
Abstract
Background
In the UK, approximately 1.5 million people have an intellectual disability, and this group of people are at a greater higher risk of mental health problems compared to the general population (Cooper et al., 2007; Shimoyama et al., 2018). Prevalence rates for anxiety in this group range from 8.1% (compared to 3.9% in the general population), to as high as 15–20%, depending on the study (Bond et al., 2020; Cooper et al., 2015; Reid et al., 2011). Syndromic prevalence varies, with 9% of individuals with Down’s syndrome and up to 73% of those with Rett syndrome affected by anxiety (Edwards et al., 2022). Anxiety disorders often worsen over time, exacerbated by negative life events, leading to reduced quality of life and increased psychological trauma (Cooray et al., 2022).
These challenges underscore the need for effective, tailored interventions for anxiety in individuals with intellectual disability. Traditional single-component psychological interventions have shown variable effectiveness in addressing mood disorders in this population, highlighting the need for more comprehensive approaches (Dagnan et al., 2018; Unwin et al., 2016). The multi-faceted nature of anxiety in this group requires interventions that address various contributing factors simultaneously (Moskowitz et al., 2019). However, a limited number of studies have specifically examined interventions targeting anxiety in this population. In the UK, the National Institute for Health and Care Excellence (NICE) recommends the development and evaluation of multi-component approaches to address the complex nature of anxiety in individuals with intellectual disability (National Institute for Health and Care Excellence, 2016).
Multi-component approaches to anxiety management integrate multiple therapeutic strategies that focus on different aspects of anxiety (Pitman and Knauss, 2020). These approaches often include a combination of psychoeducational and therapeutic components to provide a holistic framework for anxiety management (Antony and Stein, 2008). Evidence suggests that simplifying psychological therapies and integrating techniques such as exposure therapy, and relaxation training can be effective for this group (Graser et al., 2022; Moskowitz et al., 2019; Unwin et al., 2016). Although the evidence base is limited, some studies suggest relaxation-based interventions including progressive muscle relaxation or guided imagery may support anxiety reduction in individuals with intellectual disability (Chapman et al., 2013; Griffith et al., 2016).
Mindfulness and acceptance-based strategies have also demonstrated efficacy in increasing individuals’ awareness and acceptance of their anxious thoughts and feelings (Idusohan-Moizer et al., 2015; Patterson et al., 2019). Teaching individuals with intellectual disability coping strategies in accessible and understandable ways empowers people to more effectively manage their symptoms (Robertson, 2011).
Building on this evidence, we co-developed a Multi-Component Anxiety Management Programme (M-CAMP) with individuals who had a lived experience of intellectual disability and anxiety, as well as their families and caregivers. This collaborative approach ensured the programme was tailored to the unique needs and preferences of this population group. The M-CAMP intervention incorporates adapted cognitive-behavioural therapy, exposure therapy, relaxation training, and mindfulness strategies.
Due to the innovative nature of this multi-component approach and its lack of prior testing within this population, a feasibility study was conducted, to determine acceptability of the intervention, rather than a full definitive trial. Feasibility studies are used to evaluate key variables that are uncertain and require estimation before designing a primary study. This study aimed to assess the feasibility of recruitment and retention; practicality, acceptability, adherence, and preliminary effects of the intervention in supporting self-management of anxiety. Additionally, this enabled an exploratory analysis of the intervention’s effectiveness across various outcome measures, allowing identification of the most appropriate primary outcome measure and calculation of the sample size required for a future definitive trial.
Method
This study was registered (ISRCTN:16062949) and approved by the Research Ethics Committee (REC) and Health Research Authority (23/EM/0044) in March 2023.
Study design
A single-blind feasibility trial was conducted using a quasi-experimental design to compare the M-CAMP intervention with treatment as usual (TAU). Four community intellectual disability teams were randomised, with the aim of recruiting 60 participants, 30 in each arm. The sample size was determined to ensure sufficient data for calculating a sample size for a definitive randomised controlled trial (RCT) (Sim and Lewis, 2012).
Randomisation was completed by an independent administrator using a sealed-envelope method (https://www.sealedenvelope.com/). An unblinded member of the research team subsequently informed the community intellectual disability teams of their group allocations.
