
Abstract
A growing body of evidence has attested to the higher impact of COVID-19 on individuals with intellectual disabilities (IDs) than on members of the general population during the pandemic, mainly showing their higher vulnerability. However, we believe it is important to better understand how their situation interacts with the specific circumstances of the pandemic. In this article we discuss recent findings regarding individuals with IDs through the lens of two theories – the social disability model and the ecological model of trauma and recovery – and propose an integration, namely a social model of disability in crisis and trauma situations. Such a model allows for a wider perspective on understanding the way people living with disabilities (PLWDs) cope in these situations, integrating the individual aspects of coping with the social and environmental ones.
Keywords
Introduction
The novel coronavirus (or SARS-Co-V-2, the virus that causes COVID-19) pandemic has caused unprecedented global public health and economic crisis since its onset in late 2019. The uneven impacts on regions and communities across the globe have revealed stark disparities across race, income, gender, health status, and disability (WHO, 2022). People living with disabilities (PLWDs) comprise one group whose multiple health, social, and employment vulnerabilities are high even during routine times, and these vulnerabilities lowered their capacity to cope with the challenges presented by COVID-19 as well as their access to health services. Indeed, recent research has demonstrated the negative effects of the COVID-19 pandemic and lockdowns on the health and mental well-being of this population (Jesus et al., 2021; Kamalakannan et al., 2021; Wang et al., 2022).
Though of concern to all PLWDs, COVID-19 appears to present a particular risk to individuals with intellectual disabilities (IDs). The definition of intellectual disability (ID) has evolved over the past century, with consensus in the scientific and practice communities around a framework that includes two critical elements - significantly lower than average cognitive functioning (information processing and reasoning skills), and challenges in everyday activities in home, school, community, and employment environments (the navigation of day-to-day life) (Fidler & Lanfranchi, 2022).
Individuals with IDs tend to have high rates of physical disorders (Perera et al., 2019), show significantly lower levels of physical activity than the general population in respect to all consequences for health (Nutsch et al., 2022), and a higher prevalence of specific comorbidities associated with poorer COVID-19 outcomes than do individuals without IDs (Turk et al., 2020).
Individuals with IDs were also found to be more vulnerable to the emotional and occupational effects of the pandemic than were members of the general population (Rose et al., 2020). These individuals often live in communal settings such as group homes, where the risk of virus transmission is elevated (Landes et al., 2021), resulting in higher rates of infection (Mills et al., 2020) and severe disease. COVID-19 case-fatality rates were significantly higher among individuals with IDs than among others (Gleason et al., 2021; Mark et al., 2020). In addition, distinct age-related differences in case-fatality were found between individuals with and without IDs, with the highest difference being found among young adults (Turk et al., 2020).
Although these studies indeed demonstrated that the health risks of individuals with IDs intensified during the COVID-19 pandemic, we believe it is important to better understand how their situation interacted with the specific circumstances of the pandemic. In this article we discuss the recent findings regarding individuals with IDs through the lens of two theories – the social disability model (Oliver, 2004) and the ecological model of trauma and recovery (Harvey, 1996; Harvey et al., 2003) – and propose an integrated model, namely a “social model of disability in crisis and trauma situations.” The model allows a wider perspective on understanding the coping of PLWDs in these situations, integrating the individual aspects of coping with the social and environmental ones. For this purpose, we attempted to focus primarily on research regarding individuals with IDs, although many studies have used mixed samples of PLWDs.
The social model of disability and the COVID-19 pandemic among individuals with IDs
The social model of disability (Oliver, 2004) emphasizes the role of environmental and societal factors in its construct of disability (Shakespeare & Watson, 2001). In accordance with the Fundamental Principles of Disability document (UPIAS 1976), people are not disabled by their impairments but by the disabling barriers they face in society. This perspective lies in contrast to the medical model of disability which considers people to have a disability based on a health condition that limits their ability to carry out expected individual and social obligations (Harris, 2006).
