
Abstract
Keywords
Introduction
Attention for self-determination of persons with intellectual disabilities increased significantly in recent decades in the fields of education, health care, and research (Mumbardó-Adam et al., 2023; Wehmeyer et al., 2017, Wehmeyer, 2020). However, it is still not clear how to apply this concept with persons with severe or profound intellectual and multiple disabilities (SPIMD). This population is characterized by a combination of cognitive limitations and additional motor, sensory, communication, and health problems that make them heavily dependent on others for everyday tasks (Nakken & Vlaskamp, 2007; Van Timmeren et al., 2017). Access to their subjective experiences and point of view is furthermore limited (Maes et al., 2021). Research on self-determination, like on other topics, often engages with closely involved caregivers, studying and describing their intimate understanding of the person with complex support needs within specific settings and feeding back those findings (Jacobs et al., 2018; Kruithof et al., 2020; Petry et al., 2005; Watson, 2012). To address the call for better understanding how self-determination may be related to interventions and outcomes (Kuld et al., 2023; Mumbardo-Adam et al., 2023), the current study sought to operationalize the psychological constructs of autonomy support and basic psychological needs as perceived by parents or other family carers of persons with complex support needs.
According to Basic Psychological Needs Theory (BPNT), a mini-theory under Self-Determination Theory (SDT), every person possesses three innate basic psychological needs (BPNs), the satisfaction of which are important for psychological health. The BPNs regard autonomy, competence, and relatedness (Deci & Ryan, 2012). Opportunities for fulfilling these BPNs contribute to the emergence of intrinsic motivation, self-regulation, and well-being (Deci & Ryan, 2000; Ryan & Deci, 2000a, 2000b). Material and especially social environmental circumstances may thwart or promote autonomous behaviour. Need satisfaction is linked to having an autonomy supportive social context, in which the voluntariness of action is respected and encouraged, feedback on competent performance is informative, and the person is made to feel accepted and part of a group (Deci & Ryan, 2000; Soenens et al., 2007). Although cognitive and functional impairments may hamper one’s ability to be a causal agent who creates and takes opportunities for need fulfillment (Fusinska-Korpik & Gacek, 2022; Shogren et al., 2017; Wehmeyer, 2020), associations between perceived autonomy support, BPN satisfaction, autonomous motivation, and well-being have been empirically demonstrated among persons with less severe intellectual disabilities (e.g., Behzadnia et al., 2022; Frielink et al., 2018). Regarding persons with the most complex support needs, Beadle-Brown et al. (2021) found positive associations between active (i.e., empowering) support and several quality-of-life domains. Thus, the relation between quality of support and quality-of-life may potentially be conceptualized in a self-determination framework for this latter group as well.
Skarsaune et al. (2021) argued for a relational understanding of the phenomenon of self-determination for persons with the most complex support needs. Self-determination would be facilitated in this population if others around the person look out for the many ways in which the person expresses desires, volition, and satisfaction, and are likewise aware that self-determination lies “not only in decisions about where to live or how to spend money, but also in ongoing processes of being understood—for instance, help with burping after eating or being met on the need for proximity” (Skarsaune et al., 2021: p. 324). Van Tuyll van Serooskerken et al. (2022) also explored what deeper meanings BPNs might have for persons with complex support needs through conversations with their primary relatives. Again, self-determination went beyond “making choices.” While there appeared little to no self-awareness of one’s abilities or actions (e.g., movements), gratification could occur when persons with complex support needs “just” did or experienced the things they liked. According to their relatives, BPNs could be found in both subtle, idiosyncratic proactive and reactive expressions of preferences regarding, for example, food, bedtime rituals, motor actions, and persons in the environment. In addition, support of BPNs resulted from complex interactions in which sensitive responsiveness was crucial.
Autonomy-supportive interactions imply intensive involvement of social partners, such as carers (Watson, 2012). A literature review by Hostyn and Maes (2009), for example, emphasized that high-quality interactions with parents and others (e.g., family members, healthcare professionals) would positively affect the quality-of-life of persons with complex support needs. However, providing helpful scientific insights to partners involved in their support is fraught with methodological challenges. This makes it difficult to assess support requirements for persons with extensive needs and evaluate support that may be given to carers (Kuld et al., 2023). Despite the risk for bias, one way to access inner experiences of persons with complex support needs in research and practice is to seek the perspectives of parents. Parents have a lifelong connection with their child and usually fulfill the role of crucial advocate for sharing knowledge about their child’s needs with other involved parties (Kruithof et al, 2020). Mothers of children with complex support needs believed that their understanding of their children's needs added to what they believed that the perspectives of healthcare professionals were (Adams & Jahoda, 2019). The perspectives of parents on what their children may be thinking and feeling are thus valuable sources of information in their own right.
