
Abstract
This study used qualitative surveys and focus groups to evaluate the implementation of an end-of-life care planning toolkit within intellectual disability social care services, by exploring whether it is beneficial and workable in this setting. Participants were staff trialling the toolkit and submitting feedback forms. Focus groups with support staff and service managers were also conducted. Feedback forms and focus group transcripts were coded using a modified framework approach. Data and analyses were discussed within the team (including researchers with intellectual disabilities). Thirty-four participants submitted 44 feedback forms. Two focus groups with seven participants were held. Participants found the toolkit approach and resources acceptable and appropriate, prompting positive eye-opening conversations. There were significant adoption and feasibility implementation challenges such as printing the resources, lack of time, and the sensitive end-of-life topic. Exploration of how to overcome these challenges is needed to successfully implement the toolkit in social care services.
Background
People with intellectual disabilities experience marked health inequities and are less likely to access skilled end-of-life support, including specialist palliative care (Tuffrey-Wijne et al., 2015). Intellectual disability service providers are at the forefront of end-of-life care support for people with intellectual disability in residential care or supported living (Todd et al., 2021). However, most deaths of adults within social care settings are unanticipated by staff (Bernal et al., 2014). This is despite reviews and inquiries recommending that social care services engage in end-of-life care planning, involving people with intellectual disabilities and families (Heslop et al., 2013; National Institute for Health and Care Excellence, 2018).
Communication difficulties, issues with capacity, and a death avoidance culture often prevent end-of-life care planning (Adam et al., 2020; Tuffrey-Wijne and McEnhill, 2013; Tuffrey-Wijne and Rose, 2017). There is also a lack of guidance on how to involve people with intellectual disabilities in the planning process (Noorlandt et al., 2020). The evidence shows that support staff lack skills, knowledge, and confidence in end-of-life issues and planning (Adam et al., 2020; Bruun et al., 2024a; Tuffrey-Wijne et al., 2020a).
Four fundamental principles have been identified as central to the success of end-of-life care planning with people with intellectual disabilities: individualising the approach so that it meets the specific preferences and needs of each person; easing concerns; working in partnership with the person about their plan; planning holistically; and, identifying the person’s own choices and/or will and preference (McKenzie et al., 2024). The approach may involve specific resources that can support staff in having end-of-life care discussions adhering to these principles. Several end-of-life care planning resources for people with intellectual disabilities have been identified (Tilley et al., 2024), where some have been found to be helpful in terms of structuring the conversation, approaching topics, and encourage and prompt rich and detailed discussion (McKenzie et al., 2017).
To address these barriers that social care staff are facing, a toolkit of resources and approaches for end-of-life care planning with people with intellectual disabilities was developed together with people with intellectual disabilities, families, support staff, and healthcare professionals (Tuffrey-Wijne et al., 2025). Following a thorough co-design process, it is necessary to explore how feasible the use of the toolkit is in practice.
Study aim
To evaluate the implementation of an end-of-life care planning toolkit within intellectual disability social care services, by exploring whether it is beneficial and workable in this setting.
The study was part of a project co-developing an end-of-life care planning toolkit with people with intellectual disabilities (see Tuffrey-Wijne et al., 2025).
Methods
Study design
To address the study aims, the framework by Proctor and colleagues were followed (Proctor et al., 2011). This framework includes eight conceptually distinct implementation outcomes: acceptability, adoption, appropriateness, feasibility, fidelity, implementation cost, penetration, and sustainability. For each implementation outcome, the authors list different available measures as well as the level of analysis and salience by implementation stage in their taxonomy of implementation outcomes. The current study explores some of the early-stage implementation outcomes in relation to the newly developed end-of-life care planning toolkit: Acceptability, adoption, appropriateness, feasibility, and fidelity. The taxonomy includes the following existing measures to assess these five outcomes: Surveys, interviews, administrative data, refused/blank, observations, focus groups, checklists, and self-reports.
In this study, we conducted surveys (a core evaluation survey completed by intellectual disability support staff trained to use the toolkit and a wider feedback survey completed by a wider group of people involved in end-of-life care planning) and focus groups to assess the five implementation outcomes. Surveys and focus groups included participants reporting their experience of using the toolkit, including details about what they did during their sessions (covering acceptability, appropriateness, and fidelity implementation outcomes). Participants were asked if they had used the toolkit within the study period; including reasons why if that was not the case (covering adoption and feasibility). Administrative data, including participant refusal/blank survey responses, were also collected and analysed (covering acceptability, adoption, and feasibility).
The Consolidated Criteria for Reporting Qualitative Research reporting guideline was followed (Tong et al., 2007).
Research team
The research team comprised a Professor [IT-W] with 20+ years’ experience in end-of-life research involving people with intellectual disabilities; three Research Associates [AB, RA-K, and SG] with experience in co-producing qualitative research including within palliative care; four Research Assistants with intellectual disabilities [AC, DJ, LJ, and RK-B] (Anderson et al., 2023) with some research training (Tuffrey-Wijne et al., 2020b) and end-of-life research experience; and a Research Assistant [JG], with end-of-life experience, supporting them.
Collaborators were intellectual disability service providers MacIntyre and Dimensions with project leads employed to help with the study [FG and MW], both with research and adult social care experience. Project leads were supported by [NP and SS] who were part of conceptualising the overall project.
The study was supported by a Research Advisory Group involving a range of stakeholders.
Setting
The toolkit was developed for support staff working with adults with intellectual disabilities within social care in England. It was further assessed by a wider range of people involved in end-of-life care planning.
Participants and sample
Two groups were involved in the study: ‘facilitators’ and ‘planners’. ‘Facilitators’ were the study participants; they were staff testing the toolkit with people they support. This includes participants involved in the ‘core evaluation’ and those in the ‘wider feedback survey’. Each facilitator formed dyads with one or more ‘planners’. ‘Planners’ refer to all other people involved in end-of-life care planning such as the person with intellectual disabilities themselves and/or other people who know the person well.
‘Facilitators’ were the main study participants, providing the majority of research data (i.e., toolkit feedback). End-of-life care planning is a process which should happen within intellectual disability organisations as standard or usual care as it is a service requirement from the Care Quality Commission (England’s independent health and social care regulator and inspector) to have such plans in place (Care Quality Commission, 2016). ‘Planners’ therefore engaged in end-of-life care planning with facilitators using the toolkit without the requirement to be recruited as research participants themselves.
