
Abstract
Objective
Our goal was to assess how many chronic pain patients seek psychological treatment for their condition and what psychological and demographic characteristics are associated with that decision.
Methods
The association between pain intensity, quality of life and psychological treatment seeking was tested in two hypothetical models which differed according to beliefs about either external or internal control over pain.
Results
A minority of patients had experience with psychological treatment of chronic pain. Patients who had that experience were younger, suffered from more intense pain, and applied many more coping strategies than patients who never tried this kind of treatment. Intense pain and low quality of life motivated chronic pain patients to seek psychological treatment only if they believed that doctors could control their pain.
Discussion
The study results stress the importance of diversifying the methods used to treat chronic pain and educating patients about the benefits of psychological treatment. Low numbers of chronic pain patients who take advantage of psychological treatment indicate that encouragement from medical professionals might be necessary.
Keywords
Introduction
Medical interventions often prove ineffective in the treatment of chronic pain (CP).1–10 On the other hand, recent meta-analyses confirm that psychological treatment (PT) might be an effective alternative.11–14 PT researched in the literature typically consists of either cognitive-behavioural therapy, mindfulness-based stress reduction, or acceptance and commitment therapy, delivered in a group format11,13,14 by a mental health specialist (usually a psychologist). Some research also examined applications such as mHealth or eHealth. 12 All the abovementioned treatments include pain assessment, education about the mechanisms of CP, and psychological interventions such as cognitive restructuring, behavioural activation, relaxation techniques, and acceptance of pain.
A few studies have examined the use of PT in the population of CP patients,15,16 but none of them looked at psychological factors associated with PT seeking. Establishing what motivates CP patients to seek PT could be helpful to pain specialists when advising their patients on the best course of treatment.
In previous studies on CP patient populations, medical treatment seeking was associated with higher intensity and duration of the disorder.17,18 Furthermore, PT seeking was shown to be predicted by symptom severity in psychiatric patients.19–21 Therefore, it is hypothesized here that high pain intensity in CP patients would predict PT seeking.
Quality of life (QoL) is another factor associated both with CP and PT seeking; 22 however, it is uncertain whether QoL is associated with PT seeking in CP patients. The results of relevant studies on other populations are inconsistent.22–25 Since more data points to the relationship between symptom intensity and PT seeking rather than low QoL and PT seeking, it is hypothesized here that low QoL mediates the association between pain intensity and PT seeking in CP patients.
Some researchers have explored whether psychological traits, such as locus of control (LoC – an individual's belief regarding the causes of one's experiences), could predict PT seeking.19,26,27 However, the results vary depending on the population. Moreover, none of the studies explored the association between LoC and PT seeking in CP patients. The studies that did focus on the population of CP patients examined their medical health-care-seeking behaviour and not PT seeking. 17 In one of those studies, 28 lower back pain patients with external LoC were more likely to seek medical care.
CP patients are often referred by their primary care providers to pain management programmes involving PT due to high-intensity pain that other interventions have failed to alleviate. 29 Therefore, it is also hypothesized that the association between pain intensity and PT seeking is stronger among patients who believe that doctors can control their pain (i.e., have an external LoC). This belief might be generalized to other pain specialists, including psychologists, thus increasing PT seeking. However, since PT requires an active approach to the management of one's symptoms, it is also hypothesized that a belief in personal control over pain could moderate the relationship between pain and PT seeking. Therefore, two models were constructed, each exploring a different set of beliefs. Furthermore, age, sex, and the kind of coping strategies patients use were compared between individuals who had undergone PT and those who had not, since research on other populations suggests that these factors may differ between the two groups of patients.20,30–34
The aim of this study, which was conducted on a large sample of CP patients, was to determine (a) what percentage of CP patients seek PT; (b) how CP patients using PT for the management of their pain differ from those who are not in terms of pain intensity, coping strategies, LoC and QoL; (c) whether low QoL mediates the relationship between pain intensity and PT seeking; (d) whether LoC moderates the relationship between pain intensity and PT seeking.