The social model of disability is well reflected in recent reviews emphasizing the centrality of the environment in PLWDs’ coping with the effects of COVID-19 on their interactions with the social environment and on their employment. It has been argued that societal barriers intensified PLWDs’ vulnerabilities (Kamalakannan et al., 2021), and the lack of disability-inclusive responses and emergency preparedness targeted toward PLWDs exacerbated their vulnerabilities (Jesus et al., 2021). For example, for individuals with IDs, the inconsistent/inaccessible public health messaging (Gleason et al., 2021) and the vast amount of COVID-19-related information and disinformation caused social barriers, confusion, and stress: issues that did not receive sufficient recognition in COVID-19 policies (Lake et al., 2021). Preventive measures, such as “social distancing,” hygiene practices, and self-isolation, were clearly more challenging for individuals with IDs than for others. The total dependence of individuals with IDs on their sources of assistance meant that they could not in fact honor social distancing messages; social distancing was not an option for them, and the sudden avoidance of physical interaction was difficult for them.
The lack of targeted communication about these measures and their importance in preventing severe health consequences is consistent with evidence regarding not involving individuals with IDs in sensitive health situations, such as in matters of dying and death (Cithambaram et al., 2019), and in their exclusion from advance-care planning and decision-making (Voss et al., 2019). This state of affairs may have arisen for various reasons, among them insufficient knowledge of and awareness about disabilities among healthcare professionals (Liasidou & Mavrou, 2017). These social environmental barriers have contributed, at least in part, to the higher comorbidity among individuals with IDs compared to those without IDs and to a higher case-fatality rate of COVID-19 among those under 75 years of age (Turk et al., 2020).
Understanding the role of the environment in the life of people with IDs in accordance with the social model of disability would have been helpful in providing them access to public health messages about COVID-19. For example, disseminating messages that used easy-to-understand language across accessible formats and/or the wearing of transparent masks by healthcare providers may have removed barriers and allowed caregivers and family members to continue supporting individuals with IDs. These efforts may have helped individuals with IDs to maintain their routines while simultaneously allowing them to adhere to the required changes in living with COVID-19.
Employment – another important aspect of interacting with the environment – provides individuals with IDs emotional security in everyday life through structure, a sense of belonging, achievement, and a sense of safety through predictability (Scheffers et al., 2020). Although COVID-19 disrupted work and employment opportunities for everyone, it is reasonable to assume that, in accordance with the social model of disability, these effects were particularly severe for individuals with IDs, as many of them were likely in vulnerable employment situations without adequate social protections (Embregts et al., 2020). Yet a more recent report from the U.S. (Ne’eman & Maestas, 2022) suggests otherwise. Employment rates declined significantly in the second quarter of 2020, but PLWDs had similar employment losses compared to their non-disabled counterparts. After the pandemic, PLWDs experienced faster employment growth, reaching pre-pandemic levels before their non-disabled counterparts did, and then exceeding them by 2022. This trend was driven mainly by those employed in teleworkable, essential, non-frontline occupations. It may be that because PLWDs have long been more likely to find employment in teleworkable jobs, the pandemic-induced shift to telework created new employment opportunities for them (Ne’eman & Maestas, 2022). The report does not provide data by type of disability; yet it is reasonable to assume that those with IDs did not benefit from such employment gains. Unfortunately, unlike the evidence regarding the physical and mental health consequences of COVID-19, the employment situation of individuals with IDs has not been sufficiently researched in the context of the pandemic, despite its importance and tremendous impact.
This lacuna in the research reflects a perspective that aligns with the medical model of disability and illustrates a lack of consideration for the effect of the social environment on the lives of individuals with IDs.
These two important aspects of interacting with the environment illustrate the existing gaps between the requisite application of the social model of disability in health-related policy, and the actual prevention messages, gaps that were significantly exacerbated during the COVID-19 pandemic. Additionally, coping with the pandemic was further complicated for individuals with IDs because of the pandemic’s potential to become a traumatic experience.
The ecological model of trauma and recovery and COVID-19 among individuals with IDs
According to the ecological model of trauma and recovery, the person, the event, and the environment all interact in the development of a wide range of different individual reactions to violent and traumatic events (Harvey, 1996). Regarding the person, we must take into consideration the individual’s coping capacities, as well as the history of this person’s coping with prior trauma. Regarding the event, one must take into account the frequency, severity, and duration of the violent and/or traumatic events, and the resultant subjective perceptions of fear and terror experienced by the individual. Lastly, the degree of community support, both during and after exposure to violent and traumatic threats, is significant (Harvey, 1996; Harvey et al., 2003). Thus, the ecological model of trauma and recovery suggests that resilience and coping are transactional consequences of the complex relationships between individuals and their environment, their communities.