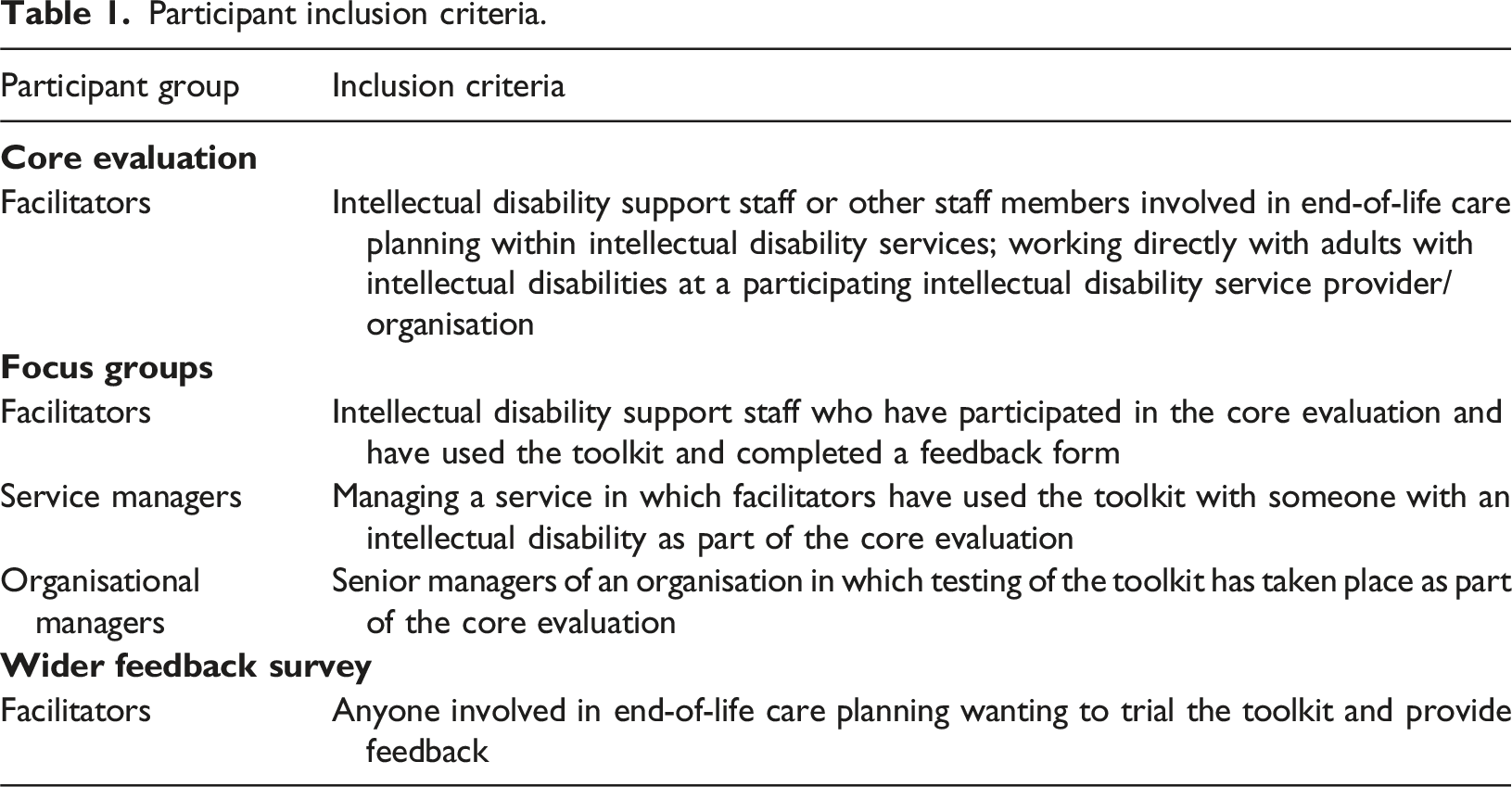
Participant inclusion criteria.
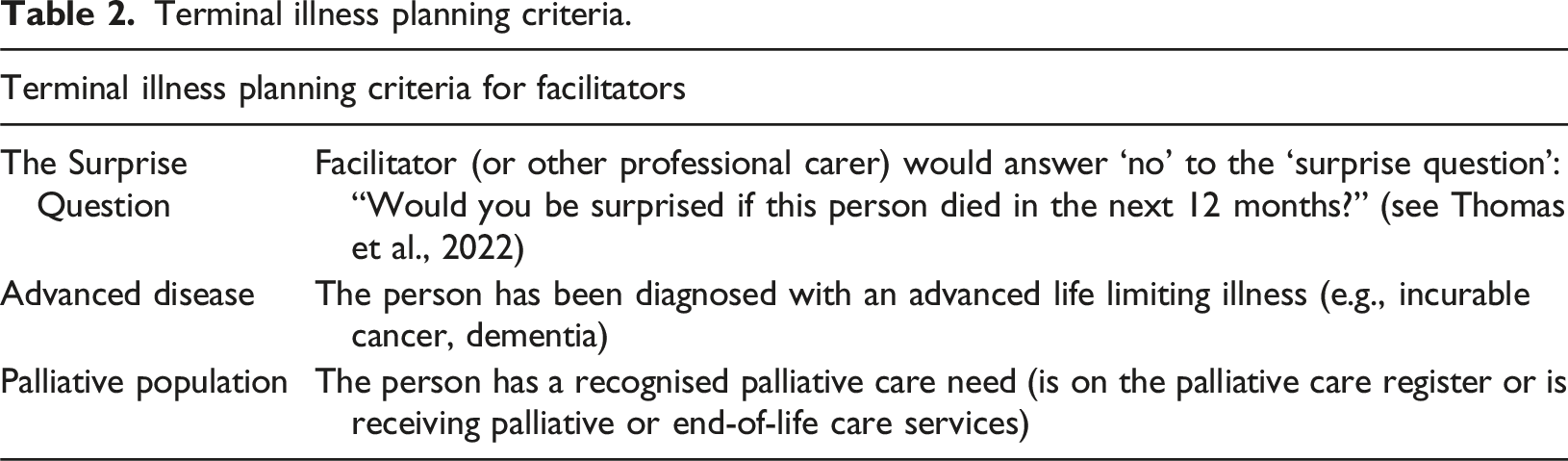
Terminal illness planning criteria.
The aim was to have three focus groups with a total of approximately 20 facilitators from the core evaluation, and one focus group with approximately eight service managers.
End-of-life care planning toolkit
Toolkit resources.
