
Abstract
To investigate how having a child without a disability is related to maternal mental health and its predictors, we compared mothers of a single child with intellectual disabilities (single-child group, n = 117) and mothers of children with and without intellectual disabilities (multiple-children group, n = 457), in Japan. Compared to the multiple-children group, the single-child group had lower hope and social capital and poorer mental health; furthermore, 42.5% of them had decided not to have another child, despite desiring one. Hope was the strongest predictor of mental health in both groups but was more positively related to mental health in the multiple-children group. The fear of the possibility of the next child having a disability and receiving inadequate support were the obstacles for mothers who had decided not to have another child. Thus, greater support and more opportunities for obtaining adequate information about the implications of having another child may be needed.
Keywords
Introduction
Having another child after the birth of a child with an intellectual disability is not always an easy decision for mothers. Since children with intellectual disabilities often show behavioral problems and require long-term care and cost (Gallagher et al., 2008; Marchal et al., 2016; Nam and Park, 2017), their parents are more likely to have higher levels of stress, depression, anxiety, and poorer family functioning than those of children without disabilities (Dabrowska and Pisula, 2010; Gallagher et al., 2008; Hamlyn-Wright et al., 2007; Hedov et al., 2002; Marchal et al., 2016). The impact appears to be greater on mothers than on fathers (Azeem et al., 2013; Boström et al., 2011; Olsson and Hwang, 2006), likely because fathers are less likely than mothers to be more involved in their childcare (Dyer et al., 2009) and are more likely to continue their involvement in paid work (Olsson and Hwang, 2006). Thus, numerous studies have shown that having a child with an intellectual disability can increase the risks of stress, depression, and anxiety in mothers (Baker et al., 2003; Emerson, 2003; Gallagher et al., 2008; Hastings et al., 2006; McConkey et al., 2008; Olsson and Hwang, 2006: Singer, 2006).
Matsuoka et al. (2002) investigated the mothers of children with physical or intellectual disability in Japan, and reported that 32.9% of the mothers had past experience of being blamed by their husbands or other people for the child’s disability, while 54.3% of the mothers always or sometimes blamed themselves. Both of these experiences were correlated with depressive symptoms in mothers. Moreover, most mothers of children with intellectual disabilities appear to tackle the caregiving of such children on their own, even when they have multiple children with such disabilities (Kimura and Yamazaki, 2013). In the past, we conducted a qualitative study to explore mothers’ experiences of deciding on whether to have another child after the birth of a child with autism spectrum disorder (ASD). In that study, we found that uncertainty, recurrence risk, severity of disability, fears of putting a burden on later born children, the negative effects of any subsequent births on the children with disabilities, altering marital relationships, and lack of social support and social acceptance were major obstacles to having another child without disabilities (Kimura et al., 2010). Therefore, in Japan, having another child can be exceedingly difficult for some mothers of children with disabilities.
Research on the fathers of children with intellectual disabilities has been less than that on mothers, but the importance of involvement of fathers in childcare has been emphasized (Boström and Broberg, 2014; Davys et al., 2017; Flippin and Crais, 2011; MacDonald and Hastings, 2010). Hastings et al. (2005) considered that fathers are seen to be less affected than mothers because they may have different coping strategies including the avoidance of children and engagement in other activities unrelated to childcare. Davys et al. (2017), in their review, explained three aspects of fathers’ work by examining the impact of a child with an intellectual disability on work (e.g. reducing earnings and losing opportunity), the impact of work on fathers’ caregiver role (e.g. fewer opportunities for getting involved in caregiving tasks), and that the work can also have functions other than fulfilling the role of a father (e.g. work can be used as a coping strategy). In short, fathers’ work can be considered a coping strategy as well as a barrier to getting involved in childcare. However, the studies have shown that fathers’ involvement in intervention programs for children with intellectual disabilities/ASD benefits mothers (May et al., 2013) as well as their children (de Falco et al., 2008; Flippin and Crais, 2011). Therefore, increasing father involvement in caregiving should be expected, especially, it is important for mothers who desire to have further children.
Of course, having a child with an intellectual disability has numerous positive effects on family members. According to Beighton and Wills (2017), the commonly mentioned positive aspects of parenting their child with intellectual disabilities were as follows: an increased sense of personal strength and confidence, changed priorities, greater appreciation of life, pleasure in the child’s accomplishments, increased faith/spirituality, more meaningful relationships, and the positive effect that the child has on the wider community. In addition, evidence shows that parents of children with intellectual disabilities/ASD have positive perceptions that coexist with anxiety and depression, and these mothers reported more depression and more positive perceptions than fathers did (Hastings et al., 2005; Vilaseca et al., 2014). Further, two studies that analyzed a birth cohort (Totsika et al., 2011a) and national survey data (Totsika et al., 2011b) in the United Kingdom revealed that positive maternal mental health and positive well-being do not differ among mothers of children with intellectual disabilities, mothers of children without intellectual disabilities, and mothers of children with ASD. These results imply that even though mothers of children with intellectual disabilities have higher stress, this does not directly decrease maternal well-being. Similarly, we previously examined the perceived positive changes among parents of school-aged children with intellectual disabilities and found that 79.9% of them reported a positive change in their lives, self, and relationships with others following the diagnosis of their children’s disabilities despite almost half of them reporting clinical levels of mental health symptoms (Kimura and Yamazaki, 2014; 2016a). Thus, there is a need to consider how positive perceptions and positive experiences can be promoted among parents of children with disabilities.
Hope
Hope is considered an effective resource for alleviating stress and improving perceptions of positive change among mothers of children with intellectual disabilities. Hope can be defined as both having a specific goal and one’s perceived ability to reach that goal (Lloyd and Hastings, 2009). It is positively related to psychological well-being, a construct comprising facets of positive affect, emotional ties, and life satisfaction (Shorey et al., 2007). Later on, Lloyd and Hastings (2009) studied 138 mothers and 58 fathers of children with intellectual disabilities and found that hope predicted greater psychological well-being and decreased psychological distress. Kausar et al. (2003), in a qualitative study, interviewed 19 parents of children with disability (e.g. Down syndrome, autism) and found that hope could be conceptualized as a dynamic process of positive transformation that helps support parents in reframing their lives in light of the experience of having a child with special needs. Similarly, as we have already mentioned, some Japanese mothers of a child with ASD desired to have another child, despite the various obstacles that they faced in doing so (Kimura et al., 2010). These mothers expressed having a future (healthy) child as “hope.” Therefore, having another child without disability might be considered as a factor leading to increased hope among mothers of children with intellectual disabilities.
