
Abstract
Challenges exist in respect of people with intellectual disabilities who, with the increasing life expectancy, have a growing risk of age-related degenerative conditions. Changes in bone health are associated with increasing age and the bone health of people who have intellectual disabilities is well documented in the literature as being poor in comparison to the general population. A heel scan clinic was set up in an intellectual disability service as a service improvement initiative. There were 12 females and 17 males scanned using a heel scanner. Only 3 (10.3%) people with intellectual disabilities were in the normal bone mineral density (BMD) range. Peripheral BMD screening for people has been shown to provide important information about the bone health of people with intellectual disabilities which has prompted further treatment by general practitioners and has the potential to provide an accessible way to obtain information on the bone health of people with intellectual disabilities.
Background
An ageing population is one of the success stories of modern society, however, it also poses a real and significant challenge to individuals and families as well as for social, economic, and healthcare systems. It increases the person’s chance of developing long-term medical conditions such as frailty and dementia, which can result in increased disability, dependence and social isolation. Challenges also exist in respect of people with intellectual disabilities who, with the increasing life expectancy, have a growing risk of age-related degenerative conditions (Emerson et al., 2012). People with intellectual disabilities are living longer, yet, compared to the general population, they still experience a lower age of death (LeDeR, 2018). The risks of long-term mental and physical health conditions among people with intellectual disabilities have been reported as higher than the general population (Truesdale and Brown, 2017). ‘Diagnostic overshadowing’ has been highlighted repeatedly as a major risk to the health of people with intellectual disabilities (Disability Rights Commission, 2006; While and Clark, 2010). This occurs when changes in aspects a person’s presentation are explained as being part of the person’s intellectual disability and are not further investigated. This can include, but is not limited to; physical appearance (unexplained weight loss /weight gain), appetite, or general level of behaviour (fatigue, more sleeping, less engaged in previous activities), loss of previous skills, increased reports of pain and discomfort, reducing mobility, or fractures. In effect, the presence of intellectual disabilities ‘overshadows’ an underlying health condition (Sowney, 2019).
Internationally, over two decades, literature has persistently reported that people with intellectual disabilities often have more complex health needs than members of the general population. Many of these health needs can go unrecognised and unmet (Barr et al., 1999; Kinnear et al., 2018; Northway et al., 2017) resulting in shorter life expectancy compared with the general population (Heslop et al., 2013; LeDeR, 2020). In a recent study carried out by Kinnear et al. (2018), assessing the extent of multi-morbidities presented by adults with intellectual disabilities, the highest number of physical health conditions experienced by one person was 28. In this study, 98.7% (n = 1010) of participants had two or more conditions with only eight participants having no physical health conditions. Furthermore, Martin et al. (2017) identified that people with intellectual disabilities at 50 years of age have similar rates of frailty as adults aged 80 years or more, without intellectual disabilities.
One of the major issues identified has been a failure to make ‘reasonable adjustments’ to facilitate access to services and difficulties in communication within and between people and services involved is repeatedly highlighted (Heslop et al., 2013; Michael, 2008). Reasonable adjustments which are a requirement, under legislation related to disability discrimination or equality legislation internationally, are not always made (Barr, 2019; Finlayson et al., 2019). In particular, the lack of reasonable adjustments made in relation to sharing information and listening to people with intellectual disabilities and their carers’ communication, accommodating anxieties and preferences of people about their treatment have been highlighted. In contrast to this, a study about providing equitable access to a Dual-energy X-ray absorptiometry (DXA) scan for 30 people with intellectual disability, found that this enabled 29 people to have a successful scan (Finlayson et al., 2019). Those authors also reported that the majority of health care professionals who responded to their questionnaire reported that the reasonable adjustments were easy or very easy to implement in their departments.
A commonly reported finding is the need for improved inter-agency collaboration and communication, and increased awareness of the needs of people with intellectual disabilities (Iacono et al., 2014; LeDeR, 2020). Many staff working within general health care services have indicated that trying to treat people with intellectual disabilities can be more difficult. This is often related to the need for more time in busy care environments and the limited availability or timely sharing of information about the person’s abilities and needs in advance (Heifetz and Lunsky, 2018; Sowney and Barr, 2007). This has at times resulted in people with intellectual disabilities receiving fewer health investigations and being less likely to get the healthcare they require (Disability Rights Commission, 2006).