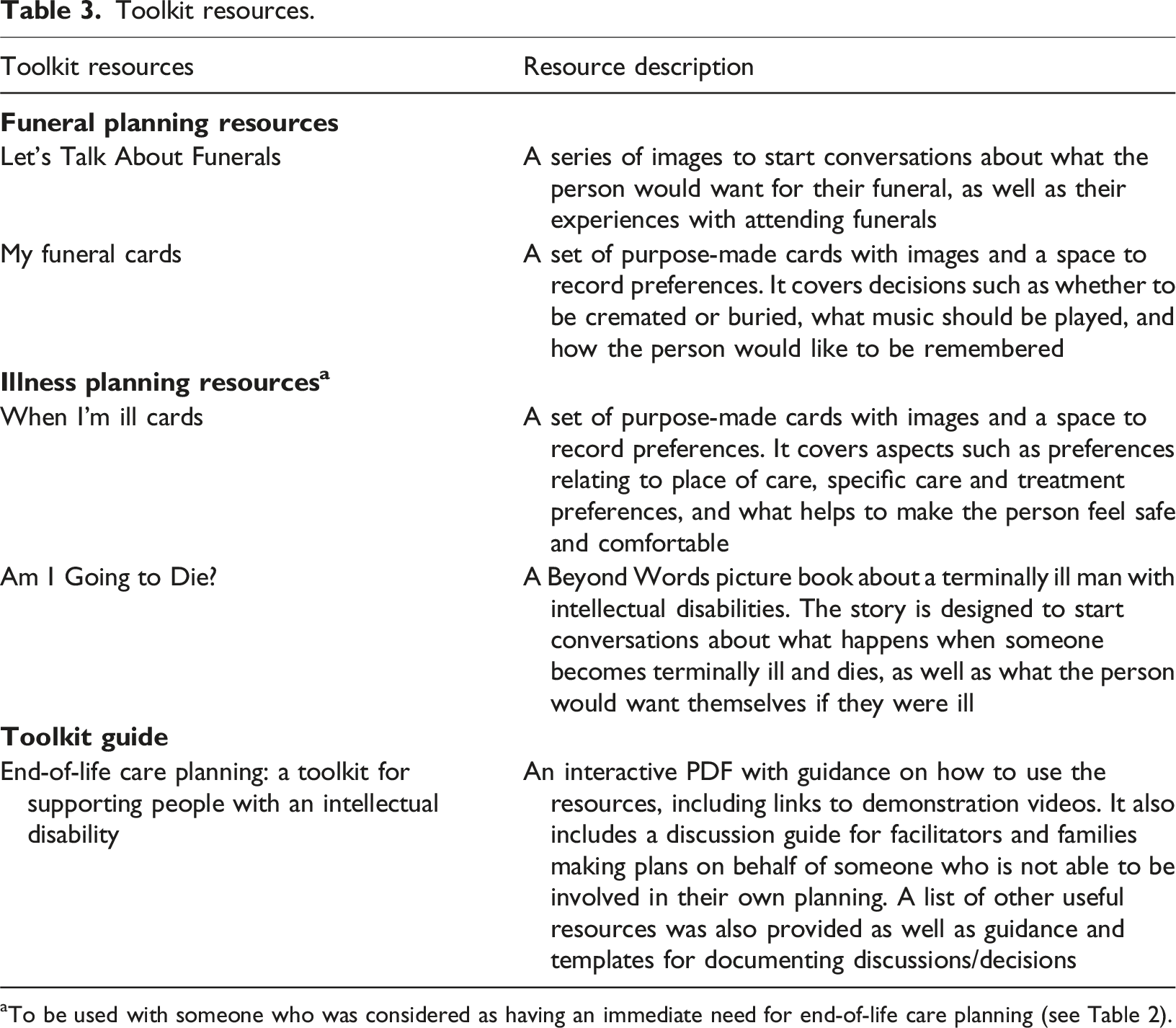
aTo be used with someone who was considered as having an immediate need for end-of-life care planning (see Table 2).
Recruitment
Core evaluation
Potential participants from MacIntyre and Dimensions were approached by the project leads. Smaller intellectual disability organisations were invited to take part, where the organisations identified potential participants. Study information was passed on with consent being obtained by the research team.
Wider feedback survey
Potential participants completed an online sign-up form; providing contact details, information about themselves, and who they intended to use the toolkit with. Consent was obtained as part of completing the sign-up form. The form was developed in Microsoft Forms, and distributed through the study website, social media, existing networks, and promoted at conferences.
Focus groups
Participants in the core evaluation were invited to take part in focus groups. Managers (not trialling the toolkit themselves) were invited to participate in a separate focus group. Smaller intellectual disability organisational managers were invited to take part, using snowball sampling. Study information was circulated with consent being obtained by the research team.
Data collection tools
Feedback forms (core evaluation and wider feedback survey)
Participants in both the core evaluation and the wider feedback survey completed an online feedback form, which involved responding to questions about who they used the toolkit with, which parts of the toolkit they used and how, and what they liked and/or disliked about the toolkit.
The forms were piloted by the team and with support staff from the toolkit co-design group (see Bruun et al., 2024a). Both forms were developed using Microsoft Forms. An example of the core evaluation form is included in Supplemental File 1. Paper versions and the option to complete forms over the phone were also offered.
Participants who withdrew from the study or did not manage to try the toolkit were asked to provide a reason why. They could still provide feedback on the guidance, training (if relevant), and general suggestions for improvements to the toolkit.
Focus groups
Participants were asked about their experiences of using the toolkit; viability, acceptability, usefulness of the toolkit; and sustainability of this approach to end-of-life care planning, including continued implementation within the organisation, and parameters and contexts. Topic guides are included in Supplemental File 2.
Two-hour online focus groups were held on Zoom. Sessions were recorded and transcribed verbatim. Researchers took field notes after and/or during each session.
Study procedures
Data were collected from October 2023 to February 2024.
Core evaluation
Participants attended training before testing the toolkit. The training was developed by the research team [AB, IT-W, and SG] and piloted with the wider team [FG, MW, NP, and SS], incorporating advice from the co-design group. The training covered: • Talking about death and dying in general and with people with intellectual disabilities. • How to plan with people with severe and profound intellectual disabilities. • Introduction to end-of-life care planning in general. • Presentation of the toolkit resources and how to use them.
The training initially involved two days of two-hour sessions. For day two, participants chose to focus on either funeral or illness planning. Later in the study, compressed three-hour “all-in-one” sessions were offered. Sessions were held on Zoom and facilitated by a minimum of two researchers. Sixteen training sessions were offered from October to December 2023.
Individual emails with links to the toolkit and the feedback form were then sent to each participant. A sheet with emotional support resources was also circulated. Participants were asked to print the toolkit resources themselves. The resources could be used as many times as the participants could manage within the study period. They were asked to submit one feedback form per planning session within the study period. A record of facilitators’ study progress was kept.
Wider feedback survey
Participants were contacted via email and sent the toolkit and feedback form. Participants had to print the resources themselves and could use them as many times and with as many people they wanted (one feedback form per planning session) within the study period.
Data analysis
Qualitative data from feedback forms, focus group transcripts, and field notes were coded using a modified framework approach. The Framework Method falls under the umbrella term for thematic analysis or qualitative content analysis approaches (Gale et al., 2013). The method involves creating a matrix of cases and codes with summarised data that provides a structure used to systematically reduce and then analyse the data. It is a flexible tool which is adaptable and allows the engagement of people without qualitative research experience (including researchers with intellectual disabilities) (Gale et al., 2013). The method was adapted to enable inclusive team discussions.
A matrix of deductive codes was produced based on questions from the topic guides and questionnaires. Data and analyses were discussed within the research team (including researchers with intellectual disabilities).
Results
Core evaluation and wider feedback survey participant numbers.

Core evaluation and wider feedback survey participants’ demographics.