Social capital
Of the various environmental factors that influence the family of children with intellectual disabilities, social capital may be one of the most important. Social capital is defined as the degree of connectedness and the quality and quantity of social relations (Harpham et al., 2002). It is related to the mental health of mothers of children with disabilities. For example, Kojo and Fukumaru (2015) investigated depression and its related factors in 208 fathers and 257 mothers of children with spina bifida in Japan, and reported that higher social capital was associated with a lower risk of depression in mothers. We examined the perceived positive changes in mental health and its predictors using the Double ABCX model (McCubbin and Patterson, 1983) and confirmed that social capital predicted perceived positive changes among mothers of school-aged children with intellectual disabilities (Kimura and Yamazaki, 2016b). In Japan, most children with intellectual disabilities enrolled in special-needs schools oriented toward intellectual disabilities. However, there are a limited number of such schools, and they are not always located near children’s living areas, which may cause the children to become isolated from their local community. By contrast, general public schools enroll typically developing children who live in the immediate area and organize various activities within the local community. Because of this, mothers of children with and without disabilities might have greater opportunities to participate in the local community, thereby leading to a more positive perception of social capital.
The present study
Although there is a global body of research on the impacts of children with intellectual disabilities on families, there is very little research on the effects of having another child without disabilities on such families. As noted above, hope is related to the psychological well-being of parents of children with intellectual disabilities (Lloyd and Hastings, 2009), while having children without disabilities can be regarded as a symbol of “hope” for mothers of children with intellectual disabilities (Kimura et al., 2010). Accordingly, having another child without disabilities might improve the psychological well-being of such mothers. It might also improve these mothers’ community involvement and perceived social capital, both of which might be related to better mental health. If these hypotheses are correct, then there would naturally be differences in hope, social capital, and mental health between mothers of a single child with an intellectual disability and mothers of children with and without intellectual disabilities. In other words, what are the differences between mothers of a single child with an intellectual disability and mothers of children with and without intellectual disabilities? Do mothers of a single child with an intellectual disability have less hope and social capital and poorer mental health than do the mothers of children with and without intellectual disabilities? If so, how do we improve the situation of mothers of a single child with an intellectual disability?
In the present study, we answered these questions by comparing mothers of a single child with intellectual disabilities (single-child group) and those of children with and without intellectual disabilities (multiple-children group). The following specific points were explored: Differences in the general characteristics, hope, social capital, and mental health between these two groups. Differences in the main predictors of mental health between the two groups. The obstacles to having another child after the birth of a child with intellectual disabilities.
Methods
Procedure and participants
This study was conducted from February through March 2011. Participants were mothers of children with intellectual disabilities aged 19 years or younger and residing in Tokyo. With the cooperation of the presidents of parent–teacher associations (PTAs) in 10 special-needs schools (elementary, junior high, and high schools), we distributed a questionnaire and a self-addressed return envelope to 1645 parents/guardians and received their answers through postal mail. The response rate was 40% (n = 666). Of these, we chose 574 mothers (117 mothers in the single-child group and 457 mothers in the multiple-child group) for this study. The children’s disorders were categorized as “ASD” (including developmental delay) and “Down syndrome/other intellectual disabilities” (including cerebral palsy and other chromosomal anomalies but excluding ASD). Inclusion criteria for the mothers were having a child who is living in Tokyo and being formally certified by municipal organizations as having an intellectual disability (regardless of the type or severity) or who has a medical certificate of intellectual disability.
Research instruments
The questionnaire assessed the following general characteristics of the mothers: mothers’ age, employment, marital status, educational level, and decision about having another child; the number of children with disabilities in the home; and children’s gender, age, siblings, and the type of disability.
Hope
We used the Japanese version of the Herth Hope Index (HHI; Herth, 1992; translated into Japanese by Yamaki and Yamazaki, 2005). The HHI consists of 12 items rated on a 4-point Likert scale ranging from 1 (“strongly disagree”) to 4 (“strongly agree”). A higher score indicates a greater presence of hope. Example items on this questionnaire include “I have a positive outlook toward life” and “I can recall happy/joyful times.” The Cronbach’s α for this study was 0.891.
Social capital
To assess social capital, we used the subjective social capital scale (Togari, 2006). The scale has six items, which comprises three subscales of two items each: “collective efficacy,” “psychological sense of community,” and “neighbourhood cohesion.” Example items in this scale include, “This neighbourhood has a friendly atmosphere; we take care of others’ homes when they are away” (neighborhood cohesion) and “Our neighbours are willing to help others who need support” (psychological sense of community). The items were rated on a 5-point scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). A higher total score indicated greater social capital. The Cronbach’s α of this study was 0.81 (M = 18.09, SD = 4.53).
Mental health
To assess mothers’ mental health, we used the Japanese version of the 12-item General Health Questionnaire (GHQ-12; Goldberg, 1972; translated into Japanese by Nakagawa, 1981). Example items on this questionnaire include, “Have you recently been able to concentrate on whatever you’re doing?” and “Have you recently lost sleep due to worrying?” Items are rated on four response options: 3 (“much more than usual”), 2 (“rather more than usual”), 1 (“no more than usual”), and 0 (“not at all”). Higher scores indicate poorer mental health. The Cronbach’s α of the GHQ-12 in this study was 0.897.
Obstacles to having the next child
Based on a previous qualitative study, wherein I interviewed 39 mothers of children with intellectual disabilities in Japan (Kimura, 2012), we created a questionnaire including 10 items that assess mothers’ fears and difficulties in relation to having another child after the birth of a child with an intellectual disability. Example items in this questionnaire include the “possibility of the next child having a disability” and “possibility of not being able to sufficiently take care of the child with intellectual disabilities.” All items are scored as 1 (“yes”) or 0 (“no”).