Methods
A cross-sectional study was conducted to answer the research questions. The authors contracted a clinical research company to conduct the study. The company has access to potential participants through a proprietary research panel where individuals with different demographic profiles register as potential participants in research projects. The panel represents the population of internet users, defined as people who use the internet at least once a week. By registering, the respondents agreed to the terms of use of their personal data by the clinical research company. Data obtained from the same sample was used in another study conducted by our research team. 35
Participants
Individuals who had suffered from a CP condition, i.e., for more than three months, were qualified for the study. The panelists were asked, “Has a medical doctor diagnosed you with a CP condition?” Answering “yes” to the question qualified them to participate in the study (N = 2 856; 7.3% of the total number of people registered in the panel). The final sample consists of the panelists who answered “yes, “agreed to participate in our study, and completed all the questionnaires (N = 600). Characteristics of the sample are presented in Table 1.
Sociodemographic, pain-related and healthcare characteristics of the sample.
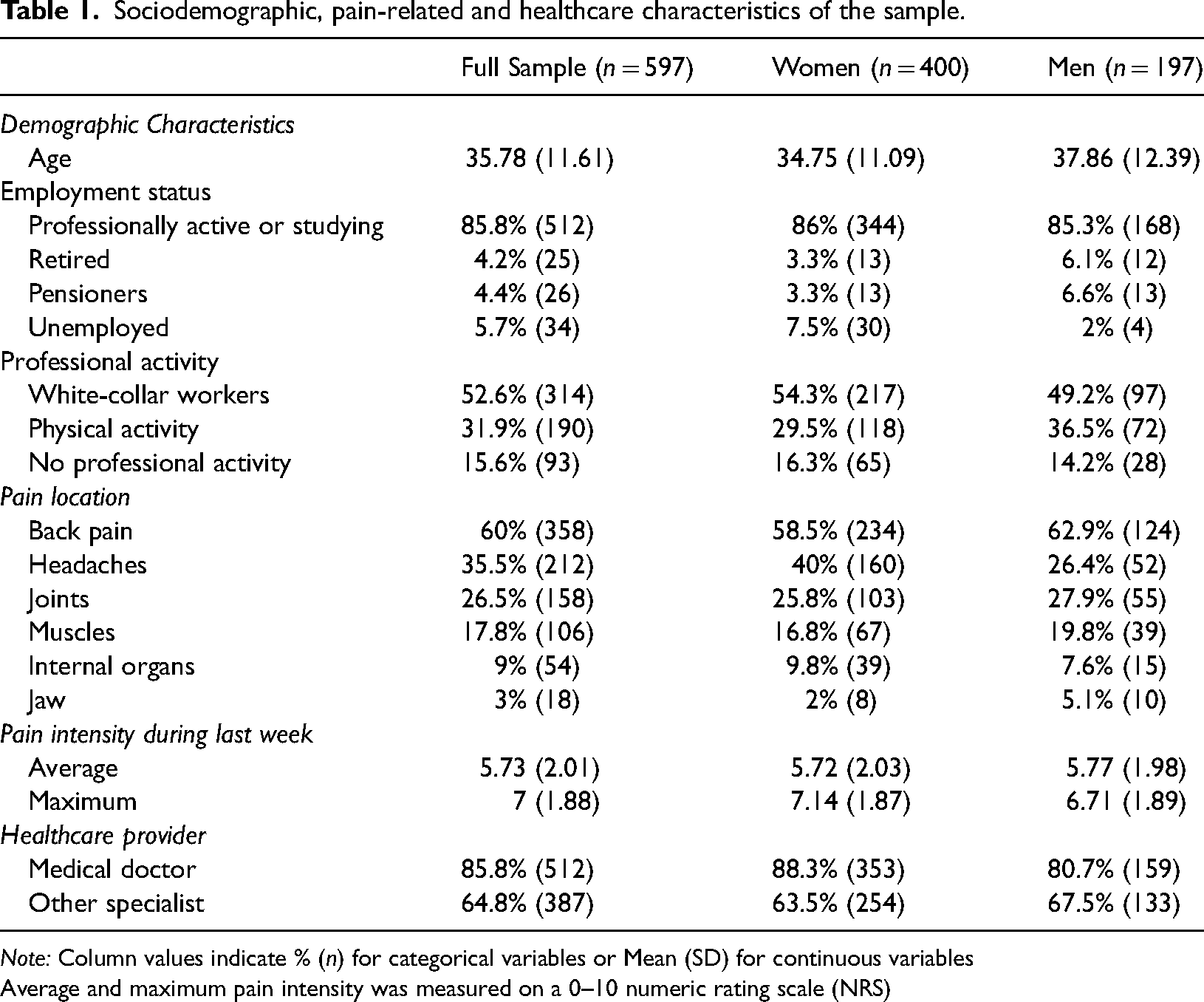
Note: Column values indicate % (n) for categorical variables or Mean (SD) for continuous variables
Average and maximum pain intensity was measured on a 0–10 numeric rating scale (NRS)
The participants who completed all the questionnaires were compensated for participating in the study with points they could exchange for electronic goods. All respondents expressed their informed consent in a written, digital form. The participants learned about the purpose of the study before taking part in it, and they could resign from participating at any point in time. The study was carried out following The Code of Ethics of the World Medical Association (Declaration of Helsinki). The clinical research company encrypts the files with research data and stores them on a server dedicated to this purpose to prevent the results from being associated with a specific individual. The research company's policy complies with the European General Data Protection Regulation. A local research ethics committee accepted the study protocol.
Measures
The study involved completing an online survey which consisted of four sets of questions about (a) demographic data (sex, age, employment status, and professional activity); (b) pain data (location, duration, and intensity); (c) medical care data (whether or not they use medical care; how many doctors they see about their CP condition; how many pain specialists – doctors or otherwise – they had consulted; how satisfied they are with the medical treatment and the doctor-patient relationship) and (d) questions about PT seeking for the management of CP. For the purposes of the study, PT was defined as working with a psychologist or a psychotherapist specifically to better cope with CP. The participants were asked whether they were using PT at the time or had ever used PT, and if so, how long they had been using it and how satisfied they were with the results. If the participants had no experience using PT for the management of