To maintain the integrity of the single-blind design, Clinical Study Officers, who were separate from the study team and remained blind to group assignments, obtained consent from participants, and conducted all assessment measures. Participants were instructed not to disclose their trial arm during the study.
Recruitment
Recruitment commenced in March 2023 and continued until May 2024 (15 months). Participants were recruited from four National Health Service (NHS) community intellectual disability teams within one NHS Trust in Cheshire and Merseyside. Individuals with intellectual disability were approached about the study by a member of the community intellectual disability team. Those interested in taking part in the study were provided with an accessible participant information sheet giving details of the study and what participation would involve. Everyone interested in taking part in the study, who met the inclusion criteria, was referred to the trial study team to complete eligibility assessment.
Details of participants who met the eligibility criteria were forwarded to the NHS Trust research team clinical studies officers to obtain written consent in accordance with the Mental Capacity Act (Department of Health, 2005) and complete assessment measures.
Inclusion criteria
➢ Aged 18 years or over. ➢ Confirmed diagnosis of mild or moderate intellectual disability. ➢ Scores above 7 or above on the anxiety component of the Moss Psychiatric Assessment Schedules for Adults with Intellectual Disability (Prosser et al., 1998). ➢ Provide informed consent and signed a declaration form indicating agreement to participate.
Exclusion criteria
➢ Declined involvement in the study. ➢ Severe or profound intellectual disability. ➢ Score below 7 on the anxiety component of the Moss Psychiatric Assessment Schedules for Adults with Intellectual Disability (Prosser et al., 1998). ➢ Lack capacity to consent for the study.
Intervention
M-CAMP is a co-produced 10-week intervention that adopts a goal-based therapeutic approach, integrating various psychological models and therapeutic modalities.
The sessions include mindfulness exercises, which help participants focus on the present moment and embrace a more flexible mindset. Cognitive Behavioural Therapy (CBT) techniques are employed to examine patterns and behaviours, while sessions focused on soothing exercises and mindfulness to develop practical coping mechanisms for anxiety. Additionally, the programme includes relaxation techniques, well-being practices, and lifestyle adjustments, providing a robust framework for developing effective anxiety management skills. Practicing these techniques between sessions is encouraged to facilitate skill acquisition and integration into daily life. Graded exposure techniques are introduced to help participants gradually confront and manage anxiety-provoking situations, building confidence and reducing avoidance behaviours. Concurrent psychological therapy sessions further support these exercises, promoting the development of self-management skills and ensuring continuous progress. Accessible patient and clinician workbooks provide structured guidance and resources, allowing for the individual tailoring of the programme to meet people’s person-centred needs.
Therapists and clinical training
Therapists included clinical staff working within intellectual disability community teams’ consisting of psychologists, intellectual disability nurses; occupational therapists; and assistant psychologists. All therapists received a training programme facilitated by a clinical psychologist and a member of the research team with intellectual disability who had lived experience of anxiety. This provided clinicians with practical insights and perspectives on living with anxiety and intellectual disability.
Clinical supervision
Clinical psychologists provided bi-weekly supervision sessions to support the delivery of the intervention. These sessions ensured the programme’s quality and effectiveness by offering expert guidance on applying therapeutic techniques, addressing challenges, and tailoring the intervention to individual needs. This support helped clinicians to maintain best practices and the integrity of the therapeutic approach.
The sessions also allowed clinicians to review progress, reflect on their experiences, discuss successes and challenges, and receive feedback.
Control arm
TAU for anxiety management consisted of standard clinical practices currently employed within NHS services. These practices primarily included providing self-help advice and general information aimed at empowering individuals in their mental health management. Support and informational resources were provided for families and paid carers. Monitoring and follow-up appointments were conducted to evaluate progress and make necessary adjustments to individuals treatment plans.
Feasibility and acceptability outcomes
Feasibility and acceptability were assessed based on the preliminary effects of the intervention, recruitment into the trial and retention rates, in both arms of the study. Therapy attendance and fidelity of treatment was evaluated using a fidelity checklist and satisfaction questionnaire. Qualitative interviews with participants and clinical staff were completed to understand adherence; practicality and quality of delivery of the intervention; challenges and adaptations; and perceptions of effectiveness.
Clinical outcomes
Clinical study officers, blinded to the allocation group, conducted face-to-face screening and assessments at the initial baseline interview, as well as at the end of intervention (12-16 weeks) and follow-up (20-22 weeks).