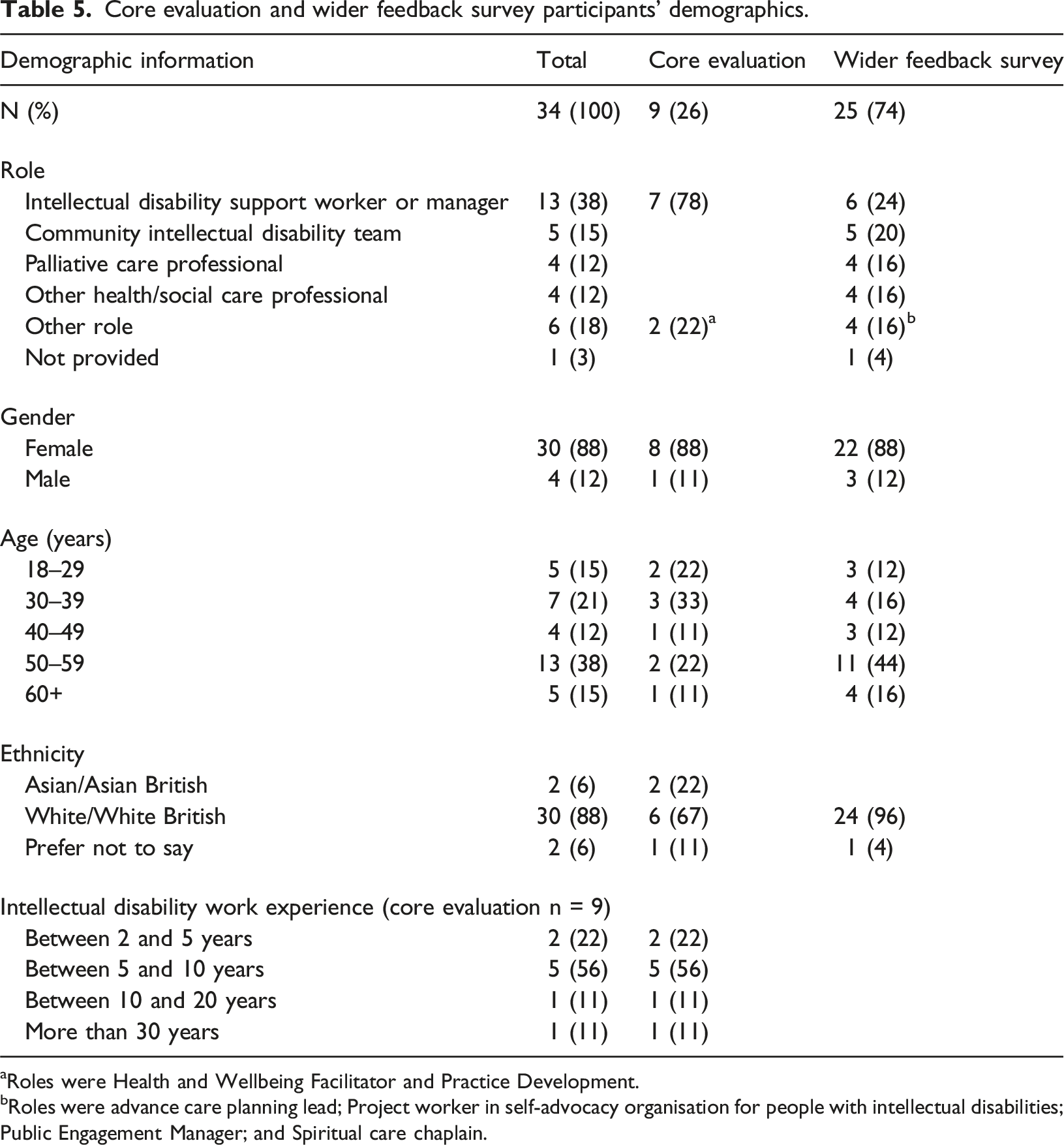
aRoles were Health and Wellbeing Facilitator and Practice Development.
bRoles were advance care planning lead; Project worker in self-advocacy organisation for people with intellectual disabilities; Public Engagement Manager; and Spiritual care chaplain.
Overview of study feedback forms.

Focus groups participants’ demographics.
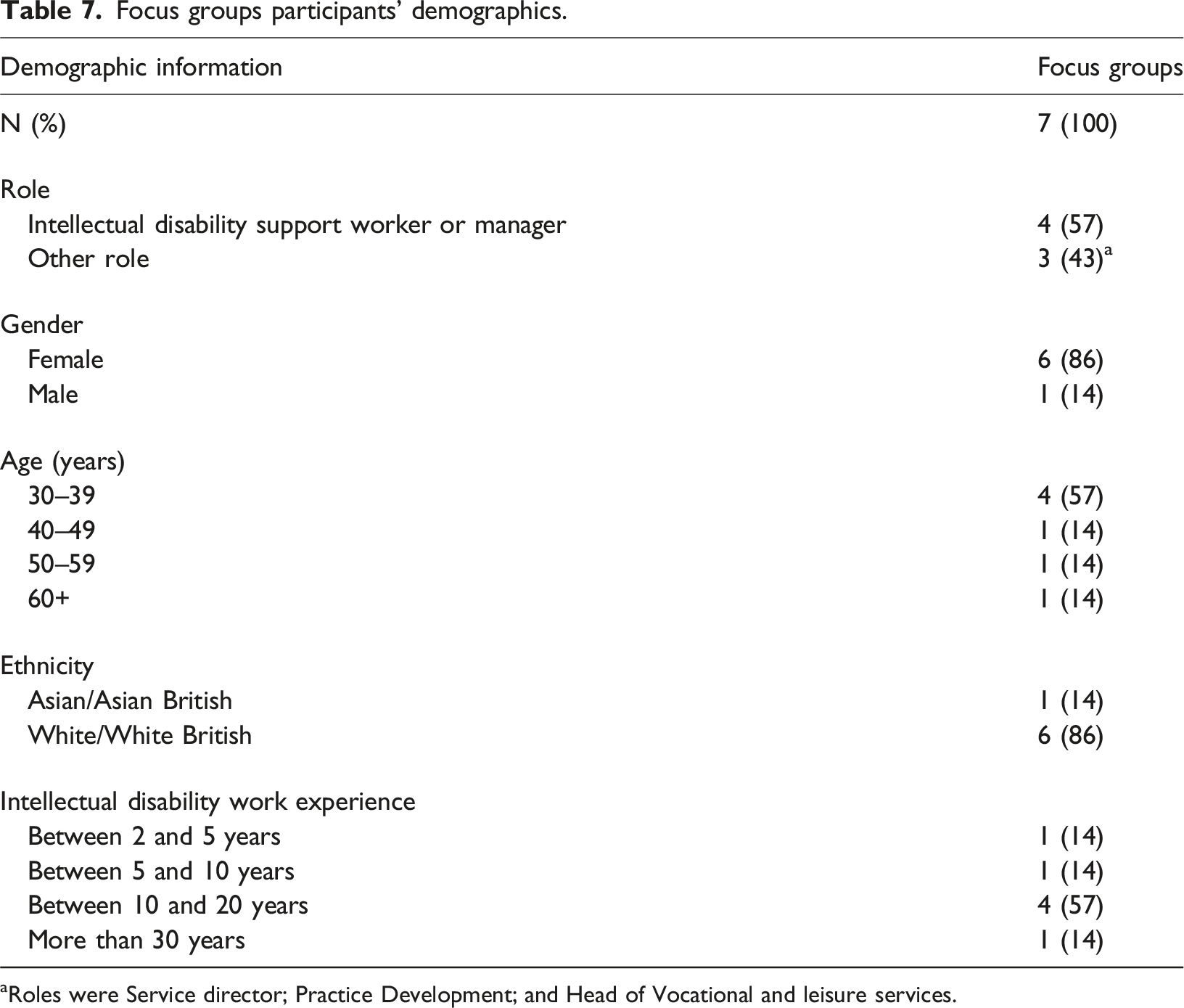
aRoles were Service director; Practice Development; and Head of Vocational and leisure services.
