
Abstract
This study aimed to assess the validity and reliability of the world health organization quality of life questionnaire for people with intellectual disability (WHOQOL-DIS-ID). This was a cross-sectional study of 118 adults with intellectual disability. Internal consistency and temporal reliability were evaluated using Cronbach's alpha and intraclass correlation coefficient (ICC), respectively. Construct validity of the structure was assessed using confirmatory factor analysis. Multiple linear regression analysis was performed to determine the factors associated with the quality of life. Cronbach's alpha for all, but not for discrimination area, as well as ICC for all questions except for 23 and 6, were higher than 0.7. The variables such as periodic check-up, number of friends, entertainment outside the home, parental separation, physical activity, unmet needs score, caregiver's mental health status, and available facilities were the predictors of QOL. The Persian version of the WHOQOL-DIS-ID shows acceptable validity and reliability.
Keywords
Introduction
Intellectual disability or intellectual developmental disability is one of the most common neurodevelopmental disabilities worldwide (des Portes, 2020). Intellectual disability refers to a significantly reduced ability to understand new or complex information and learn and apply new skills, leading to reduced ability to cope independently (impaired social functioning). It begins before adulthood and has a lasting effect on development (WHO, 2010). In high-income countries, the prevalence of this disorder has been reported from 3.21 to 36.75 per 1000 people this amount is almost double and sometimes more in low-income countries (Maulik et al., 2011). According to census results in 2011, the prevalence of intellectual disability is around 13/1000 population in Iran. (Soltani et al., 2015)
People with disabilities need a wide range of health services, ranging from simple to expensive and complicated interventions. (WHO, 2011). Minorities' participation (in health research e.g., individuals with disabilities) is not only a civic right but also a step toward improving study integrity and accuracy, as well as interpretability in policymaking and the development of care and treatment systems. (Rios et al., 2016).
The general concept of quality of life (QoL) was initially introduced as a complement to traditional health and functional status concepts. According to World Health Organization, an ideal health assessment involves measuring physical health and activity, social and psychological performance, and quality of life (The Whoqol, 1998). Traditionally the QoL of people with an intellectual disability has been defined through objective measures of their life circumstances, such as standard of accommodation, patterns of time expenditure, the extent of interaction with the general community, and so forth. Meanwhile, numerous studies have shown that there is remarkably little relationship between, the objective condition of living and degree of satisfaction, actually under relatively stable but diverse living conditions most people feel satisfied with their lives (Cummins, 2005). Accordingly, current QoL measurements consist of both objective and subjective dimensions.
Monitoring and reporting, quality improvement, and research are all becoming more common uses for assessed QoL scores. In research studies, QoL scores should be measured using an instrument that is (1) based on a validated QoL conceptual model that is operationalized through culturally sensitive domain-referenced indicators that meet the criteria of suitability, importance, observability, and sensitivity; (2) developed using best practices that include field testing, establishing psychometric properties, and publishing an administration and standardization manual; and (3) uses proxy report. (Schalock et al., 2018).
In order to create a valid, reliable, and usable tool in different cultures international cooperation was promoted under WHO supervision; and world health organization QoL questionnaires (WHOQOL) were developed for the general population and various subgroups, including people with disabilities (Power and Green, 2010). The WHOQOL-DIS has been developed in two versions for people with physical disability (WHOQOL-DIS-PD) and people with intellectual disability (WHOQOL-DIS-ID) to assess the impact of service provision and different health and social care structures on QoL (Power and Green, 2010). The physical disability module of this tool has been validated in many countries including Brazil, Spain, Korea, Turkey, Malaysia, and Iran (Bredemeier et al., 2014, Lucas-Carrasco et al., 2011, Lee et al., 2017, Eser et al., 2018, Jani et al., 2020, Chehelamirani et al., 2016). However psychometric properties of the intellectual disability module are not consistently addressed yet. Not only this tool but also all QoL assessment tools for people with intellectual disability lack rigorous demonstration of psychometric properties throughout the QoL literature. the first aim of this study is to assess the psychometric properties of the Persian version of WHOQOL-DIS-ID.
As outlined above, research results from low and middle-income countries report a higher prevalence of intellectual disability (Maulik et al., 2011). Additionally, people with disability face multiple barriers to accessing various services, particularly in developing countries. People with disability experience poorer health status than those without disabilities. Higher rates of poverty, lower educational and occupational opportunities, and restrictions on inclusion in society in developing countries contribute to disadvantages experienced by individuals with a disability (WHO, 2015). Studies show that people with intellectual disabilities in Iran experience poorer health status as a consequence of disability and barriers to access to health services (Soltani et al., 2017). It is recommended in recent studies that less developed countries should give more importance to improving infrastructure that helps in the rehabilitation of individuals with disability including people with intellectual disabilities To establish practices for improving QoL evidence-based information is required. (Memari and Hafizi, 2015) Previous studies demonstrated the impact of personal characteristics, environmental factors, support strategy, and preserved social support and unmet needs on the QoL of people with intellectual disabilities (Simões and Santos, 2016, Simões and Santos, 2017, Lombardi et al., 2016, Memisevic et al., 2016) Additionally, it is important to note that the impact of parental mental illness on the psychological, social, and intelligence outcome of their offspring was highlighted in previous studies (Lancaster, 1999, Havinga et al., 2017) and another study demonstrated the impact of responsive parenting on QoL of pediatrics (Botello-Harbaum et al., 2008). Considering all the above-mentioned points regarding the necessity of evaluating the psychometric properties of the QoL instrument and the QoL level of people with intellectual disability and also the higher prevalence and lower well-being of these populations in lower-income countries, this study aimed to primarily evaluate psychometric properties of the Persian version of WHOQOL-DIS-ID and then examine the QoL of a sample of individuals with intellectual disabilities as well as its influencing factors.
