
Abstract
Background: Self-injurious behaviour (SIB) is a serious and persistent phenomenon affecting a substantial proportion of autistic individuals. Autistic individuals with severe intellectual disabilities and co-occurring mental health disorders may be at increased risk of engaging in SIB. However, knowledge is limited concerning the relationship between mental health and SIB in this population. Methods: Multimodal, comprehensive mental health assessments of 10 autistic adults with severe intellectual disabilities and severe and persistent SIB were conducted, following current recommendations and including multiple assessment tools. Results: All participants were diagnosed with a mental health disorder. While all participants had displayed SIB for decades (M = 22.80 years), for 8/10 participants, co-occurring mental health disorders had not been previously assessed or diagnosed. Conclusion: Persistent SIB in autistic people with severe intellectual disabilities may be associated with unmet mental health needs. These results highlight the importance of conducting comprehensive mental health assessments in these individuals.
Introduction
Self-injurious behaviour (SIB) is a serious issue affecting a substantial proportion of autistic individuals, with a recent meta-analysis estimating that 42% are affected by SIB (Steenfeldt-Kristensen et al., 2020). In people with intellectual disabilities, prevalence estimates vary from 1.7% to 41% (Cooper et al., 2009), with prevalence in adults estimated at 16.2% (Folch et al., 2018). SIB ranges from devastating and potentially life-threatening behaviours, such as head-banging and eye gouging, to less severe forms, such as hair-pulling and self-scratching (Dimian and Symons, 2022; Folch et al., 2018; Steenfeldt-Kristensen et al., 2020). Several longitudinal studies have found SIB to be a persistent phenomenon. In a sample of autistic individuals recruited in childhood/adolescence, persistent SIB was found in 77.6% after three years (Richards et al., 2016) and in 44% after ten years (Laverty et al., 2020). Similar findings have been made in adults with intellectual disabilities (Cooper et al., 2009; Emerson et al., 2001). Specifically for adults with severe/profound intellectual disabilities, Taylor et al. (2011) found persistent SIB in 84% after nearly 20 years.
SIB is associated with poor quality of life (Bradley et al., 2018; Minshawi et al., 2015; Taylor et al., 2011), more restrictive placements (Minshawi et al., 2015), and a risk of social isolation and exclusion (Bradley et al., 2018). Moreover, SIB may involve a risk of being subjected to mechanical and physical restraint (Jones and Kroese, 2007; Lovell, 2004), as well as increased use of psychopharmacological medication (Folch et al., 2018; Lovell, 2004). In addition to the person affected, SIB can have a negative impact on their family members, professional caregivers and healthcare professionals (Fish, 2000; Folch et al., 2018; Minshawi et al., 2015).
SIB in people with intellectual disabilities appears to be a complex and multifactorial behavioural phenomenon, involving a wide range of aetiologies, risk factors and triggers: genetic, biological, environmental, and psychological (Cooper et al., 2009; Dimian and Symons, 2022; Lovell, 2004; Samways et al., 2024; Soke et al., 2017). The identified risk factors, which are likely to interact (Oliver and Richards, 2010), include co-occurring autism (Bradley et al., 2018; Folch et al., 2018; Richards et al., 2012), mental health problems (Bradley et al., 2018; Folch et al., 2018; Soke et al., 2017; van Den Bogaard et al., 2018), communication skills (van Den Bogaard et al., 2018), overactivity/impulsivity (Cooper et al., 2009; Richards et al., 2012, 2016; Soke et al., 2017), lower levels of ability (Bradley et al., 2018; Cooper et al., 2009; Folch et al., 2018; Jones et al., 2008; Richards et al., 2012), physical health problems or pain (Folch et al., 2018; Jones et al., 2008; Richards et al., 2016; Soke et al., 2017), and visual impairment (Cooper et al., 2009; Jones et al., 2008). Thus, autistic people with severe intellectual disabilities and co-occurring mental health disorders appear to have a particularly high risk of engaging in SIB. However, studies of the relationship between mental health and SIB in autistic people with severe intellectual disabilities are sparse, and the specific mental health problems of autistic people with severe intellectual disabilities and SIB remain relatively unexplored.
Moreover, while the risk of mental health disorder appears to be high among autistic people with intellectual disabilities (Bakken et al., 2010; Lai et al., 2019; Mazza et al., 2020), the prevalence among those with severe intellectual disabilities remains unclear. In addition, mental health assessment in this specific population may be challenging (Helverschou et al., 2011; Kildahl et al., 2024). There is a lack of validated diagnostic assessment tools, and these individuals often have difficulties in self-reporting of mental health symptoms. There are also surface symptom overlaps between autism characteristics and mental health symptoms, making it challenging to distinguish between the two, particularly in people with limited verbal language skills (Appleton et al., 2019; Halvorsen et al., 2025).
Another challenge in mental health assessment involves symptoms of mental health disorder potentially manifesting in atypical or unusual ways in autistic people with intellectual disabilities (Helverschou et al., 2011; Rosen et al., 2018). This includes apparent changes to the frequency, type or intensity of “challenging” behaviour and SIB (Emerson, 2001; Kildahl et al., 2023), particularly in people with more severe levels of intellectual disabilities (Painter et al., 2018). However, Melville et al. (2016) found that “challenging” behaviours were primarily associated with emotional dysregulation, indicating that emotion regulation skills may moderate the relationship between mental health disorder and these behaviours (Kildahl et al., 2023). In line with this, Ferguson et al. (2025) recently highlighted the interplay between internalising symptoms and emotion regulation difficulties in the development and maintenance of SIB in autistic people with moderate, severe, or profound intellectual disabilities. Thus, the relationship between mental health and SIB may be mediated by negative emotional states and moderated by the individual’s ability to regulate these states (Ferguson et al., 2025; Melville et al., 2016).
Current recommendations for mental health assessment involve the use of a combination of conventional assessment tools and assessment tools developed for autistic people or people with intellectual disabilities (Halvorsen et al., 2025), as well as the use of proxy informants and multiple sources of information (Deb et al., 2022; Kildahl et al., 2024). However, the use of proxy informants is not interchangeable with self-reporting regarding subjective states involving discomfort or distress (Havercamp et al., 2022; Kildahl et al., 2024; Santoro et al., 2022), highlighting another challenge in these assessments. Along with potential bias in clinicians (Kildahl et al., 2024), these challenges in assessment contribute to the risk of diagnostic overshadowing (Jopp and Keys, 2001; Reiss et al., 1982), in which symptoms of a mental health disorder are misinterpreted and misattributed to the individual’s autism or intellectual disability. Thus, there is a possibility that co-occurring mental disorders remain undiagnosed in autistic people with severe intellectual disabilities and SIB (Peña-Salazar et al., 2022), and that the persistence of SIB in some of these individuals may be linked to unmet mental health needs.