CP, they were asked how interested they were in trying PT for their CP and why they had not done so before. Most of the questions about PT were answered using a 4- or 5-point Likert-type scale. Other types of questions included: binary answers (e.g., Have you ever used the services of a psychologist or a psychotherapist to cope with CP? Answers: yes/no), multiple choice and open-ended questions (e.g., Why have you never used the services of a psychologist or a psychotherapist to cope with CP? Answers: Lack of knowledge about PT for CP; no availability within the national health system; not enough financial resources; I think that PT is meant for psychiatric patients only; I do not believe in the efficacy of PT for CP; other (what?)).
Apart from the abovementioned questions, three standardized questionnaires were applied.
Coping Strategies Questionnaire (CSQ) measures the use of coping strategies in CP patients. It consists of 42 statements outlining different ways of coping with pain and two questions about assessing one's own ability to cope with and reduce pain. The statements are combined into six subscales representing cognitive strategies (diverting attention, reinterpretation of pain, catastrophizing, ignoring pain, praying/hoping, coping self-statements) and one subscale related to a behavioural strategy (increased behavioural activity). Each subscale can be scored between 0 and 36. A higher score is related to more frequent use of a certain strategy. CSQ demonstrated high internal consistency, with alpha coefficients ranging from over 0.80 (five subscales) to 0.60 (two subscales) and 0.80 for the whole questionnaire.36,37
Beliefs about Pain Control Questionnaire (BPCQ) was developed to measure the strength of individual beliefs about controlling pain. It comprises 13 items that merge into three subscales that measure the power of one's beliefs about factors that affect one's pain: Doctors’ control, personal control, and chance. Each subscale's score is calculated separately and sums up points awarded for each item. The higher the score, the greater probability that pain is influenced by the given factor. The Cronbach's alpha for the whole questionnaire was 0.75, for the subscales 0.85 (doctor's control), 0.82 (personal control), and 0.58 (chance).36,38
Short Form-36 Health Survey (SF-36) is a 36-item tool measuring health-related QoL. The items are combined into eight subscales that rate physical functioning, role limitations due to physical health problems, bodily pain, general health perceptions, vitality, social functioning, role limitations due to emotional problems, and general mental health. However, in the version of SF-36 used here, the results form one combined scale. The highest score means the lowest value, while the lowest score means the highest value in the QoL assessment.39,40 We decided to use that scale because we were interested in the QoL as a global factor for our model. 39 Moreover, previous studies evaluating psychometric properties of Polish translations of SF-36 and SF-36 v2 using different samples did not confirm the original structure of the questionnaire suggesting a different number of factors.41,42 Cronbach's alpha for the total scale obtained in the current version of the scale (0.86) suggests a high internal consistency of this questionnaire.