The main themes identified from the matrix template domains are presented in the following sections. Key participant quotes have been included to illustrate the themes.
Use of the toolkit
Facilitators reported using the resources in different ways, where they sometimes used all of the pictures or cards and at other times, they only used some of them. The reported length of planning sessions varied between 10 minutes and 2.5 hours.
Selection of individual pictures and cards
Facilitators explained how they were led by the person when selecting cards and pictures. This included spreading out the pictures or cards and letting them choose which ones to talk about, reflecting what they learned in the training. I placed the cards on the table, and they chose which ones they wanted to use TE-MC-20, Health and Wellbeing Facilitator (Feedback form entry, core evaluation)
Participants also described how they “worked through” the cards. They explained how they would discuss relevant ones and skip the ones that the person did not want to talk about. It seemed important to be led by the person and respect their boundaries. We worked through them together, using the checklist and talking about each one as they came up, but if the member did not wish to speak about them then we’d just move on TE-TK-23, Project worker in self-advocacy organisation for people with intellectual disabilities (Feedback form entry, wider feedback survey)
Other participants selected the cards in game-style activities where they took turns picking a certain number of cards in a group of people (including the Support Worker themselves).
Giving the person control
The importance of letting the person have control and decide whether they wanted to talk about the subject was implied from participants’ descriptions of what happened during the sessions. They explained how they asked the person if they wanted to have the conversation and try the resources. This could even involve a pre-meeting to “test the water” about how the person felt about it. We had a pre-meeting in the pub where we had a chat about age and plans and funeral planning, that meeting was to engage how up for it the person was to have further discussions and how difficult they may find it. We then made plans for a meeting to discuss further. FG-SM-03, Practice Development (Feedback form entry, core evaluation)
Some participants described how the person had been reluctant to discuss the topic at first, but then engaged more later in the session. Participants explained that the person had discarded certain cards (the guidance suggests having a ‘bin option’) where focusing on other cards could help to open up. Often the person wanted to revisit discarded cards, indicating increased comfort throughout the session. At first they did not respond well, but putting some of the cards aside and showing things like flowers, family, memorial plant the person began to slowly engage more TE-SM-01, Care/Support Worker (Feedback form entry, core evaluation)
Flexible, adaptable, and timely approach
Participants mentioned that a flexible approach was needed where several sessions over weeks or months may be needed. So it’s just making sure that people know that you don’t have to cover all of it. You could cover aspects of it in a day, and then not revisit again for two weeks it wouldn’t matter, or you can take half the cards out or so, knowing that it’s a really flexible bit of paperwork is very important. TE-MC-05, Service Manager (Focus group input)
It was stressed that it was important to allow enough time for the session. Time before and after for staff to prepare and debrief was needed as these were sensitive conversations. It’s one of the most important parts of their life at the end of the day. So you don’t want them to feel like you just rush there and then you’re doing it kind of at all. So, time to prepare for that time afterwards, you know, for both of you. So you can give them five min, or whatever is needed to make sure they’re okay. TE-SM-08, Service Manager (Focus group input)
Sessions could also be done in less formal ways, where one participant described having talked about relevant topics on park walks and asking questions throughout the day.
Participants explained how they used or planned to use the resources in combination with existing documentation or forms. Yeah, to look at what they think they already have in place and cross-checking that information because some people don’t have access to their funeral plans. They’re kept in the office. So, some staff don’t even know, because obviously staff change, don’t they? Staff move around. But luckily, I’m working with a guy who can tell me exactly what’s in his funeral plan. I’ve been checking with the individual people you’re supporting what they think they’ve already got in place. And then what conversations they might like to have. FG-SM-03, Practice Development (Focus group input).
They also mentioned how the resources could be used at annual reviews. These different ways of using the resources further highlighted their flexible and adaptable approach. In relation to this, it was noted that flexibility was important in adapting to individual communication needs to ensure understanding. I don’t feel like for every person you could just turn up with a toolkit and kind of crack on, so to speak. I do feel like you need to get it already, and then work out what you think may be better for that person. And yeah, adapt it, depend on the person. But no, I think it’s really, yeah, really, really good in that way TE-SM-08, Service Manager (Focus group input)
Involving others
Who should be involved in the planning was also discussed; participants mentioned the person’s family, friends, support staff, and other people important to the person. For example, my gentleman, in the past, when he was more able and able to communicate things. And I really thought about his past staff team, who no longer work with him. But how important they were in his life at the time. And they’ve since retired, or you know, maybe they’re not here anymore but the people that are still here. Maybe it would be really important to draw on some information from them TE-DM-07, Home Manager (Focus group input)
It was clear that who would or should be involved depended on what aspect you were planning for. One participant had worked closely with a hospice to support a man at the end-of-life and stressed how they should have been involved in the discussions.
It was also mentioned how some people with intellectual disabilities did not want to engage with the resources and wanted it left to their family.
Involvement of others, especially family members, was deemed particularly important if the person had severe and profound intellectual disabilities. I do think sometimes the family is a big impact on helping us understand them sometimes as well, especially if they’re non-verbal. Yeah. Cause sometimes somebody put a song on the phone and this person will just come alive. Yep, sorry the pun. But they sparkle. Didn’t realize they like that song family have such a big input, sometimes we forget because we don’t see them with the family much TE-SM-08, Service Manager (Focus group input)
It was also highlighted that involvement should be carried out according to the individual preferences of the person with intellectual disabilities. It’s knowing the families of the people you’re supporting as well, and how much involvement they would want to have and how to go about that, because some people you can be very informal with, and some people you need to have more formal. So you might want to wait for their sort of annual review and then bring it up then, or actually, it might just be oh, you know what we’ve done this document together? Can I share that with mum, and then you just send it across. You know, it really does depend on the person. TE-MC-05, Service Manager (Focus group input)
One Support Worker also questioned whether they were the right person to have this discussion with the person.
The environment
The importance of the environment in which the conversations took place was also highlighted. Participants mentioned being in a quiet setting and creating a cosy atmosphere with biscuits and tea. Setting up and having everything ready to avoid disturbance or interruption of the flow was also mentioned.