In sum, autistic people with severe intellectual disabilities are at high risk of engaging in SIB and appear to be at high risk of having a co-occurring mental health disorder. Even though some case studies describe how identifying and taking account of a co-occurring mental health disorder in this population may contribute to a reduction of SIB and other “challenging” behaviours (Kildahl et al., 2021; Kildahl and Jørstad, 2022), current knowledge regarding the relationship between mental health and SIB in this population is limited.
Aims
The current, explorative study aims to describe the comprehensive mental health assessments, conducted in a specialised mental health department, of autistic adults with severe intellectual disabilities who engage in severe and persistent SIB. The research questions are: 1. What are the conclusions from comprehensive mental health assessments in autistic adults with severe intellectual disabilities who engage in severe and persistent SIB? 2. Have these comprehensive assessments identified previously unrecognised mental health needs?
Materials and methods
Design and setting
This study was designed as an explorative study of the mental health status of autistic adults with severe intellectual disabilities engaging in SIB who were referred to a secondary specialised mental health service for children, adolescents and adults with moderate, severe or profound intellectual disabilities. This service is organised in one of Norway’s public hospitals, covering a geographical area in Eastern Norway with a population of around 500.000. The service is part of the hospital’s department of mental health, and referrals are accepted from the other mental health departments, disability/habilitation services, as well as the patients’ GPs. While these specialised mental services are primarily provided as outpatient services, the service also has an inpatient ward with three beds. For further information about services in Norway, see Bakken et al. (2018).
The current study was designed as a retrospective study, using records of clinical data collected during the standardised initial assessments conducted in the service. These assessments are interdisciplinary, comprehensive and multimodal, based on a fixed protocol, and are conducted in the first six weeks after outpatient admission. For each assessment, the team includes a clinical psychologist, a psychiatrist, as well as intellectual disability nurses and special educators. As the service is specialised, these clinicians have relevant training and experience working on mental health assessment in this population.
Because autistic adults with intellectual disabilities constitute a small proportion of the intellectual disability population, and not all patients in this group engage in SIB, it was assumed that the sample would be too small for extensive statistical analyses. We therefore chose to use a combination of the exploration of group-level data and presenting short vignettes for each participant, to increase the transparency and the potential clinical usefulness of the study.
Participants
The inclusion criteria were that the patients were engaging in SIB at referral and had been diagnosed with co-occurring severe intellectual disability and autism spectrum disorder (ASD) according to the ICD-10 (World Health Organization, 1992). In addition, inclusion was limited to patients who had been under assessment at the service between 2021 and 2024. A review of the service’s records showed 13 potentially eligible participants for the study, whose family members/legal guardians were contacted. Of these, 10 consented. Thus, the final sample comprised 10 participants (3 females, 7 males), ages 25-56 (M = 37.10, SD = 9.98), all of whom had been referred for mental health assessment in the context of severe SIB, and all of whom lived in different group homes. On average, the participants had been displaying SIB for more than two decades (M = 22.80, SD = 6.92, range = 11-32 years). All participants had received the initial mental health assessment as outpatient services.
All participants had been diagnosed with autism and severe intellectual disability prior to referral, and these diagnoses were independently reviewed and confirmed by the assessment team. Autism diagnoses were reviewed based on a combination of records from previous assessments, clinical observations/judgement, comprehensive patient histories, and the Social Communication Questionnaire (SCQ; Rutter et al., 2003). SCQ scores ranged from 20-28 (M = 25.64, SD = 3.20), well above the cut-off of >15. The level of intellectual disability was reviewed based on a combination of records from previous assessments, clinical observations/judgement, comprehensive patient histories based on interviews with families and professional caregivers, and using the Vineland Adaptive Behavior Scales, second edition (Vineland-II; Sparrow et al., 2008). Vineland-II scores ranged from 20 to 30 (M = 22.00, SD = 4.00) in the communication skills domain, 20 to 30 (M = 23.82, SD = 4.69) in the daily living skills domain, and 20 to 24 (M = 21.27, SD = 1.35) in the socialisation skills domain, all within the expected range for severe intellectual disabilities.
Materials
All assessments included multiple structured assessment tools with multiple proxy informants. In line with recent recommendations (Halvorsen et al., 2025), the assessment tools developed for autistic people/people with intellectual disabilities were supplemented with conventional diagnostic tools. Also, all assessments included reviews of the participants’ developmental history and records from previous assessments, as well as a general medical examination and a review of their medical and pharmacological status. All assessments included at least three clinical observations by the assessment team, in the participant’s home and other relevant arenas, by at least three different professionals from the team for each participant (clinical psychologist, psychiatrist, and special educator or intellectual disability nurse). The participants’ family members and professional caregivers were involved throughout the assessments. None of the assessments included interviews with the participant, as they all had limited verbal and non-verbal communication skills.
Aberrant behaviour checklist (ABC)
Originally developed to monitor the treatment effects in individuals with intellectual disabilities (Aman and Singh, 2017), the ABC is a well-studied and commonly used checklist for “challenging” behaviour (Aman, 2012; Halvorsen et al., 2025). Its psychometric properties have been found to be satisfactory to excellent across varying levels of intellectual disabilities, including in individuals with severe intellectual disabilities (Aman, 2012; Flynn et al., 2017; Halvorsen et al., 2023), in autistic people (Halvorsen et al., 2025), and in the Norwegian version (Halvorsen et al., 2019; Kildahl et al., 2025). In the current assessments, the ABC was completed by special educators or intellectual disability nurses in interviews with the participants’ family members or professional caregivers.
The ABC comprises 58 items rated on a four-point scale (not a problem = 0, minor problem = 1, moderate problem = 2, severe problem = 3), and item scores are summed into five subscale scores: irritability (15 items), social withdrawal (16 items), stereotypic behaviour (7 items), hyperactivity/noncompliance (16 items), and inappropriate speech (4 items). The ABC is a dimensional measure, and higher scores on the respective subscales reflect more severe difficulties within these domains. In its original factor structure, the three items describing SIB are included in the irritability subscale. However, previous studies in predominantly autistic samples have found these items to emerge as a separate factor (Brinkley et al., 2007; Halvorsen et al., 2019; Kaat et al., 2014; Kildahl et al., 2025). Thus, in addition to including these items in their originally designated subscale, we also used these three items to calculate a score for the proxy-reported severity of SIB for each participant (range 0-9).
Psychopathology in Autism Checklist (PAC)
The PAC (Helverschou et al., 2009; 2021b) is a mental health screening checklist developed for autistic adults with intellectual disabilities. Previous studies have identified its psychometric properties as good to acceptable (Helverschou et al., 2009; 2021b), with one finding indicating that its psychometric properties may be somewhat better in autistic people with severe/profound intellectual disabilities (Helverschou et al., 2021b). The PAC has been found to reliably distinguish between autism characteristics and mental health symptoms, between autistic adults with intellectual disabilities who have co-occurring mental health disorder and those who do not, and to some extent between different mental health disorders in this population (Helverschou et al., 2009; 2021b). In the current assessments, the PAC was completed by a clinical psychologist in the form of an interview with the participants’ family members and professional caregivers.