Taken together, the aim of the present study was to develop and test two questionnaires for parents of persons with complex support needs. One construct we sought to operationalize was parents’ perceptions of autonomy-supportive experiences of their child with all key partners in the environment. The second construct regarded parents’ perceptions of their children’s signals reflecting BPNs. Both constructs were chosen because, according to SDT, autonomy support and signals of basic needs relate to quality-of-life and well-being but have not been studied in people with complex support needs. Currently available scales for mapping constructs related to self-determination are often designed on the basis of the concepts within causal agency theory (Vicente et al, 2020). However, these instruments seem less suitable for persons with extensive support needs as items assume higher cognitive functioning, like goal setting and having beliefs about achieving that goal. As a result, these instruments differentiate little between individuals (i.e., they all score low on all items) and yield little information other than the fact that persons with more severe intellectual disabilities show very limited self-determination capacity levels (Carter et al. 2009). Building on work on universal dimensions of autonomy support and BPNs, instrument development was based on existing instruments on both constructs, while informed by research into their meaning for parents (Van Tuyll van Serooskerken et al., 2022). We asked first what the most unambiguous and parsimonious internal structure was for each questionnaire within this sample. Second, we examined the internal consistencies of the found structures. Third, we examined evidence for construct validity by assessing conceptually related constructs (i.e., subjective well-being and quality-of-life of the person with complex support needs as perceived by the parent). The communication and influence domain of quality-of life was chosen because of the conceptual overlap with self-determination which also underlies the constructs measured with both new questionnaires.
Methods
Data resources and study participants
Demographic Information of Participants and Persons With Complex Support Needs.
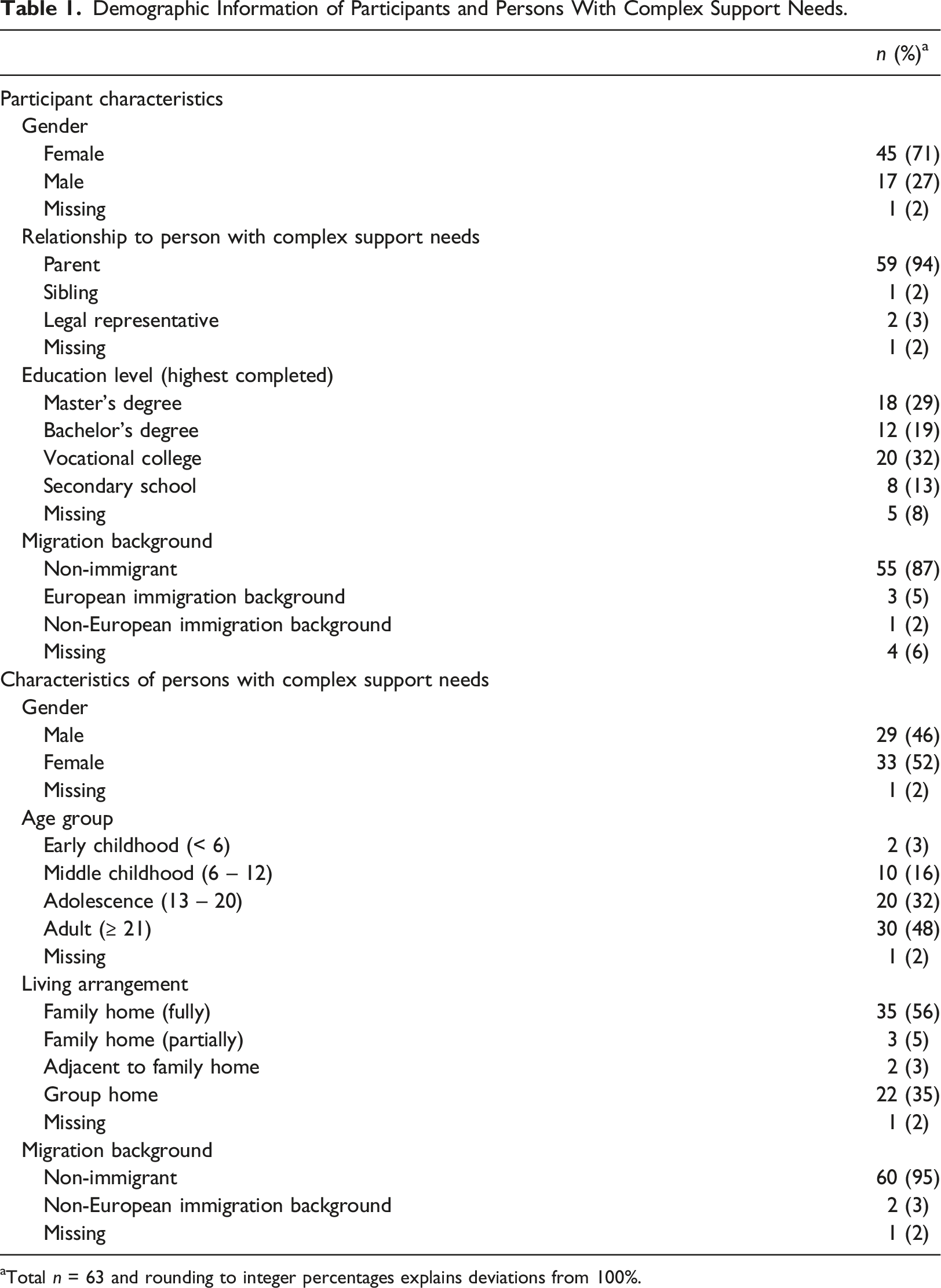
aTotal n = 63 and rounding to integer percentages explains deviations from 100%.
