
Abstract
Sexual health education among adolescents with intellectual disabilities is an area of concern among parents and educators. Special educators play a vital role in teaching sexual health and safety to their students with disabilities. The present study explores special educators' concerns in teaching sexual health among adolescents with intellectual disabilities. The participants included 35 special educators working with adolescents with intellectual disabilities in India. Summative content analysis of the data collected using a semi-structured interview schedule highlights the neglect of the issues related to sexual health among adolescents with disabilities. Special educators reported the challenges in providing sexual health education. Teachers lacked skills in imparting sexual health education. Developmentally and culturally appropriate sexual health education can help adolescents with a disability learn healthy life skills. The paper emphasizes the need for professional support and training among special educators on sexual health education.
Keywords
Special educators and sexual health education
According to the World Health Organization (WHO) report on disability (2011), 15 percent of the world population has some disability. In India, there are 2.2 percent of people have a disability as per the census of 2011 (Moger et al., 2015). Children with disabilities are vulnerable and at high risk of physical and emotional abuse (McDaniels and Fleming, 2016). Likewise, lack of sex education affects their sexual well-being and safety. It places adolescents with intellectual disabilities (moderate and severe) at risk of exposure to sexual exploitation, abuse, and unwanted pregnancy (Treacy et al., 2018). In contrast, the emphasis on sexual health education for children with special needs is minimal (Holland-Hall and Quint, 2017). The social model of disability states that people are disadvantaged, not due to their impairments but due to their limitations by social, cultural, economic, and environmental barriers (Oliver, 2013). Myths and misconceptions lead parents and society to deny the right to sex education (Finley et al., 2014). Comprehensive sexual education programs are hindered by false beliefs that, for example, children with intellectual disability are asexual and that sex education might cause them to act in sexually inappropriate ways, making it impossible to determine their requirements in this area (Gonzálvez et al., 2018).
With professional training, special educators show a comparatively higher positive attitude towards sex education for children with special needs than their parents (McDaniels and Fleming 2016). However, imparting sex education knowledge to children with special needs can be challenging. Educators have reported a lack of comfort, confidence, and skills to deliver sex education to a vulnerable population (Treacy et al., 2018). Professionals who work with children with disabilities may feel inadequate and hesitant to teach due to personal, religious, or cultural beliefs. They fear these beliefs would conflict with the actual implementation of sex education programs (Lafferty et al., 2012).
Training has a significant influence on teachers' feelings of self-competence (McDaniels and Fleming, 2016). A supportive and empathetic workplace with visionary leadership, chances for personal development, and a healthy balance between work and home life all contribute to improved job performance and happiness (Sharma et al., 2012). On the other hand, special educators who feel overburdened and unsupported would have less motivation to work in such an environment, which prevents them from adopting new teaching methods and being open to learning (Treacy et al., 2018). Facilitators who work with people with disabilities communicate their understanding of sexual health, prevent sexual abuse, normalize sex education, and enhance the quality of life (Barnard-Brak et al., 2014). In addition to these barriers, the lack of emphasis on the sexual and reproductive rights of persons with disabilities in the existing laws has made them vulnerable (Gupta & Aggarwal, 2012).
Vulnerability to sexual abuse
According to McDaniels and Fleming (2016), Children with special needs are at a higher risk of sexual abuse than their peers without special needs. Adolescents with intellectual disability were as vulnerable as children with special needs. Educators need to focus on two significant areas of sexual abuse among students with disabilities. The first is that adolescents with disabilities are more vulnerable to becoming victims of sexual abuse which may be due to their lack of knowledge about sexual abuse. Second, despite engaging in behaviours that may not have any sexual motivation, they may be classified as offenders or perpetrators (Ballan, 2012). This propels an immediate need to clarify misperceptions (Gonzálvez et al., 2018). Accepting the sexual behaviour of adolescents with intellectual disabilities helps remove the stigma related to disability and sexuality.