Numeric rating scale (NRS) ranging from 0 – ‘no pain at all’ to 10 – ‘the most pain that I have ever experienced’ was used to measure average and maximum pain intensity within the last week. The average pain intensity rating for the previous week was chosen for analyses as a more representative index.
Results
Data analysis
Skewness and kurtosis coefficients for continuous variables were in the range −1 to 1, suggesting no appreciable departures from normality; therefore, independent samples t-tests with Bonferroni correction for multiple comparisons were used to assess the differences between participants who underwent PT due to CP and those who did not. A Chi-square test was conducted to determine whether there was a significant relationship between sex and current and past use of PT. To test our hypotheses, mediation and moderated mediation models were examined with the Process Macro for SPSS 43 using a logistic regression-based approach. For the purpose of the analysis, the variable ‘intention to seek PT’, which was originally answered on a 4-point Likert scale, was dichotomized. Participants who declared that they ‘agree’ or ‘strongly agree’ with the statement that they are interested in seeking PT were classified as having the intention to seek PT help, while those who declared that they ‘disagree’ or ‘strongly disagree’ with the statement were classified as not interested in PT. We applied model 4 (simple mediation) and model 5 (moderated mediation) with 5000 bias-corrected bootstrap samples. Age and sex were added as covariates. All statistical predictors were converted into z-scores before conducting regression-based analyses.
Between-group comparisons
Participants who underwent PT differed significantly from those who did not in terms of age (they were significantly younger), level of pain (they declared a higher level of pain), as well as the frequency of using pain coping methods such as diverting attention, reinterpreting pain, coping self-statements, ignoring pain, praying/hoping and increased behavioural activity (they used all these methods more frequently than people who did not receive psychological help; see Table 2 for details).
Results of between-group comparisons between participants that underwent PT (group 1; N = 203) and those that had not been treated previously by a psychologist/psychotherapist (group 2; N = 394).