Materials and methods
This was a cross-sectional study on the adults with ID, selected from centers devoted to individuals with intellectual disability including rehabilitation centers for adults with intellectual disability and welfare organizations and specialized schools in Tehran. Inclusion criteria were age ≥18 years old, and a diagnosis of ID. Exclusion criteria were severe ID, severe mental disorder, severe speech disorder, and inability to cooperate. Simple random sampling was used to include individuals from the list of eligible ones. Five centers were revisited 2-4 weeks later to collect information for retesting. The data analyses were conducted using IBM SPSS Statistics v.18, Stata v.14, and IBM AMOS v.24 software.
Personal information questionnaire
The designed questionnaire included information on age, sex, level of education, level of education and employment status of parents, body mass index, disability level, intelligence quotient (IQ) level, the existence of multiple disabilities, living condition (with whom), economic level, number of friends, occupational/educational status, weekly physical activity, periodic checkup by a psychologist or psychiatrist, care givers' mental health status, parental separation, co-morbidity, satisfaction with parent support level, adequacy of outdoor activities, entertainment, and availability of required facilities.
WHOQOL-BREF-ID questionnaire
WHOQOL-BREF (26 items) is the short version of the WHOQOL-100 questionnaire, measuring four areas of physical, psychological, and environmental health as well as social relationships (Whoqol-Group, 1998), through 24 questions. It has also two general items not belonging to any of the areas and assessing health status and QOL generally.
In the general version of the questionnaire, the response to each item is based on a 5-point Likert scale from strongly agree to strongly disagree. For people with ID, there are a few simplifications of wording in the main questionnaire (WHOQOL-BREF-ID). The response to items is also a 3-point Likert scale including agree, uncertain, and disagree, also presented as a pictogram; exceptionally two general items are 5-point Likert-scale.
WHOQOL-DIS-ID questionnaire
The questionnaire has been developed and standardized to be used along with the general questionnaire of WHOQOL (WHOQOL-100 or WHOQOL-BREF) in people with intellectual disabilities (Power and Green, 2010). The questionnaire includes a general item addressing the overall impact of disability in a 5-point Likert scale and 12 other items for assessing discrimination, autonomy, and social inclusion which are 3-point scale. It was used in conjunction with the WHOQOL-BREF-ID in the present study and contained 39 items in total.
Unmet needs assessment questionnaire
This questionnaire was developed in a study conducted in collaboration with the Massachusetts Department of Health by the University of Massachusetts Research Center and the Disability Policy Coalition (Mitra et al., 2011). It includes two areas of activities of daily living (ADL) and instrumental activities of daily living (IADL). Ten other questions measure individual needs in the areas of home services, service management, information, access to medical care, physiotherapy and occupational therapy, medicine, food, assistive devices, and transportation. Answers are "yes-no", "sometimes" and "need more help". The lowest score is zero, while the maximum score is 12.
Translation
First, the WHOQOL-DIS-ID jointly with the WHOQOL-BREF-ID questionnaire was translated into the Persian language by two separate translators. Then, a single copy of these two translations was extracted. The relevant Persian version was translated into English twice separately, and then a single English version was prepared from the two relevant versions; finally, it was compared and matched with the original questionnaire.
After that, the final version of the Persian questionnaire was given to a translator expert in the disability field to examine the final Persian version in terms of the desirability of expressions, clarity, use of simple and understandable words, and avoiding the use of technical and specialized words.