Data analysis
We used SPSS Statistics for Windows (IBM Corp., Armonk, NY, USA) for all statistical analyses. All statistical tests were two-tailed. First, to compare mothers’ characteristics and main variables between the single-child and multiple-children groups, we used Pearson’s χ2 tests and t tests. Second, to confirm the relationships between mothers’ mental health and its related factors, Pearson’s correlation coefficients were used for quantitative variables. By contrast, categorical variables were transformed into binary variables, which we then assessed using point-biserial correlations (quantitative variable × binary variable) or the phi coefficient (binary variable × binary variable). Third, to confirm the relationships between mental health (the dependent variable) and the various predictors that were significant in the correlational analysis, a hierarchical regression analysis was performed. Finally, after identifying mothers who decided not to have another child despite desiring one, we compared mothers’ specific fears and difficulties between the single-child and multiple-children groups using Pearson’s χ2 tests or Fisher’s exact tests.
Ethical considerations
The proposal for this study was preapproved by the institutional review board, the Department of Medicine at the University of Tokyo.
Results
Differences in the characteristics of mothers and main variables
The differences in the characteristics and main variables between the single-child and multiple-children groups are shown in Table 1. Both mothers and children were younger in the single-child group than in the multiple-children group. Furthermore, the single-child group had higher GHQ-12 scores, a higher proportion of mothers who were “currently not married,” and a higher proportion of children who were diagnosed with “ASD.” The single-child group also had significantly lower hope and social capital. The desire to have another child differed between the groups: 48 (42.5%) and 40 (8.9%) mothers in the single-child and multiple-children groups, respectively, had decided not to have another child despite their desire to have one.
General characteristics of the single-child and multiple-children groups.
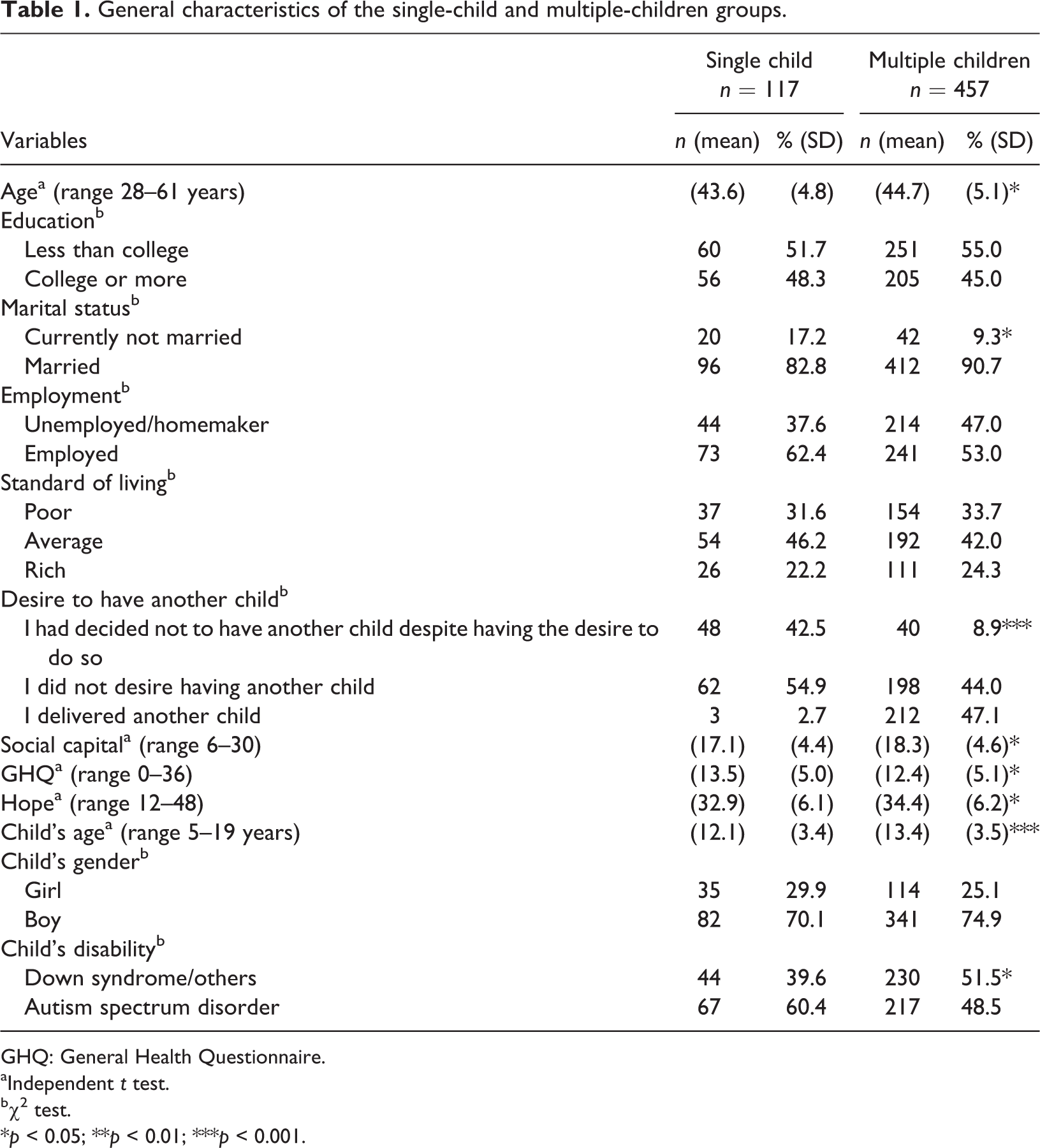
GHQ: General Health Questionnaire.
aIndependent t test.
bχ2 test.
*p < 0.05; **p < 0.01; ***p < 0.001.
Correlation between mental health and each variable
To assess the factors related to their mental health, we examined the correlations between the GHQ-12 score and child’s age, sex, disability type, mother’s educational level, marital status, employment, standard of living, the decision not to have another child, social capital, and hope. In the single-child group (Table 2, above the diagonal), the GHQ-12 scores were positively correlated with child’s disability type (ASD, r = 0.205, p < 0.05) and employment (unemployed/homemaker, r = 0.212, p < 0.05), while they were negatively correlated with hope (r = −0.433, p < 0.01). On the contrary, GHQ-12 and social capital did not show a significant correlation. However, social capital was positively correlated with hope (r = 0.322, p < 0.01).