The PAC comprises 42 items rated in two domains: “Extent of problems” (not a problem = 1, minor problem = 2, moderate problem = 3, severe problem = 4) and “change from usual behaviour” (worsened, unchanged, improved). “Extent of problems” scores are used to calculate scores on the five subscales: psychosis (10 items), depression (7 items), anxiety disorders (6 items), obsessive-compulsive disorder (OCD; 7 items), and general adjustment problems (GAP; 12 items). Cut-off values for screening have been identified (Helverschou et al., 2009).
Diagnostic assessment of the severely handicapped (DASH-II)
The DASH-II (Matson, 1995; Matson et al., 1991) is a checklist for mental health problems in individuals with severe/profound intellectual disabilities. It is one of the very few measures that has been found to be reliable and valid for the assessment of mental health problems in this population (Flynn et al., 2017; Sevin et al., 1995). However, the diagnostic specificity of the DASH-II may be limited, and it may primarily be suited for screening for the need for further assessment (Myrbakk and Von Tetzchner, 2008). In the current study, the participants’ families and professional caregivers completed the DASH-II.
The DASH-II comprises 84 items, all rated in three domains: frequency (0 = “No occurrence”, 1 = “1-10 times in the preceding 2 weeks”, 2 = “More than 10 times in the previous 2 weeks”), severity (0 = “No disruption or damage”, 1 = “No damage, but interrupted activities at least once”, 2 = “Caused injury or property damage at least once”), and duration (0 = “<1 month”, 1 = “1-12 months”, 2 = “>12 months”). For 8/13 subscales (organic syndrome, anxiety disorder, mood disorder, mania, pervasive developmental disorder/autism, schizophrenia, stereotypies), cut-offs are derived from in the original validation sample (Matson et al., 1991). Cut-offs for the remaining five subscales (self-injurious behaviour, eliminating disorders, eating disorders, sleep disorders, sexual disorders) involves at least one item for the respective subscale to be rated at a severity level of 1 or 2.
MINI international neuropsychiatric interview (MINI)
The MINI (Sheehan et al., 1998) is a validated, semi-structured diagnostic interview for the assessment of mental health disorders according to the DSM-IV and the ICD-10. As such, the items of the MINI are designed to elicit information relevant to the formal diagnostic criteria for mental health disorders. While not adapted for autistic people with intellectual disabilities, smaller clinical studies have shown that conventional assessment tools such as the MINI can be used with proxy informants in this population (Dalhaug et al., 2023; Rysstad et al., 2022). In the current study, the MINI was completed by a clinical psychologist in the form of an interview with the participants’ family members or professional caregivers. In addition, available knowledge from other sources, e.g., clinical observations and the patient history, were considered during the scoring of the MINI.
Other conventional assessment tools
When relevant, conventional assessment tools for specific mental health disorders were used in addition to the MINI. These were all completed by a clinical psychologist in the form of interviews with the participants’ family members or professional caregivers.
The Montgomery Åsberg Depression Rating Scale (MADRS; Montgomery and Åsberg, 1979) is a ten-item questionnaire measuring the severity of depressive episodes. Scores range from 0 to 60, with higher scores indicating more severe depressive symptoms.
The Young Mania Rating Scale (YMRS; Young et al., 1978) is a frequently used scale for measuring mania symptoms, comprising 11 items derived from the core mania symptoms. Four items are graded on a scale of 0-8, while the remaining seven items are graded on a scale of 0-4, resulting in a total score of 0-60 with higher scores indicating more severe mania symptoms.
The Yale-Brown Obsessive Compulsive Scale (Y-BOCS; Goodman et al., 1989) is a 10-item checklist for the severity of obsessions and compulsions according to the time spent on these, degree of interference, subjective distress, internal resistance, and degree of control. Scores range from 0-40, with higher scores indicating more severe OCD symptoms.
Diagnostic conclusions
Following comprehensive assessments, the diagnostic conclusions were made in interdisciplinary meetings involving all the department’s relevant professionals: clinical psychologists, psychiatrist, intellectual disability nurses, and a special educator. The formal criteria from the ICD-10 were applied, with support from the Diagnostic Manual-Intellectual Disabilities 2 (Fletcher et al., 2017). The diagnostic conclusions were based on the totality of the information in each case, including scores on assessment tools, patient histories, and clinical observations. In these discussions, reflective practices were used, and particular attention was paid to potential convergence and divergence in the reports and scores on assessment tools. In cases involving divergence, the team sought to explore potential reasons for this divergence using strategies such as those described by Kildahl et al. (2024), rather than seeking immediate agreement. This exploration included available knowledge about the strengths and weaknesses of the assessment tools (Halvorsen et al., 2025) and item-level analyses considering information from the clinical observations and the patient history.
Procedure
The first author collected data from the diagnostic reports from each assessment.
Research ethics
This study was approved by the Data Protection Officer at the Vestre Viken Hospital Trust (#21-05654-1). Written informed consent was obtained from the participants’ next of kin and/or appointed legal guardians according to the legal requirements and the approval of Data Protection Officer. All participants have been anonymised and given a pseudonym.
Results
Demographic and background information, final diagnoses.