Content and face validity
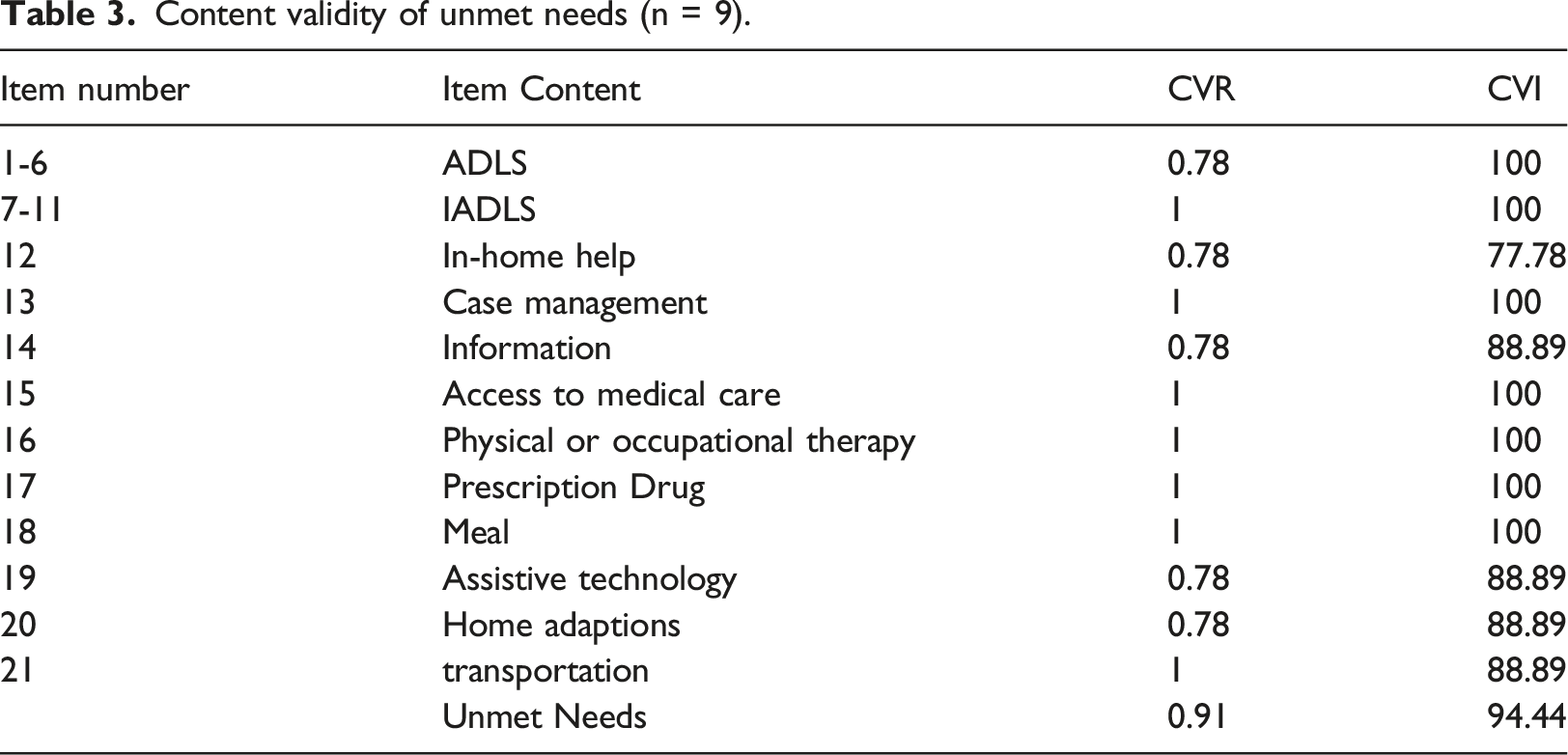
Nine experts in rehabilitation, psychology, occupational therapy, quality of life, welfare sciences, and education were consulted to determine and evaluate the face and content validity of the questionnaires. Accordingly, changes were made in the relevant tools to make it easier and more understandable for the target group. In addition, to receive the opinions of the target community, an interview was conducted with three of them, and their opinions in the field of ambiguity, the meaning of the questions, and the meanings of the words were applied to the questionnaires. Then, content validity index (CVI) and content validity ratio (CVR) indices were calculated for WHOQOL-BREF-ID, WHOQOL-DIS-ID, and unmet needs questionnaires as well. According to Lawshe and Lyn for nine-panel members, 0.78 and 78% were the minimum values to validate acceptable content validity ratio and content validity index, respectively. (Polit et al., 2007, Lynn, 1986)
Construct validity
First-order confirmatory factor analysis (CFA) was utilized using AMOS 24 to evaluate the accuracy and validity of the factor structure of a set of observed variables. First, the Kaiser-Meyer-Olkin test was performed to measure the sample size's adequacy to evaluate the confirmatory factor analysis. A value higher than 0.7 for the Kaiser Meyer index was considered a sufficient sample size in the present study. Bartlett test was also used to examine the correlation matrix among variables. To check the measurement model validity, the goodness of fit indicators were assessed. Widely accepted global goodness of fit indices are ratio chi-square to degrees of freedom (x2/d.f.), the standardized root mean square residual (SRMR), root mean square error of approximation (RMSEA), and the comparative fit index (CFI), Normed Fit Index (NFI), and Goodness of Fit Index (GFI). For a good model fit, the cut-off criteria are χ2/d.f. ≤ 2, GFI ≥ 0.90, CFI ≥ 0.90, RMSEA ≤ 0.08, SRMR ≤ 0.08, NFI≥ 0.90 (Tabachnick et al., 2007, Hu and Bentler, 1999, Byrne, 2010).
Internal consistency
Cronbach's alpha was used to assess the internal consistency of WHOQOL-DIS and unmet needs assessment questionnaires. The Cronbach's alpha was calculated separately for the domains in both questionnaires.
Temporal reliability
Intraclass correlation was used to assess the temporal reliability (test-retest). A single group was interviewed twice, and the scores were compared to calculate this index. The time interval between test and re-test was between two weeks to one month. The intraclass correlation above 0.7 was considered as the appropriate limit (Tinsley and Brown, 2000).
Multiple linear regression
The association of each independent variable with dependent variables was assessed by univariate linear regression, and the variables with alpha scores smaller than 0.2 were included in multiple linear regression. Multiple linear regression was utilized to determine the predictors of the outcome variables. Regression analysis was performed by a stepwise backward method with an alpha of 0.1. In the final model (multivariable), the significance level was considered as 0.05. Due to violation of the normality assumption for outcome variables, a sensitivity analysis was performed by the bootstrap method, but P-values did not change significantly; therefore, the results of standard multiple linear regression analysis were reported (Etminan et al., 2021, Mansournia et al., 2021a, Mansournia et al., 2021b)
Ethical considerations
The study's generalities and objectives were explained to the cases and the centers' officials, and then, if they consented to participate in the study, they would be interviewed. Participants were reassured that they could leave the study at any time for any reason. All patients' personal information was kept confidential, and one code was assigned to each person instead of using his/her real name.
Results
Participants’ characteristics.