Correlations between child’s characteristics, mothers’ characteristics, hope, and mental health in the single-child (above diagonal) and multiple-children groups (below diagonal).a
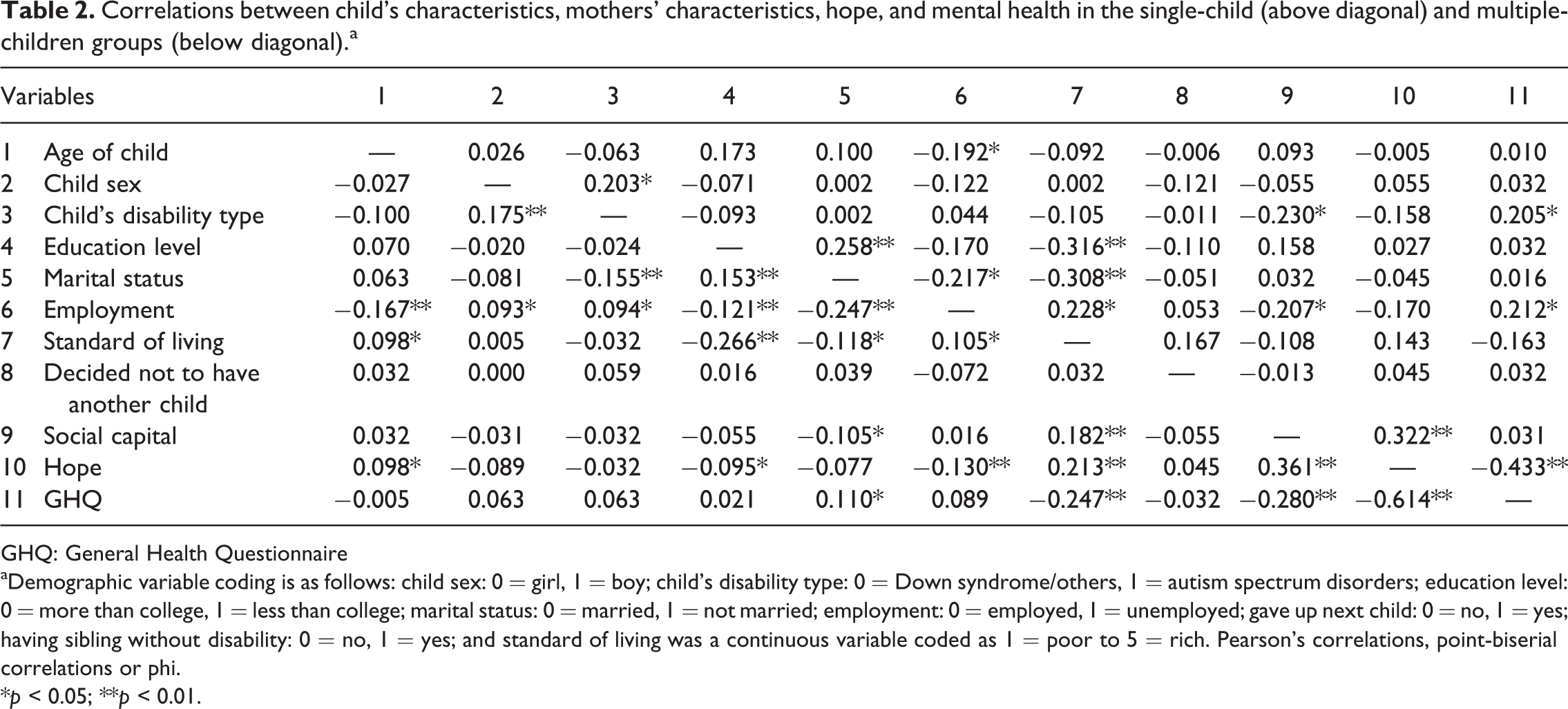
GHQ: General Health Questionnaire
aDemographic variable coding is as follows: child sex: 0 = girl, 1 = boy; child’s disability type: 0 = Down syndrome/others, 1 = autism spectrum disorders; education level: 0 = more than college, 1 = less than college; marital status: 0 = married, 1 = not married; employment: 0 = employed, 1 = unemployed; gave up next child: 0 = no, 1 = yes; having sibling without disability: 0 = no, 1 = yes; and standard of living was a continuous variable coded as 1 = poor to 5 = rich. Pearson’s correlations, point-biserial correlations or phi.
*p < 0.05; **p < 0.01.
In the multiple-child group (Table 2, below the diagonal), the GHQ-12 scores were positively correlated with marital status (currently not married, r = 0.110, p < 0.05) and negatively correlated with the standard of living (higher scores indicate higher standard of living, r = −0.247, p < 0.01), social capital (r = −0.280, p < 0.01), and hope (r = −0.614, p < 0.01). Unlike the single-child group, there were no significant correlations among the GHQ-12 score, child’s disability type, and employment status in the multiple-children group. The decision to not have another child was not correlated with any of the other variables, including hope and mental health.
Predictors of mothers’ mental health
Based on the results of the correlation analysis, we regarded child’s disability, employment, marital status, standard of living, social capital, and hope as potential predictors of mothers’ mental health. We then conducted a hierarchical multiple regression analysis, entering the predictors of mental health in the following order: (1) child’s disability type, employment, marital status, and standard of living; (2) social capital; and (3) hope. Tables 3 and 4 and Figures 1 and 2 show the results. If the β values in the model had a minus sign, the variable was considered to be related to better mental health. Among mothers of the single-child group, having a child with ASD, being unemployed or a homemaker, and social capital were all positively related to the GHQ-12 scores (step 3). Furthermore, hope was negatively and significantly related to the GHQ-12 scores (p < 0.001). This final model explained 25.3% of the variance in mothers’ mental health. Conversely, in the multiple-children group, being currently not married and being unemployed or a homemaker were positively related to the GHQ-12 scores, and the standard of living and social capital were negatively related to the GHQ-12 scores (steps 1 and 2). However, after entering “hope,” the relationships for marital status, employment, and social capital were not seen (step 3). In step 3, hope was negatively and significantly related to the GHQ-12 scores. This final model explained 39.9% of the variance in mothers’ mental health.