Enablers and facilitators
Participants positively assessed the resources and labelled them useful, helpful, and easy to use. It was mentioned how the opportunity to have a relaxed one-to-one conversation with time to simply sit, talk, and listen was enjoyable. Helpful ways of using the toolkit are highlighted in the use of the toolkit section. Other enablers are listed in the sections below.
Straightforward and personalised approach
Participants positively described how the resources were straightforward compared to other rather lengthy organisational forms and documentation. To be honest, because paperwork at the moment. The ‘my plan for: before I die’ is 45 pages and to be like, you know, flicking through it all and trying to find the right piece to talk about. If you want to skip that bit. That is quite that is quite overwhelming. Where is when you’ve got these pictures that you can just put on the table to like you say, spark the conversation, or put in the bin. If you don’t want to speak about that. TE-DM-07, Home Manager (focus group input)
Along with the flexible approach, it was mentioned how the resources could be personalised or used in combination with other pictures. You could personalise it to the person’s illness, and also what’s going to happen to them, based on professional information that you’ve been given, or that the staff have been given. FG-SM-03, Practice Development (Focus group input)
Resource as discussion prompts
Participants explained how the resources were used as prompts or an agenda for what to discuss. This was described as useful, especially when dealing with an unfamiliar topic. It helps us to know what sort of things we should be asking, what sort of things we should be talking about, because, you know, we’re support workers we’re not funeral planners. So it’s very hard for us to think about all the different things that might be involved in a funeral. (…) for us to just be able to look at the cards and say, right, these are the sort of things we need to be thinking about and covering is that relevant? Is that not relevant? And then go from there. And it’s yeah. I think in that respect it’s really helpful. TE-MC-05, Service Manager (Focus group input)
Participants positively described how the person was engaged in the conversation and how the resources helped them to think and talk about their experiences, memories, thoughts, feelings, and ideas. These conversations were often described as eye-opening and surprising as participants had not heard people talk about the subject before. I think using the cards was really amazing for opening up conversations that I have never had with people who I have worked with for over two years. I think some of these conversations would never have been had if not for these cards. TE-TK-46, Intellectual disability support worker or manager (Feedback form entry, wider feedback survey)
Participants generally reported having interesting and positive conversations. Conversations were described as both hard and comfortable, and as uplifting with humour as well.
Breaking the taboo
Talking about end-of-life care planning within the organisation, with the team, and even with families was seen as a facilitator to having these conversations. I think how we are going to use the toolkits with our parent and carer group is like showing them the tools and saying, these are some of the things that are available that we could use with people like, what are your thoughts? What scares you? You know what is good about it? What is not good about it? So, because unless you do some of that, people will always think that they’re really difficult conversations to have, but they don’t always have to be, do they? FG-SM-03, Practice Development (Focus group input)
It was noted how confidence was key, which may be gained by becoming more comfortable with discussing the topic. I think half of it is confidence. It’s confidence to have that conversation and not feel awkward, because as soon as you give off that… I don’t know what the word is, but if you’re not confident and you’re jittery, and oooooh you’re like, you know, I need to talk about this. It makes them feel uncomfortable as well. And actually, we wanna be talking about this really, openly and comfortably. And you know, just a general chitchat about it rather than ‘Right! Let’s sit down and make this funeral plan’ TE-DM-07, Home Manager (Focus group input)
One participant shared how a recent death in the service had opened up conversations about another person’s funeral preferences.
Staff training and support
Staff highlighted the need for support in doing end-of-life care planning, including management support after using the resources. But if they [staff] did, and if they did go out and do this with somebody, I, you know. Besides. And you need to tell me what you need. Do you need time before and after, like I was suggesting? Or, you know, do you wanna have a chat to me? [….] I am here. If they need that. It’s just about like communication. I think, with them, knowing that there’s options if they need it. TE-SM-08, Service Manager (Focus group input)
Staff training was also mentioned, and participants suggested this should ideally be facilitated by people with intellectual disabilities to increase impact. Dedicated end-of-life care planning sessions were also suggested.
Organisational investment
It was highlighted from an organisational management perspective that work should be put into creating awareness of and implementing the toolkit on a strategic level. But I also think that there needs to like be some strategic stuff like about what we do as an organisation. Because we do that stuff where we talk about giving people good support, employment. You know, active in their communities. But having some really broad statements that we’re going to get people to have really good end of life care planning systems in place, you know as well, because I think sometimes, I’m not saying that organisations don’t think that they’re important. That’s not what I’m saying. But okay. But I think they become important at really difficult times. And so, you know, you have to also invest that in your staff team as well, don’t you? With, you know, from an organisational point of view. FG-SM-03, Practice Development (Focus group input)
This also involved sharing good practice and building resources as an organisation.
Barriers
Emotional and taboo subject
It was acknowledged that end-of-life care planning was not an easy subject. I don’t think there is anything about the toolkit that hasn’t worked well, I think it’s more the subject itself is hard to approach sometimes. TE-TK-20, Intellectual disability support worker or manager (Feedback form entry, wider feedback survey)
Participants explained that it had required multiple attempts before the person opened up (which then led to a positive experience). One participant stressed how thorough and timely feedback to the person’s family was important, which further underlined the sensitive nature of these conversations.
Staff highlighted how it could be difficult to naturally initiate the conversation despite using the resources. I think one of the problems we’re having is starting the conversation, because how do you? You know you go into someone’s flat as usual in the morning, like, talk about your funeral today. And it’s a really weird thing to start organically. TE-MC-05, Service Manager (Focus group input)
Similarly, the end-of-life was seen as a taboo within organisations.
The fear of upsetting or worrying the person with intellectual disabilities was also mentioned. One of my questions is because when I looked, am I going to die? Book? I immediately thought, [name] lady with cancer is not gonna like that. And she’s gonna worry then. And I need to talk someone before showing her the book, even because I just think It’s gonna worry her. She’s going to do nothing but worry. TE-SM-18, Care/Support Worker (Focus group input)
Staff were also aware of how their own fear of the topic could lead them to postpone the conversation. They thought guidance materials were useful but they did not provide them with the confidence needed. Yes, that went alongside the toolkit. I did like that, and I thought it read really well, but I still don’t think it gives you the confidence on that side of things. TE-DM-07, Home Manager (Focus group input)
Organisational challenges
Facilitators mentioned several organisational and practical challenges as barriers, including staffing, collaboration and coordination, and printing the resources.