Instrument development
The two new instruments were developed by six researchers from the field of child development who all had substantial work experience with persons with intellectual disabilities. One of the researchers is also a parent of a child with complex support needs. For each of the two key concepts (autonomy-supportive experiences and BPN signals), pre-existing measures were identified through literature search. Results of a qualitative study by Van Tuyll van Serooskerken et al. (2022) on primary relatives’ perspectives about the meanings and support for the three BPNs in their family member with complex support needs guided the selection of base instruments and their further adaptation and expansion.
Parental perceptions on autonomy-supportive experiences
The Perceptions of Parents Scale – College-Student Scale (POPS; Robbins, 1994) was used as a starting point for the development of the questionnaire on autonomy support for persons with complex support needs. This questionnaire was chosen because it operationalized domain-general autonomy support rather than domain-specific autonomy support, which regards support in domains in which persons with complex needs seldom participate (e.g., school, sports, paid work). Items were translated and adapted to suit parents reporting on the support they themselves provided as well as that of other caregivers closely involved (e.g., social workers) in their child’s life. All items were therefore initially focused on the parent by starting with the phrase “To what extent do you notice that persons currently most involved in your child’s environment …,” with the instruction to answer the question from their child’s perspective as much as possible. Example items that followed this phrase were “… involve him/her in matters that concern him/her?” or “… present him/her with suitable choices?” After leaving out 5 items that did not apply (e.g., “My mother/father listens to my opinion or perspective when I’ve got a problem”), the 16 remaining adjusted items had to be rated on a 5-point Likert scale ranging from “not at all” to “very much.” Because participants were not always parents, instruction was added to read “the person with complex support needs” if it said “my child” when applicable.
Parental perceptions on basic psychological need signals
The initial aim was to adapt an existing questionnaire from the perspective of BPNT, in collaboration with experts (i.e., parents and professionals) in the field (n = 7), as a proxy version suitable for parents of persons with complex support needs. The Dutch Basic Psychological Need Satisfaction and Frustration Scale seemed most appropriate as it already was successfully adapted for self-report by persons with mild intellectual disability (BPNSFS-ID; Frielink et al., 2019). However, despite exhaustive modification attempts, it was impossible to create a meaningful version of the existing items that could potentially lead to variation within the target population. The experts did not perceive these aspects in their child or clients, but they did notice other things that they associated with the psychological basic needs (Van Tuyll van Serooskerken et al., 2022). Consequently, the approach changed towards generating new items within the dimensional space of the BPNSFS-ID (i.e., constructs related to satisfaction or frustration of autonomy, competence, and relatedness). Furthermore, the scope was changed to parents’ perceptions about “reading” or noticing signals that they believe reflected BPNs, rather than trying to capture the actual experience of satisfaction or frustration of BPNs as experienced by the child, a task that according to the experts was virtually impossible.
During the generation process all items were continuously discussed and tested with the experts, based on which further adjustments were made. In total 36 new items were developed, six for each construct, which all had to be rated on a 5-point Likert scale ranging from “never” to “always”. Subsequently, to optimize the number of items on relevance and burden for respondents, the draft questionnaire was subjected to item reduction. First, the distribution of item responses was inspected to check for variability within this target population. Because people with complex support needs are highly heterogeneous in their behaviors and expressions, variation in item responses were expected. Any item where more than 40% of participants answered “never” or “always” combined with less than 5% answering the other extreme was removed (i.e., 5 of 36 items, see Supplementary material, Table 1). These items were indicative of high skewness and kurtosis, and thus indicate low informational value. Second, participants’ feedback on items was checked. An item was removed when at least two participants had substantial issues with it (e.g., it was not applicable or it was expressed differently than item described). This included further omitting 10 of 31 items. Third, item reduction was based on removing duplicate items. High inter-item correlations (r ≥ .50) along with high linguistic concurrence were therefore inspected (see Supplementary material, Table 2). To maintain a homogeneous set, the duplicate item that correlated least often above .30 with other items was removed. This included omitting item 7 (r = .78, with item 8), 10 (r = .54, with item 4), 12 (r = .61, with item 8), and 20 (r = -.50, with item 14). Finally, item 24 was the only item with no correlation above .30 and was therefore also removed, leaving 16 items for further analyses.
