findings were coded to the SEM by five reviewers working independently (ELG, ES, JB, MC, ET).
Step 4 – Synthesis of findings. Step 4 develops the categories of similar data from step 3 by grouping categories based on the overarching narrative of the whole data set. As this review applied the SEM, the synthesis of findings occurred within each of the level of the SEM and provided the narrative of the data at each level. The synthesis of findings does allow for some reviewer interpretation and all synthesis of findings were discussed at length between reviewers to ensure grounding in study data.
Step 5 – Development of recommendations. The final step used the synthesis of findings to inform the development of recommendations. Recommendations provide a single summary of the narrative presented and provided the outline for future practice and policy. The development of recommendations within this review was completed through discussions within the review team.
Assessment of methodological quality
Methodological quality assessment was determined using the Checklist for Qualitative Research (The Joanna Briggs Institute, 2017). This checklist apprised the specific components of each included study to assess for the possible bias in design, conduct, and analysis. This checklist was applied by multiple reviewers working independently (ES, EG, JB, JH, MC, ET).
Results
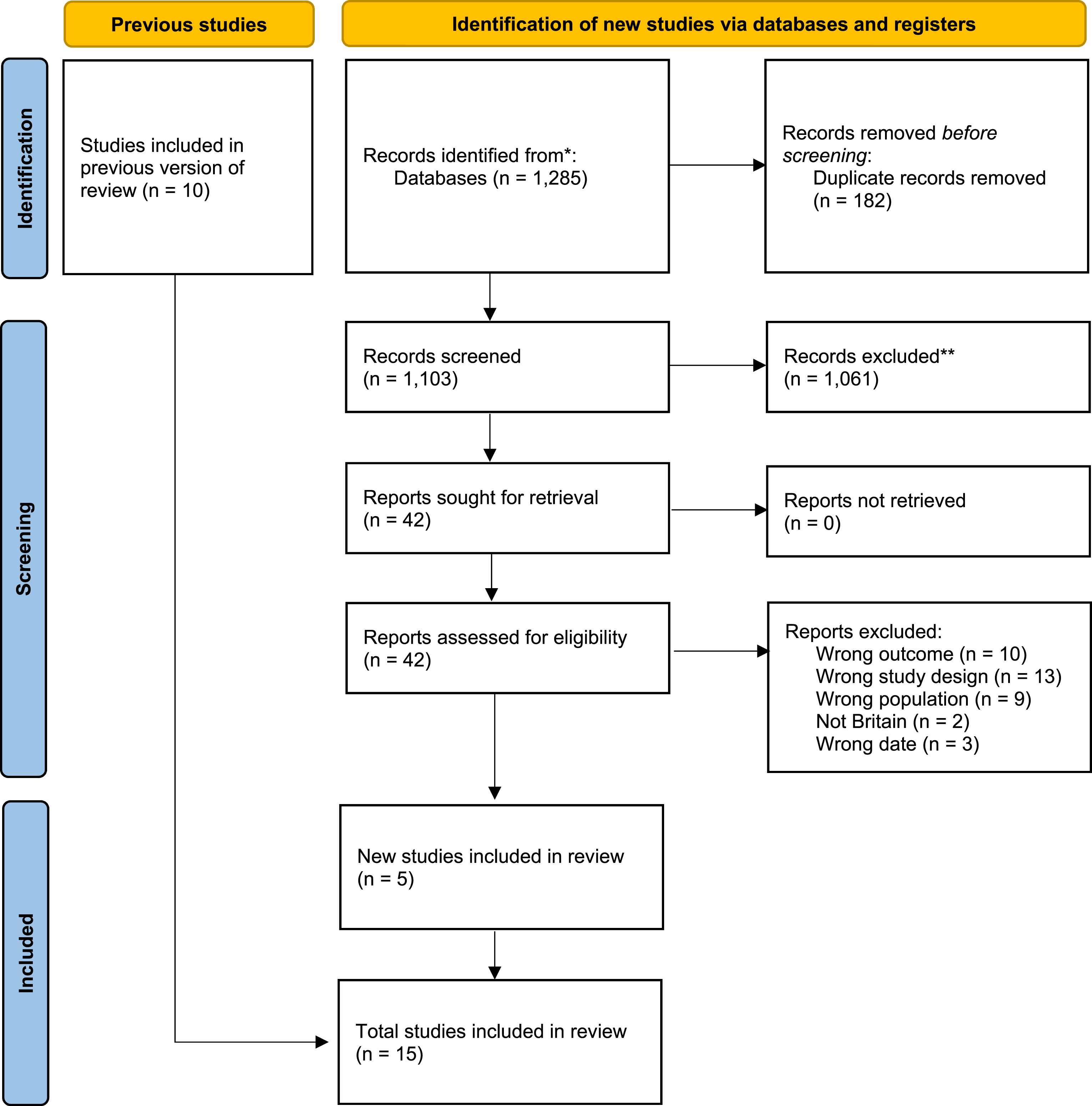
From the initial search in March 2023 and the updated search in June 2024, a total of 1,727 studies were identified following database searches, with 222 duplicates, leaving a total of 1,505 studies screened at stage 1. Of the 1,505 studies screened at stage 1, there were 80 taken to stage 2 screening. A final fifteen studies were included in this scoping review and meta-aggregation. A completed PRISMA flowchart has been used to detail the study selection process in Figures 2 and 3. Original PRISMA diagram. Updated PRISMA diagram.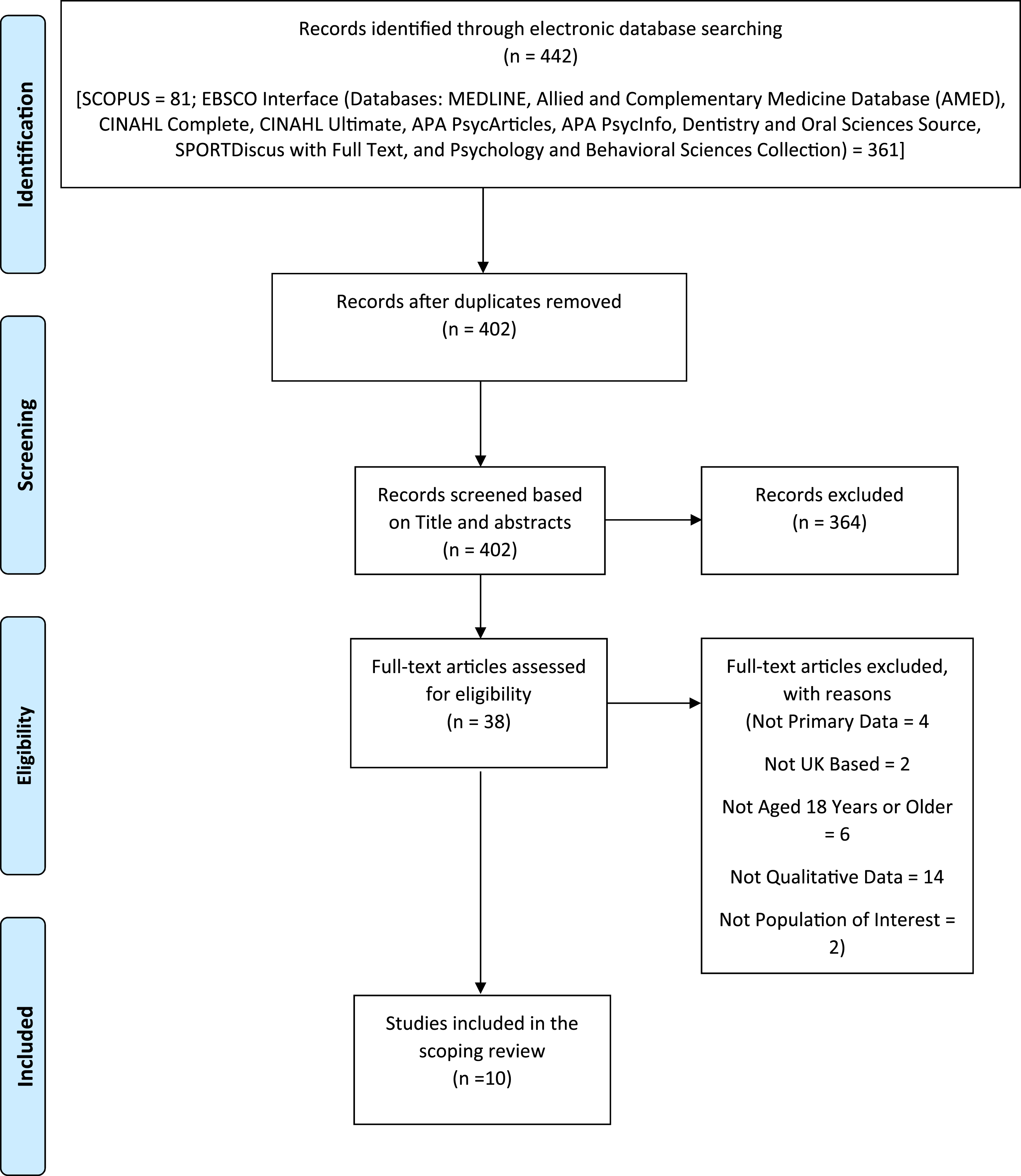