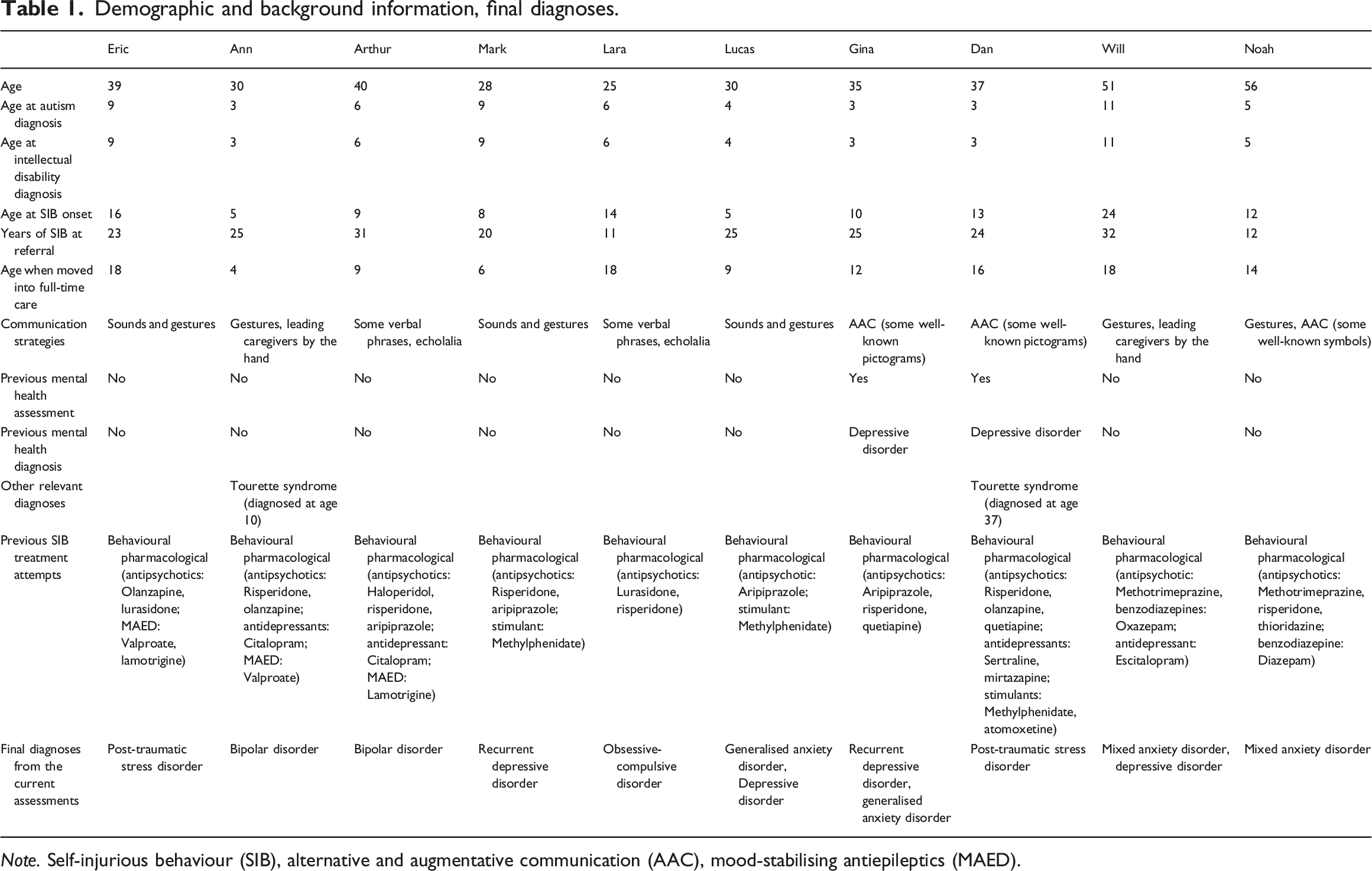
Note. Self-injurious behaviour (SIB), alternative and augmentative communication (AAC), mood-stabilising antiepileptics (MAED).
Checklist scores.
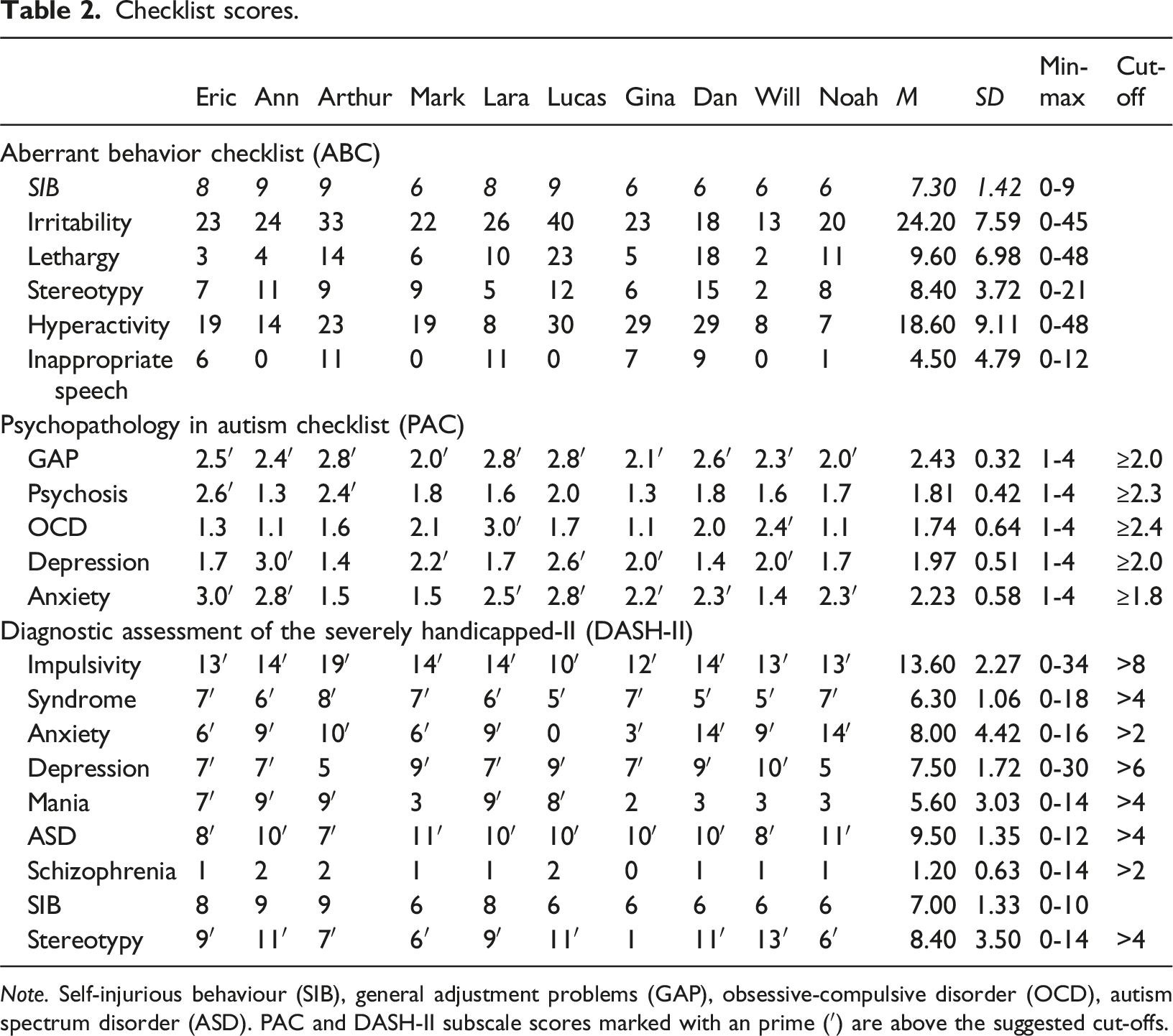
Note. Self-injurious behaviour (SIB), general adjustment problems (GAP), obsessive-compulsive disorder (OCD), autism spectrum disorder (ASD). PAC and DASH-II subscale scores marked with an prime (′) are above the suggested cut-offs.