Measures for construct validity
Subjective well-being
To test associations expected based on SDT, well-being as perceived by parents was assessed with the Dutch translation (Maes et al., 2016) of the Mood, Interest and Pleasure Questionnaire (MIPQ; Ross & Oliver, 2003). The questionnaire contains 23 items on a 5-point Likert scale ranging from “never” to “always.” Each item had “not applicable” as additional response category. The total score reflected an overall indicator of positive mood. Specifically for persons with complex support needs, Petry et al. (2010) demonstrated evidence for construct validity, good internal consistency (i.e., Cronbach’s alphas between 0.84 and 0.94), and good test-retest and inter-rater reliabilities (i.e., above 0.86 and 0.69 respectively) for the subscales and total scale. Reliability scores for the total subjective Well-Being scale in the current study was 0.88 (i.e., good).
Quality-of-life in the communication and influence domain
Self-determination-related quality-of-life as perceived by parents was assessed using the Communication and Influence subscale of the Quality-of-Life of people with Profound Multiple Disabilities questionnaire (QOL-PMD; Petry et al., 2008). This 10-item subscale uses four response categories (i.e., agree, partly agree, disagree, and do not know). A higher score indicates better quality-of-life. A preliminary validation study of the overall QOL-PMD in persons with complex support needs showed promising construct validity and psychometric properties with a Cronbach’s alpha of 0.82 and item-remainder correlation of 0.51 for family informants on the subscale Communication and Influence (Petry et al., 2009b). In the current study, the reliability score was 0.87 (i.e., good).
Procedures
Ethical approval was obtained from the Scientific and Ethical Review Committee of the Faculty of Behavioural and Movement Sciences, Vrije Universiteit Amsterdam, The Netherlands (registration number: VCWE-2019-047). Recruitment was done through social media, newsletters, website posts, and word-of-mouth by support staff of several Dutch care and client advocacy organizations that support persons with disabilities and their caregivers. When all inclusion criteria were met and the researchers received the consent form, a telephonic appointment was planned for the administration of the BPN Signals questionnaire and other questionnaires not included in the current study. Prior to this appointment, participants had to fill in a battery of measures online, including information on demographic, additional characteristics, and the Autonomy-Supportive Experiences, Well-Being, and Quality-of-Life questionnaires. Due to the outbreak of the COVID-19 pandemic, data collection was temporarily paused. On resumption of the study, burden for the final 15 participants was reduced by only letting them complete the Autonomy-Supportive experiences, BPN Signals, and Quality-of-Life questionnaires.
Analysis strategy
All data were analysed using SPSS Statistics ((IBM Corp, 2020) Version 27). The first research question on the internal structure within this sample was answered using Principal Component Analyses (PCAs). The PCA method was chosen because it reduces the dimensionality of the data and is often used when the factor structure is unknown (Fokkema & Greiff, 2017). The first PCA for both questionnaires was done without rotation, after which the number of components (i.e., factors) was selected based on parsimonious descriptions given by eigenvalues above 1.00 or the scree plot point of inflexion (Cattell, 1966). All subsequent PCAs for solutions with more than one component were done with oblimin rotations and interpretability of components was assessed by strength of factor loadings. This process ended when the most unambiguous parsimonious solution had no more items loading below .30 on any component
The second research question on the internal consistencies of components was answered by computing Cronbach’s alpha. Specifically for a small sample size, internal consistency coefficients were considered sufficient (i.e., good or excellent) when these did not fall below 0.70 for scales with 6 or fewer items, below 0.75 for scales between 7 and 11 items, or below 0.80 for scales with 12 or more items (Ponterotto & Ruckdeschel, 2007).
The third research question on the construct validity of both new instruments was answered with bivariate correlation analysis, using Spearman’s rho for ordinal variables. Missing data within the Well-Being and Quality-of-Life in the Communication and Influence Domain questionnaires were imputed as per the instrument manual (Maes et al., 2016; Petry et al., 2008). Bivariate correlations were computed for all found constructs of the two new questionnaires with the Well-Being and Quality-of-Life questionnaires. Correlations above .20 were interpreted as supportive for construct validity (Swank & Mullen, 2017).