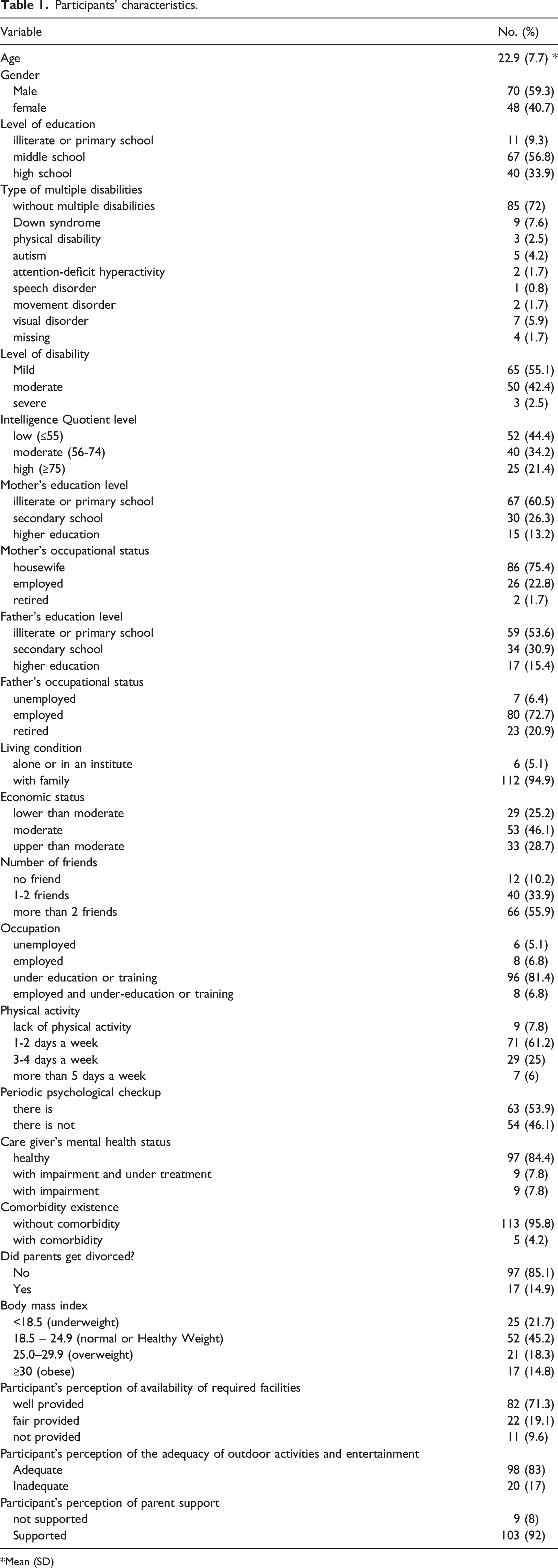
*Mean (SD)
Content validity of WHOQOL-DIS (n = 9).
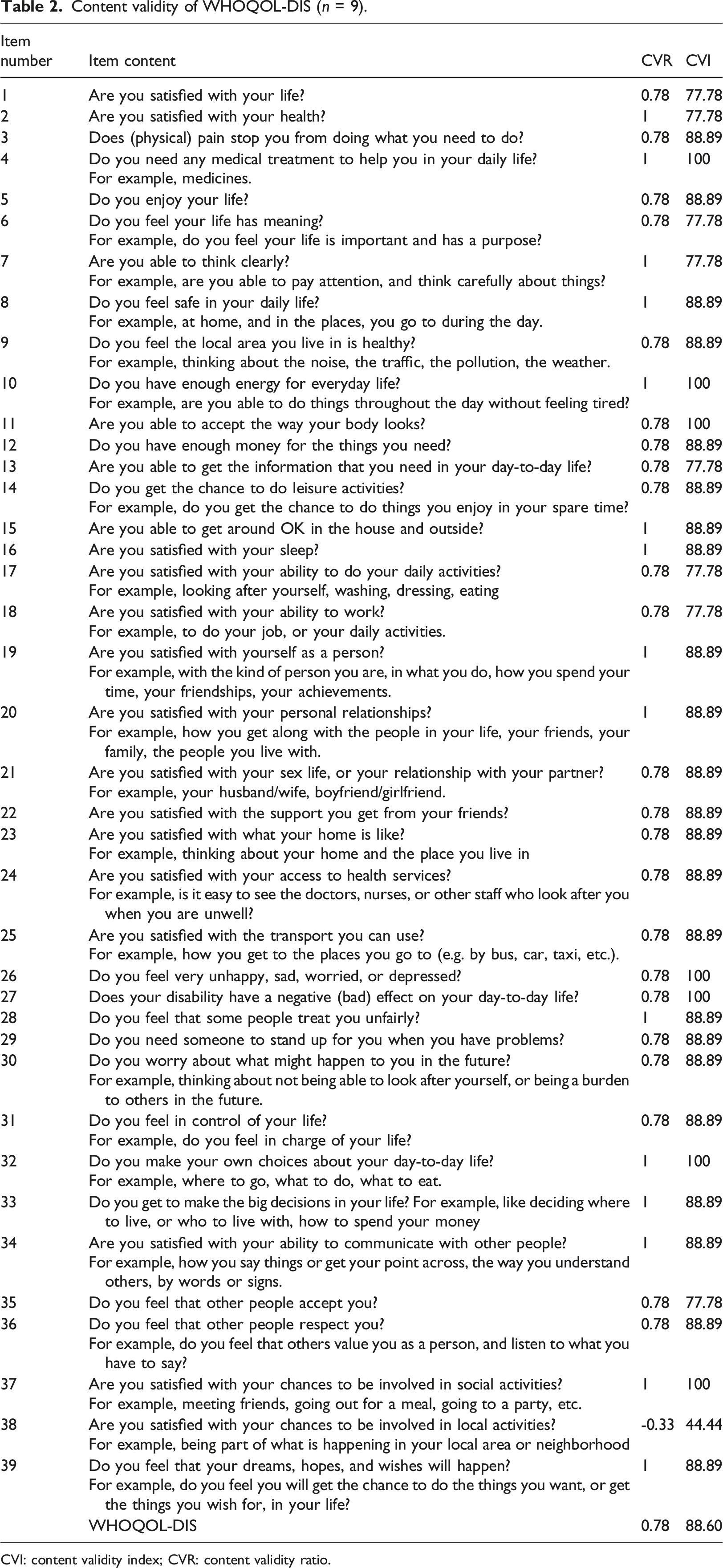
CVI: content validity index; CVR: content validity ratio.
Content validity of unmet needs (n = 9).