The COVID-19 pandemic could be seen as a traumatic event, given the acute and chronic threats it has posed (Sanchez-Gomez et al., 2021). Criterion A of the DSM-5 (the event criterion) and the four clusters of post-trauma symptoms and functioning (Criteria B, C, D, and E) all align with the recognition of COVID-19 as a traumatic event (Gouzman, Soskolne & Dekel, 2022). In other words, COVID-19 comprises exposure to actual or threatened death, and evidence of post-traumatic stress disorder (PTSD) reactions has already accumulated. Prevalence rates ranging from 7% to 53.8% in the general population in several countries (Xiong et al., 2020), and relatively high PTSD symptomatology has been found worldwide in young adults (Liu et al., 2020) and among COVID-19 survivors (Bo et al., 2021).
There is growing evidence that adults with IDs are more vulnerable to traumatic experiences and abuse than are members of the general population (Beadle-Brown et al., 2010; Nixon et al., 2017), resulting in PTSD and trauma-related disorders (Wigham & Emerson, 2015). Though exact prevalence rates are difficult to estimate due to the differing criteria used, biased sampling, and the use of case note reviews to determine disability and traumatic incidents (Byrne, 2022), research suggests that rates of developing mental health difficulties are two to four times higher among adults with IDs than among individuals with no IDs (Cooper et al., 2007; Einfeld et al., 2011). Additionally, studies among individuals with IDs have shown that more severe and significant psychological distress is associated with multiple trauma exposure in childhood and adulthood in contrast to trauma that is only experienced in adulthood (Mason-Roberts et al., 2018).
The impact of diverse and potentially traumatic events, such as institutionalization and early separation from caregivers (Tomasulo & Razza, 2007), or abuse by perpetrators specifically targeting individuals with IDs because of their known difficulties in communication (Byrne, 2018), has been well-documented. The numerous COVID-19-related challenges for individuals with IDs introduced unique potential sources of trauma and stress within the disability community, including concerns about healthcare rationing and ableism in health care, isolation, and the deaths and illnesses of loved ones and community members (Lund et al., 2020). Psychiatrists treating individuals with IDs reported a rise in requests for psychotropic medications (Courtenay, 2020), and caregivers of individuals with IDs reported increases in depression/anxiety, stereotyped behaviors, aggression toward others, and weight gain in the individuals they cared for (Linehan et al., 2022). Of particular importance are studies that demonstrated the broad impact of the pandemic and its implications for the mental states of people with IDs (Lund et al., 2020) and those showing that social isolation as well as stigma and worries about COVID-19 are the strongest predictor of depression and anxiety, (Wang et al., 2022). These findings underline the importance of understanding the centrality of the environment in the coping of this population and the need to address systemic and institutional ableism and how this ableism intersects with other forms of oppression (Lund et al., 2020).
In our view, there were insufficient levels of inquiry during the COVID-19 pandemic regarding the third crucial factor of the ecological model of trauma and recovery (Harvey, 1996), “the degree of community support, both during and after exposure to violent and traumatic threats” (Harvey, 1996; Harvey et al., 2003). It is evident that many countries’ policies during the pandemic aligned with the medical model of disability, separating and segregating from the general population individuals with IDs – those who are already more vulnerable to the effects of trauma – and increasing their risk of developing PTSD.
Integrating the models: A social model of disability in crisis and trauma situations
The evidence showing that individuals with IDs are more vulnerable than others to the health, emotional, and occupational effects of the COVID-19 pandemic highlight the important role played by environmental factors. As such, it points to the wisdom of viewing this population by employing a perspective that integrates both the social model of disability and the ecological model of trauma. During emergency times, the socio-structural barriers that lead to exclusion and limit individuals with disabilities from participating in society can be particularly daunting. Among them are the lack of adapted communication about prevention and care, the abrupt changes in routine and in employment, and the barriers in accessing community support.