Bone health
The World Health Organisation (WHO, 2004) described osteoporosis as a multifactorial disorder characterised by low bone mass and micro-architectural deterioration of bone tissue leading to enhanced bone fragility. This can result in a marked rise in susceptibility to bone fracture. Changes in bone health are associated with increasing age in the general population, particularly older women. It has been reported that people with intellectual disabilities may experience increased osteoporosis and fractures (Frighi et al., 2019). Frighi et al. (2019) have argued that people with intellectual disabilities may also have increased risk factors including the use of anti-epileptic medication, reduced mobility and reduced vitamin D. As the onset of the condition is often silent and asymptomatic, it may only be recognised after a person has fallen and sustained a fragility fracture (Burke et al., 2017).
Harper (2017) highlighted that people with intellectual disabilities have increased susceptibility to developing osteoporosis and osteopenia due to comorbid health complications, including hypothyroidism, and polypharmacy. The use of antiepileptic and antipsychotic medications, limited opportunities for exercise and unhealthy diet, with deficiencies in vitamins and minerals necessary for good bone health are of particular note (Emerson and Baines, 2010). People with
Srikanth et al. (2011) reported that more than half a sample of people with intellectual disabilities over the age of 40 had osteoporosis or osteopenia. In a study of 29 people with intellectual disabilities who had a DXA scan after reasonable adjustments were put in place, it was reported that 79% of participants had either osteoporosis (41%) or osteopenia (38%) (Finlayson et al., 2019). A similar overall rate of 76% was found among 36 people with intellectual disabilities who had DXA scan, with osteoporosis reported in 23.7% and osteopenia reported in 52.6% of participants (Frighi et al., 2019).
Peripheral bone density measurement
Due to the insidious nature of osteoporosis, clinical diagnosis is often only obtained post fracture by means of bone mineral density measurement (BMD) which is measured by dual-energy X-ray absorptiometry (DXA). DXA is recognised as the ‘gold standard’ for diagnosis of osteoporosis, fracture risk and the monitoring of skeletal changes (Burke et al., 2017; Kanis et al., 2008). The early identification of osteoporosis and treatment can be compounded by having limited access to and difficulties in cooperating with screening for bone mineral density (Burke et al., 2017; Frighi et al., 2014, 2019).
However, for some people with intellectual disabilities, the need to lie down and remain still on a table for the duration of a scan can be difficult. It has been reported that there are some people for whom a DXA scan may not be acceptable or provide a high enough quality image, for example due to involuntary movements, a refusal to participate or lack of clinical benefits (Frighi et al., 2019). While Finlayson et al. (2019) have reported that the implementation of ‘reasonable adjustments’ enabled 29 out of 30 people to have a sufficiently high quality image in the DXA scan, for one person with intellectual disability this was still not successful. The reasonable adjustments included the provision of information about the DXA scan, careful planning of appointment at quieter times, longer appointment times, convenient parking, assess to toilet and refreshment and use of a hoist to transfer a person to the scanning table.
The National Osteoporosis Society (2001: 4) stated that ‘Low quantitative ultrasound (QUS) parameters are stronger predictors of low bone mass than clinical risk factors; individuals found to have low QUS parameters (as defined by machine-specific normative data) may either be referred for confirmation of the diagnosis by axial (preferably hip) BMD measurement or be advised to receive preventative therapy if other strong clinical risk factors are present’. The development of alternative screening devices has been recognised by the International Society for Clinical Densitometry (ISCD) to have value in undertaking screening in relation to fracture risk and recognising people who may benefit from require further diagnostics. The ISCD (2019) also note that, where possible, central DXA measurements at the spine and femur are preferred for therapeutic decision making and should be used but ‘if central DXA cannot be done, pharmacologic treatment can be initiated if the fracture probability, as assessed by heel QUS, using device specific thresholds and in conjunction with clinical risk factors, is sufficiently high’ (https://www.iscd.org/official-positions/2019-iscd-official-positions-adult/).
QUS can be used to undertake a scan of the os-calcis (heel) (Burke et al., 2017), and has several potential advantages including, no patient or operator exposure to ionising radiation, low cost and portability of equipment, making the screening accessible to people who may require to travel a long distance to access a DXA scan. Furthermore, measurements are typically accomplished in less than a minute, requiring no mechanical indexing or moving parts, making this type of screening more accessible to people with intellectual disabilities. This is particularly important given the well documented poor health outcomes for people with intellectual disabilities. As identified, an area often neglected or omitted on physical health checks is bone health with preventative services also under used (Srikanth et al., 2011; Truesdale and Brown, 2017).