Study characteristics
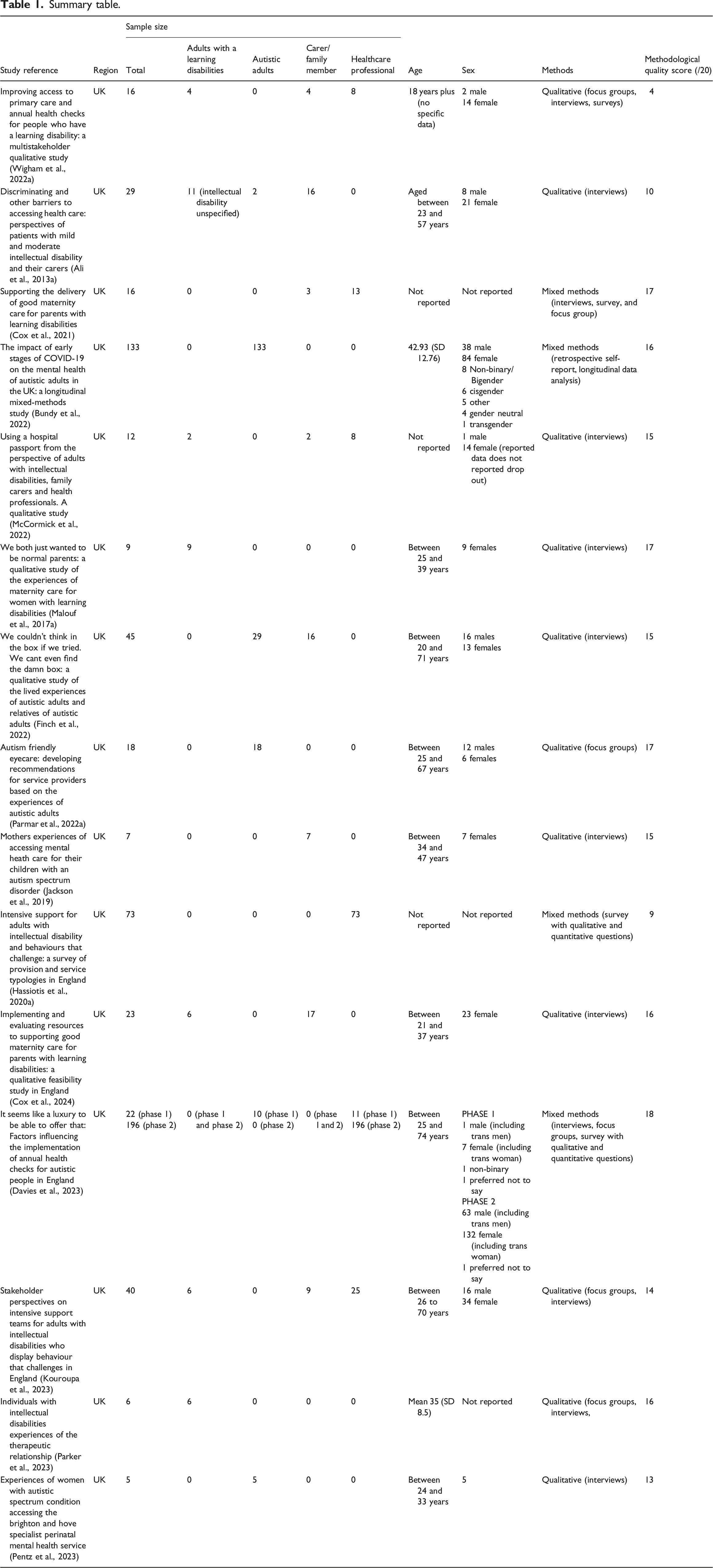
Due to the eligibility criteria, all 15 included studies were based in the UK (Ali et al., 2013a; Bundy et al., 2022; Cox et al., 2021, 2024; Davies et al., 2023; Finch et al., 2022; Hassiotis et al., 2020a; Jackson et al., 2019; Kouroupa et al., 2023; Malouf et al., 2017a; Mccormick et al., 2022; Parker et al., 2023; Parmar et al., 2022a; Pentz et al., 2023; Wigham et al., 2022a), with thirteen published in 2020 or thereafter. Twelve studies were of qualitative design (Wigham et al., 2022a; Ali et al., 2013a; Malouf et al., 2017a; Mccormick et al., 2022; Finch et al., 2022; Parmar et al., 2022a; Hassiotis et al., 2020a; Jackson et al., 2019; Kouroupa et al., 2023; Cox et al., 2024; Parker et al., 2023; Pentz et al., 2023), and three mixed methods (Bundy et al., 2022; Cox et al., 2021; Davies et al., 2023). Eleven studies used interviews as the data collection method (Ali et al., 2013a; Cox et al., 2021, 2024; Davies et al., 2023; Finch et al., 2022; Jackson et al., 2019; Kouroupa et al., 2023; Malouf et al., 2017a; Mccormick et al., 2022; Parker et al., 2023; Pentz et al., 2023), two used focus groups (Parmar et al., 2022a; Wigham et al., 2022a), and two used surveys (Bundy et al., 2022; Hassiotis et al., 2020a). To analyse data, ten studies used thematic analysis (content, framework, general) (Wigham et al., 2022a; Ali et al., 2013a; Cox et al., 2021; Bundy et al., 2022; Mccormick et al., 2022; Finch et al., 2022; Hassiotis et al., 2020a; Parmar et al., 2022a; Kouroupa et al., 2023; Pentz et al., 2023), three used interpretative phenological analysis (Parker et al., 2023; Malouf et al., 2017a; Jackson et al., 2019), and two used framework analysis (Cox et al., 2024; Davies et al., 2023).