Comprehensive and data-driven sex education programs are found to reduce deviant behaviour or inappropriate sexual behaviour (Holland-Hall and Quint, 2017). Parents of adolescents with disabilities strongly emphasize that they need professional guidance from educators rather than relying on unauthentic sources (Ballan, 2012). Educating people with disabilities will help them communicate more clearly about abuse or assault and express their rights (Badjena, 2014). Educators advocate for the rights of their students; thus, empowering the educators becomes more significant in preventing the sexual abuse of students with intellectual disabilities.
Sexually abused students are more likely to engage in maladaptive sexual behaviours, attempt suicide, or engage in self-injurious behaviours (Jones et al., 2012). Adolescents with intellectual disabilities have a lack of awareness about sexual health, intercourse, reproduction, and the variations between male and female reproductive organs, which is exacerbated by a lack of education about sexual and reproductive health (McDaniels and Fleming, 2016). Despite being a significant concern, the importance of sexual development and sex education for children with special needs is ignored to a larger extent (Gonzálvez et al., 2018). Neglecting the need for developmentally appropriate sex education would lead to the ignorance and exploitation of children with special needs.
Concerns of caregivers
The caregivers in the family and the professionals who work with children with special needs strongly support sex education and emphasize the importance of contraception (Holland-Hall and Quint, 2017). However, parents of children with special needs lack knowledge on educating their children about sexual health and well-being (Treacy et al., 2018). Often parents are not psycho-educated to understand the sexual life of their children to an adequate level. Therefore, it is necessary to educate parents about sexual development and the importance of sex education for children with intellectual disabilities (Medina-Rico et al., 2018).
Parents and educators of children with mild intellectual disabilities reported taking responsibility for their children’s sexuality. However, sometimes youngsters tend to develop sexually inappropriate behaviour from their environment. Parents and educators take the responsibility of taking decisive disciplinary actions against inappropriate sexual behaviour. (Stoffelen et al., 2013). As a result, the prevalence of adolescents expressing sexually harmful behaviour is high. Proper intervention and attention at an early stage facilitate a preventive measure of sexual abuse (Banks, 2014).
Sex education for children and adolescents with special needs
In earlier years, sexuality and sexual health education were not given importance. The current decade gives importance to sex education; but, the quality of training and content of sex education is not adequate. Special educators reported a lack of knowledge, skills, and practical exposure to impart sex education (Borawska-Charko et al., 2017; Gonzálvez et al., 2018). On the other hand, they nurture a positive attitude towards sex education and consider sexuality a fundamental human right (Gonzálvez et al., 2018). Sex education provides insight into the importance of consent, and proper understanding of sexual activity to adolescents with intellectual disabilities. When considering sexual health issues, male students' sexual health and hygiene are neglected. Male students were perceived to exhibit inappropriate sexual behaviour compared to females (Medina-Rico et al., 2018).
Research emphasizes the importance of sex education and the need to increase the competency of special educators to deliver sex education to children with intellectual disabilities (Schaafsma et al., 2015). However, sex education for children with special needs should use a more data-driven approach. The sex education curriculum must be prepared based on the child’s understanding, kind, and needs based on the disability. This could facilitate a proper and clear perspective of sexual health and education for children with special needs (Schaafsma et al., 2015).
The prejudice of families, caregivers, and educators regarding sex and sexuality is a major stumbling block in imparting sexual health education (Gireesan et al., 2013). The attitude, unpreparedness, and conforming social taboos by professionals and family members affect the possibility of adolescents with special needs exploring their sexuality and getting the proper sex education (Tamas et al., 2019). When sex education is imparted successfully to assist people with intellectual disabilities, it creates awareness and paves a pathway to leading a healthy sex life. But there were limitations in imparting sex education, such as verifying the effect of imparted knowledge on long-term behavioural change and reducing unhealthy sexual lifestyles (McCann et al., 2019). To reduce sexual abuse, professionals and parents should understand the importance of sexual health education. Furthermore, sexual health education should aim at promoting an inclusive and positive attitude towards sexual health, exploration of sexual orientation, intimacy, and romantic relationships (Murray, 2019).