Hierarchical regression analysis predicting mental health (single-child group).a
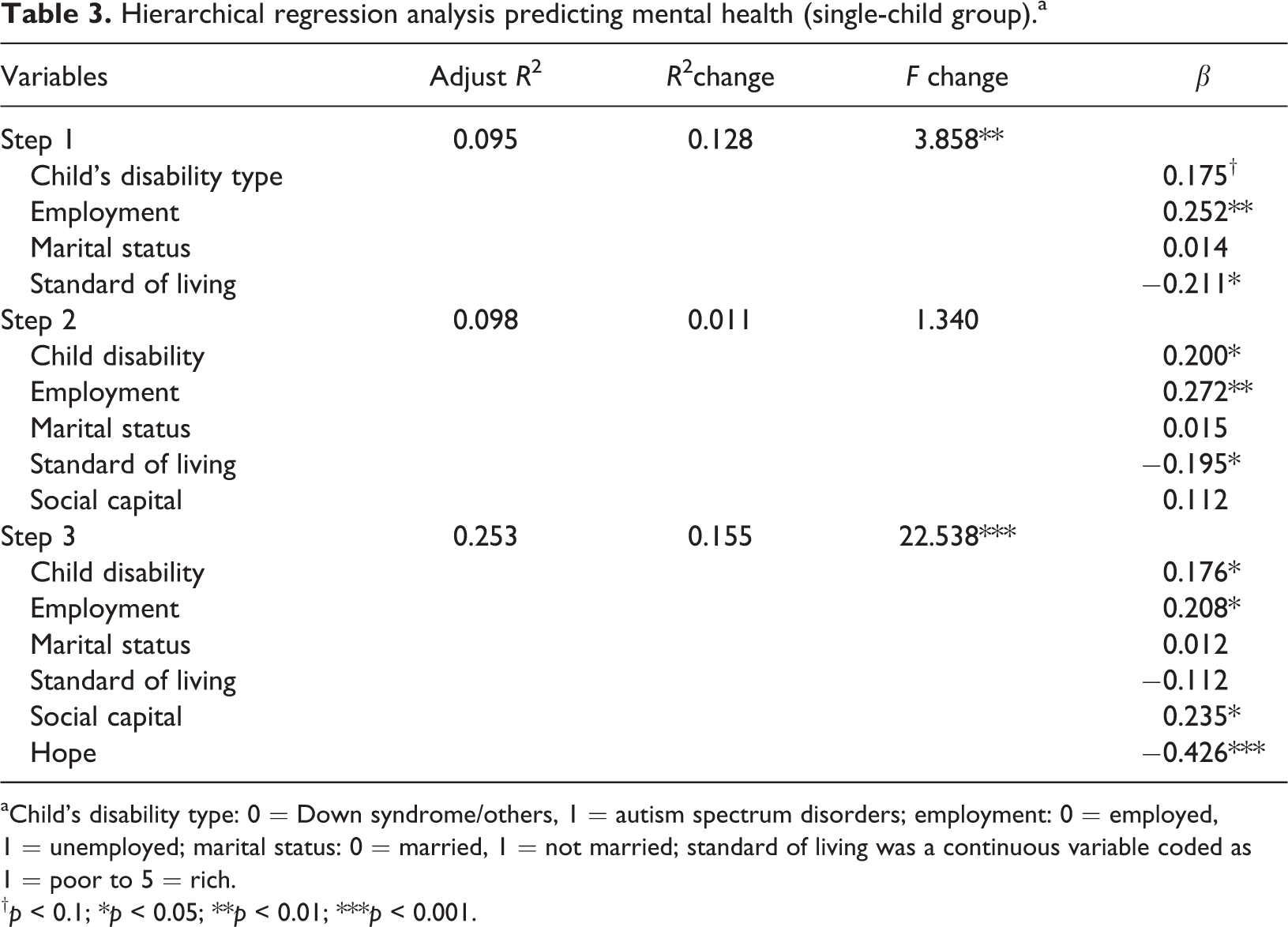
aChild’s disability type: 0 = Down syndrome/others, 1 = autism spectrum disorders; employment: 0 = employed, 1 = unemployed; marital status: 0 = married, 1 = not married; standard of living was a continuous variable coded as 1 = poor to 5 = rich.
†p < 0.1; *p < 0.05; **p < 0.01; ***p < 0.001.
Hierarchical regression analysis predicting mental health (multiple-children group).a
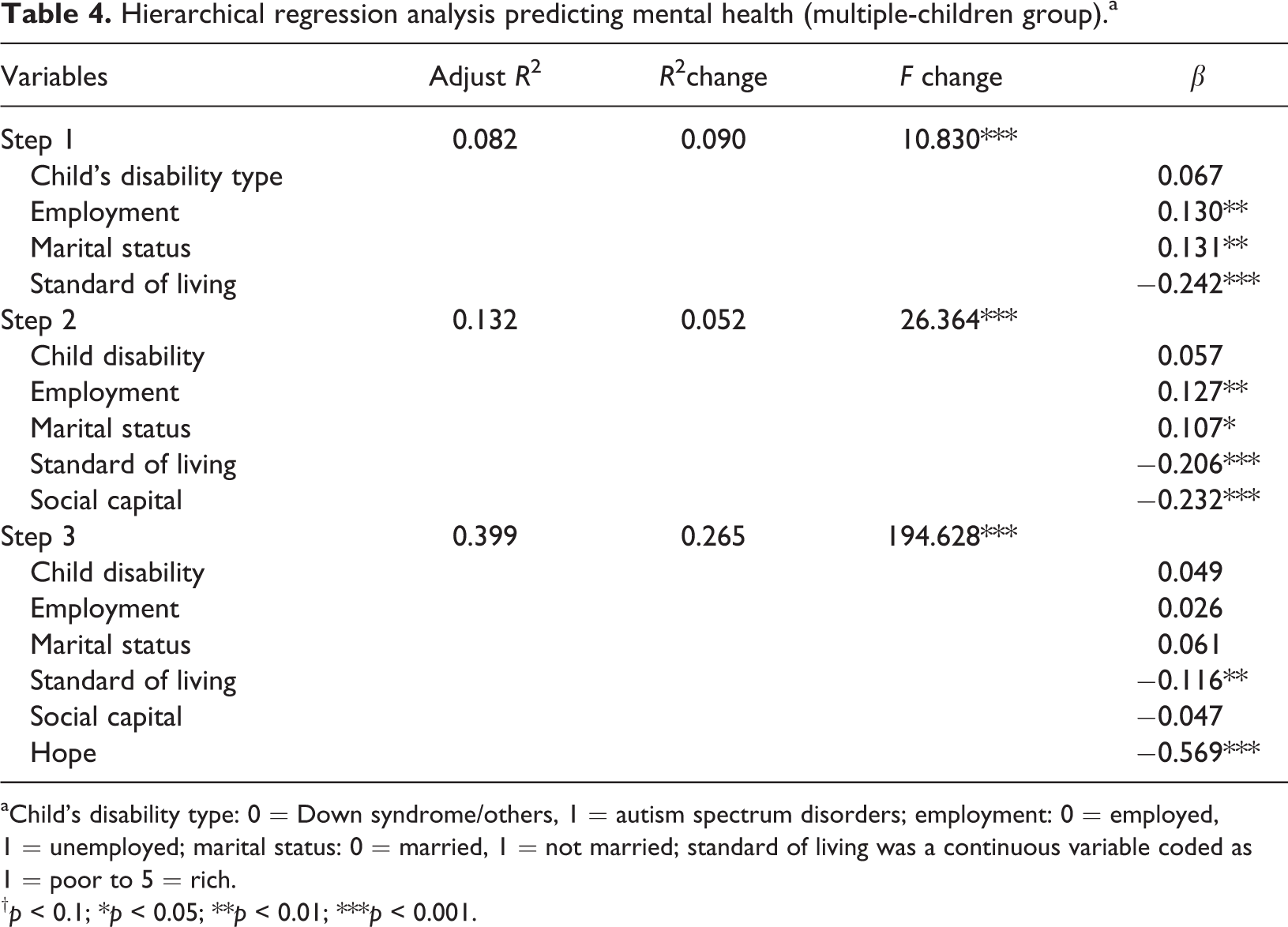
aChild’s disability type: 0 = Down syndrome/others, 1 = autism spectrum disorders; employment: 0 = employed, 1 = unemployed; marital status: 0 = married, 1 = not married; standard of living was a continuous variable coded as 1 = poor to 5 = rich.