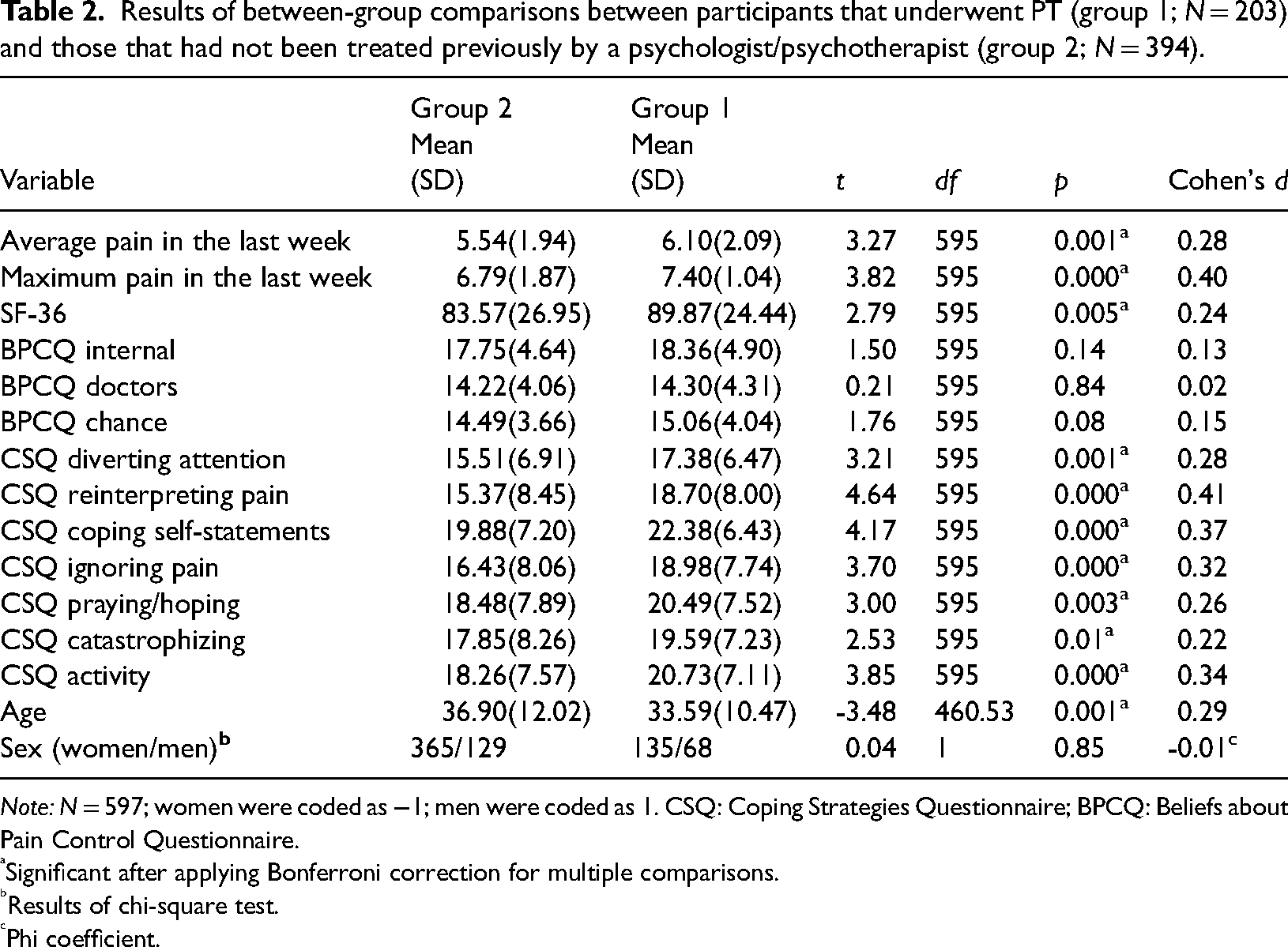
Note: N = 597; women were coded as −1; men were coded as 1. CSQ: Coping Strategies Questionnaire; BPCQ: Beliefs about Pain Control Questionnaire.
Significant after applying Bonferroni correction for multiple comparisons.
Results of chi-square test.
Phi coefficient.
Mediation model
The results of the analysis examining the mediating effect of low QoL in the relationship between pain and intention to seek PT is presented in Table 3. The total effect of pain on intention to undergo PT was positive and significant (B = 0.41, SE = 0.13, CI95%low = 0.17; CI95%high = 0.60, p < 0.01). Furthermore, pain intensity was positively related to low QoL (B = 0.25, SE = 0.05, CI95%low = 0.16, CI95%high = 0.35, p < 0.001), which in turn was positively related to the intention to seek PT (B = 0.53, SE = 0.13, CI95%low = 0.28, CI95%high = 0.78, p < 0.001). After controlling for low QoL, the relationship between pain and intention was still positive and significant, but it became weaker (B = 0.30, SE = 0.13, CI95%low = 0.06, CI95%high = 0.54, p < 0.05). The indirect effect was significant (B = 0.13, SE = 0.05, CI95%low = 0.06, CI95%high = 0.24), thus indicating partial mediation.