Staffing
One barrier was the unpredictable nature of staffing. In hectic care environments, staff schedules may change last minute due to unforeseen circumstances. Staff leave, meaning their knowledge of the person can be lost. Staffing challenges meant involvement of bank staff who were only periodically involved in the person’s care. I don’t know how it works, and it’s like that is the next step to find out and suggest to my boss, you know. Give it both options. What do you want to do, because I’m not here every day of the week. If I was here every day of the week I’d be on it. But cause I’m not here every day of the week. Yeah, I visit once a week. Maybe so. Yeah, I am. Find it bit more difficult once a week. TE-SM-18, Care/Support Worker (Focus group input)
Collaboration and coordination
Coordination and documentation of the conversation were considered important. This was to avoid duplication of work and overburdening the person with intellectual disabilities. You’d have to be mindful of when you’re using it, because in these organisations you have people, so many people that you might find one person service user having someone talking about it all the time. So I think it has to be regulated or noted when it’s being used. Because if we don’t know each other’s using it, that poor person has someone talking about being poorly and going to hospital every day of the week, but I think it just needs, it needs control. It needs to be controlled. But I do think it’d be helpful for everyone to know it, and be mindful TE-SM-18, Care/Support Worker (Focus group input)
It was also highlighted that coordination between services should be in place to avoid conflicts between teams, for example between support staff and in-home palliative care staff. Yeah, cause sometimes the conversations would contradict themselves. You know I would go in and say to him, oh, you know, ‘have you considered changing to a profiling bed?’ And he’d be like, ‘no, absolutely not’. And then the hospice work would come in the next day and be like, ‘oh, he’s agreed to have a profiling bed’. It’s like, ‘oh, okay’, how the conversation went TE-MC-05, Service Manager (Focus group input)
Printing the resources
Staff explained how they needed time to get into an office to print the resources. It is just finding the time to go to the office and get things printed. TE-SM-18, Care/Support Worker (Focus group input)
The practical aspect of not having laptops and needing help from administrative staff was a fundamental barrier to implementing the toolkit in practice.
Supporting people with severe and profound intellectual disabilities
The idea of using the resources with people with severe and profound intellectual disabilities or with people who lack capacity was described as challenging. It’s not always easy with people who have good communication and all of that but for people with profound and multiple learning disabilities and medical you know, it, it’s quite hard you have to do those things, because you know, you would be relying on a lot of information that’s written, or by people that know them, but you know it could be people that haven’t got no family, and histories of being forgotten or lost along the way. FG-SM-03, Practice Development (Focus group input)
This was related to a general critique of most resources being tailored to more able people.
No one size fits all
While the toolkit was described as a more straightforward alternative to lengthy planning forms, it remained overwhelming to some participants. I think the only thing I would worry about is on face value. The toolkit can look a bit overwhelming. It’s like, oh, there’s a lot of things to talk about. TE-MC-05, Service Manager (Focus group input)
It was also noted how these resources may not be useful for everyone, where some people may prefer something on TV instead.
Guidance and training feedback
The guidance resource was positively assessed as ‘really good and motivational’, and ‘very helpful’. It was described as positive, encouraging, and supportive, and the format was descried as attractive and looking nice. Some participants mentioned they had rushed through it, and that it would have been helpful to offer it in larger print, although they still evaluated it positively.
The training was also described as helpful. It is really helpful and gave us ideas and tips how to do it and got a chance for us all talk about it TE-SM-15, Care/Support Worker (Feedback form entry, core evaluation)
Other feedback
Participants were encouraged to list cards or pictures that were missing in the toolkit. Most participants expressed that a wide range of topics was covered, but suggestions included hospital forms, animals/pets, family members and partners, order of service, and bed baths.
Participants also thought the resources could be used with other groups of people such as people living with dementia.
Participants who did not use the toolkit
The study team experienced significant difficulties with recruiting participants. A high number of participants were lost to follow-up or withdrew from the study. Many participants did not reply to reminder, follow-up, and check-in emails. Others remained in the study but were unable to use the toolkit with a planner within the study period.
The main reason for not having tried the resources was the pressure of other work commitments or unforeseen circumstances. Time was an important factor, and participants explained they had not had the opportunity yet. Just have not had time with other work commitments, and with the time given and the sensitivity need more time TE-DM-08, Home Manager (Feedback form entry, core evaluation)
Similarly, those who withdrew from the study said they did not have the time to take part (including attending training, testing the resources, and completing forms).
Some participants from the wider feedback survey also explained how they did not have anyone eligible to use the toolkit with (e.g., palliative care professionals with no people with intellectual disabilities in their current caseload).
Another significant barrier was the study period, which included Christmas, where participants reported that it was not the right time to bring up the topic.
Preliminary feedback
Despite not having tried the resources, it was clear that participants who completed feedback forms had looked at the resources and read the guidance. Participants liked the guidance, which they described as clear, informative, and useful. They liked its format and found the videos helpful.
Those who had participated in training sessions thought it was good and helpful.
Participants positively evaluated the overall toolkit and its potential benefits. Some people still hoped to try the toolkit outside the study period. They also mentioned the potential wider applicability of the toolkit with people with dementia or acquired brain injury.
Discussion
Main study findings
Participants generally welcomed the end-of-life care planning toolkit resources and its flexible, straightforward, and adaptable approach. They reported how the resources prompted positive and eye-opening conversations. Barriers persisted around the sensitive end-of-life topic; the need for breaking the taboo and for staff training and support was highlighted. Lack of time was a major barrier. Other organisational challenges included staffing issues and problems with printing the resources.
Findings in relation to existing literature
The positive evaluation of the toolkit indicates that the participants found the end-of-life care planning toolkit acceptable and appropriate, according to the implementation outcome framework. This further indicates that the toolkit co-design process was successful. This aligns with evidence suggesting that materials are perceived to be more applicable to end users as a result of co-design (Slattery et al., 2020). Participants described the ways in which they had used the toolkit resources, which aligned with the training they had received and the intention behind the toolkit, indicating a high degree of implementation fidelity. Participants valued the flexible approach involving visual resources, which has also been deemed successful in other contexts with people with intellectual disabilities such as planning for the future (Anderson-Kittow et al., 2024) and projects on talking about dying (MacIntyre, 2023). The findings add to the evidence showing how conversation starter resources can be successful in facilitating advance care planning (Eneslätt et al., 2021; Möller et al., 2020; Sussman et al., 2022). The toolkit was refined based on the findings, and the final toolkit was launched on the study website (www.victoriaandstuart.com/) in June 2024.
Despite the positive feedback, there seem to be significant overarching challenges to effectively implementing the toolkit in practice. There were issues with toolkit uptake, which relates to implementation adoption and feasibility. One of these challenges was the end-of-life topic that the toolkit covered. It is well-known that there are challenges with talking about death and breaking bad news to people with intellectual disabilities (Bruun et al., 2024b, 2025; Tuffrey-Wijne, 2013; Tuffrey-Wijne et al., 2013, 2017, 2020a, Wiese et al., 2013, 2014). The study team anticipated that the end-of-life topic would be challenging and included a section during the training session focusing on talking about death and dying in general and with people with intellectual disabilities. However, the fact that the topic was still a major barrier calls for the need for wider cultural and organisational changes within intellectual disability services. To gain the confidence needed, staff need to talk about death and dying not only with the people they support, but also with each other and their managers. Services should offer ongoing staff training and support as such initiatives are necessary to effectively implement end-of-life care planning tools (McKenzie et al., 2024). It should be acknowledged that death and dying also present a barrier on a societal level (Sallnow et al., 2022); which may also explain some of the recruitment challenges.