Health screening for people with intellectual disabilities
To tackle these disparities, health care organisations can improve access to screening programmes and primary care to increase the detection of conditions that may have been unidentified. Access to earlier screening such as cervical screening and mammography has been shown to be successful in the identification of cancer risk and the need for further investigation among people with intellectual disabilities (Howeison and Clarke, 2013). However, challenges with communication difficulties between people with intellectual disabilities and staff, not knowing such screening programmes exist, lack of provision of appropriate easy to read material and obtaining informed consent can be difficult (Howeison and Clarke, 2013).
The need for increased opportunities for the delivery of accessible health promotion in local communities for people with intellectual disabilities has been highlighted internationally (Taggart and Cousins, 2014). In a review of the literature by Heller et al. (2014), health screening offered to people with intellectual disabilities was found to increase knowledge of the importance of screenings and the uptake of screenings while decreasing behaviours that challenge.
Providing access to a national screening programme for people with intellectual disabilities
The National Clinical Programme for Older People (NCPOP) is a joint initiative between the Directorate of Clinical Strategy and Programmes Division (CSPD) of the Health Services Executive (HSE) and the Royal College of Physicians of Ireland (RCPI). The overall aim of the programme is to improve the quality and efficiency of care for older people with complex healthcare needs. It brings clinical leadership to the heart of the decision-making process by working in partnership across services, with the aim of improving quality, access and value of healthcare (HSE, 2012).
Healthcare professionals in general, have a poor understanding of frailty (Gwyther et al., 2018; HSE, 2016a, 2016b). With this in mind, the NCPOP developed the National Frailty Education Programme (NFEP). The NFEP is a collaboration between the National Acute and Emergency Medicine Programmes, the Clinical Strategy and Programmes Division, Health Service Executive, in partnership with The Irish Longitudinal Study on Ageing (TILDA). The Intellectual Disability Supplement to this study, IDS-TILDA, ‘is a longitudinal study researching ageing in Ireland among people with an intellectual disability aged 40 and over’. (https://idstilda.tcd.ie). In developing the NFEP, expertise was sought from all nursing disciplines including nursing in the field of intellectual disability and one of the authors was nominated to represent the National Intellectual Disability Managers Association on the advisory group.
The opportunity to commence a service improvement initiative of peripheral bone density measurement in people with intellectual disabilities was provided as part of the NFEP, due to the involvement of some of the authors on this national group. Having attended the launch of the Wave 3 report of IDS-TILDA on behalf of the Director of the NCPOP, one of the authors learned of the benefits of peripheral BMD as a possible screening procedure for measuring bone mineral density in people with intellectual disabilities, who may have difficulty in successfully cooperating for or accessing DXA scan, for some of the reasons noted earlier (Burke et al., 2017; Frighi et al., 2014, 2019). It was believed that a service improvement initiative in relation to providing a peripheral BMD clinic would benefit people with intellectual disabilities in accessing health screening and health promotion and improve their bone health.
Heel scan clinic for people with intellectual disabilities
The heel scan clinic was a service improvement initiative, building on the work of the NFEP. It was a direct result of the collaboration between the authors who were involved in the NFEP and who contributed to the programme content that was being delivered across the Republic of Ireland. These links were developed through discussion with the interdisciplinary members of the NFEP, who were very keen on the pilot idea and embraced the concept of the heel scan clinic for people with intellectual disabilities in accessing health screening.
The heel scan clinics were organised in collaboration with the Disability Service Manager, Older Persons Service Manager, Disability Area Coordinator, and Clinical Nurse Managers. This project was undertaken as a service improvement project for people with intellectual disabilities. Following the provision of an outline of the project and how considerations of voluntary participation, informed and ongoing consent and anonymity were addressed, senior managers decided that formal ethical approval was not required for this service improvement project. To inform Clinical Nurse Managers and staff in General Practitioner services about the heel scan clinic, a PowerPoint presentation on bone health and information on the heel scan clinic and the heel scanner itself, along with supporting evidence-based literature, was provided in advance of the clinic being arranged.