A total of 686 participants provided data across the fifteen studies, with age data reported in ten studies (Bundy et al., 2022; Cox et al., 2024; Davies et al., 2023; Finch et al., 2022; Jackson et al., 2019; Kouroupa et al., 2023; Malouf et al., 2017a; Parker et al., 2023; Parmar et al., 2022a; Pentz et al., 2023) ranging from age 21 to 74 years. There were 325 (47.4%) participants reported as female, 158 (23%) as male, and four (0.6%) as other in twelve of the included studies. Three studies did not report on this data (29%) (Cox et al., 2021; Hassiotis et al., 2020a; Parker et al., 2023). Three studies involved autistic people only (Bundy et al., 2022; Parmar et al., 2022a; Pentz et al., 2023), and two studies involved people with a learning disability only (Malouf et al., 2017a; Parker et al., 2023). One study involved autistic people and carers (Jackson et al., 2019) and one study involved people with a learning disability and carers (Ali et al., 2013a). One study involved autistic people, people with a learning disability and carers (Finch et al., 2022). Three studies involved people with a learning disability, carers, and HCPs (Cox et al., 2021; Mccormick et al., 2022; Wigham et al., 2022a). One study involved autistic people, people with a learning disability, carers, and HCP (Hassiotis et al., 2020a). One study involved people with a learning disability and HCP (Cox et al., 2024). One study involved autistic people and HCP (Davies et al., 2023). Finally, one study involved autistic people, carers, and HCP (Kouroupa et al., 2023).