The high number of participants who either withdrew from the study or never used the resources also indicates issues with implementation adoption and feasibility. This may be because of a lack of time, which is a sign of an overstretched social care sector. Sensitive and personalised end-of-life care planning requires time, including practical aspects as time for printing. However, adult social care in England is facing several workforce challenges including high vacancy rates, rising demand, high turnover, low pay, and little standardisation of training and qualifications (Foster, 2024). Nevertheless, it is a service requirement to have such plans in place (Care Quality Commission, 2016). End-of-life care planning should be a priority, and solutions to these overarching challenges are needed.
In this study, we have taken the first step in assessing early implementation outcomes by evaluating the use and uptake of an end-of-life care planning toolkit. The findings indicate that the focus of future work should not be on further development of new resources for end-of-life care planning, as the co-produced resources were found to be acceptable and appropriate. Rather, next steps would include further exploration of how to overcome the significant challenges with adoption and feasibility of using these resources in practice. An exploration of the remaining, mid- to long-term, implementation outcomes (i.e., costs, sustainability, and penetration) would also be beneficial.
Study strengths and limitations
The comprehensive and complex study design, including lengthy Participant Information Sheets, was the main barrier to participant recruitment and retainment. Future research should be mindful of an overstretched social care sector when designing evaluation studies to ensure they are feasible in practice. Research Ethics Committees should accept that study information materials may need to be short and straightforward. More time should be spent piloting procedures with staff to ensure they are manageable and can be completed within study and staff timeframes.
The complexity of the feedback forms meant that some data could not be analysed in depth. Data on which resources participants had used could not be linked to the individual resources. Future research should be aware of such limitations when creating surveys. More research is needed to understand and assess the implementation fidelity of the toolkit resources.
Due to recruitment and retainment challenges, further testing is warranted, particularly with individuals who are terminally ill and approaching the end-of-life and people with severe and profound intellectual disabilities.
The study sample lacks ethnic and cultural diversity. As end-of-life care planning is impacted by the person’s ethnicity and cultural background (Bruun et al., 2025), it is important to explore those views further. Future research should aim at recruiting a more balanced study sample.
Conclusion
The co-designed toolkit of resources and approaches for end-of-life care planning with people with intellectual disabilities was positively evaluated by participants. However, to effectively implement the toolkit within intellectual disability practice, more research is needed, and attention should be paid to address the overarching challenges around the sensitive nature of discussing death and dying and a lack of time within an overstretched health and social care sector.
Supplemental Material
Supplemental Material - Evaluating a toolkit for end-of-life care planning with people with intellectual disabilities: An exploration of implementation outcomes within intellectual disability social care services
Supplemental Material for Evaluating a toolkit for end-of-life care planning with people with intellectual disabilities: An exploration of implementation outcomes within intellectual disability social care services by Andrea Bruun, Amanda Cresswell, David Jeffrey, Leon Jordan, Richard Keagan-Bull, Jo Giles, Faye Gardiner, Meg Wilding, Nicola Payne, Sarah Swindells, Sarah L. Gibson, Rebecca Anderson-Kittow, Irene Tuffrey-Wijne in Journal of Intellectual Disabilities.
Supplemental Material
Supplemental Material - Evaluating a toolkit for end-of-life care planning with people with intellectual disabilities: An exploration of implementation outcomes within intellectual disability social care services
Supplemental Material for Evaluating a toolkit for end-of-life care planning with people with intellectual disabilities: An exploration of implementation outcomes within intellectual disability social care services by Andrea Bruun, Amanda Cresswell, David Jeffrey, Leon Jordan, Richard Keagan-Bull, Jo Giles, Faye Gardiner, Meg Wilding, Nicola Payne, Sarah Swindells, Sarah L. Gibson, Rebecca Anderson-Kittow, Irene Tuffrey-Wijne in Journal of Intellectual Disabilities.
Footnotes
Acknowledgments
We would like to thank all the collaborators, services, and all the people who were involved in the study. We would like to thank our wonderful All Together Group members for all their hard work in developing our toolkit: David, Dimensions; David Whilton, MacIntyre; Jordan Smith, Dimensions; Pat Charlesworth, PCPLD Network; Sui-Ling Tang, MacIntyre; Jan Blair, Dimensions; Jo Allmond, MacIntyre; Kaddy Thomas, Elijah’s Hope CIC; Martin Boniface, Dimensions; Parmi Dheensa, Include Me TOO; Brenda Pothecary, Dimensions; Jan Michael Kendall, MacIntyre; Mia Green, Dimensions; Mika Pickles, MacIntyre; Ryan Mitchell, Dimensions; Tina Murray, MacIntyre; Astrid Ubas, MacIntyre; Chris O'Donnell, Enfield Integrated Learning Disability Service; Dr Jo Elverson, St Oswald’s Hospice; Phoebe Mooney, St Christopher’s; and Sarah Pope, Enfield Integrated Learning Disability Service. We would also like to thank our Research Advisory Group members for valuable input throughout the study: Adrienne Betteley, Macmillan Cancer Support; Dr Annie Stewart, PCPLD Network; Dr Catherine Millington-Sanders, RCGP & Marie Curie; Chris O'Donnell, Enfield Integrated Learning Disability Service; Gary Bourlet, Learning Disability England; Hille Voss, Ben Sajet centrum; Jean Willson OBE, Centre 404; Joanna McIlmurray, Battersea Healthcare CIC; Justine Button, Care Quality Commission; Kathryn Mannix; Lucy Winter, L'Arche UK; Making Families Count; Melanie Taylor, Hospice UK; NHS England; Dr Nic McKenzie; Peter Allum, GRASSroots and PCPLD Network; Sarah Pope, Enfield Integrated Learning Disability Service; Sam Royston, Marie Curie; Samantha Clark, Learning Disability England; Sarah Offley, Dudley Voices for Choice; Simon Blake; Sue Marsden, Greenwich & Bexley Community Hospice; Usha Grieve, Compassion in Dying; and Vince Peters, Dudley Voices for Choice.
Ethical considerations
The study received ethical approval from Social Care Research Ethics Committee (23/IEC08/0033) on 03/10/2023.
Consent to participate
All study participants had to read and understand a detailed Participant Information Sheet and provided informed written consent to participate in the study.
Author contributions
Study design: AB, AC, DJ, IT-W, JG, LJ, RA-K, RK-B, SG; Recruitment: AB, FG, MG, NP, SG, SS; Data analysis: AB, SG; Manuscript writing: AB; Approval of manuscript: AB, AC, DJ, FG, IT-W JG, LJ, MG, NP, RA-K, RK-B, SG, SS.
Funding
The study was part of a research project funded by The National Institute for Health Research (NIHR) Research for Social Care (RfSC), Research for Patient Benefit (RfPB) Programme (NIHR202963).
Declaration of conflicting interests
Prof Irene Tuffrey-Wijne is a Beyond Words trustee and one of the authors of the Am I Going to Die? Book.
Data Availability Statement
Descriptive metadata will be made available on the Kingston University London Research Data Repository in 2024. Full data will not be available, as they are not anonymised. Other relevant and shareable study data are presented in the paper or available in the supplementary files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.