Confirmatory factor analysis (CFA) was performed to test the construct validity of the questionnaires. Based on Kaiser-Meyer-Olkin (KMO) and Bartlett tests, there was enough sample size to perform factor analysis (KMO = 0.73, Bartlett's = 463.9 and P-value <0.001). Although factor loads showed that the correlation of explicit and implicit variables in the three-domain model was desirable, questions 28 and 29 needed to be re-examined (Figure 1). In this analysis, using the maximum likelihood estimation method, it was shown that the 3-domain model of the disability module (CFI = 0.906, NFI = 0.828, RMSEA = 0.089, χ2 = 78.63, d.f. = 41, p <0.001) fitted better than the single domain model (CFI = 0.775, NFI = 0.708, RMSEA = 0.132, χ2 = 134.17, d.f. = 44, p <0.001). For the 3-domain model, GFI was 0.91, higher than the cut-off point. Furthermore, SRMR, RMSEA, and chi-square ratio to the degree of freedom (χ2/d.f.) were 0.001, 0.89, and 1.92, respectively, among which SRMR and χ2/d.f. met goodness of fit measure. Best fitting CFA model for 12-item disability module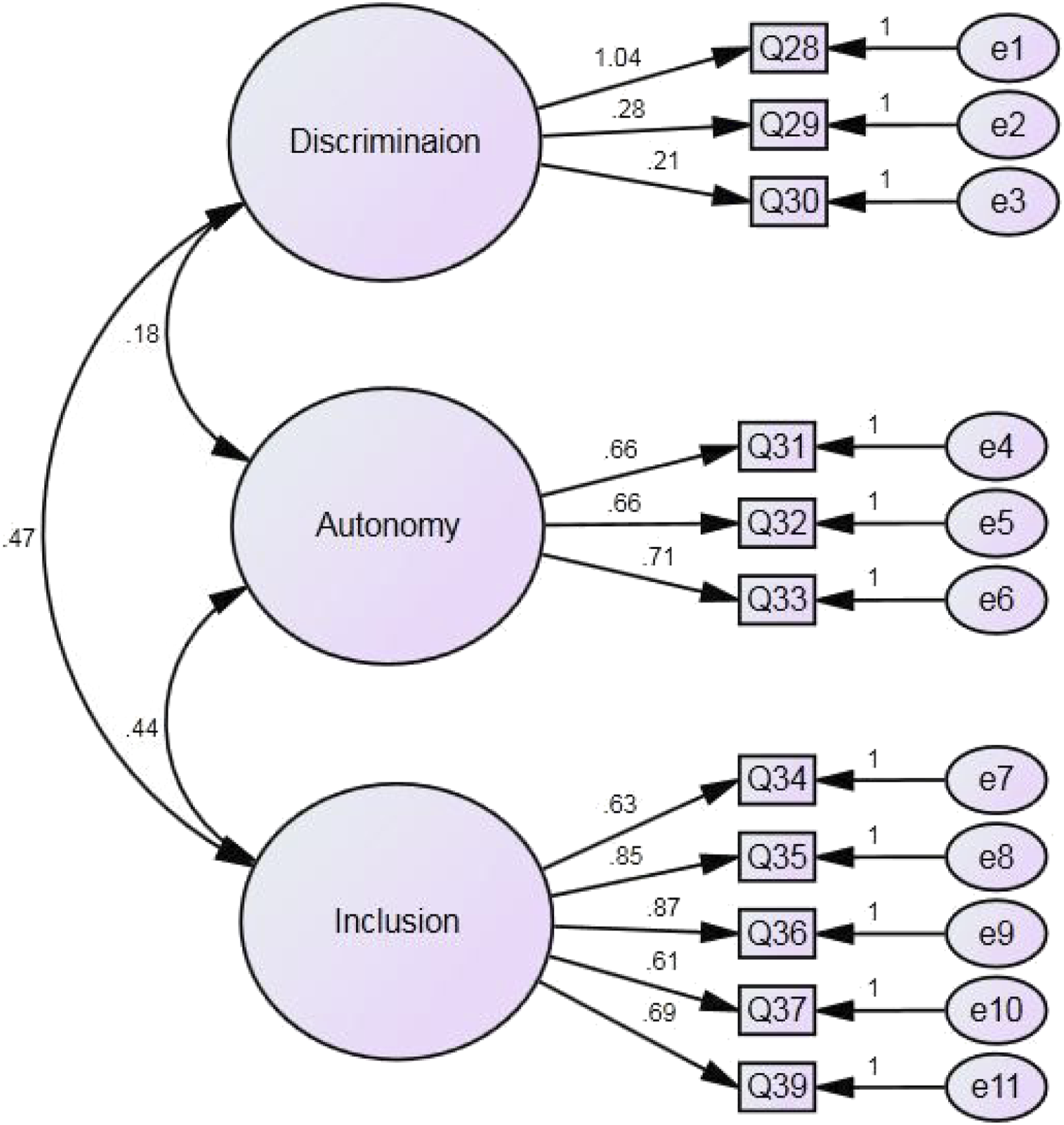