Present study
The current study examines the perspective of sexual health education and the challenges faced by special educators in imparting the same to adolescents with intellectual disabilities. Exploring the factors that hinder effective sexual education, health, and safety of adolescents with intellectual disabilities is essential (Wilkinson et al., 2015). There is a need for sexual health education among adolescents with intellectual disabilities to help in expressing themselves. Sexuality and sexual health issues among adolescents with disabilities need attention (Holland-Hall and Quint, 2017). Well-planned sex education provides insight into sexual health and prevents sexual abuse to an extent as there is increased importance among the academicians to provide sex education to facilitate their students. Sex education prevents the sexual exploitation of adolescents with intellectual disabilities (McCann et al., 2019). Misconceptions held by family members and society become a challenge for special educators.
Research questions
1. What are the views of special educators on sexual health and safety education for adolescents with intellectual disabilities? 2. What challenges do special educators face in imparting sexual health education among adolescents with intellectual disabilities?
Method
Research design
Qualitative descriptive research design aims to acquire information and insight into special educators' views and challenges while imparting sexual health and safety education to adolescents with intellectual disabilities. Qualitative descriptive research does not give any relations between the variables but gathers information from the participants from observation and experience (Nassaji, 2015). In this study, the researchers familiarised themselves with the necessary information, such as special educators' perspectives about the available resources and challenges they face in imparting sexual health education to adolescents with intellectual disabilities by using an exploratory design. In addition, it facilitated a general understanding of the current scenario on knowledge of special educators on sexual health and their ability in handling sexual health education and concerns they face (Neuman, 2014).
Participants
The sample included 35 special educators who consented to participate in the study. The sample included four males and 31 female special educators from Coimbatore, Tamil Nadu, India. The age of the participants ranged from 24 to 40 years, with an average age of 33 years. All the participants had a Bachelor’s degree in special education, recognized by the Rehabilitation Council of India (RCI). All participants worked in a special school with work experience ranging from 2 years to 10 years, and the average work experience was 7 years. Purposive sampling was used in the study to help the researcher decide which individuals would best provide the desired information. Purposive sampling techniques facilitated the researcher in identifying experts (Sharma, 2017) in the field of intellectual disabilities and thus facilitate gathering the information from the experts.
Operational definition
The Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM–5; DSM-5 American Psychiatric Association, 2013) defines the term intellectual disability as a developmental condition in which the person shows deficits in intellectual functioning and adaptive behaviour such as understanding concepts and has difficulty with social and practical skills.
Research tool
A semi-structured interview schedule allows the researcher to use probing questions and clarify the participants' answers within the constructed frame (Kallio et al., 2016). The extensive literature review facilitated identifying the broad questions in the interview schedule.
Validation process of the semi-structured interview schedule
The semi-structured interview schedule was developed based on a literature review. Two psychologists with over 5 years of research experience, and a special educator with 3 years of work experience with adolescents with intellectual disabilities, validated the interview schedule. The experts were asked to ‘accept, modify or reject questions in the interview schedule and provide feedback on the items. The interview schedule was modified based on the comments from the experts. The reviewed and finalized interview schedule consisted of 20 questions such as ‘Do you think the students should be given sex education?’ and ‘What are a few steps that you can take to help your students understand exploitation or abuse?’ A few close-ended questions were followed by the probing questions, which explains their response to the close-ended questions. For example, ‘Have you given any information to the students regarding how to prevent abuse?’ and the close-ended question was followed by probing questions such as ‘What are the preventive measures that can be taken to avoid sexual abuse?’ A pilot interview was conducted with one special educator to verify the congruency of the interview schedule with the objective before finalizing.
Data collection procedure
All procedures performed in studies followed the ethical standards as per the institutional ethics review board and followed the 1964 Helsinki declaration. The researcher explained the nature and purpose of the research to each participant. The participants were upraised about their rights. The participants had the right to withdraw from the study at any point they wished, and it was voluntary. The place and time for the interview were decided based on the convenience of the participants. Each interview lasted for approximately 30–45 min. All interviews were audio-recorded with the consent of the participant. Pseudo acronyms were assigned to each participant to ensure confidentiality. The interview data was saved on the password-protected hard disk, which the researchers could access only.