†p < 0.1; *p < 0.05; **p < 0.01; ***p < 0.001.
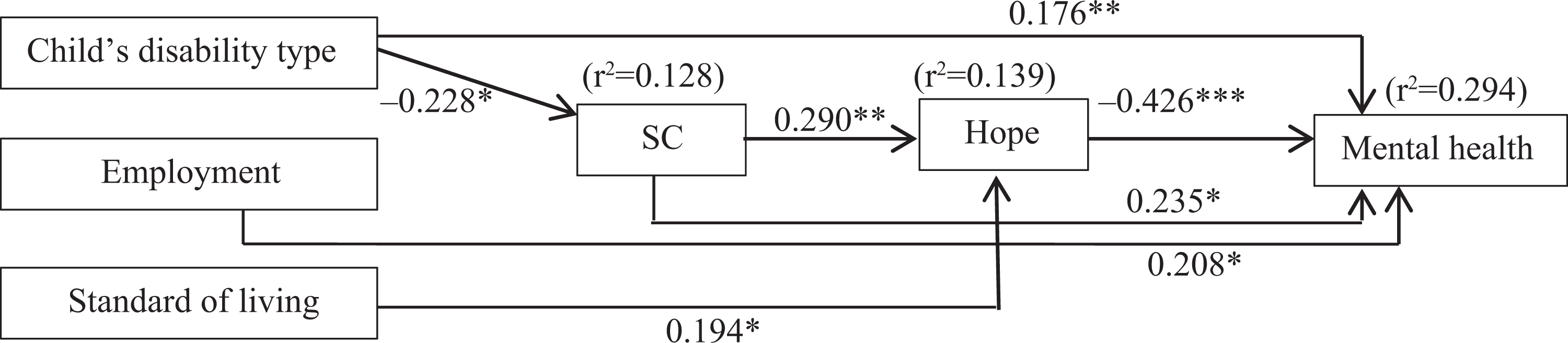
The significant predictors of mental health using β values from hierarchical multiple regression (single-child group).
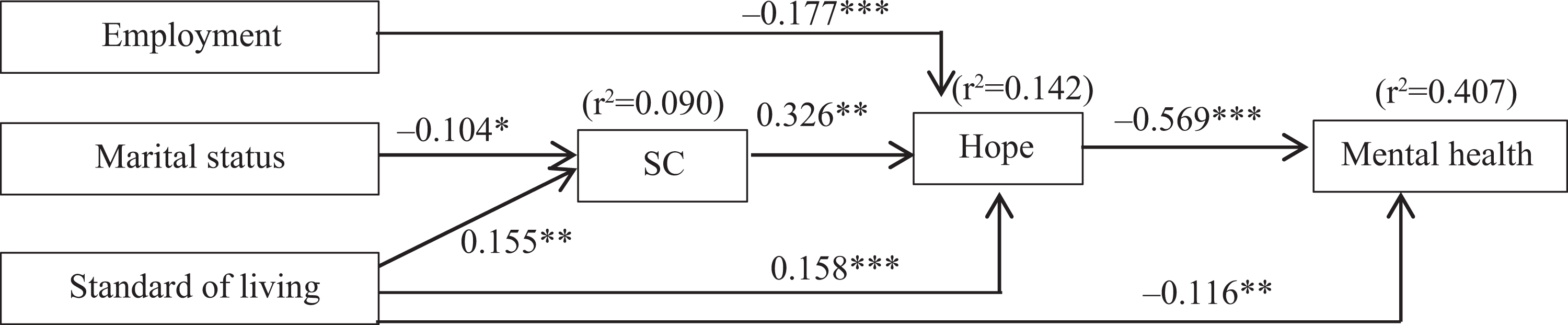
The significant predictors of mental health using β values from hierarchical multiple regression (multiple-children group). Standard partial regression coefficients (β) are presented, *p < 0.05, **p < 0.01, ***p < 0.001. r2: coefficient of determination. SC: social capital; child’s disability type: 0 = Down syndrome/others, 1 = autism spectrum disorders; marital status: 0 = married, 1 = not married; employment: 0 = employed, 1 = unemployed; and standard of living was a continuous variable coded as 1 = poor to 5 = rich.