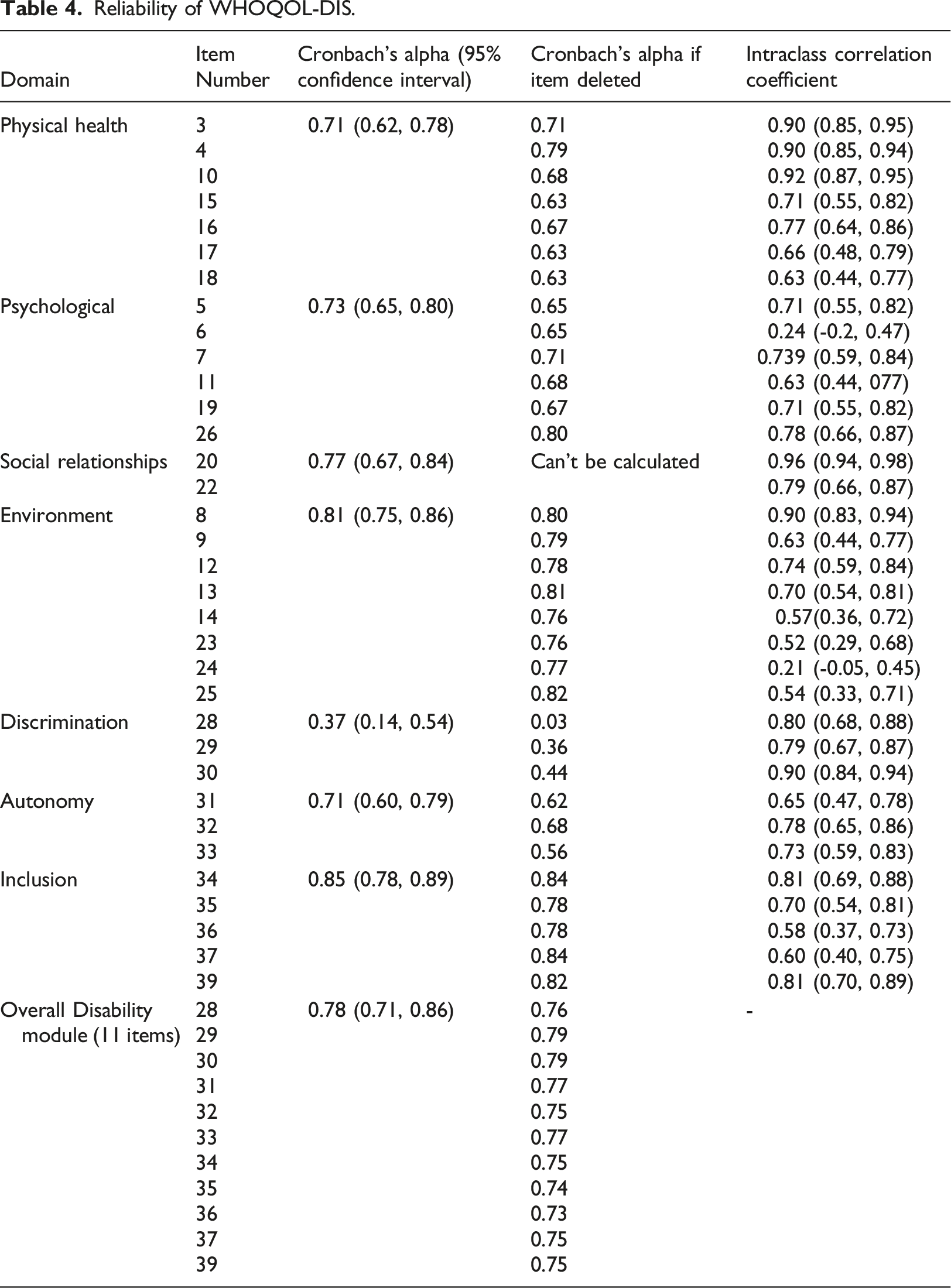
Reliability of WHOQOL-DIS.
Reliability of unmet needs.
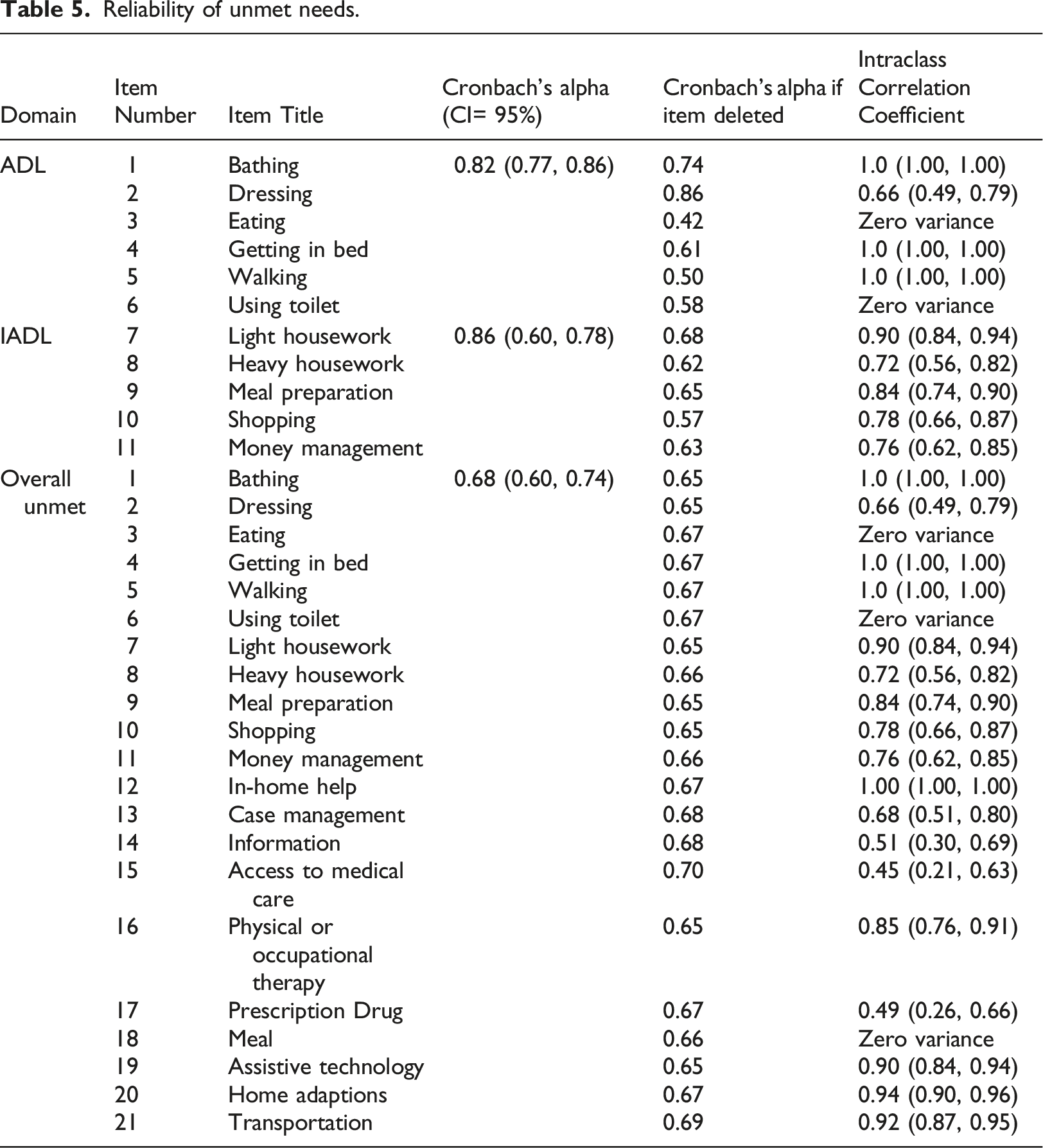
The lowest temporal reliability in the QOL questionnaire was for the question 24 (ICC = 0.27, 95% CI: (0.05, 0.45)), whereas the highest was for the question 20 (ICC = 0.96, 95% CI: (0.94, 0.98)). ICC was desirable for all questions (except 24 and 6); higher than 0.7 (0.71 to 0.99) (Table 4). Generally, the unmet needs questionnaire was temporally reliable. ICC could not be estimated for some questions because there was no variance between the data. In general, the lowest reliability was for the question associated with access to medical care (ICC = 0.45, 95% CI: (0.21, 0.63)), and questions related to bathing, getting in bed, walking, and in-home help were perfectly correlated over time (ICC=1) (Table 5).