Data analysis
The data was transcribed, and the steps recommended by Braun and Clarke (2019) mentioned below were used to conduct the reflexive thematic analysis. The thematic analysis provides flexibility, a detailed account of data, and an accessible form of analysis that facilitates understanding of the different participants’ perceptions of similarities and dissimilarities, leading to unexpected insights (Braun and Clarke, 2019; Nowell et al., 2017). Step one was getting familiar with the transcripts through reading and re-reading them. Step two was to form initial codes by identifying the critical information shared by the participants with the help of lines of enquiry. Step three was to identify the themes using codes identifying themes. Step four was to review and re-analyze the identified themes to check if it was congruent with the research objective. Step five was to define the identified themes and name them as per the research objectives. Finally, step six was to frame reports with the help of analyzed themes and lines of enquiry (Braun and Clarke, 2006; Nowell et al., 2017). Based on Gibb’s recommendation in 2007, pragmatic validity was used in the study to see the impact of research findings. Member checks were done with participants to verify the validity of the results (as cited in Creswell, 2011).
Results
Organizing themes and basic theme of special educators’ perspective on sexual health among adolescents with intellectual disability.
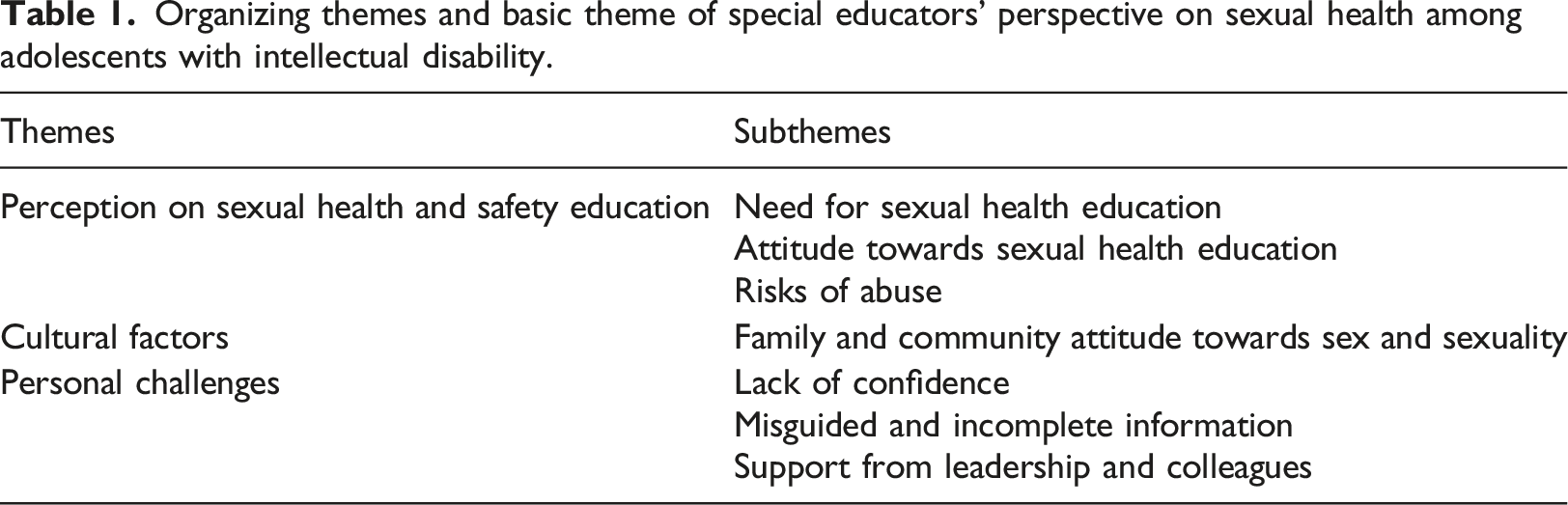
Theme 1: Perception of sexual health and safety education
Participant special educators' opinion about sexual health education and their training plays a significant role in their attitude towards the same. Special educators believe that sexual health education helps prevent sexual abuse.