Quality assessment
Ten studies were deemed to have high levels of methodological quality (answering yes to more than eight out of ten questions) (Davies et al., 2023; Parker et al., 2023; Pentz et al., 2023; Kouroupa et al., 2023; Cox et al., 2021, 2024; Bundy et al., 2022; Parmar et al., 2022a; Malouf et al., 2017a; Jackson et al., 2019), three studies as medium levels (answering between four and seven questions as yes) (Ali et al., 2013a; Finch et al., 2022; Mccormick et al., 2022), and two as poor levels (Hassiotis et al., 2020a; Wigham et al., 2022a), based on the JBI quality assessment checklist. Three studies scored yes to all ten questions of the JBI checklist (Cox et al., 2021; Bundy et al., 2022; Jackson et al., 2019). Six studies provided evidence of congruity between their philosophical perspective and research methodology (Bundy et al., 2022; Cox et al., 2021, 2024; Davies et al., 2023; Jackson et al., 2019; Parker et al., 2023). Twelve studies were deemed to have congruence between their research methodology and aims and provided evidence of congruence between research methodology, data collection methods, data analysis, and interpretation of results (Davies et al., 2023; Parker et al., 2023; Pentz et al., 2023; Kouroupa et al., 2023; Cox et al., 2021, 2024; Bundy et al., 2022; Mccormick et al., 2022; Malouf et al., 2017a; Parmar et al., 2022a; Finch et al., 2022; Jackson et al., 2019). Five studies provided an overview of the researcher approach and the influences between research and researcher (Ali et al., 2013a; Cox et al., 2021; Bundy et al., 2022; Parmar et al., 2022a; Jackson et al., 2019). Twelve studies adequately represented all participants in the use of illustrative quotes (Ali et al., 2013a; Bundy et al., 2022; Cox et al., 2021, 2024; Davies et al., 2023; Finch et al., 2022; Jackson et al., 2019; Kouroupa et al., 2023; Malouf et al., 2017a; Mccormick et al., 2022; Parker et al., 2023; Parmar et al., 2022a; Pentz et al., 2023), with thirteen studies providing sufficient evidence for the research (Ali et al., 2013a; Bundy et al., 2022; Cox et al., 2021, 2024; Davies et al., 2023; Finch et al., 2022; Jackson et al., 2019; Kouroupa et al., 2023; Malouf et al., 2017a; Mccormick et al., 2022; Parker et al., 2023; Parmar et al., 2022a; Wigham et al., 2022a). Finally, fourteen studies provided conclusions that were justified based on the research presented (Ali et al., 2013a; Bundy et al., 2022; Cox et al., 2021, 2024; Davies et al., 2023; Finch et al., 2022; Hassiotis et al., 2020a; Jackson et al., 2019; Kouroupa et al., 2023; Malouf et al., 2017a; Mccormick et al., 2022; Parker et al., 2023; Parmar et al., 2022a; Pentz et al., 2023).
Results of the meta-aggregation
A total of 94 individual findings were extracted from the 15 included studies, all deemed as ‘unequivocal’ or ‘credible’. While some studies displayed lower methodological quality, all findings included were deemed ‘credible’ or ‘unequivocal’ based on evidence provided, ensuring their validity for meta-aggregation despite methodological limitations. Data were coded into 49 facilitators and 42 barriers to the accessibility of healthcare appointments and 3 were coded as both facilitators or barriers depending on population and context. From the data extracted, 11 syntheses of findings were created within the four levels of the SEM. These 11 syntheses of findings are outlined in detail below and informed the recommendations for future practice. Figure 4 outlines the results of the meta-aggregation showing a pictorial representation of the levels of the SEM at the centre (individual, relationships, society/policy, and organisation). Around the centre is the 11 synthesised findings (e.g. Training of HCP and Support Infrastructure). Around these are 70 barriers and facilitators coloured either red, green or white. Findings are presented based on the data available and report on the barriers faced by both people with learning disabilities and autistic adults. Results from the meta-aggregation.
Individual
At the individual level of the SEM, there were two overarching narratives: training of HCPs and impact of positive attitudes. Data within the training of HCPs category included five barriers, one facilitator and two context dependent points, from nine papers (Cox et al., 2021, 2024; Davies et al., 2023; Kouroupa et al., 2023; Malouf et al., 2017a; Mccormick et al., 2022; Parker et al., 2023; Parmar et al., 2022a; Pentz et al., 2023).
Within the papers reporting on this area, there was a need to ensure appropriate training for HCPs, with authors reporting a lack of specialist knowledge specifically around learning disabilities impacting the delivery of care (there was a lack of data to comment on knowledge of autism) (30, 39,40). A lack of understanding also led to barriers delivering information, or HCPs did not have the appropriate knowledge to adjust their delivery of information to match the person’s needs. This created a reported sense of stigma against people with a learning disability with a suggestion that HCPs should be routinely considering if a person requires reasonable adjustments. Encouragingly it was reported within one study that HCPs wanted more awareness, specialised training in this area (Cox et al., 2024; Davies et al., 2023; Mccormick et al., 2022).
The second category, impact of positive attitudes, recognised that the approach and attitudes of HCPs affected the people with a learning disability or autistic adults engagement with care (Cox et al., 2021; Malouf et al., 2017a; Kouroupa et al., 2023; Pentz et al., 2023; Parker et al., 2023). HCPs who held positive attitudes, provided continuity of care, were flexible with times and appointment locations, were viewed as more supportive. Those HCPs who did not have a positive attitude and increased perceptions of stigma affected the care offered/received.
Relationships
The relationship level of the SEM contained the largest amount of extracted with 32 data points from 13 studies (Ali et al., 2013a; Bundy et al., 2022; Cox et al., 2021, 2024; Davies et al., 2023; Finch et al., 2022; Kouroupa et al., 2023; Malouf et al., 2017a; Mccormick et al., 2022; Parker et al., 2023; Parmar et al., 2022a; Pentz et al., 2023; Wigham et al., 2022a). There were three syntheses relating to the relationship level; appointment environment, communications between HCPs and person, and the need for more HCP training.
The appointment environment was a critical point when people had to engage to access care and support (Ali et al., 2013a; Bundy et al., 2022; Davies et al., 2023; Kouroupa et al., 2023; Parker et al., 2023; Parmar et al., 2022a; Wigham et al., 2022a). Included studies suggested current booking systems, such as automated telephone based or transport booking, provided a significant barrier (Ali et al., 2013a; Davies et al., 2023; Kouroupa et al., 2023). People felt using an online self-service system or email option would be useful as appointment reminders (Parmar et al., 2022a). People felt this would allow them more time to consider options and time to respond to questions (Ali et al., 2013a). People also felt having reasonable adjustments such as the option to book a longer appointment time was positive and would benefit from having the option of a remote appointment method (Wigham et al., 2022a; Bundy et al., 2022; Kouroupa et al., 2023; Parker et al., 2023).