Obstacles to having another child
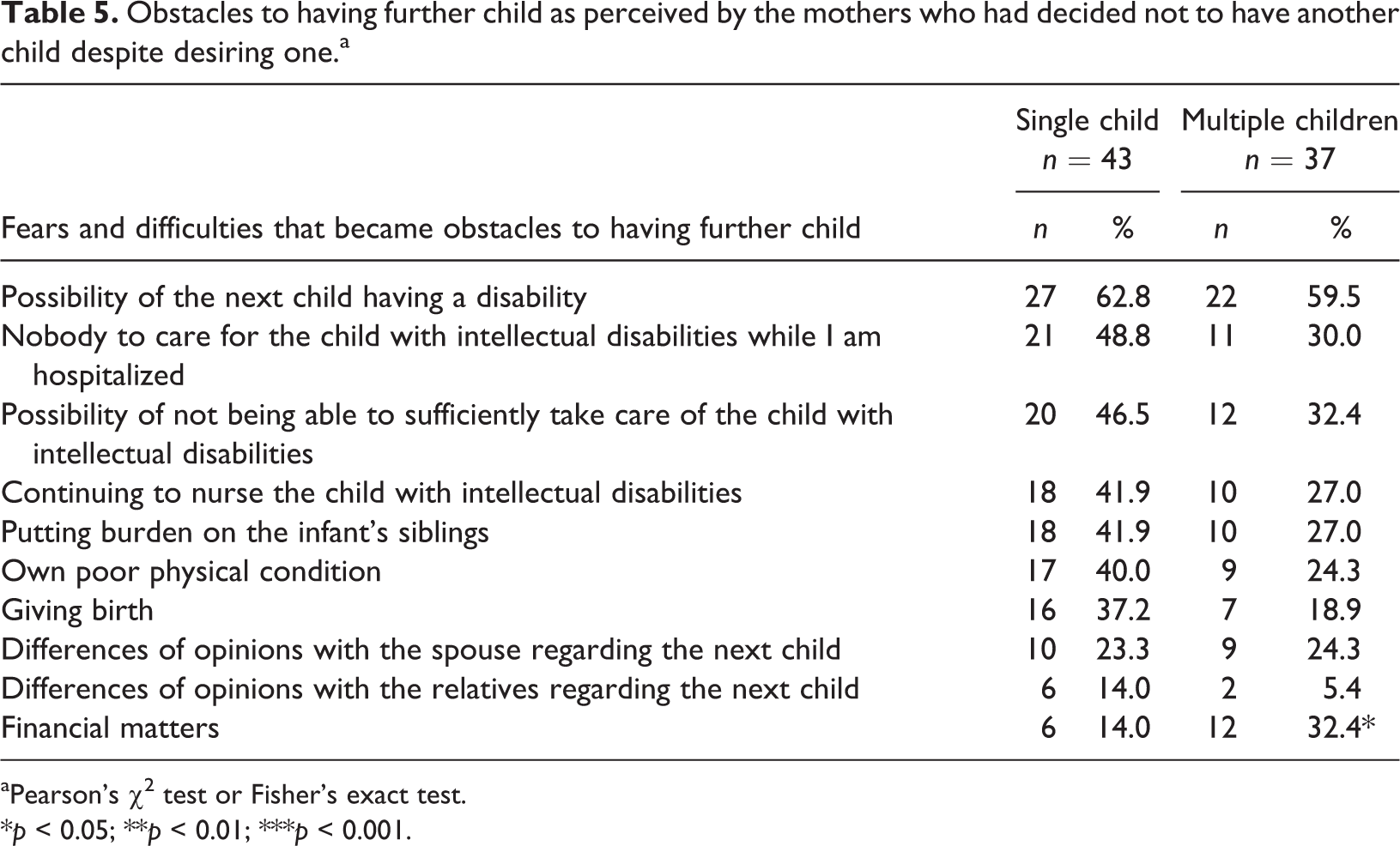
To obtain a better understanding of how to improve the situation for mothers who had decided not to have another child after the birth of a child with intellectual disabilities, we focused only on these mothers in this analysis. Specifically, we described and compared the obstacles to having another child in the single-child and multiple-children groups (Table 5). For both groups, the most commonly reported fear was the “possibility of the next child having a disability” (62.8% in single-child group and 59.5% in multiple-children group). While the differences were not significant, a greater proportion of mothers in the single-child group reported having the following fears/difficulties: “nobody to care for the child with an intellectual disability while I am hospitalized” (48.8%), “possibility of not being able to sufficiently care for the child with an intellectual disability” (46.5%), “continuing to nurse the child with an intellectual disability” (41.9%), “putting burden on the infant’s siblings” (41.9%), and “own poor physical condition” (40.0%). We found a statistically significant difference between the groups only for “financial matters” (p < 0.05): the multiple-children group was more likely to report financial difficulties (32.4%) than the single-child group (14.0%).
Obstacles to having further child as perceived by the mothers who had decided not to have another child despite desiring one.a
aPearson’s χ2 test or Fisher’s exact test.
*p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
In this study, we compared the mental health and its related factors between mothers of a single child with intellectual disabilities and mothers of multiple children with and without such disabilities. First, compared to the multiple-children group, the mothers of the single-child group tended to be younger, currently not married, have poorer mental health status, have less hope, have younger children with intellectual disabilities, and have children with ASD. These results have various explanations. Since the mothers in the multiple-children group had raised two or more children, they were more likely to be older than mothers of a single child with intellectual disabilities. Additionally, younger mothers are more likely to have younger children. It should be noted that being single while caring for a child with intellectual disabilities might make it difficult for mothers to have another child. Moreover, around 60% of the mothers in the single-child group had children with ASD, which tends to be characterized by more behavioral problems than, for example, children with Down syndrome; this might also make it more difficult for them to have another child. This difficulty in having another child, coupled with the above factors, may cause these mothers to have less hope.
Second, 42.5% of the mothers in the single-child group had decided not to have another child after the birth of a child with intellectual disabilities despite having the desire to have another child. The main obstacles to them having another child, according to their reports, were a fear of the next child having a disability and lack of support (e.g. finding someone to take care of the child with intellectual disabilities while the mother is hospitalized). In our previous qualitative study (Kimura et al., 2010), recurrent risks and a lack of social support were the key factors that led mothers of children with ASD to hesitate to have another child; thus, the results of the present quantitative study support the findings of our previous qualitative study. Available family support in Japan tends to be rather limited, and 99.8% of all births take place in a hospital or clinic (the average period of hospital admission for childbirth is approximately 1 week). These factors appear to have influenced the decision of mothers of children with disabilities to have a second pregnancy (Kimura et al., 2010).