To ensure the people with intellectual disabilities had the opportunity to make an informed decision about accepting or deciding not to accept the offer of a heel scan, the person with intellectual disabilities was provided with information about the heel scan clinic, in a manner accessible to them, and by a member of staff who worked with them, several days before the heel scan clinic was due to take place. The person only attended the clinic if they had initially agreed to attend the heel scan clinic and accepted the offer of a heel scan. To ensure the person with intellectual disabilities was still willing to have a heel scan, on the day of clinic, the heel scan procedure was demonstrated by a member of staff who had been trained in the use of the QUS Scanner. Any questions the person with intellectual disabilities had about the procedure were answered in a relaxed manner. The heel scan, was only performed after the continuing consent of the person with intellectual disabilities was confirmed on the day of the heel scan clinic.
All the people with intellectual disabilities invited to attend agreed to have a heel scan completed. One person with intellectual disabilities refused to have the alcohol conductor sprayed on their heel, but when offered, sprayed the alcohol onto their own heel and then were happy to proceed with the scan.
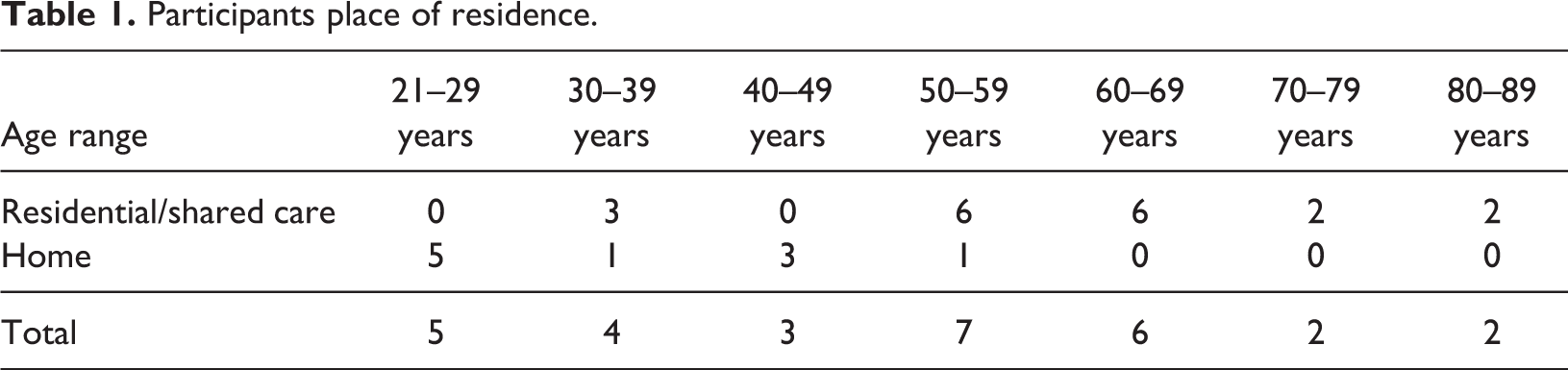
Thirty-one people with intellectual disabilities from residential care, shared care, respite and day services were invited to attend for this non-invasive baseline assessment. Twenty nine people availed of a heel scan (Table 1). The two people who did not avail of the scan were away from their accommodation at the time.
Participants place of residence.
As an approach to raise awareness among staff and family members about bone health, the people accompanying the person with intellectual disabilities also had the opportunity to have a heel scan. All availed of the opportunity for a heel scan which elicited further conversations about their own bone health and the bone health of people with intellectual disabilities.
Seventeen people were independently mobile, three were able to walk with support of another person and nine people used a wheelchair. To make the process of the heel scan more streamlined and reduce the time taken to perform the heel scan, the above data was entered into the heel scanner at the clinic, prior to the heel scan being undertaken. Information was also obtained from the person with intellectual disabilities as to whether they were on any current treatment for osteopenia or osteoporosis.
Findings
Of the 29 people with intellectual disabilities who had a heel scan completed, the age range was 21 years to 83 years. On completion of the clinics, and with the consent of the people with intellectual disabilities, the data was gathered and returned to the clinical nurse managers in each area; the result of the heel scan of each person with intellectual disabilities was sent to their GP. Some of the results were in line with treatment that had been prescribed by GPs but some of the results were unexpected (Table 2). Normal bone density is −1 or above, with osteopenia falling within the range of −1.1 to −2.5 and osteoporosis being a score of −2.5 or below. Measurements of bone density are reported using T-Scores which show how much lower or higher bone density is, compared with that of a healthy 30 year old adult. Although not widely used in the UK national health service (Finlayson et al., 2019), the WHO cut off points were designed as diagnostic thresholds and were not developed to provide criteria for selecting people forwhom to initiate therapy. Many clinicians use the WHO level for osteoporosis (T score ≤ −2.5) as the treatment intervention threshold (Siris et al. 2004).