The communication between HCPs and people with a learning disability or autistic adults was discussed in detail within the included papers (12 facilitators and 10 barriers) (Ali et al., 2013a; Cox et al., 2021, 2024; Davies et al., 2023; Finch et al., 2022; Kouroupa et al., 2023; Malouf et al., 2017a; Mccormick et al., 2022; Parker et al., 2023; Parmar et al., 2022a; Pentz et al., 2023; Wigham et al., 2022a). Included studies reported that an essential facilitator was the ability to develop a positive and trusting relationship between HCPs and the person they were supporting (Wigham et al., 2022a; Ali et al., 2013a; Cox et al., 2021, 2024; Mccormick et al., 2022; Malouf et al., 2017a; Finch et al., 2022; Parmar et al., 2022a; Davies et al., 2023; Parker et al., 2023; Pentz et al., 2023). HCPs need to ensure they could be flexible and accommodating of any reasonable adjustments required and that they took the time to understand these needs and work with the individual (Ali et al., 2013a; Cox et al., 2021; Kouroupa et al., 2023; Parmar et al., 2022a). There was a need to ensure there was use of simplified language, which was jargon free, and where possible, a choice of communication method offered (Makaton, written, or visual communication for example) (Cox et al., 2021, 2024; Davies et al., 2023; Parmar et al., 2022a; Wigham et al., 2022a).
Studies reported that people wanted the opportunity to ask questions or seek clarification on what will happen in an appointment, or where equipment would be used, allowing individuals the chance to interact with HCPs before the appointment (to decrease sense of unfamiliarity and fear) (Ali et al., 2013a; Davies et al., 2023; Malouf et al., 2017a; Parmar et al., 2022a). Many of the barriers extracted from included studies centred around poor communication people felt they had with HCPs and this fostered a sense of inequity and disempowerment (Ali et al., 2013a; Finch et al., 2022; Kouroupa et al., 2023; Malouf et al., 2017a; Wigham et al., 2022a). The poor communication had a negative effect on both the relationship with the individual HCP but also across all healthcare appointments (Ali et al., 2013a; Kouroupa et al., 2023; Parmar et al., 2022a; Wigham et al., 2022a).
Finally, there was a narrative around the need for additional training in the use of hospital passports and more generally around appointments (Davies et al., 2023; Kouroupa et al., 2023; Malouf et al., 2017a; Mccormick et al., 2022; Parker et al., 2023). The use of hospital passports (healthcare passports) are helpful for people with a learning disability or autistic adults when accessing in-patient healthcare, where it will detail information about communication preferences or reasonable adjustments to HCPs (Mencap). The hospital passport is a tool to aid communication, however, the findings suggest that HCPs did not always read them and faced issues with the legality or risk management of their implementation (Mccormick et al., 2022). Therefore, additional training would be required to address knowledge and practical gaps to support the use and engagement with this tool.
Organisational
Within the organisational level of the SEM, there were four syntheses consisting of 21 facilitators and 12 barriers from twelve studies (Ali et al., 2013a; Bundy et al., 2022; Cox et al., 2021, 2024; Davies et al., 2023; Finch et al., 2022; Kouroupa et al., 2023; Mccormick et al., 2022; Parker et al., 2023; Parmar et al., 2022a; Pentz et al., 2023; Wigham et al., 2022a).
The structure of appointments offered by healthcare providers impacted the accessibility of care for people with a learning disability or autistic adults (Ali et al., 2013a; Cox et al., 2024; Kouroupa et al., 2023; Parker et al., 2023; Parmar et al., 2022a; Pentz et al., 2023; Wigham et al., 2022a). Allowing flexibility in booking (for example additional time slots or attend with someone else) was seen as a positive facilitator (Cox et al., 2024; Kouroupa et al., 2023; Parker et al., 2023; Pentz et al., 2023; Wigham et al., 2022a). Organisations need to ensure there are systems in place to allow for the booking of appointments to be with the same practitioner and where appropriate, there is a learning disability liaison nurse available to provide support (Parmar et al., 2022a). The nurse could then assist with understanding information, arranging follow-up testing or reasonable adjustments with other HCPs to facilitate engagement (Ali et al., 2013a; Parmar et al., 2022a).
At the organisational level, included studies outlined barriers with appointment waiting times and spaces (Bundy et al., 2022; Wigham et al., 2022a). The narrative around this suggested there needs to be allocated waiting room which are tailored to the needs of people with a learning disability and autistic adults (Wigham et al., 2022a). Studies suggested that there was significant value in ensuring that people are not made to wait long periods for appointments and that they are seen promptly and with continuity of support (Bundy et al., 2022; Wigham et al., 2022a).
Thirdly within this level, the follow up support was an important factor in the accessibility (Cox et al., 2024; Davies et al., 2023; Finch et al., 2022; Kouroupa et al., 2023; Mccormick et al., 2022; Parmar et al., 2022a; Pentz et al., 2023; Wigham et al., 2022a). Studies concluded that it was important to ensure there was a follow up support plan in place, possibly with the inclusion of a learning disability nurse, to aid support offered as some felt there was a lack of continuity in aftercare (Davies et al., 2023; Mccormick et al., 2022; Parker et al., 2023; Parmar et al., 2022a; Wigham et al., 2022a). Providing a planned follow up may also reduce the issued faces with having to encounter multiple HCPs, which was reported to reduce the likelihood of attending in the future (Cox et al., 2024; Davies et al., 2023; Kouroupa et al., 2023; Parmar et al., 2022a).
Finally, within the organisational level of the SEM, ensuing information that is provided to people is accessible was a key facilitator to the accessibility of healthcare appointments (Ali et al., 2013a; Cox et al., 2021, 2024; Davies et al., 2023; Kouroupa et al., 2023; Mccormick et al., 2022; Parmar et al., 2022a; Wigham et al., 2022a). Included studies presented the narrative that HCPs need to ensure they could accurately and appropriately deliver healthcare information to people with a learning disability and autistic adults. Information provided should avoid using jargon and be presented in a format (visual or audio for example) based on the preferences of the individual (Ali et al., 2013a; Cox et al., 2021, 2024; Mccormick et al., 2022; Wigham et al., 2022a). The use of hospital passports could be used as a useful tool, where information is in an easy-carry format and can be both understood by the individual and the HCP, however, more training is needed for HCP staff in this area (Davies et al., 2023; Mccormick et al., 2022; Wigham et al., 2022a).