Results
Structure and validity of the parental perceptions on autonomy-supportive experiences questionnaire
Missing data and data pre-treatment
In total, 61 of 63 participants completed this questionnaire. One participant stopped due to the COVID-19 pandemic, the other withdrew without giving a reason and could no longer be reached. Examination of item descriptives (see Supplementary material, Table 3) in the sample of completed questionnaires (16 items x 61 respondents = 976 values) showed a total of 2 (0.2%) missing item values. These two missing values were completely at random (MCAR), as these were the result of a computer error. In addition, the percentage of missing data was well below 5%, justifying a replacement of the missing values by the item average in further analyses (Eekhout et al., 2013).
Internal structure and internal consistency
Final Pattern Matrix After Principal Component Analysis of the Parental Perceptions on Autonomy-Supportive Experiences Questionnaire.
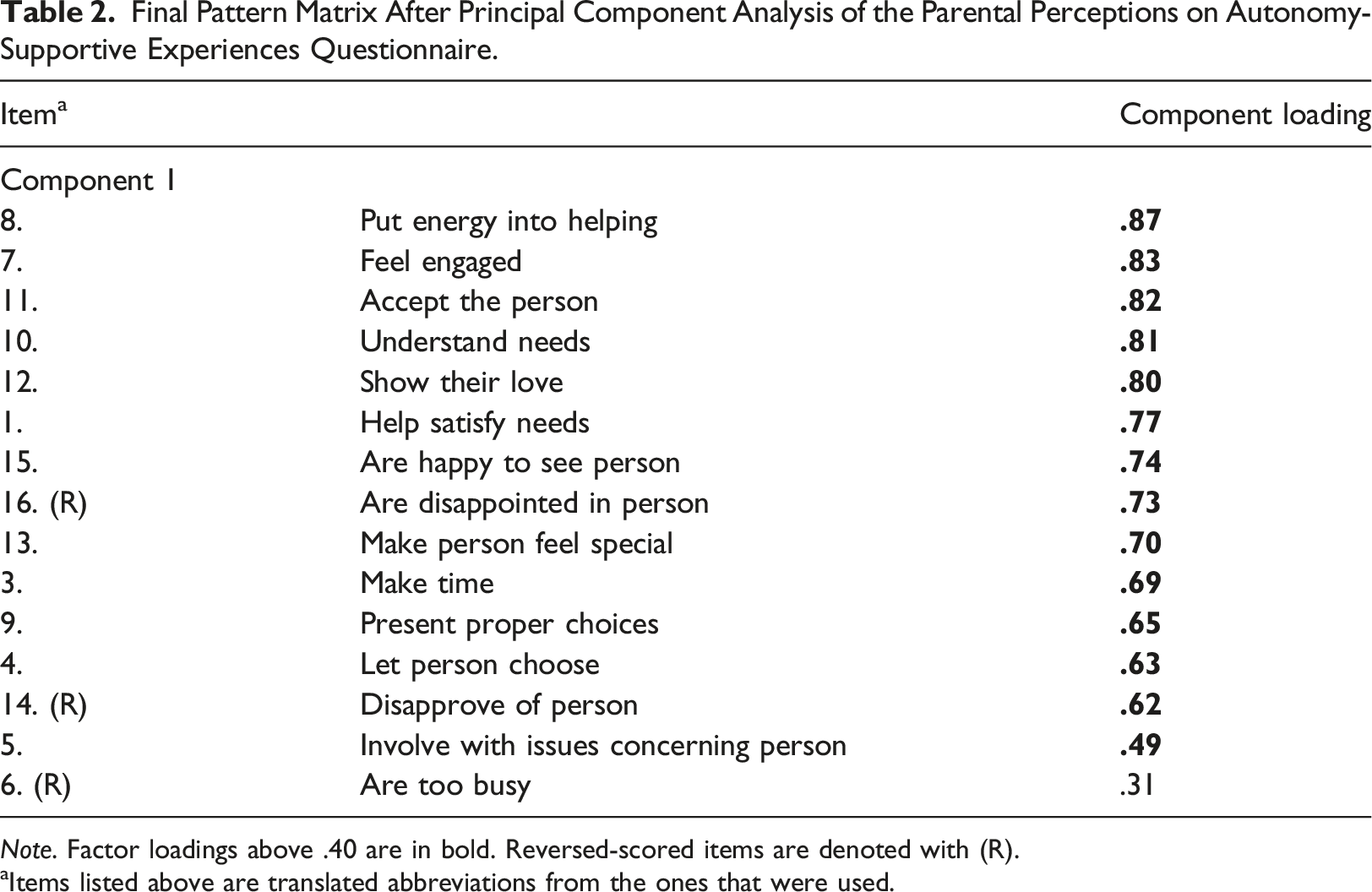
Note. Factor loadings above .40 are in bold. Reversed-scored items are denoted with (R).
aItems listed above are translated abbreviations from the ones that were used.