Fragility risk screening results.
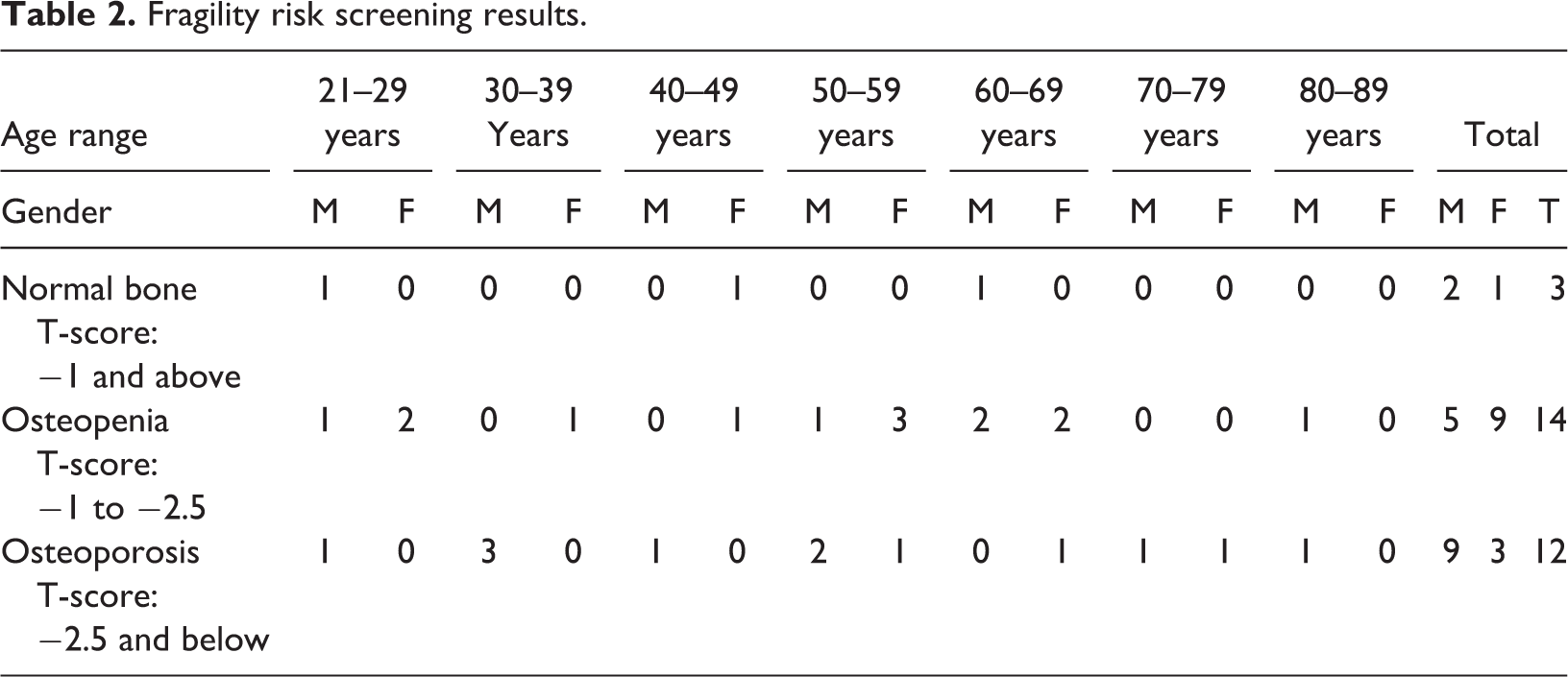
There were 12 females (23–74 years) and 17 males (21–83 years). Only 3 (10.3%) people with intellectual disabilities were in the normal BMD range, 14 (48.2%) were in the osteopenia range, 4 of whom were not on any treatment and 12 (41.3%) in the osteoporosis range, with 5 not on any treatment (Table 2). This also shows the extreme osteoporotic result of one person who was not on current treatment. This person had no ambulatory difficulties, nor were they exposed to polypharmacy, they had never sustained a fracture or smoked. This result was unexpected. Subsequent to the person’s information being shared by care staff with the person’s permission, their GP reviewed this information and the person was prescribed therapy based on the peripheral BMD results and referred for further diagnostic testing via DXA.