Subtheme: Need for sexual health education
Special educators shared their views on implementing sexual health education. Most participants believed that information on sexual health is not available to students irrespective of their disabilities. The prevalent preconceived assumption was that sex education was irrelevant since an adolescent with an intellectual disability would not grasp the content and would impede the process of transferring information. Their ability to understand such skills is significantly less. We assume they don’t understand though they can be taught to a certain extent. Some teachers may have a notion like ‘any way they won’t be able to understand; then why would I try doing it? (Participant 18, Female special educator)
Subtheme: Attitude towards sexual health education
Special educators expressed the need to impart sexual health awareness among students to prevent them from being abused. They report that it would be challenging to work on such topics with children with intellectual disabilities, as there may not be immediate feedback or response, or it is difficult to measure the outcomes. The time constraints and the importance given to other skills make it difficult for special educators to give importance to sexual health education. We can make creative lesson plans and implement them properly rather than brushing over the topics… These topics won't be included in the syllabus, so there won't be enough time to discuss these topics as well… If we teach them this, they will learn to protect themselves; they will also know the appropriate behaviour that they should be disciplined in public (Participant 17, a female special educator).
However, educators expressed that most of the existing programs are not sufficient to create awareness among students. As most focus on creating awareness among parents but parents were reluctant to give importance to sexual health education unless there was a threat. Educators reported that parents tend to not give importance to sexual health education like any other life skill. Participant 8, a female special educator, said, "Parents question us for not teaching any other skill but not for these (sexual health concerns). They think it is not very important until the need arises."
Subtheme: Risks of abuse
Special educators have observed that the chances of sexual assault are higher in schools, buses, public areas, and unfamiliar and abandoned locations. Special educators stated that raising parental understanding about developmental stages and physically separating females and boys in the classroom will assure children’s safety. “We should teach them to maintain distance from males; this can avoid bad touch and speak of inappropriate words.” (Participant 16, Female special educator)
Special educators had different suggestions regarding the age for sexual health education as 10 or 5 years. Aside from age, sexual health education should be delivered considering physiological changes due to growth, psychological development, and individual differences. It could help prevent maladaptive behaviour. Abuse can happen at any age, so it is better to start above five years when they do a few things independently or out of school. Preventing it is better than worrying about it later. They need to know who can touch them and who cannot. They may think 'what will happen if he touches, it is not a serious issue or 'what’s the big deal in touching’ if the person is known or not, they should be adequately informed before. (Participant 17, Female special educator)
Theme 2: Cultural factors
Participants mentioned the misconception and stigma parents have regarding sexual health education as a challenging factor to handle. Proper awareness and education are thus needed to reduce the stigma and normalise sex education in society.
Subtheme: family and community attitude towards sex and sexuality
Special educators reported that parents and teachers play a significant role in their children’s decision-making regarding sexual health. A special educator who was a parent mentioned that they prefer explaining homosexuality as a bad practice to adolescents with intellectual disabilities, and they want to recommend avoiding such relationships.
Participant 1, A female special educator, expressed her views on homosexuality. “They should know because it (homosexuality) is wrong, and I would not let my children behave in such a way.”
Theme 3: Personal Challenges
Special educators shared their challenges in imparting sexual health and reproductive health education to adolescents with intellectual disabilities. It ranges from inadequate training, which leads to questioning their ability to impart sex education, to the lack of support from the organisation.
Subtheme: Lack of confidence
Special educators reported lower comfort levels and confidence in imparting sexual health education. In addition, participants mentioned that their preservice and in-service training did not help develop competencies and skills in teaching sexual health education confidently. “... this may create anxiety that I should convey the content in a short period without making the child misunderstand or over-generalize it” (Participant 2, Female special educator)
Subtheme: Misguided and incomplete information
The participants expressed concerns about the media’s influence in providing inaccurate sexual and reproductive health information. The provision of accurate information that is not censored decreases the risk of misinterpretation. But the concept of sexual health is taboo for discussion in India, leading to the hesitation to provide accurate information. I don’t know exactly why, but they are being censored. I now realise that the information I received (when I was a student) was incomplete or unclear. As for these children again, it is very doubtful about what they receive (Participant 10, Male special educator).