Moreover, both of the abovementioned models emphasize the fact that individuals’ reactions to the event depend on their subjective cognitive perceptions of their situation, a crucial factor in initiating efforts to cope with said situation (Lazarus & Folkman, 1984). In both models the individual's perception of time-related factors (i.e., temporary/permanent disability, duration/severity/frequency of trauma), other characteristics of the situation, the available resources and potential outcome is critical. Society can help people with disabilities integrate by focusing on their healthy aspects rather than by focusing on their disabilities, reducing barriers and/or PTSD by offering meaningful support. The social model of disability emphasizes the interaction between the individual and the environment. At times of major crisis and trauma, the ecological model of trauma and recovery may elaborate this perspective as it suggests that resilience and coping are transactional consequences of the complex relationships between individuals and their communities. Inserting the pre-existing sociocultural barriers into the ecological model of trauma allows us to obtain a triple interaction that reflects the environment and sources of support post-event. As such, in integrating these two models, we propose a social model of disability in crisis and trauma situations, which may shed light on understanding the coping of PLWDs, integrating the individual parts of coping with the social and environmental ones. (Figure 1) A social model of disability in crisis and trauma situations.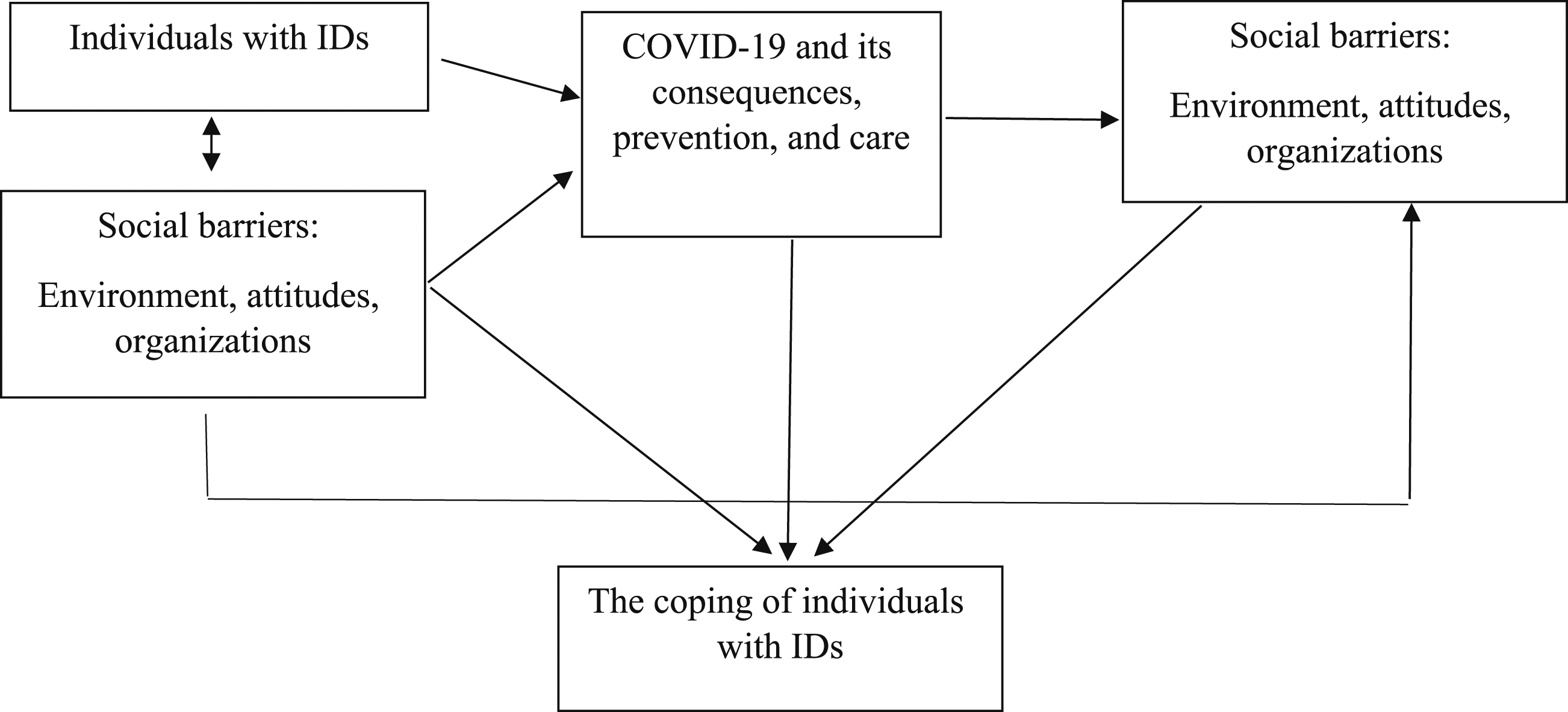
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.