Discussion
This service development initiative, which facilitated locally accessible heel scanning for people with intellectual disabilities, provides further evidence of the need to raise awareness of bone health and its treatment among people with intellectual disabilities, their carers and families. The majority of participants (89%) in this service development were identified as having screening results indicating osteopenia or osteoporosis, including several people who would not have been identified on other clinical risk factors alone. These findings support the need for the development of this service and add to previous studies that used DXA scan to diagnose osteopenia or osteoporosis which also found the majority of participants had results indicating osteopenia or osteoporosis (Burke et al., 2017; Finlayson et al., 2019; Frighi et al., 2019). Due to the different methods of measurement, with a QUS scanner using the speed of sound and broadband ultrasound attenuation measurements, and the DXA scanner uses ionising radiation, the T-score provided when using a QUS heel scanner is not directly comparable to that from a DXA scan (Lewiecki and Lane, 2008). The score from the QUS scanner does provide a recognised indication of bone health, however, the QUS scores may be higher than those from a DXA scan and can provide a false reassurance of bone density, although an evaluated fracture risk may still be present (Lewiecki and Lane, 2008). Despite this, it is recognised that the QUS scanner has a role in identifying people who may be a low or high risk of osteoporotic fracture. The QUS scan results are screening results and need to be interpreted alongside the person’s wider clinical factors when deciding if further investigation with a DXA scan may be required (Hans and Biam, 2017).
Four people in the osteoporosis range were referred for DXA following sharing of the QUS results by their GPs. The authors’ vision for the heel scan clinics is to have this opportunity extended to all people with intellectual disabilities. Discussions are underway with senior staff about how to increase access to this important health screening opportunity and undertake a research study on this topic.
The high level of participation in the heel scan procedure among people with intellectual disabilities in this initiative suggests that the examination was acceptable to participants. The relative ease of accessing the heel scan locally also appears to have contributed to the success of the clinic. The high level of people who had screening results, indicating that they were within the osteopenia and osteoporosis range, reinforces the need for such screening opportunities to be provided to people with intellectual disabilities.
Importantly, the invitation extended to staff and family to avail of a heel scan gave them an opportunity to examine their own awareness of their bone health allowing for a broader understanding of the health needs of people with intellectual disabilities in their care. When staff are involved and feel that they too are being looked after (HSE, 2015), the conversation about bone health and improving the health outcomes for people with intellectual disabilities is likely to become a wider conversation. This can promote improved health awareness and changes in staff behaviour thereby improving health outcomes for themselves and for people with intellectual disabilities. The real success is in the actions that are taken following the scans, follow up with GP referrals, and getting access to treatment.
Implications for practice
The implications are that heel scans have good usability for screening a large number of adults with intellectual disabilities, even in non-clinical settings, because they are mobile. The use of heel scans were found to be acceptable to people with intellectual disabilities, particularly when their carers can be involved. Importantly, the results can influence the GPs decision to refer a person with intellectual disabilities for a DXA scan, which is the gold standard for diagnosis and has been shown to be accessible to the majority of people with intellectual disabilities when practical, reasonable adjustments are put in place (Finlayson et al., 2019).
More information on bone health should be provided to people with intellectual disabilities, family members and staff in services. Paper-based bone health screening tools may be used in some places as part of an overall annual health assessment for people with intellectual disabilities. However, it has been argued that commonly used screening tools such as ‘FRAX’, which is an assessment tool based on clinical risk factors with or without BMD tests (Kanis et al., 2008), are likely to be unsuitable as they do not consider the additional risk factors such as epilepsy, Down syndrome and immobility (Finlayson et al., 2019).
Heel scanning should be considered as part of annual health checks for people with intellectual disabilities. Equally, staff in services for people with intellectual disabilities should identify the arrangements within their area for BMD screening available to members of the general population, and work collaboratively with these services to facilitate access for people with intellectual disabilities. The heel scan clinic described in this paper is a prime example of what can be achieved through interdisciplinary collaboration.
Internationally, the importance of reasonable adjustments for people with disabilities is now high on the agenda of all health care providers to ensure equal access to healthcare for all. The peripheral bone mineral density heel scan clinic for people with intellectual disabilities is believed to be the first of its kind in Ireland, when it was conducted in 2018. It provided easy access to BMD screening for people with intellectual disabilities who otherwise would not be suitable for DXA. If the health care needs of people with intellectual disabilities are to be met in a prompt timely manner then their additional health risks and needs must be recognised, and access to health screening should be provided.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.