Clinical vignettes
“Eric” (39)
Eric’s SIB started following a sexual assault when he was 16. At the time, he had been reported as displaying changed behaviour, including anxiety symptoms, being more easily startled, restlessness, sexualised behaviour, as well as hitting his fists on walls and windows. At age 39, Eric was referred for assessment due to his ongoing SIB and other “challenging” behaviours, sleep disturbance, restlessness, and episodes of sudden movements and screaming. At intake, the results from the MINI indicated symptoms of previous and ongoing post-traumatic stress disorder (PTSD) and anxiety disorder. These results were in line with the clinical observations, and the comprehensive patient history. Furthermore, Eric scored well above the cut-offs on PAC anxiety and DASH-II anxiety, in addition to several other scores above the cut-offs on these tools, clearly indicating the presence of a mental health disorder. It was concluded that Eric met the criteria for PTSD, which had likely been triggered by the sexual assault. Because hyperarousal symptoms were observed to occur shortly prior to and during his SIB, and this was reported to be a common trajectory of these symptoms, it was concluded that PTSD symptoms were a likely contributing and triggering factor for Eric’s SIB.
“Ann” (30)
Ann’s SIB started when she was five years old, with frequent wrist biting and hitting her face with her fists. Her SIB had gradually deteriorated over time, and at referral involved severe head banging against walls, floors, trees, and her caregivers’ head or back, as well as hitting her eyes and ears with her fists. At intake, the results from the MINI indicated an ongoing depressive episode and previous episodes of hypomania, which was in line with the clinical observations and the patient history. On the PAC, Ann scored above the cut-offs for anxiety and depression, while she scored above cut-offs on almost all the DASH-II subscales, including anxiety, depression and mania. Further exploration unearthed information about previous episodes typically lasting for 4-5 months, involving more frequent crying, increased SIB, social withdrawal, sleepiness, reduced food intake, and low energy. The symptoms in these episodes resulted in a MADRS score of 32, which in typically developing individuals would indicate a severe depressive episode (Montgomery and Åsberg, 1979). Episodes of potential hypomania involved elevated mood, restlessness, irritability, increased SIB, and significantly reduced amounts of sleep. These symptoms equalled an YMRS score of 21, which in typically developing individuals would indicate moderate mania (Young et al., 1978). Clinical observations and use of the Yale Global Tic Severity Scale (YGTSS; Leckman et al., 1989) confirmed a prior diagnosis of Tourette Syndrome (TS). It was concluded that Ann met the criteria for TS and bipolar disorder, with increased SIB in both depressive and hypomanic episodes. Reports and clinical observations indicated that Ann showed signs of anxiety during both depressive and hypomanic episodes, which were understood as secondary to bipolar disorder.
“Arthur” (40)
Arthur started displaying SIB at age nine, hitting his head with his fists and knees, and banging his head against walls or floors. At intake, the results from the MINI indicated previous depressive and manic episodes, as well as an ongoing manic episode. On the PAC, he scored above the cut-off for psychosis, while DASH-II scores were above the cut-offs for mania and anxiety, as well as on some other subscales. Further exploration of potential mania symptoms using the YMRS resulted in a score of 31, which in typically developing individuals would indicate severe mania (Young et al., 1978). In line with the clinical observations, it was concluded that he met the criteria for bipolar disorder. Converging reports indicated increased SIB in both depressive and manic episodes, suggesting that Arthur’s bipolar disorder contributed to the frequency and severity of his SIB. The divergence between the PAC and the DASH-II in the anxiety scores were understood to be a consequence of the DASH-II to a larger degree including items describing visual signs of restlessness, shaking or crying in its anxiety scale, as also reflected by the ABC hyperactivity score. However, while Arthur had mania symptoms at intake, the patient history indicated that he had more anxiety symptoms in his depressive episodes.
“Mark” (28)
Mark’s SIB started in his early school years, with Mark biting himself and hitting his head and chin with his hands. At age ten, Mark also started displaying aggressive behaviours, including hitting/kicking family members and professional caregivers. At intake, the results from the MINI indicated ongoing and previous depressive episodes. He scored above the cut-offs for depression on both the PAC and the DASH-II, as well as several other subscales on the DASH-II, including anxiety. Further exploration unearthed regular episodes throughout Mark’s life, each lasting for at least 12 weeks, involving increased sleep, reduced energy, reduced food intake, apathy, and increased SIB. These symptoms equalled a MADRS score of 25, which in typically developing individuals would indicate a moderate depressive episode (Montgomery and Åsberg, 1979). This was in line with the clinical observations, and it was concluded that Mark met the criteria for a recurrent depressive disorder. These symptoms were understood to contribute to his SIB, as observations and reports from professional caregivers indicated increased SIB during his depressive episodes.
“Lara” (25)
Lara’s SIB started at age 14, with Lara hitting her head with her fists, biting her arm, and banging her head against walls or floors. At intake, the results from the MINI indicating ongoing OCD and a previous depressive episode. Converging with these results, Lara scored above the cut-offs on PAC anxiety and OCD, as well as on the DASH-II anxiety, depression, and mania subscales. Further exploration of OCD symptoms using the Y-BOCS revealed symptoms of excessive handwashing, cleaning, compulsive emptying of bottles in a specific manner, and an excessive need for symmetry. Clinical observations revealed signs of anxiety prior to, and temporary relief following, these compulsions. If Lara was prevented from performing these actions, it was reported and observed that she would display signs of anxiety, her SIB would be triggered, and she would re-initiate the same compulsions. It was reported that these actions would often prevent her from doing things she found enjoyable. Thus, it was concluded that Lara met the criteria for OCD, and that her OCD symptoms contributed to her SIB.
“Lucas” (30)
Lucas’ SIB started at age five, with onset following a period of (physical) illness. The current referral was due to a period of increased SIB, sleep disturbance, reported apathy, and restlessness. At intake, the results from the MINI indicated an ongoing depressive episode. On the PAC, Lucas scored above the cut-offs on the depression and anxiety subscales, while he scored above the cut-offs for depression and mania on the DASH-II but not for anxiety. Further exploration of these symptoms using the MADRS resulted in a score of 27, which in typically developing individuals would indicate a moderate depressive episode (Montgomery and Åsberg, 1979). In addition, clinical observations and informant reports unearthed symptoms of restlessness, irritability, and occasional panic attacks, which was in line with reports of anxiety on the PAC but not the DASH-II. The reason for this divergence was unclear, but it was hypothesised to be a consequence of the DASH-II being completed by the informants themselves, while the PAC and the MINI were scored in interviews. What was understood as panic attacks may not have been recognised as such prior to the assessment, potentially being misinterpreted as temper tantrums, as the behavioural manifestations of the anxiety symptoms outside of the panic attacks appeared to be quite subtle. After being presented with anxiety as a hypothesis, however, Lucas’ caregivers were able to recognise anxiety symptoms and agreed on their presence. It was concluded that Lucas met the criteria for generalised anxiety disorder and a moderate depressive episode. Lucas displayed observable anxiety symptoms prior to and during his SIB. In addition, a clear increase in his SIB was reported following onset of the depressive symptoms. Thus, the depressive symptoms were understood as contributing to the severity and frequency of his SIB, while his anxiety symptoms appeared to serve as a trigger.