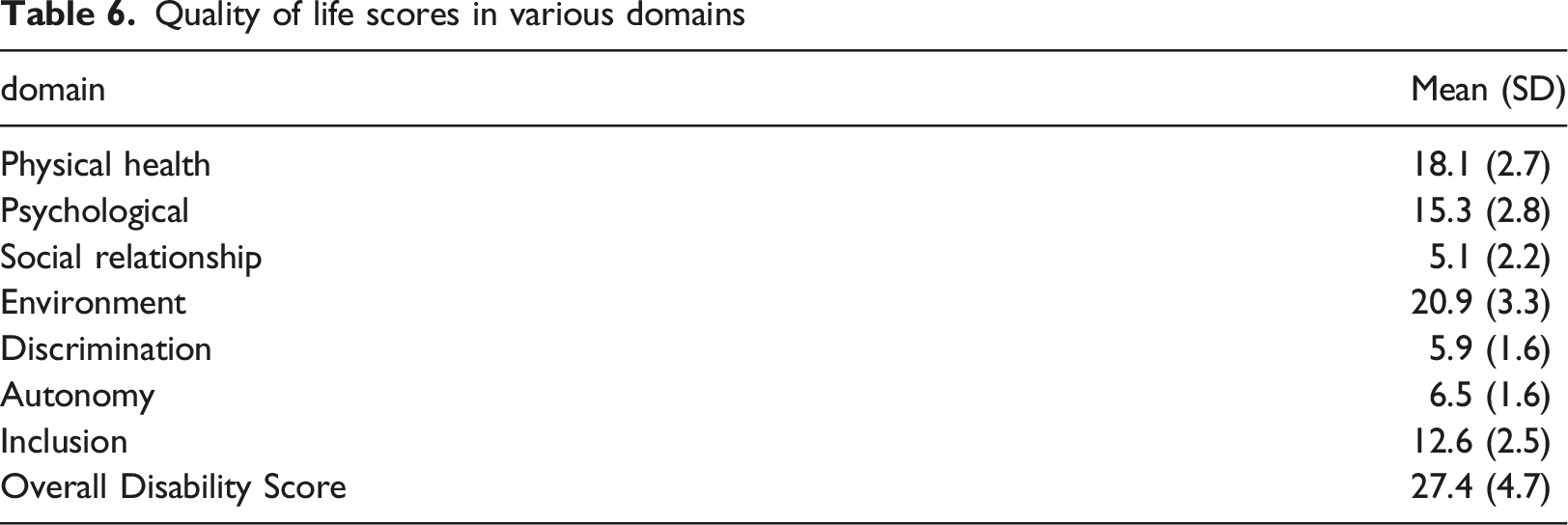
Quality of life scores in various domains
Associated factors to quality of life score in various domains
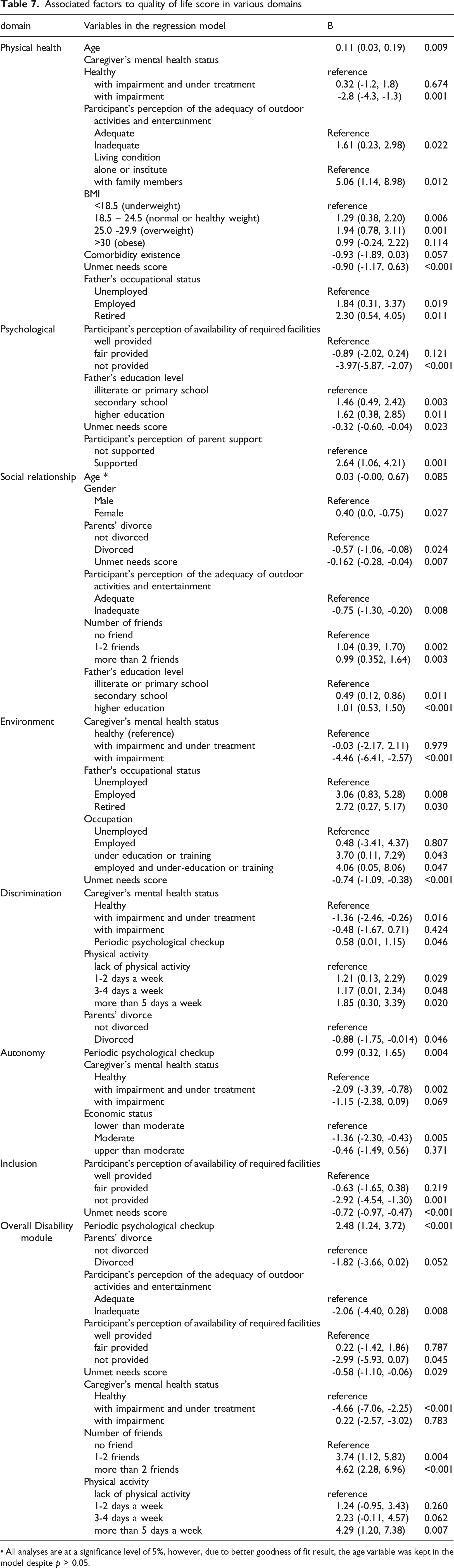
• All analyses are at a significance level of 5%, however, due to better goodness of fit result, the age variable was kept in the model despite p > 0.05.