Construct validity
The association between Autonomy-Supportive Experiences and Well-Being was positive and statistically significant with Spearman’s rho being .34 (n = 41; p = .028). The association with the communication and influence subscale of Quality-of-Life was not statistically significant (n = 59; Spearman’s rho = .16, p = .22).
Structure and validity of the parental perceptions on basic psychological need signals questionnaire
Missing data and data pre-treatment
In total, 58 of 63 participants completed the BPN Signals questionnaire. One participant dropped out due to personal reasons unrelated to the study, two withdrew because of the COVID-19 pandemic, and the other two withdrew without giving a reason and could no longer be reached. Examination of item descriptives (see Supplementary material, Table 4) of the 16 items (i.e., 16 x 58 = 928 values) indicated a total of 2 (0.22%) missing item values. Further analyses were done with imputed values for these two missing values (Eekhout et al., 2015).
Internal structure and internal consistency
Final Pattern Matrix After Principal Component Analysis of the Parental Perceptions on Basic Psychological Need Signals Questionnaire.
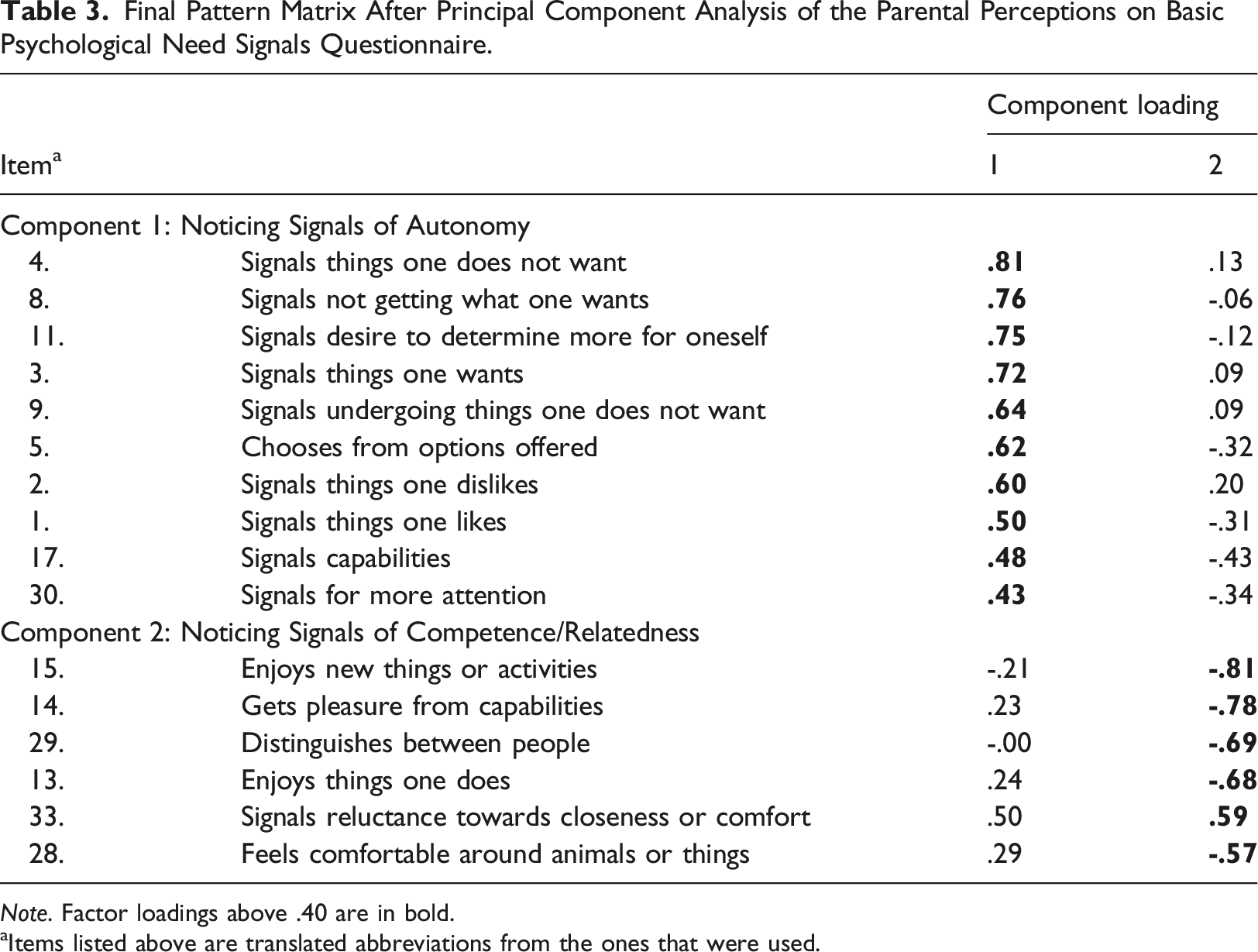
Note. Factor loadings above .40 are in bold.