“Gina” (35)
Gina’s SIB started at age 10, with frequent head banging, hair pulling, and throwing her entire body against the floor or items of furniture. At intake, the results from the MINI indicated a previous depressive episode, as well as ongoing depressive and anxiety disorders. Converging with this, Gina scored above the cut-offs for anxiety and depression on both the PAC and the DASH-II. Further exploration unearthed information about regular periods typically lasting 8-9 weeks involving increased frequency of crying, social withdrawal, increased sleep, lower food intake, lower energy, and increased frequency of SIB. On the MADRS, these symptoms resulted in a score of 21, which in typically developing individuals would indicate a moderate depressive disorder (Montgomery and Åsberg, 1979). Reported anxiety symptoms included panic-like states, restlessness, excessive sweating, worry and clinging, and the frequency of her anxiety symptoms appeared to increase during depressive episodes. It was concluded that Gina met the criteria for a recurrent depressive disorder and generalised anxiety disorder. SIB was reported to increase in frequency and intensity during her depressive episodes, while increasing levels of anxiety appeared to trigger episodes of SIB. Thus, Gina’s anxiety and depression were both understood to contribute to her SIB.
“Dan” (37)
Dan was the victim of sexual assault at age ten. His SIB started at age 13, and he had been admitted to inpatient mental health wards twice in his twenties due to restlessness, low energy, reduced appetite, hyperventilation, sleep difficulties, SIB, and possible verbal and motor tics. In his thirties, a new behavioural intervention (overcorrection; Foxx and Azrin, 1973) was introduced by his professional caregivers to manage his SIB, compulsive behaviour, and verbal/motor tics. During this time, Dan’s difficulties escalated, including an increase in his SIB, and he refused to stay in his residential care home. At intake, the results from the MINI indicated a previous depressive episode, as well as ongoing PTSD and anxiety disorder. On the PAC and the DASH-II, Dan scored above the cut-offs for anxiety and depression, converging with the MINI results. Further exploration unearthed episodes of anxiety/hyperarousal symptoms, including hypervigilance and increased startle response, as well as sleep difficulties and extensive irritability. In addition, reports indicated the presence of verbal and motor tics from Dan’s early childhood, which converged with the results from the YGTSS (Leckman et al., 1989). It was concluded that Dan met the criteria for TS and PTSD. PTSD was understood to be a consequence of the sexual assault, as well as the unhelpful behavioural intervention. It was observed that different episodes of SIB appeared to have qualitatively distinct patterns, with SIB associated with apparent PTSD symptoms having a different frequency and intensity than TS-related SIB. It was therefore concluded that both TS and PTSD likely contributed to Dan’s SIB.
“Will” (51)
Will’s SIB started at age 24, with Will hitting his head with his fists or banging his head against the floor or the bodies of his professional caregivers. Prior to the current referral, Will was reported to show increased SIB, sleep difficulties and extensive irritability. At intake, the results from the MINI unearthed symptoms of previous and ongoing depressive and anxiety disorders, converging with scores on the DASH-II where he scored above the cut-offs for anxiety and depression. On the PAC, Will scored above the cut-offs for depression and OCD but not anxiety. Reported anxiety symptoms included specific phobias, compulsive behaviours, and occasional panic attacks. The divergence between the PAC and DASH-II were understood to be a consequence of the differences in the specific items making up the two anxiety subscales, with Will’s specific configuration of anxiety symptoms resulting in an elevated score on the PAC OCD rather than the PAC anxiety subscale. Further exploration using the MADRS resulted in a score of 23, which in typically developing individuals would indicate a moderate depressive episode (Montgomery and Åsberg, 1979). It was concluded that Will met the criteria for a mixed anxiety disorder and a depressive disorder. Anxiety was observed and reported to occur shortly before and during episodes of SIB, and the frequency of SIB was reported to increase during depressive episodes, leading to the conclusion that both anxiety and depression likely contributed to Will’s SIB.
“Noah” (56)
Noah’s SIB started at age 12, with Noah frequently hitting his face with his fists and biting his arms and hands. A few years prior to the current assessment, Noah’s professional caregivers had increased their focus on communication, reduced their expectations of Noah’s skills in accordance with his level of functioning, and worked to increase his ability to influence his everyday life. This had somewhat decreased the frequency of his SIB. However, at the time of the referral Noah still had episodes where he hit his head with his fists approximately 20-30 times a day. At intake, the results from the MINI indicated symptoms of ongoing generalised anxiety disorder, panic disorder, and social phobia, as well as a previous depressive episode. These results converged with the PAC and DASH-II scores, with Noah scoring over the respective cut-offs for anxiety on both tools. Further exploration unearthed episodes of hyperventilation, clearly dilated pupils, screaming, clinging to staff, SIB, and aggressive behaviour. These occurred when Noah heard about or was about to encounter doctors, white coats, dentists, tunnels, snow/ice on the ground, or the possibility of falling over. His anxiety symptoms were reported to increase when someone made demands on him, changes in routines, new activities, and new people. It was concluded that Noah met the criteria for a mixed anxiety disorder. Because these symptoms were described and observed to occur shortly prior to and during his SIB, anxiety appeared to be a contributing factor in, and a potential trigger to, Noah’s SIB.
Overall results
Despite displaying SIB for a mean of 22.80 years, only 2/10 participants had previously received a mental health assessment, and these were the only ones who had previously been diagnosed with a mental health disorder. During the current assessments, all the participants were assessed to meet the criteria for one or more mental health disorder. Moreover, even though some participants had prior mental health diagnoses, these assessments unearthed unmet mental health needs for all the participants resulting in new, additional or changed mental health diagnoses.
Co-occurring mental health disorders appeared to contribute to SIB by either increasing its frequency, intensity and/or severity, or by serving as triggers for SIB. The latter appeared more typical of anxiety and PTSD symptoms, while the former appeared to be primarily linked to mental health disorders involving phases (e.g., recurrent depressive disorder, bipolar disorder). While the mental health diagnoses varied considerably in the sample, anxiety or PTSD symptoms appeared to be present in all the participants, either as a primary disorder or as secondary to another disorder. Two participants met the criteria for Tourette Syndrome, which in both cases appeared to be associated with SIB.
While the PAC and the DASH-II have limitations regarding detection of specific mental health disorders (Helverschou et al., 2021b; Myrbakk and Von Tetzchner, 2008), scores on these assessment tools frequently converged with each other and the results from the MINI. All participants were screen positive for a possible mental health disorder on both the PAC and the DASH-II. In addition, anxiety scores were above the respective cut-offs both on the PAC and the DASH-II for 6/10 participants, while the remaining four participants had anxiety scores above the cut-off on one of these tools. Thus, while the MINI appeared to identify all primary diagnoses in the current cases, the combination of the MINI, PAC and DASH-II was helpful to achieve a more in-depth and nuanced understanding of the individual’s symptoms, particularly with regard to recognition of secondary anxiety symptoms.