Society/policy
The final level of the SEM is the society/policy level, which included two synthesised narratives, the set-up of care services and supporting carers and included four barriers and seven facilitators. Included studies supported the narrative of the implementation of facilitators in the set-up of care services. These included creating a better code for medical records which flagged reasonable adjustment needs, the role of primary care in identifying needs in a preventative capacity and ensuring appointment prioritisation for long term conditions within this population (Ali et al., 2013a; Cox et al., 2024; Davies et al., 2023; Kouroupa et al., 2023; Wigham et al., 2022a). This narrative suggested the need for policy changes to support the accessibility of healthcare appointments for people with a learning disability and autistic adults. Additionally, it was suggested that there needs to be a societal shift to ensure a greater understanding of the reasonable adjustments that may be required depending on the individual (Ali et al., 2013a; Wigham et al., 2022a).
Finally, within this level there was a narrative reported within two papers that looked at the additional support required at a policy level for carers of people with a learning disability and autistic adults (Ali et al., 2013a; Kouroupa et al., 2023). Carers felt their ability to support was emotionally draining and the barriers they faced with supporting someone with a learning disability or autistic people to access appointments affected their own health. A change to the way carers are supported would aid the provision of care they could offer to the people they help care for (Ali et al., 2013a).
Discussion
This scoping review identified several barriers and facilitators to the attendance of people with a learning disability and autistic adults at healthcare appointments within the UK. First, there was a significant gap in the training of HCPs regarding the needs of people with a learning disability and autistic adults. Additionally, perceived stereotypes and a lack of specialist knowledge were found to lead to inadequate care and negative attitudes. Following the death of Oliver McGowan in 2016, a significant push for better training standards emerged. This mandatory training aims to address knowledge gaps and improve the quality of care (Department of Health and Social Care, 2019; NHS England, 2023a). Despite these efforts, there remains a substantial need for continuous education and awareness-raising among HCPs to combat stigma and ensure high-quality care (National Development Team for Inclusion, 2022).
These findings also align with a similar study (Sykes, Mcgeechan & Giles, 2024a) on inequalities faced by women with learning disabilities in accessing cervical and breast cancer screening. The study highlights similar barriers such as inadequate training for healthcare providers, the necessity of reasonable adjustments, and the importance of effective communication. Both studies highlight the critical need for continuous education of healthcare professionals and systemic changes to ensure equitable healthcare access.
A closer analysis of both the individual and meta-aggregated findings revealed a layered, complex landscape of factors affecting healthcare access for people with learning disabilities and autism. The synthesis of findings highlighted distinct themes that emerged across various levels, from individual experiences to broader systemic issues. While facilitators like flexible appointment times and dedicated liaison support positively influenced engagement, significant barriers persisted, particularly in areas such as primary care and specialist services. The meta-aggregated data highlighted that barriers and facilitators are deeply interconnected, with accessibility often impacted by both situational variables and underlying systemic limitations.
The findings from our scoping review align with broader policy developments, highlighting the need for specialised training for HCPs, including the use of health passports. Inadequate training and prevailing stereotypes about learning disabilities and autism can lead to stigmatisation and negative attitudes, thereby reducing the quality of care provided to these individuals. Therefore, training on using health passports and making reasonable adjustments, as highlighted in the core capabilities frameworks (Skills for Health, 2019a; Skills for Health, 2019b) is essential. Additionally, others (Northway et al., 2017) emphasise that while health passports can be effective in documenting necessary adjustments, the lack of awareness and utilisation among healthcare staff perpetuates health disparities.
This review found that the structure and environment of healthcare appointments is critical in ensuring equitable access to healthcare services for people with a learning disability. Appointment structures and environments presented significant barriers and facilitators. Inaccessible booking systems and insufficient communication resulted in feelings of disempowerment and inequity among people with a learning disability and autistic adults. Adjustments such as longer appointments, flexible booking times, and the presence of a learning disability liaison nurse were found to significantly enhance the patient experience. These adjustments are well evidenced (50). Effective communication between service users and HCPs was also viewed as pivotal. Adjusted language, the use of Makaton or Picture Exchange Communication (PEC) cards, and the ability to familiarise oneself with clinicians before appointments enhanced the healthcare experience for people with a learning disability and autistic adults.
The ANB code is a novel development, and as such, there are currently very few direct references to it in existing academic literature. This lack of references highlights the innovative nature of the code, however, what can be established from the broader literature is a strong consensus on the necessity for such an initiative. Numerous studies highlight the pressing need for systemic changes to address barriers faced by individuals with learning disabilities and autistic adults in accessing healthcare appointments. These barriers include inadequate healthcare professional training (Hassiotis et al., 2020b; Wigham et al., 2022b), communication difficulties (Parmar et al., 2022b; Sykes, Mcgeechan & Giles, 2024b), and the absence of tailored support mechanisms (Doherty et al., 2020; Malouf et al., 2017b). These barriers have often led to missed appointments and suboptimal health outcomes (Ali et al., 2013b; NHS England, 2024b), thereby justifying the creation and implementation of the ANB code to provide a more supportive healthcare framework. Future research should focus on evaluating the effectiveness of the ANB code in reducing missed appointments and improving healthcare engagement for these populations.