Subtheme: Support from leadership and colleagues
The participants shared the barrier to providing quality sexual health education, as the lack of support from the institutional administrators and parents, trained educators, and lack of resources. Without their support, imparting knowledge and skill would be difficult. Participant 18, a female special educator, described how the preconceived notion of schools affects sexual health education. She mentioned that adolescents with intellectual disabilities won’t understand the concept of sexual health education. We assume they don’t understand though they can be taught to a certain extent. Some teachers may have a notion that they (adolescents with intellectual disabilities) won’t be able to understand why I would try doing it (sexual health education). (P18, Female special educator)
Discussion
The present study aimed to understand special educators’ perspectives on sexual health education for adolescents with intellectual disabilities and the challenges special educators face in imparting sexual health education. In India, talking about sexual health is still taboo (Manivasakan and Sankaran, 2014). Social structures and support systems impact special educators’ perceptions and views. Special educators emphasised the lack of sexual health education among their students. Students' gender and intellect significantly determine how teachers discuss sexual health and safety (McDaniels and Fleming, 2016).
Children with disabilities are at double the risk of being abused (McDaniels and Fleming, 2016; Singh et al., 2014). Possible perpetrators range from strangers to known family members and even a parent (Jones et al., 2012). Most preventive programs focus on creating awareness among students rather than teaching them skills to defend themselves (Schaafsma et al., 2015). Providing awareness to adolescents with intellectual disability and their parents helps them understand certain conditions like physical changes due to puberty, be sexually safe, and identify and protect themselves in risk situations (McDaniels and Fleming, 2016). Children who are sexually abused are more likely to engage in sexually acting out or abusive behaviour, attempting suicide, or other self-injurious behaviour (Jones et al., 2012). Most special educators reported that sexual health and safety education is important for female students. Abuse prevention for male students is often neglected (Banks, 2014). Sexual health knowledge is essential for adolescents' psychological and personal development (McDaniels and Fleming, 2016). Classroom teaching is necessary for students to acquire knowledge about sexual health apart from what they learn as they grow up (Nelson et al., 2020). The right age to impart sexual health education depends on the special educator’s judgment and the student’s level of understanding. Instead of treating them as a child based on their mental age, their chronic age and physical development should be considered (Barnard-Brak et al., 2014).
The myths around sexuality hinder inclusiveness and lead to a lack of proper healthcare needs. Physical and mental health needs more attention and care (Majumder and Kar, 2021). Educating necessary stakeholders and the community about the sexual behaviour of adolescents with intellectual disabilities helps to remove the stigma related to disability and sexuality (Schaafsma et al., 2015). Parents and special educators have difficulty accepting sex education and sexuality in a traditional community (Tamas et al., 2019). The prejudice and stigma associated with homosexuality are higher. Many families and communities do not accept homosexuality and consider it abnormal (Srivastava and Singh, 2015). Adolescents with intellectual disabilities’ rights to explore their sexuality and follow their sexual orientation are restricted (Holland-Hall and Quint, 2017). Special educators and parents feel responsible for the sexuality of their children and believe homosexuality often can be disciplined, which leads the youngsters to develop social strategies to cope with their surroundings (Stoffelen et al., 2013). Parents being part of sexual health and safety education helps the adolescents better (Haruna et al., 2018). But at times, parents are uncomfortable and do not prefer discussing sexual health with their adolescent kids with intellectual disabilities (Nelson et al., 2020). It was difficult to disregard the assumption that it was unnecessary for them. Unfortunately, parents tend to hinder such training if they believe it is not required unless serious situations arise (Jones et al., 2012; Thomas et al., 2014).
Special educators play role in educating students with intellectual disabilities on sexual health. Media influences students’ awareness of issues including sexual health, however not all media content may provide students with the right information (Döring, 2021). To address this crisis, special educators can sort resort in two ways. 1) they have to be equipped scientifically to educate the students on sexual health with a developmentally appropriate method (Treacy et al., 2018); 2) regular monitoring of the information intake from educators and parents is required to reduce exploitation and misinformation overload (Winges-Yanez, 2014). Though the latter seems to have limited the special educator’s role, proper training and scientific resources could be made available, making them resourceful to facilitate the learners. External agencies could provide in-house training and follow-up for the special educators on current pedagogical skills and information on teaching sex education to children with intellectual disabilities (Fine, 2013).