Despite 8/10 participants not being previously diagnosed with a mental health disorder, all of them had undergone several treatment attempts involving psychopharmacological and behavioural interventions. For at least one of the participants (“Dan”), the use of a particular behavioural intervention appeared to have resulted in an increase in his SIB and deterioration of his mental health difficulties.
ABC SIB and PAC scores at intake and follow-up, with the reliable change index.
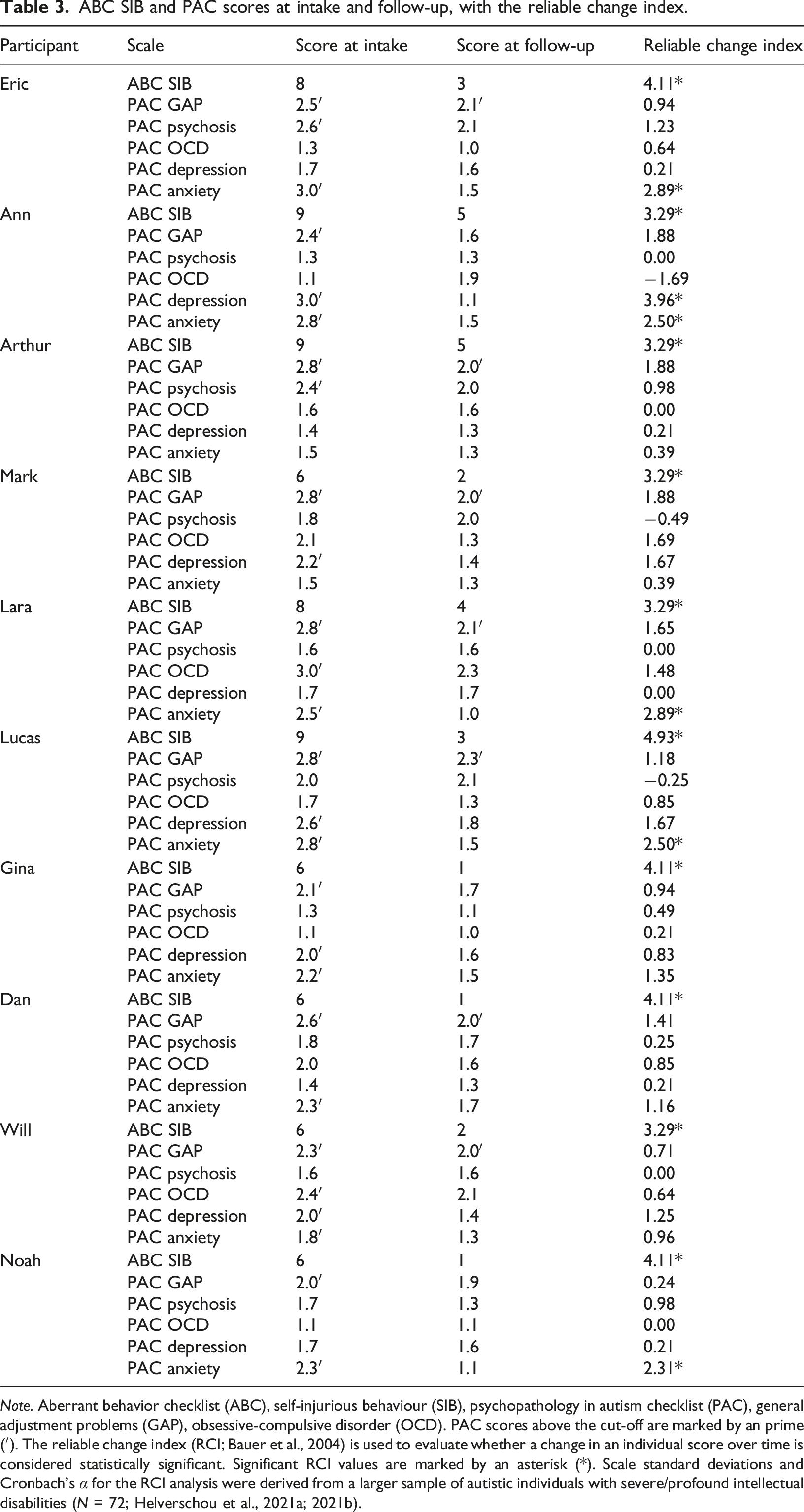
Note. Aberrant behavior checklist (ABC), self-injurious behaviour (SIB), psychopathology in autism checklist (PAC), general adjustment problems (GAP), obsessive-compulsive disorder (OCD). PAC scores above the cut-off are marked by an prime (′). The reliable change index (RCI; Bauer et al., 2004) is used to evaluate whether a change in an individual score over time is considered statistically significant. Significant RCI values are marked by an asterisk (*). Scale standard deviations and Cronbach’s α for the RCI analysis were derived from a larger sample of autistic individuals with severe/profound intellectual disabilities (N = 72; Helverschou et al., 2021a; 2021b).
While SIB remained a problem for some participants, clinical observations indicated that their SIB had changed in nature to a less severe form (e.g., from head banging to self-scratching) or was reduced in frequency and/or intensity. For all participants, these changes resulted in less injuries and reduced use of physical restraint.
Discussion
In this explorative study describing the mental health assessments of ten autistic adults with severe intellectual disabilities and severe and persistent SIB, all participants were diagnosed with a co-occurring mental health disorder. All assessments unearthed previously unrecognised mental health needs, despite participants having displayed SIB for 11-32 years and having undergone several treatment attempts. These findings highlight the potentially harmful consequences of autistic people with severe intellectual disabilities being an underserved group in mental health services. Moreover, the current results suggest that untreated mental health disorders may trigger or influence the frequency and severity of SIB, highlighting the importance of intervention being based on a comprehensive understanding of the underlying causes and triggers for SIB in each specific individual, and the potential importance of including mental health in this understanding.
In all the current participants, clinical observations and informant reports indicated that mental health symptoms were associated with exacerbating and/or serving as triggers for SIB. However, the specific mental health disorders identified differed across participants, showing that SIB may be associated with different types of mental health problems in this population. These findings are in line with the recent model suggested by Ferguson et al. (2025), who emphasised the interplay between emotion regulation difficulties and internalising symptoms, more broadly. Symptoms of an affective disorder were reported to be present in 9/10 of the current participants, while anxiety or PTSD symptoms were present in all the participants. In the interplay between these symptoms and the participants’ SIB, anxiety or PTSD symptoms appeared to primarily serve as direct triggers while depressive symptoms appeared to increase the frequency, severity, and/or intensity of SIB over time. These observations suggest that symptoms of different mental health disorders may affect SIB in different ways, highlighting the importance of identifying the specific mental health disorders also in this population, including differentiating between different internalising disorders, such as anxiety and depression.