From a policy perspective, the flagging of medical records to highlight necessary reasonable adjustments was found to be essential; this of course links closely to the ANB strategy and code emanating from the North East and North Cumbria region, and links to the findings in this review. Greater societal understanding and acceptance of reasonable adjustments can drive policy changes and improved healthcare accessibility (NHS England, 2024c). Supporting carers and providing them with the necessary resources and information were also seen to be critical components of a holistic approach to healthcare for people with a learning disability and autistic adults. The LeDeR report (King’s College London, 2023) identifies long-term health conditions associated with avoidable deaths among individuals with learning disabilities, further highlighting the importance of early identification and proactive healthcare measures. Implementing a comprehensive and inclusive approach that incorporates training, flexible appointment structures, effective communication, and supportive policies can therefore significantly reduce health disparities and improve outcomes for people with a learning disability and autistic adults.
One of our findings included the need for a better code for medical records. The introduction of the ANB code aims to address this critical issue in healthcare, ensuring people with a learning disability or autistic adults do not miss essential medical appointments (Learning Disability Network, 2024). One year into the ANB code implementation, our review did not find any evidence on its use and implementation. Whilst it is very early for such information to be published, it is imperative that future research is undertaken to evaluate its effectiveness, understand the barriers and facilitators identified and whether reasonable adjustments are being used to address them, and discuss future direction for the ANB code and strategy. Whilst the primary goal of the ANB code is to reduce missed appointments and improve healthcare outcomes for vulnerable populations, this review suggests that the code alone may not suffice to achieve this objective. Comprehensive research that measures not just the reduction in missed appointments but also improvements in health outcomes and patient satisfaction is necessary.
Despite advancements in healthcare services, substantial barriers persist that prevent individuals with learning disabilities and autism from accessing equitable healthcare (Simpson, 2020). Key issues include communication challenges, diagnostic overshadowing, and limited application of necessary adjustments to accommodate neurodivergent individuals. Research has highlighted that these barriers are ingrained within healthcare systems and are exacerbated by inadequate policy adaptations (Doherty et al., 2020). Even though specialised services have increased, a lack of systemic change in policy and practice has led to ongoing disparities in access and quality of care for neurodivergent populations (Malik-Soni et al., 2021).
Changes in government and policy can significantly support healthcare initiatives for vulnerable populations. For example, evolving primary care initiatives and comprehensive frameworks like the WHO’s “Health 2020” (World Health Organization, 2013) emphasise the importance of supportive policy environments to improve health equity. Adequate funding and resources are crucial for reducing health disparities and improving access to care. The Fairer Access Update by the Outpatient Transformation Board (Stamp, 2024) outlines practical steps to address health inequalities and enhance service accessibility. The multiagency Fairer Access Group uses a Health Inequalities Dashboard to provide insights into disparities in outpatient services, highlighting higher no-show rates among the most deprived and non-white populations. Pilot programmes, such as proactive patient engagement in paediatric and maternity clinics, have effectively reduced these rates, demonstrating the value of targeted interventions. Additionally, addressing barriers to antenatal care for minority ethnic mothers highlights the need for culturally appropriate care.
The Reasonable Adjustment Digital Flag, a national NHS record (NHS England, 2024a), identifies and shares the needs of individuals requiring accommodations due to disabilities. This initiative, aligned with findings on preventing ANB scenarios, emphasises the importance of recording and communicating patient needs to ensure appropriate care. Both the Digital Flag and the review call for specialised training for healthcare professionals to overcome knowledge gaps and stereotypes and recommend flexible appointment systems. This unified approach aims to address healthcare disparities and ensure equitable access to medical services for vulnerable populations.