Educators must provide uncensored, accurate, and informative knowledge to facilitate adolescents with intellectual disabilities to prepare themselves for society. Appropriate sex education helps prevent exploitation, unwanted pregnancy, sexually transmitted disease, and abuse (Treacy et al., 2018). Special educators must integrate sexual health education in lesson plans for better facilitation (Nelson et al., 2020) of learning among preadolescents and adolescents with intellectual disabilities. The lesson plans must be creative, including narration, interactive sessions, and games for effective implementation (Haruna et al., 2018). Special educators believe that the gender and age of students determine the need for students to receive sexual health and safety education (Barnard-Brak et al., 2014). A student with intellectual abilities would require an individualised education plan to comprehend sexual health, and a standard curriculum may not meet the needs of all learners (McDaniels and Fleming, 2016). Similarly, the factors such as prioritising other skills, teaching based on curriculum, and time constraints influence special educators to decide whether to teach sexual health or not (Tamas et al., 2019).
Special educators sometimes feel burdened with subjects that they reduce allotted time or do not teach sexual health. Along with the pedagogical skills and content knowledge, the special educators disclosed that a comfort level and alignment of oneself to the lessons affect the quality of the teaching. Stepping out of the comfort zone is not entirely about addressing the emotional blocks of the educator but more about the underlying cultural and societal factors that take their place in their belief system (Harrison and Ollis, 2015). Some schools take the initiative to bring in external agencies whose expertise in sexual health can help the children for greater understanding and facilitate the educators in ‘normalising’ the contents (Smith et al., 2013). However, collaboration from the administration and follow-up from the teachers form a required base to enhance the quality of learning among students with intellectual disabilities. Support from a multidisciplinary team would enhance outcomes (Jacob, & Kumar, 2021).
Unclear roles and multiple responsibilities the school gives sometimes make the special educators spend less with the students. It reduces the opportunity for extra instruction and support. The special educators' roles vary, implying that professionals dealing with intellectual disabilities may not feel qualified and are hesitant to teach (Treacy et al., 2018). Special educators reported a lack of support from leaders and colleagues. Schools follow an eclectic range of strategies. However, this will work for the benefit of the learners when they work collectively to promote similar values (Sharma et al., 2012). Successful collaboration from colleagues at different levels ensures the quality of the content presented to the students and higher success in the inclusion practice (Mulholland & O’Connor, 2016: 1070).
Conclusion
Special educators need extensive training in sexual health and safety education for adolescents with intellectual disabilities. Sexual and reproductive health education is a crucial concern for special educators. They should educate parents and students to handle sexual health concerns using multiple mediums. Sexual health programs should be developed based on the individual needs of the learner with special needs especially considering age, gender, and disability. Support from parents, colleagues, school administration, and society plays an essential role in successfully implementing such programs.
Implication and recommendations
Special educators require training and support to facilitate topics of sexual health and safety among adolescents with intellectual disabilities. The special education teacher education programs should include topics of sex education and safety as key elements in the training curriculum. There is a need for evidence-based and culturally competent models to support special educators and the models should focus on the sexual health and wellbeing of adolescents with intellectual disabilities. Many have the misconception that the sexual health and well-being of adolescents with intellectual disabilities are not required. At the same time, the sexual needs of adolescents with intellectual disabilities are considered non-existent. These models should help bust the myths and misconceptions among educators, parents, and the community. Parents should be partnered with for interventions and effective collaboration between parents and school can strengthen the program outcomes (Kumar and Paul, 2019). The topics of sexual health and safety education would have aspects that require the support of medical and mental health professionals. Hence intervention by a multidisciplinary team approach by trained professionals like medical doctors, psychologists, counselors, and social workers is integral (Jacob, & Kumar, 2021). It would empower adolescents with intellectual disabilities with accurate information about sexual health and safety.
Limitations
The study was limited to a particular geographical area, which reduces the possibility of understanding the concern on a large scale. There are taboos on openly talking about sex in India and hence would have impacted responses. Subjective preference and moral value could have influenced their perspective even though the primary knowledge providers cannot afford biased opinions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study involves only human participants and no harms were inflicted on the participants. The research protocols were reviewed and approved by the IRB at the University.