aItems listed above are translated abbreviations from the ones that were used.
Construct validity
The associations between the two BPN Signals subscales and both Well-Being and Quality-of-Life were all statistically significant. The subscale interpreted as Noticing Signals of Autonomy correlated moderately with Well-Being (n = 37; Spearman’s rho = 0.36, p = .030) and strongly with Quality-of-Life (n = 54; Spearman’s rho = 0.64, p < .001). The subscale interpreted as Noticing Signals of Competence/Relatedness correlated strongly with Well-Being (n = 37; Spearman’s rho = 0.55, p < .001) and moderately with Quality-of-Life (n = 54; Spearman’s rho = 0.32, p = .018).
Discussion
In this study, two parent-informant questionnaires were developed, one about autonomy-supportive experiences by their child with complex support needs and one about noticing signals that reflect BPNs in this target population. Regarding the first research question, the most unambiguous and parsimonious structure for the 15 remaining items of the Autonomy-Supportive experiences questionnaire was a one-dimensional model. Although the Autonomy-Supportive experiences items were derived from the three subscales of the POPS questionnaire (i.e., Autonomy Support, Involvement, Warmth), these subscales could not be distinguished as separate factors in the PCA. Setting aside the limited sample size, the limited set of items that were deemed applicable and the extent of their revisions may have obscured finer nuances in ways in which carers may support autonomy in persons with complex support needs. It may also indicate that the various aspects of autonomy support are highly integrated in interactions with persons with more complex support needs. This corresponds to the complex process of understanding and supporting the needs of people with complex support needs as described by Van Tuyll van Serooskerken et al. (2022). However, without directly testing the variance in the structure of the new Autonomy-Supportive experiences questionnaire across populations, this remains speculative.
The 16 remaining items of the BPN Signals questionnaire fell alongside two dimensions. One component reflected noticing signals of autonomy and the other reflected noticing signals of both competence and relatedness. These components encompassed the extent to which caregivers noticed need expressions (e.g., signals things one wants), manifestations of need-related behaviours (e.g., chooses from options offered), and expressions of need satisfaction (e.g., enjoys things one does). However, this degree of at least noticing needs and need fulfillment is a necessary but not sufficient condition to actually guarantee effective support and satisfaction of BPNs.
Because virtually no frustration-related items of competence and relatedness resulted from the item construction and social validation stage, those constructs also did not emerge in the final item set. Negative affective states in persons with complex care needs have been found to be expressed in a more diffuse and sometimes paradoxical way compared to positive states and to people without disabilities (Vos et al., 2013a; Vos et al., 2013b). This aligns with the difficulties we encountered when attempting to create a proxy questionnaire based on the BPNSFS-ID (Frielink et al., 2019). It must be noted, also, that the validity of the basic psychological needs frustration scale has recently come under scrutiny and may need to be reconceptualized (Murphy et al., 2023). Yet, due to the small sample size, the results should be interpreted with caution. Conclusions about the structure found therefore only concern this sample for the time being. Nevertheless, being able to detect and interpret BPN signals of persons with complex support needs is an important step in creating effective possibilities for self-determination (Van Tuyll van Serooskerken et al., 2022).