Lastly, Longitudinal studies to evaluate the impact of the ANB code on health outcomes, patient satisfaction, and healthcare utilisation are necessary. These studies should also assess the cost-effectiveness of the code. Involving patients and their carers in the development and refinement of the ANB code can ensure that it addresses their needs more effectively (Saini et al., 2021). Future research should explore the most critical areas that require immediate attention and improvement. The ANB code could potentially be aligned with other health initiatives which have more traction, such as cancer screening and diabetes management programmes, to ensure a holistic approach to healthcare for people with a learning disability and autistic adults. Lessons learned from successful implementations in these areas can provide valuable insights (Tuschick et al., 2024).
Figure 5 outlines recommendations for future practice. Recommendations.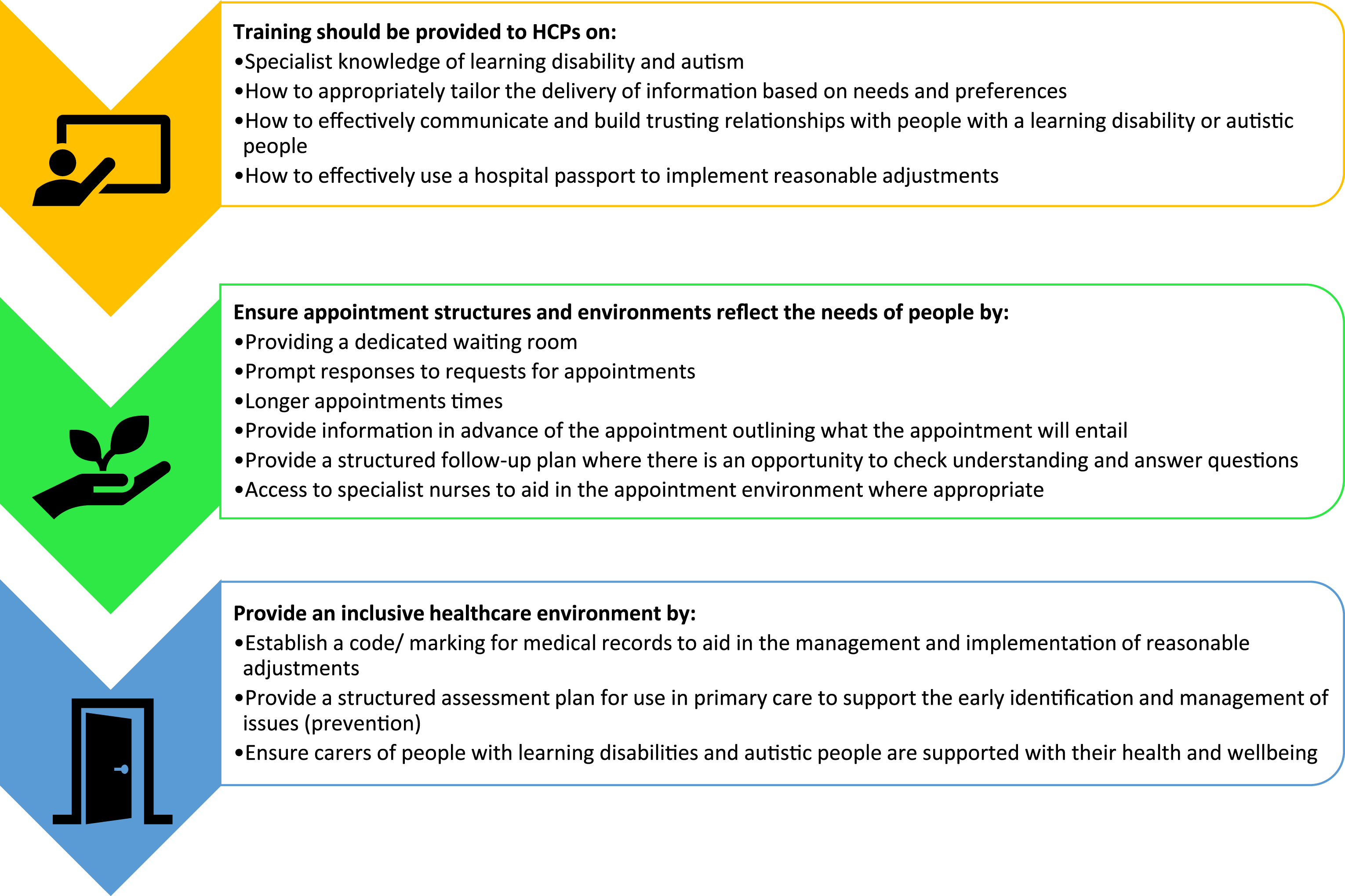
Conclusion
Summary table.
Strengths and limitations of the review
It should also be noted that the recommendations provided are grounded in evidence from research with people with learning disabilities, autistic adults or people from both groups. Therefore, recommendations should be tailored with input from patients if applied within practice.
This scoping review has several strengths. The use of the JBI Scoping Review Network Manual and PRISMA guidelines lends credibility and a structured approach to the review, enhancing the reliability of the findings. The review successfully identifies critical barriers and facilitators at various levels (individual, relational, organisational, and societal/policy), providing a holistic view of the factors affecting healthcare appointment attendance for people with a learning disability and autistic adults. Additionally, it offers clear and actionable recommendations, such as the need for professional training, improved communication strategies, and enhanced support systems, which can directly inform policy and practice.
However, there are notable limitations. Despite the broad initial search, only 15 studies were included, which might limit the generalisability of findings. The review also restricted papers to the UK only, which could lead to a geographical bias and may not accurately reflect trends or outcomes seen in other regions. The reliance on qualitative data, while rich in detail, may be subject to researcher interpretation and bias. Future research therefore could benefit from incorporating more quantitative data and expanding the geographic scope to enhance the generalisability of the findings.
Supplemental Material
Supplemental Material - Barriers and Facilitators to Healthcare Access for Adults With Learning Disabilities and Autistic Adults in England: A Scoping Review and Meta-Aggregation
Supplemental Material for Barriers and Facilitators to Healthcare Access for Adults With Learning Disabilities and Autistic Adults in England: A Scoping Review and Meta-Aggregation by Matthew Cooper, Emma Tuschick, Emma L. Giles, Josh Hodgson, Enya Stubbs, Jill Barker in Journal of Intellectual Disabilities.
Supplemental Material
Supplemental Material - Barriers and Facilitators to Healthcare Access for Adults With Learning Disabilities and Autistic Adults in England: A Scoping Review and Meta-Aggregation
Supplemental Material for Barriers and Facilitators to Healthcare Access for Adults With Learning Disabilities and Autistic Adults in England: A Scoping Review and Meta-Aggregation by Matthew Cooper, Emma Tuschick, Emma L. Giles, Josh Hodgson, Enya Stubbs, Jill Barker in Journal of Intellectual Disabilities.
Supplemental Material
Supplemental Material - Barriers and Facilitators to Healthcare Access for Adults With Learning Disabilities and Autistic Adults in England: A Scoping Review and Meta-Aggregation
Supplemental Material for Barriers and Facilitators to Healthcare Access for Adults With Learning Disabilities and Autistic Adults in England: A Scoping Review and Meta-Aggregation by Matthew Cooper, Emma Tuschick, Emma L. Giles, Josh Hodgson, Enya Stubbs, Jill Barker in Journal of Intellectual Disabilities.
Ethical considerations
Ethical approval was not needed due to this being a scoping review.
Footnotes
Acknowledgements
We would like to thank Kehinde Kanmodi and Eyinade Egbedina who contributed to the setup of this work as part of their Master’s in Public Health.
Author contributions
All authors meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors and all authors agree with the manuscript. The lead author affirms that this manuscript is an honest, accurate, and transparent account of the study reported. The lead author affirms that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been explained. JB conceived of the study, acted as principal investigator, supported with data collection and analysis, resolution of queries, advice on protocol design, and oversight of data synthesis and interpretation. MC and ET were the research associates for the project and were involved in the research data collection and analysis and led on the draft of the final manuscript. ELG, JH, ES were co-applicants for the project, supported with research data analysis and interpretation, and contributed to the final manuscript.
Funding
This study/project did not receive funding.
Declaration of conflicting interests
All authors declare that they have no conflicts of interest.
Data Availability Statement
Data available on request from the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.