Primary outcome
Glasgow Anxiety Scale (GAS) was used to measure cognitive, behavioural and somatic symptoms of anxiety (Mindham and Espie, 2003). Higher scores indicate greater levels of anxiety.
Secondary outcomes
Hospital Anxiety and Depression Scale (HADS) was used to assess the relationship between levels of anxiety and depression in people with intellectual disability (Zigmond and Snaith, 1983). Higher scores indicate more symptoms.
World Health Organisation Quality of Life Measure (WHOQOL-8) was used to evaluate changes in quality of life (Skevington, Lotfy and O'Connell, 2004). Higher scores indicate better quality of life.
Client Satisfaction Questionnaire (CSQ-8) was used to measure the acceptability of the intervention and quality of mental health service provision (Attkisson and Zwick, 1982). Higher scores indicate greater satisfaction.
Client Service Receipt Inventory (CSRI) was adapted in collaboration with lived experienced partners to evaluate the cost of health resources in the future RCT. The modified CSRI was piloted in the study and used to capture the baseline clinical characteristics of participants in the feasibility study (Beecham and Knapp, 1992).
Analysis
The feasibility outcomes were the primary focus of the analysis. Descriptive statistics were used to compare baseline clinical characteristics of the M-CAMP intervention and TAU arms. Median values and interquartile ranges (IQRs) were reported for continuous data, reflecting the non-parametric distribution of the data.
The outcome measures, including the Glasgow Anxiety Scale (GAS) total and subtotal scores, Hospital Anxiety and Depression Scale (HADS) scores, and WHOQOL-8 scores, were analysed descriptively at baseline, end of intervention, and 20 week endpoints.
Categorical data were reported as frequencies and percentages for each group, providing comparison of characteristics such as gender, ethnicity, diagnosis, and accommodation types between the TAU and intervention groups. No formal hypothesis testing was conducted, due to this being a feasibility study and not powered to detect between group differences. In addition to outcome measures, the study reported accrual and attrition rates, the percentage of missing data across time points, and session adherence and fidelity data.
Qualitative interviews were audio-recorded, transcribed verbatim, and thematically analysed to examine participants’ perspectives (Braun and Clarke, 2006). Researchers with lived experience actively participated in this analysis, as recommended to enhance research quality in this field (Coons and Watson, 2013). During stage three of the analysis, the generated themes were reviewed with each lived experience researcher, who examined relevant qualitative data from the interviews to refine the theoretical framework.
The research team observed that the richest data emerged from interviews conducted by researchers with lived experience. While these interviews included more informal discussions and follow-up questions, potentially considered as less methodologically rigorous, crucial for fostering the trust and confidence needed for meaningful communication. The involvement of lived experience researchers mitigated communication challenges arising from power imbalances between researcher and informant (Sigstad, 2014). Their participation in the analysis enhanced the clarity in naming and describing themes, leading to a greater understanding and acceptance of these themes, thereby raising their validity as meaningful concepts.
Feasibility outcomes
The main feasibility outcomes for this study followed a stop-go criterion, which was used to guide decision-making throughout the recruitment process. The criteria assessed the success of participant recruitment and inform adjustments needed for optimal outcomes.
Stop-go criteria
(1) Green (Go): If 80-100% of the recruitment target (48-60 participants) is achieved, recruitment will proceed as planned. (2) Amber (Review & Adjust): If 50-79% of the target (30-47 participants) is achieved, recruitment strategies would be adjusted such as targeted outreach, increased feedback mechanisms, additional training, and supervision. (3) Red (Stop or Modify): If fewer than 30 participants are recruited (less than 50% of the target), significant modifications would be made to recruitment strategies.
Results
Recruitment and retention
Recruitment occurred from March 2023 to August 2024. A CONSORT diagram (Figure 1) illustrates the flow of participants through the study and Table 1 summaries the recruitment process with the corresponding stop-go criteria: Flow of study participants. Recruitment progress overview.

Recruitment was conducted from March 2023 to May 2024. A total of 69 participants expressed an interest in participating, with 66 eligible for the study. Six participants were excluded for either not meeting the inclusion criteria or choosing not to participate. The total number of participants recruited was 60 (87%). Among the 60 recruited participants, 56 (95%) completed the midpoint assessments. The four participants who did not complete these assessments were unable to participate due to illness, being on holiday, or being uncontactable.