Even though anxiety symptoms were observed in all participants, some of them had low scores for anxiety on the DASH-II, while scoring above the cut-off for anxiety on the PAC, or vice versa. Previous findings concerning the PAC (Helverschou et al., 2021b) have reported that it may lack the sensitivity to capture all instances of anxiety in autistic individuals with intellectual disabilities, and the same appears to apply when it comes to the DASH-II. This may be a consequence of both instruments relying on proxy reports of internal states, which has been found to involve a potential risk of underestimating stress and anxiety (Scott and Havercamp, 2018). Other authors have highlighted that clinical observation is an important supplement to the use of checklists in this population (Appleton et al., 2019; Helverschou et al., 2011; Kildahl et al., 2021, 2024; Valdovinos et al., 2019), and the experiences from the current assessments suggest that clinical observation may be particularly helpful when scores on different checklists diverge. As different assessment methodologies unearth information about different aspects of the person’s mental health, convergence between two or more assessment tools/strategies cannot be considered as mutual confirmation (Kildahl et al., 2024). However, such convergence can be interpreted as an indication of the validity of the results from the individual converging tools/strategies. Thus, these findings highlight previous recommendations that the anxiety scores on the PAC and DASH-II should be interpreted with caution and should be interpreted in light of clinical observations and information from other sources (Helverschou et al., 2021b; Kildahl et al., 2024). Moreover, these findings demonstrate how a low score for anxiety on either the PAC or the DASH-II cannot be used to rule out the presence of anxiety.
The assessments identified previously unrecognised mental health needs for all ten participants. Living with an unrecognised mental health disorder is challenging, and it is likely to be even more challenging when the individual has difficulties conveying their difficulties to their families and professional caregivers. In the case of PTSD, for example, Kildahl and Helverschou (2024) describe how the core symptoms of irritability/altered arousal and avoidance may easily be misinterpreted as “challenging” behaviours if the person’s caregivers do not understand these symptoms as relating to trauma and PTSD. These symptoms may then be managed in a way that exacerbates the individual’s difficulties, as the example of “Dan” from the current study shows. For “Dan”, a behavioural intervention was implemented without any investigation of potential influence from mental health difficulties on his SIB, resulting in deterioration of his SIB. In addition, his reaction to this intervention included increased anxiety/hyperarousal symptoms, more sleep difficulties, and increased irritability, as well as “Dan” refusing to stay in his residential care home (avoidance). Together, the story of “Dan” demonstrates how SIB intervention that does not take account of the person’s mental health difficulties may result in potential trauma reactions and PTSD.
In addition to the diagnosed mental health disorders, previously unrecognised anxiety symptoms were identified in all the participants, and reductions in SIB appeared to co-occur with reductions in proxy-reported anxiety symptoms for most of the participants. Oliver et al. (2017) previously highlighted anxiety as a potential target for intervention in SIB in this population, and the current results further demonstrate the need for larger-scale intervention studies to explore this potential association. In addition, there is a need for further studies involving larger samples to determine the prevalence of potentially unmet mental health needs in autistic individuals with severe intellectual disabilities and SIB. Finally, there is a need for further studies investigating the differing relationships between SIB and anxiety/depressive symptoms found in the current participants, as well as longer-term follow-up studies reporting the progress of autistic individuals with severe intellectual disabilities and severe and persistent SIB.
Clinical implications
Persistent SIB in autistic people with intellectual disabilities may be associated with unmet mental health needs. The results of the current study highlight the importance of conducting comprehensive mental health assessments in these individuals. Moreover, the current findings suggest that while this may be resource demanding, using a standardised, multimodal and inter-disciplinary assessment strategy and protocol may help to unearth and identify specific mental health needs during the first six weeks of intake. The use of multiple assessment tools is likely to be helpful, and clinicians working with this population should be careful to avoid ruling out anxiety based on a single assessment tool. Clinical observations appear to be a helpful supplement to the use of checklists, as well as information from other sources and conventional assessment tools.
Limitations
The current study was designed as a retrospective and explorative study with a small clinical sample with a wide age range obtained in a specific secondary specialised mental health service for individuals with intellectual disabilities. The current participants were specifically referred for mental health assessment after showing SIB for years, indicating that they are unlikely to be representative of autistic adults with severe intellectual disabilities and SIB in general. However, these findings may be transferrable, in that they are likely to be relevant to other cases involving persistent SIB in autistic adults with intellectual disabilities, where potential underlying mental health difficulties contributing to the maintenance of SIB have not been comprehensively assessed. Moreover, the current methodology, in-depth case-by-case exploration of individual assessments, unearthed some potential relationships between specific mental health issues and aspects of SIB that can be built upon by future studies.
The participants’ limited verbal communication skills limited the possibility of self-reporting, and the assessments all relied on external sources such as medical records, direct observations by expert mental health practitioners, and proxy ratings by family members and professional caregivers. Such proxy ratings may be influenced by the informants’ existing knowledge, expectations and personal understanding of the patient’s behaviour, as well as their relationship with and knowledge of the individual in question, and the specific contexts in which they have observed them (Kildahl et al., 2024; Kildahl and Jørstad, 2022). In other words, even multiple proxy ratings and triangulation with other sources of information are not interchangeable with self-reporting (Havercamp et al., 2022; Kildahl et al., 2024). In addition, the same team administered, interpreted and integrated the data sources, as well as delivered the intervention, which involves a potential risk of confirmation bias among the mental health professionals conducting the assessments. Despite these limitations, the current assessment strategies unearthed previously unrecognised mental health needs in all the participants, and inter-disciplinary and reflexive practices were used to limit the potential influence from clinician and informant bias in each assessment (see Kildahl et al., 2024). In addition, the third author was not part of the assessment team, and only participated in the critical re-examination, re-interpretation and overall analysis of the data for the purpose of the current study.
Conclusions
The relationship between SIB and mental health disorder appears to be complex and multifaceted, and unmet mental health needs may be a contributing factor in the emergence and persistence of SIB in autistic adults with severe intellectual disabilities. These findings highlight the importance of conducting comprehensive mental health assessments in cases involving autism, severe intellectual disability and persistent SIB, as well as recognising and mitigating anxiety symptoms and treating any other co-occurring mental health disorder in this population.
Footnotes
Acknowledgements
The authors thank the participants, their families and their professional caregivers for contributing to the study, as well as Sissel Berge Helverschou and Jane Margrete Askeland Hellerud for their helpful comments to an earlier draft of this manuscript.
Ethical considerations
This study was approved by the Data Protection Officer at the Vestre Viken Hospital Trust (#21-05654-1).
Consent to participate
Written informed consent was obtained from the participants’ next of kin and/or appointed legal guardians according to the legal requirements and the approval of the Data Protection Officer.
Consent for publication
Written informed consent for publication was obtained from the participants’ next of kin and/or appointed legal guardians.
Author contributions
ALR: Conceptualisation (lead), Data curation, Formal analysis, Investigation, Methodology, Project Administration, Resources, Writing – Original Draft Preparation, Writing – Review and editing. JS: Investigation, Validation, Writing – Review and editing. ANK: Conceptualisation (supporting), Methodology, Supervision, Writing – Review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare that they have no potential competing or conflicting interest.
Data Availability Statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data is not available.