These same difficulties were found among mothers in the multiple-children group, but they appeared to be more worried about financial matters. This is natural because raising more children—both with and without disabilities—exerts a greater financial burden on families than having a single child. To alleviate the burden on these mothers’ decision-making related to their next child, flexible support systems, including care for the children with intellectual disabilities and newborn babies, might be needed. Unfortunately, there is not yet a simple solution for reducing the fear related to the possibility of the next child having a disability; however, providing opportunities to obtain adequate information about the possible risks for the next infant might be helpful. Additionally, even if mothers do end up giving birth to another child with a disability, their lives might be somewhat improved due to more opportunities to meet with people who can share their burden (Kimura and Yamazaki, 2013). Thus, involving peer groups and providing information on available social support might be useful.
Third, the decision to not have another child might be an exceedingly stressful experience for mothers; nevertheless, it was not correlated with hope or mental health in either group. It is possible that mothers’ struggle to care for the child with an intellectual disability might alleviate their desire to have another child, or perhaps make it easier for them to adapt to their decision. Mothers’ current situation (i.e. raising a single child with intellectual disabilities or multiple children with and without such disabilities) seems to be a better predictor of their hope, social capital, and mental health.
Fourth, social capital seemed to have the opposite role for mothers in the single-child and multiple-children groups. In the former group, social capital was positively related to mental health (β = 0.235, p < 0.05) in step 3 of the hierarchical regression analysis, suggesting that higher social capital is related to poorer mental health for mothers in the single-child group. Although there was no significant association between mental health and social capital (β = 0.112) in step 2, after entering hope, its relations became significant. This may be considered a result of the impact of hope. The mothers in this group might not have many opportunities to participate in community activities or might be isolated within their neighborhood; thus, perceived higher social capital might not be related to better mental health. Conversely, among mothers of the multiple-children group, social capital was negatively related to mental health in step 2 (i.e. higher social capital was related to better mental health), but the relationship was not seen after hope was entered (in step 3). This might suggest that social capital is indirectly related to mental health via hope in the multiple-children group. It is thus possible that raising children without intellectual disabilities might increase mothers’ opportunities to become involved with and connected to their community, which in turn might improve perceived social capital and, thereby, hope. These improvements may in turn enhance mental health.
Fifth, this study showed that hope was the strongest predictive factor of mental health among mothers of children with intellectual disabilities. Similarly, Lloyd and Hastings (2009) found that lower levels of hope predicted depression among mothers of children with intellectual disabilities. Notably, the impact of hope was stronger in the multiple-children group (β = −0.569, p < 0.001) than in the single-child group (β = −0.426, p < 0.001). If mothers of a single child with intellectual disabilities have the desire to have another child, it is important that they fulfill their wishes, because it might increase their hope and, consequently, their mental health. If these mothers do not wish to have another child or decide not to have another child with the notion of doing so, it might be useful to provide them with a community-based informal support. Doing so might increase their social network and trust, which in turn might increase their social capital and promote hope. Indeed, hope was positively correlated with social capital, likely because having high social capital (e.g. living in a neighborhood with a helpful atmosphere) can increase mothers’ hope. On the contrary, for mothers of multiple children with and without intellectual disabilities, it might be necessary to provide them with the support for their children without disabilities, such as creating a peer group using social pedagogy (Carter et al., 2016).
Finally, professionals who work with mothers of children with intellectual disabilities can act as a liaison between mothers of children with intellectual disabilities and peer groups, communities, and other professionals. Midwives, obstetricians, pediatricians, and public health nurses can address regional parents’ associations of children with intellectual disabilities or create opportunities to meet peers early stage (e.g. adjusting the schedule for mothers of children with disabilities who visit the hospital for their children’s checkup so that these mothers can get the opportunity to meet and interact with other mothers of children with disabilities). This may reduce the feelings of isolation among mothers of children with intellectual disabilities and facilitate them to collect information about disabilities and support systems. Especially, talking to other mothers who have children both with and without disabilities may be useful for mothers of single child with disability, who want to have another child.
Similarly, if mothers appear to be worrying about the possibility of the next child having a disability, professionals can positively introduce the mothers to genetic counselors. Recently, genetic counseling systems have been developed in Japan, although it is regarded as being 30 years behind the United States and not fully recognized among the general population and also among medical practitioners (Kawame, 2014). In addition, prenatal screening rates were very low (approximately 5.3%) in 2013 (Sasaki, 2015), although 26.9% of the childbirths in 2013 were given by mothers aged over 35 years (Ministry of Health, Labour and Welfare, 2014). Since there is no national policy for prenatal screening, and physicians are not required to provide information about prenatal screening (Sasaki et al., 2011) and sibling recurrence risk (Kimura et al., 2010), mothers of children with disabilities may have difficulties obtaining certain information about the risks of the next child. Thus, understanding the existence of genetic counselors and how to contact them may be one of the ways to alleviate mothers’ fear.
This study has several limitations. First, we used a simple categorization of children’s disability as ASD or other intellectual disabilities (including Down syndrome), but this might not be sufficient for assessing its relationship with mothers’ mental health. Indeed, the severity of children’s disability and behavior problems might relate to mothers’ mental health (Herring et al., 2006; McConkey et al., 2008) and could relate to their decision-making about having another child. Thus, the relationship among these factors should be investigated in a future study. Second, this study was conducted in metropolitan Tokyo, which is suffused with medical services and social welfare facilities. Thus, it might be necessary to investigate this topic in rural areas of Japan. Third, the decision to have or not have another child might be better described through in-depth interviews. Although we previously revealed the difficulties that mothers face in relation to having a second child after giving birth to a child with ASD (?Kimura et al., 2010), it did not include other intellectual disabilities. Thus, how these difficulties might differ by the type of disability could be described in a future study.
In conclusion, this study examined the differences between mothers of a single child with intellectual disabilities and mothers of multiple children with and without intellectual disabilities. Furthermore, we revealed the obstacles that both mothers of a single child and mothers of multiple children perceive when having another child. Removing the obstacles to having another child might be important for mothers who would like to have one. Therefore, it is necessary to explore what mothers, especially the mothers of a single child (who are a particularly vulnerable population), would require in order to alleviate their fears about having another child.
Footnotes
Acknowledgements
The authors thank all the mothers who participated in this research and the PTAs in the 10 ID-oriented special-needs schools that participated. The authors also thank Dr Yuki Yonekura for his constructive comments.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI (grant nos. JP 26380716, JP17H02612) and the Mitsubishi Foundation.