A total of 56 participants (95%) completed their final assessments. Two participants from each arm of the study did not complete this process. The reasons for their non-completion were family and personal issues (n=1), the unrelated death of one participant (n=1), and two participants chose not to continue their engagement with the study (n=2).
Participant characteristics
Participant baseline demographics.
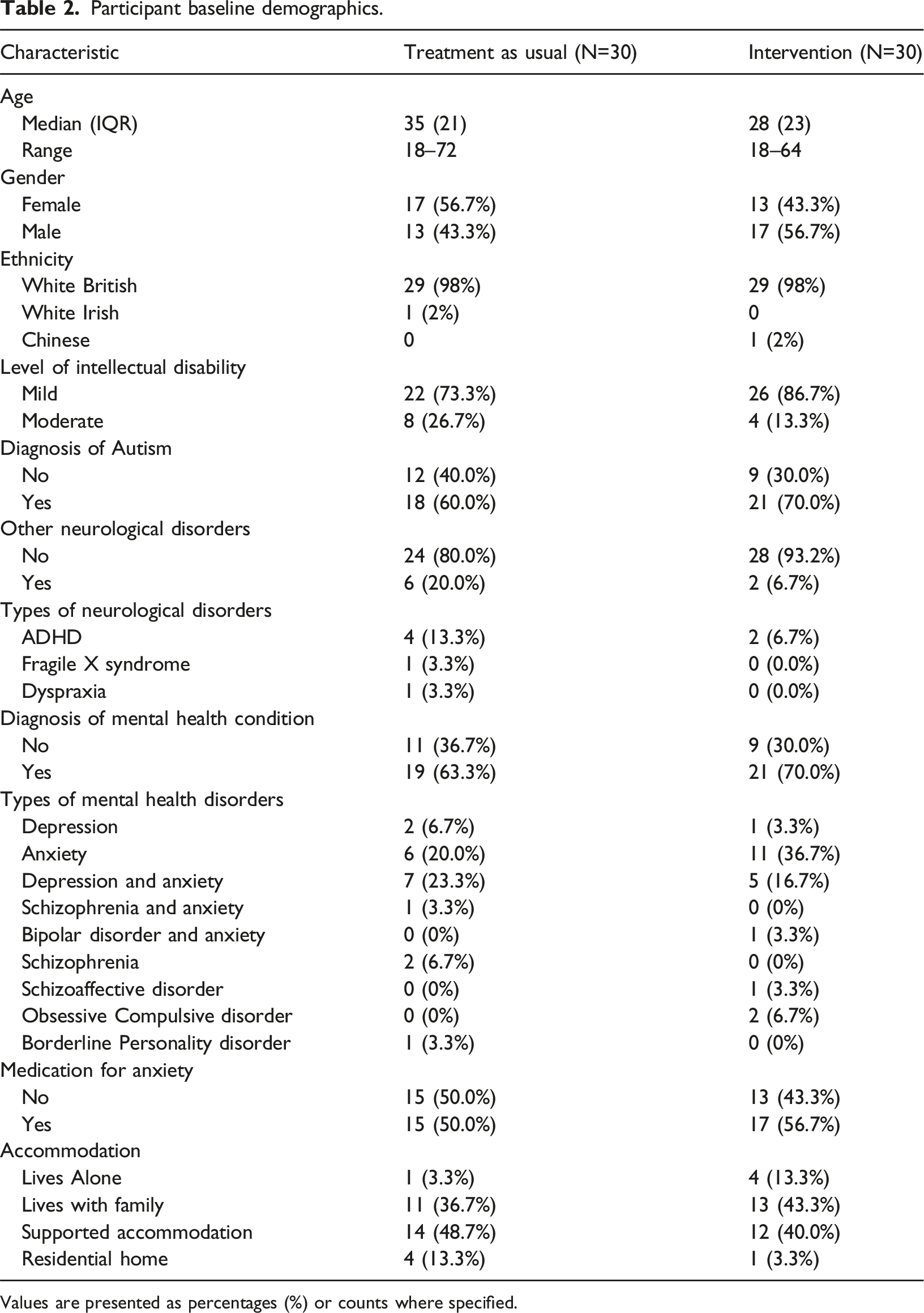
Values are presented as percentages (%) or counts where specified.