Discussion
This study aimed to assess the validity and reliability of the WHOQOL-DIS questionnaire, estimate the average score of QOL in various domains in an adult community of people with intellectual disability and determine some related factors. The WHO quality of life questionnaire for people with disabilities was presented by the WHO in 2010 to assess adults' general QOL with intellectual and physical disabilities and was formally added to the WHOQOL-BREF or WHOQOL-100 questionnaire (Power and Green, 2010). The field of QOL of people with disabilities is an entirely new field that has not been studied well in Iran and the world. The questionnaire, originally in English, has been translated into other languages, including Chinese, Korean, Spanish, and Turkish, and its validity and reliability have been assessed. In the physical disability version of the Persian translation of this questionnaire, conducted in 2016 on elderly individuals with disabilities, the total ICC was reported to be good. The minimum and maximum CVR rates were 0.53 and 0.92, respectively, and the CVI rate was 0.83. In this study, in the content validity review (using Lauche, Waltz, and Basel methods), an "acceptable" score was obtained for all items. Cronbach's alpha was acceptable for all domains except the social dimension (Chehelamirani et al., 2016).
In reliability analysis, based on the internal consistency method, the minimum Cronbach's alpha was for the social relationship domain (0.63), while the maximum was for the physical health domain (0.82). In the test-retest reliability, the lowest ICC was for the social relationship domain (0.71), whereas the highest ICC was for the environmental domain (0.88). In the Brazilian version of this tool (Bredemeier et al., 2014), as in the present study, it was stated that the Cronbach's alpha correlation coefficient for all areas of this questionnaire was acceptable. likewise, the construct validity of the Brazilian version was appropriate. In the Spanish version of this tool (Lucas-Carrasco et al., 2011), it was stated that the internal consistency of the questionnaire was excellent, and in all domains, except the social domain, it was 0.71. Similar to our results, in the Turkish version (Eser et al., 2018), based on the internal consistency, the discrimination domain (Cronbach's alpha: 0.54) was not acceptable in contrast to the other domains, which were above 0.7 and acceptable. Finally, the Korean version of WHOQOL-DIS (Lee et al., 2017) and WHOQOL-BREF showed consistency of 0.7 in the repeatability dimension. In the Korean version, internal consistency was 0.732, and the lowest correlation was related to discrimination (0.60). The results of the Korean study are consistent with those of the current study.
The mean score of the overall QOL-DIS of participants was 27.4 (74.54 in the range of 0-100). Consistent with our result on QOL score, a study carried out using WHOQOL-DIS by D.Koch showed a mean score of 72.6 QOL for adults with intellectual disabilities (Koch et al., 2015). Meanwhile, a review on the subjective well-being of individuals with intellectual disability done by Cummins (2005) indicated that although a quite different approach was utilized, the data symbiosis from 16 unrelated studies on life satisfaction resulted in a mean of 75/02 SM (SD:2,74)(Cummins, 2005). Furthermore, two studies carried out by Balboni et al. (2013) revealed a QOL score of 115.25 (70.05 in the range of 0-100 and 94.17 (72.6 in the range of 0-100) ) for people with ID, being in line with our results on the QOL score (Balboni et al., 2013, Simões and Santos, 2016)
QoL of students with and without intellectual disabilities. The findings of the study demonstrated fathers' occupation and education were predictors of QoL score among students with intellectual disabilities (Hematian et al., 2009).
The findings of the current study showed a relationship between unmet needs and reduced QOL scores in all domains except discrimination and autonomy. According to the results of two studies, the unmet needs of people with disabilities were three times more than those without disabilities (Koch et al., 2015). Moreover, other studies confirmed the relationship between unmet needs and reduced QOL scores among cancer patients, multiple myeloma, and Huntington's disease (Hansen et al., 2013, Molassiotis et al., 2017, Pereira et al., 2020, van Walsem et al., 2017). The findings of the present study suggested that besides participant characteristics, unmet needs explained a significant amount of variance in the QOL of people with intellectual disabilities. Another variable related to most domains (6 domains) was the mental health status of the caregiver. This finding was consistent with previous studies, indicating that psychological, social, and intelligence consequences were reduced in children of parents with mental disorders (Lancaster, 1999, Havinga et al., 2017)
Participants in this study were not randomly selected from society but were selected from educational and rehabilitation centers. Due to the lack of enough cooperation in the residential centers, access to people living in welfare centers was limited, and most of the participants were people living with their families or relatives. Access to the exact IQ score was not possible due to the lack of registration in the students' academic records, and the participants' IQ level was determined based on the statements of their school teachers and counselors. Due to the lack of interviews with the participants' parents, basic information was extracted based on the center's consultants' statements and information files. Question 21, measuring the quality of sexual life, was removed from the questionnaire due to referring to a culturally sensitive issue and risk of posing negative impact on the respondents' overall cooperation with the study. This study was one of the first studies in Iran to address QOL in people with ID.
Conclusion
Based on our findings, the Persian version of WHOQOL-DIS-ID showed acceptable validity and reliability. Interested researchers in this field can use this tool to study issues related to these people's QOL. The study also found out that the variables of unmet needs, the mental health status of the caregiver, monthly check-ups, adequacy of outdoor entertainment, availability of facilities, parental separation, the number of friends, physical activity, employment, and education status of fathers, age, parental support, job, and educational status, body mass index, and household economic status are the factors affecting the quality of life in people with ID.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the School of Public Health and Allied Medical Sciences, Tehran University of Medical Sciences (Approval ID: IR.TUMS.SPH.REC.1398.252).