The internal consistency coefficients for the Autonomy-Supportive experiences questionnaire and the BPN Signals questionnaire were considered sufficient as the lowest alpha was 0.78. Furthermore, the medium to large correlations between the two questionnaires and Well-Being and Quality-of-Life are a first indication of construct validity and applicability of the BPNT and SDT in persons with complex support needs (Deci & Ryan, 2000; Soenens et al., 2007), and point to their potential contribution to understanding the mechanisms that link self-determination to quality of life (Mumbardo-Adam et al., 2023). The strong correlation between the factor interpreted as Noticing Signals of Autonomy and self-determination-related quality-of-life might indicate that parents’ attentiveness towards signs of, for example, preferences and volition is related to the ability of persons with complex support needs to influence their environment (Mumbardo-Adam et al., 2023). The strong correlation between the factor interpreted as Noticing Signals of Competence/Relatedness and well-being might indicate that parents’ attentiveness towards signals of, for example, experiencing activities and comfort with regard to others is related to the positive mood of persons with complex support needs. An unexpected finding was the absence of a statistically significant association between autonomy-supportive experiences and self-determination-related quality-of-life, which is often found in typically developing persons (Ryan et al., 2008). A possible explanation for this absence might be that there is no direct but indirect relationship between the two concepts. Frielink et al. (2018), for example, showed that the link between autonomy support and health-related quality-of-life was mediated by BPN satisfaction. Another explanation might be that because the Autonomy-Supportive experiences questionnaire does not distinguish between different aspects of autonomy support, associations with the more specific concept of Communication and Influence domain of quality-of-life may have been attenuated. It is also possible that the association between autonomy support and self-determination-related quality-of-life manifests itself differently within this target group compared to persons without (severe) disabilities. Further research is warranted into the association between autonomy-supportive experiences and other Quality-of-Life domains such as personal development, activities, social relationships, physical health, and material well-being (Flanagan, 1978; Petry et al., 2009a).
Limitations and future research
In line with other research on this population (Maes et al., 2021), given the low prevalence and the demands of their time which were compounded by the COVID pandemic, the sample size was small for factor analytic work. While any factor analytic work requires cross-validation, solutions based on small samples may need to be considered extra carefully and might not reveal finer nuances in the conceptual space covered by these instruments.
Options to increase sample sizes for studies such as the current one include collaborating with relatives in the initiation of research and building of research infrastructure. This may take the form of registries where parents voluntarily enroll for scientific research (e.g., Conners et al., 2014). Another option is to increase national and international coordination and collaboration, for example using harmonized measures or minimal datasets and by asking participants for permission to share their data with other researchers (Maes et al., 2021; Ras et al., 2020).
Response set such as social desirability bias (Paulhus, 2002; 2017) may also act as a confounder. Although Autonomy-supportive experiences items concerned the support from all key partners in the environment, the extent of the participants’ own role was not clear. It is possible that participants who mainly related the items to themselves filled out the questionnaire differently than participants who included other key partners in their evaluation.
An important limitation is that parents’ perceptions cannot be equated with the thoughts and experiences of the persons with complex support needs themselves. Although Embregts et al. (2019) showed that family members were able to differentiate between their own perspectives and that of the person with complex support needs, Olsman et al. (2021) argued that key individuals in the environment of persons with complex support needs are not assessors but witnesses who, when they share experiences and knowledge about the person, should constantly remain critical and receptive.
Conclusion and implications for practice
In the current study, two questionnaires were developed and tested to measure parent-perceived autonomy-supportive experiences and BPN signals in persons with complex support needs. Both questionnaires appeared internally consistent and showed the expected associations with other constructs in the nomological network around self-determination. Although further research is needed, the development and preliminary evaluation of these questionnaires is a first step in understanding the processes of autonomy support and BPN satisfaction, which may ultimately increase the understanding of self-determination in this group (Kuld et al., 2023; Mumbardo-Adam et al., 2023). In addition to the potential empirical value of psychometric tools, questionnaires aimed at parents and other caregivers may also contribute to the introspection and reflective skills of the informant, which might indirectly benefit the person of interest. Subsequently, the questionnaires could contribute to a shared frame of reference between parents and healthcare professionals if these also prove to be valid for support staff. In turn, a shared frame of reference will ensure that their support from both sides becomes complementary and more effective. Ultimately, this will improve the quality-of-life of individuals with complex support needs.
Supplemental Material
Supplemental Material - Parent-perceived autonomy-supportive experiences and basic psychological needs of people with complex support needs: Development and preliminary psychometric evaluation of two questionnaires
Supplemental Material for Parent-perceived autonomy-supportive experiences and basic psychological needs of people with complex support needs: Development and preliminary psychometric evaluation of two questionnaires by Jacqueline M van Tuyll van Serooskerken, Agnes M Willemen, Petri JCM Embregts and Carlo Schuengel in Journal of Intellectual Disabilities
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to the parents and relatives who took the time and effort to participate in this study. Furthermore, the authors would like to thank the care and client advocacy organizations ’s Heeren Loo, EMB Nederland, and Per Saldo sincerely for their support with recruitment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Netherlands Organisation for Health Research and Development (ZonMw) Nationaal Programma Gewoon Bijzonder under Grant number 845004005; Partial funding (i.e., co-financing) for this research was provided by Stichting Wetenschappelijk Onderzoek ’s Heeren Loo, The Netherlands.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.