Clinical outcomes
Assessment measure scores.

*Glasgow Anxiety Scale [GAS], **Hospital Anxiety and Depression Scale [HADS], ***Adapted World Health Organisation Quality of Life Scale [WHOQOL-8].
The HADS anxiety scores decreased in the M-CAMP intervention group reducing from a median score of 12 at baseline to 9 at endpoint (20 weeks). In comparison, the TAU group median score remained stable at 11 at baseline and at endpoint (20 weeks). HADS depression scores decreased in both groups from 5 to 3 in the intervention group and from 6 to 3 in TAU group. WHOQOL-8 scores slightly improved in the intervention group, increasing from a median of 30 to 32 at endpoint (20 weeks), while remaining consistent in the TAU group.
Figure 2 shows mean scores with confidence intervals across time points. GAS scores in the intervention group demonstrated a reduction in anxiety from baseline to week 20, with a downward trend, while the TAU group also demonstrated a reduction in scores. Similarly, HADS anxiety scores showed reductions in the intervention group and stability in the TAU group. HADS depression scores decreased in both groups, with the TAU group showing a greater reduction. WHOQOL-8 scores, in both groups showed slight improvements in quality of life from baseline to week 20. Mean scores with 95% confidence intervals over time.
Session attendance and adherence
A fidelity checklist was completed to measure sessions attended, adherence and feedback on individual sessions. Adherence was measured by recording the number of sessions each participant attended. Figure 3 shows the number of sessions attended by participants, with 80% attending between 8-11 sessions. Sessions were held either weekly or bi-weekly and a screening checklist of clinical records was completed to provide an overview of participant engagement in the anxiety intervention. This indicated that participants were fully engaged in sessions; clinical staff recorded practice of techniques between sessions, demonstrated active involvement and skill acquisition. Number of sessions attended by participants.
Participant ratings of intervention
Participants expressed varying levels of satisfaction with the intervention as measured by the Client Satisfaction Questionnaire. A small percentage, 3.7%, rated the quality of the intervention as very good and 74.1% rated it as good/fair. When asked if the intervention met their needs, 29.6% said it met most of their needs, 44.4% said it met some of their needs, and 14.8% said it met none of their needs.
When asked if they would recommend the intervention, 66.7% of participants thought they would recommend, and 33.3% reported that they would definitely recommend the intervention. Satisfaction questions showed that 3.7% of participants were indifferent, 59.3% were mostly satisfied, and 37.0% were very satisfied with the programme. Overall feelings about the intervention were positive, with 3.7% being very positive, 22.3% being mostly positive, 37.0% being quite positive and 37.0% being indifferent.
Semi-structured interviews
To further evaluate acceptability and satisfaction, semi-structured interviews were conducted with both participants and the clinical staff involved in delivering the intervention. The interviews with participants were conducted by members of the research team, including individuals with intellectual disability who had lived experience. These research team members received specialised training in interview techniques to effectively gather valuable insights and feedback from participants.
A total of 18 individuals who completed the M-CAMP intervention programme provided feedback through face-to-face interviews. These were audio recorded and transcribed verbatim, while notes were taken for participants who preferred not to be recorded. The research team, including those with experience in intellectual disability and anxiety, conducted the interviews. Participants were asked about their mental health, their experiences of receiving the intervention, their levels of confidence, and their suggestions for programme improvements.
Qualitative interview findings
Three main themes emerged from the feedback of participants on the acceptability of the intervention. These were the learning experience, open dialogue, emotional support, and personal growth. The themes reflected people’s direct views of the intervention.
Learning experience
Participants highlighted factors that supported their learning, with many emphasising the benefit of working at a slower pace. One participant stated, “Because I’ve got Autism and Asperger’s, it takes a bit to process. So, she went slower; when she did it slower, I could understand it better.” (Participant 7). Additional factors included clear explanations, repetition, visual aids, and the integration of individual interests into sessions. Many participants enjoyed the work and valued the strong relationships formed with facilitators. Practical strategies like breathing exercises, mindfulness, and body scan techniques were also frequently praised as an enjoyable and effective part of the learning experience.
Open dialogue and emotional support
Participants valued the opportunity to discuss their feelings openly. As one shared, “I talk to people about how I’m feeling, but I used to bottle it up; but now I don’t seem to let it bother me. Say come on, let’s go and talk; it takes it off my plate.” (Participant 7). However, sensitive topics, such as discussions about death, were noted as too personal for some participants, emphasising the need for care in addressing such issues. Clinicians’ guidance and explanations, alongside family support, played a key role in helping participants feel secure during their anxiety management journey.
Personal growth
Many participants reported improved confidence and coping skills following the programme. One participant reflected, “I felt really good about myself because I felt as though I can do it, and I can manage my anxiety, and I can be in control of it.” (Participant 15). While some participants noted that anxiety levels fluctuated with life events, most felt better equipped to manage their emotions. Several expressed a desire for additional sessions or follow-up support to reinforce their learning and confidence. This highlights the potential benefit of extending the intervention for some participants.
Intervention improvement
Participants provided several recommendations to enhance the intervention. Suggestions included tailoring learning approaches to accommodate diverse processing speeds and individual needs. Participants also recommended updating visual aids to improve clarity and engagement and incorporating structured opportunities for open dialogue, such as regular check-ins or feedback groups. Recognising the role of family members, they suggested involving families in sessions or providing additional resources. Follow-up components, including refresher sessions or ongoing support groups, were proposed to help participants maintain their skills and confidence after completing the programme.
Clinical staff feedback on intervention delivery
To assess the effectiveness of the M-CAMP intervention, three focus groups were conducted, involving 14 clinical staff members who provided detailed feedback. This feedback was instrumental in refining the intervention. Staff suggested making changes to support home activities, including making resources to support skill development and adjustments to the session structure to create a more balanced delivery, ensuring equal session times for each session. They found the clinical guide helpful and well-matched to the accessible version of the intervention and appreciated the creation of a person-centred plan. However, clinical staff recommended updating some of the images used in the accessible workbook to enhance visual clarity and engagement.
Importance of supervision sessions
The supervision sessions were highlighted as particularly valuable for staff, especially in relation to enhancing the delivery of the intervention. These sessions not only provided essential support for the graded exposure component but also fostered an environment for open dialogue about challenges faced during implementation. Regular supervision helped staff refine their skills, share experiences, and receive constructive feedback, leading to improved confidence in delivering the intervention.
Comprehensive training content
A key aspect of training and overall buy-in from staff was the emphasis on the workbooks being named “BRAVE” by the lived experience co-facilitators. This naming resonated deeply with clinical staff, as the co-facilitators expressed that individuals with intellectual disability demonstrate bravery in seeking help to address and manage their anxiety issues more effectively. This connection fostered a sense of purpose and motivation among staff, enhancing their commitment to the intervention’s goals.
The training sessions were noted for their comprehensive nature, covering practical aspects of intervention delivery. However, staff suggested introducing regular refresher training sessions to ensure alignment in delivery and maintain fidelity to the intervention. While feedback on the training content was positive, staff recommended adding more interactive elements to further enhance engagement.
Service user engagement was reported as high, with staff noting that participants responded well to encouragement, which motivated them to practice techniques such as mindfulness and breathing exercises between sessions. This active engagement was viewed as a critical factor in the intervention’s success.
Intervention improvements and refinements
Feedback from clinical staff suggested a number of improvements to the anxiety workbooks and training materials. These improvements will focus on refining the intervention’s delivery, increasing accessibility, and improving its effectiveness. Updates to the workbooks should include clearer images and relatable examples, while the integration of interactive components in clinical training to promote active participation. In addition, adjustments to session structure would improve balance to sessions.
Feedback from participants and clinical staff has been instrumental in refining the intervention, leading to meaningful enhancements in its effectiveness and accessibility. Key updates include incorporating tailored learning strategies to accommodate varying processing speeds, improving the clarity of visual materials, and adding structured opportunities for open dialogue during sessions. Furthermore, added resources have been created to actively engage family members, and follow-up components will be introduced to help participants maintain their skills after completing the intervention. A post intervention follow-up system will be implemented to address any ongoing issues and provide continued support.
Progression criteria
Key progression criteria for the M-CAMP study.

Discussion
The findings of this study provide preliminary evidence supporting the feasibility and potential effectiveness of the M CAMP intervention in helping individuals develop self-management skills and reduce anxiety symptoms. Although, these results are encouraging, they should be interpreted with caution due the small sample size and variation in individual responses.
The primary outcome measure of the study focused on assessing the reduction in anxiety symptoms and the development of self-management skills over the course of the intervention. Results from the quantitative data indicated small improvements with descriptive reductions in anxiety levels as measured across assessment time points. These outcomes support the M-CAMP intervention’s potential effectiveness in reducing anxiety symptoms.
Additionally, the high retention rate demonstrated participant commitment to the programme, which not only indicates the feasibility of its implementation but also strengthens the reliability of the primary outcome findings. The consistency in participant engagement suggests that the intervention was perceived as valuable and achievable, which is crucial for its success in clinical settings.
Feedback from participants, through qualitative interviews, highlighted the feasibility and acceptability of the intervention programme. Many participants reported increased confidence in managing their anxiety. Breathing and mindfulness exercises were particularly effective in fostering self-management skills. This aligns with the quantitative findings, which showed small non-statistically significant improvements in anxiety symptoms over the course of the study. However, participant feedback also suggested areas for improvement, particularly around tailoring the programme to meet individual needs more effectively. There was a consensus that revising the BRAVE manuals would enhance the interventions applicability and impact.
Feedback from clinical staff was also positive, with staff indicating that the intervention was feasible to deliver and integrate into clinical practice. They emphasised the importance of supervision sessions and co-facilitated training sessions are crucial for maintaining a high standard of intervention delivery. Clinical staff noted that the revised “BRAVE” branding of the workbooks fostered motivation and played an integral role in enhancing engagement. However, they also recommended adjustments that could improve the intervention programme, including refining certain aspects of the content and delivery to better align with clinical settings.
A logic model for the intervention has been developed as a principal component of the study’s framework to illustrate how the M-CAMP intervention leads to the desired outcomes. Figure 4 presents the logic model, ( M-CAMP-ID logic model.
Next steps
The next steps for the intervention include seeking funding to conduct a full-scale randomised controlled trial to rigorously evaluate M-CAMP effectiveness and assess its potential for broader integration into clinical practice. In addition, we will refine the training materials and adjust the workbooks based on feedback from participants and clinical staff, ensuring they are adaptable to meet the diverse needs of participants. Additionally. we will increase the flexibility of the intervention, enabling a more tailored approach to better support individuals with intellectual disability.
Strengths and limitations
The study had several strengths. Feedback from participants, families, and clinical staff guided the iterative refinement of the intervention. Additionally, the involvement of researchers with lived experienced researchers enhanced both the trustworthiness and depth of the data collected. This collaborative approach facilitated the further development of the BRAVE intervention that is participant centred and responsive to diverse needs.
Moreover, a robust framework for training clinical staff supported the delivery of the intervention with high fidelity, while enhancing clinical staff confidence in delivering the intervention. The training, alongside ongoing supervision, supported the intervention’s effectiveness in clinical practice. The high level of participant engagement and completion of sessions, further underscores the intervention’s acceptability and its potential capacity to meet participants’ needs. However, tailored delivery approaches such as adjusting pace, and providing a variety of resources for staff to select from are critical for meeting diverse learning needs of individuals with intellectual disability. Additionally, providing family and carer resources could enhance the intervention’s long-term impact.
As with most feasibility studies, the sample size was small and not powered to detect statistically significant differences between groups. While improvements in anxiety symptoms were observed in the intervention group, these effects were modest and not subject to formal statistical testing. As such, these findings should be interpreted with caution. Further research is needed to determine whether these observed changes are replicable and clinically significant.
Footnotes
Acknowledgments
We would like to extend our thanks and gratitude to Tracey and Katie, our lived experience trainers, who became an integral part of the research team and whose contributions were integral to both the delivery of the study and the development of the intervention. In addition, we thank Lesley Gledhill for supporting and ensuring the active engagement of lived experienced trainers and supporting development of accessible information throughout the study. We are also deeply grateful to all the individuals who participated in the study, as their involvement and feedback was essential to its success and will guide further refinements to the intervention. We would like to give a special thanks to the clinical staff from the community intellectual disability teams from Cheshire and Wirral Partnership NHS Trust for their dedication and support throughout the process. Lastly, we would like to acknowledge Annabel Green and Hazel Naylor for their invaluable assistance with recruitment to the study.
Funding
This project is funded by the National Institute for Health and Care Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (Grant Reference Number NIHR204370).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.