Parameter estimates for the mediation model.
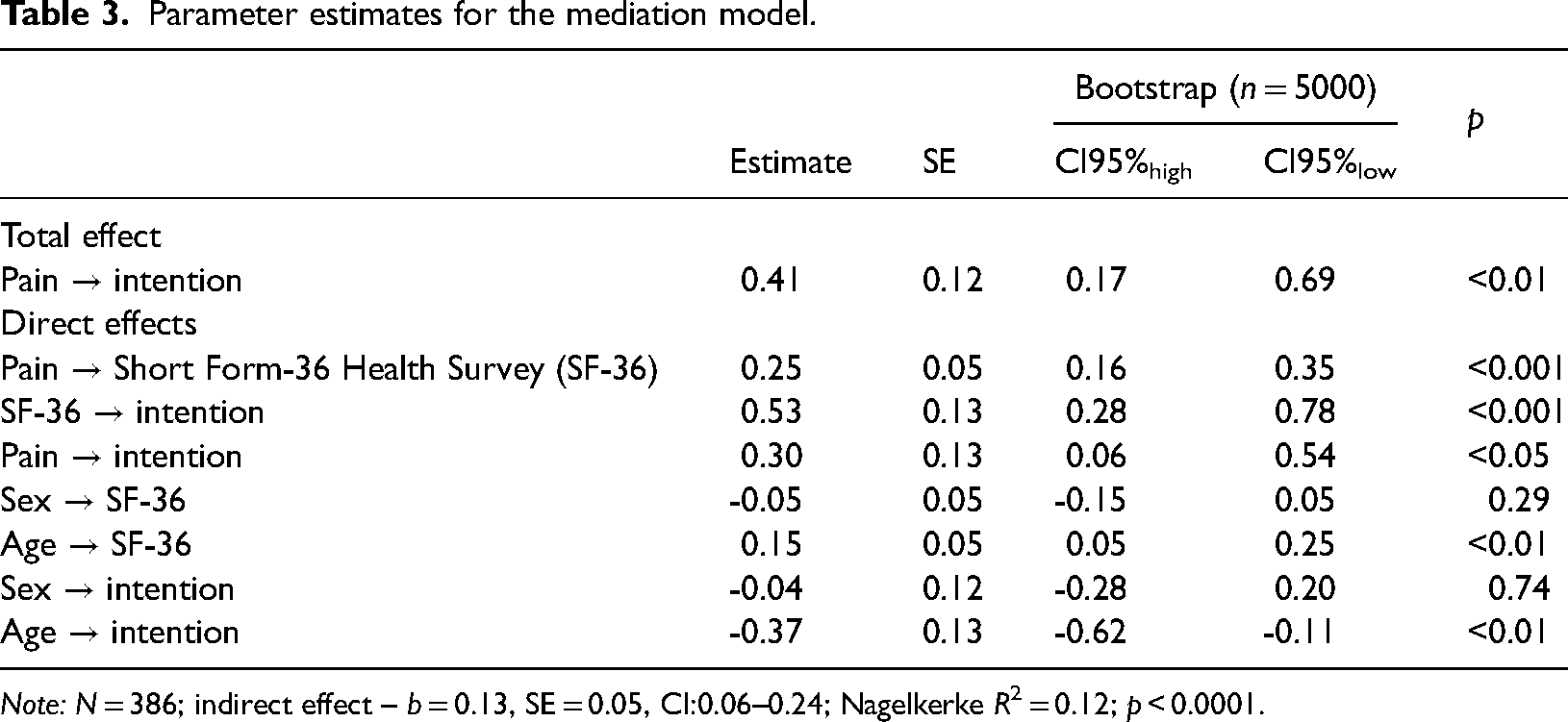
Note: N = 386; indirect effect – b = 0.13, SE = 0.05, CI:0.06–0.24; Nagelkerke R2 = 0.12; p < 0.0001.
Test of moderated mediation models
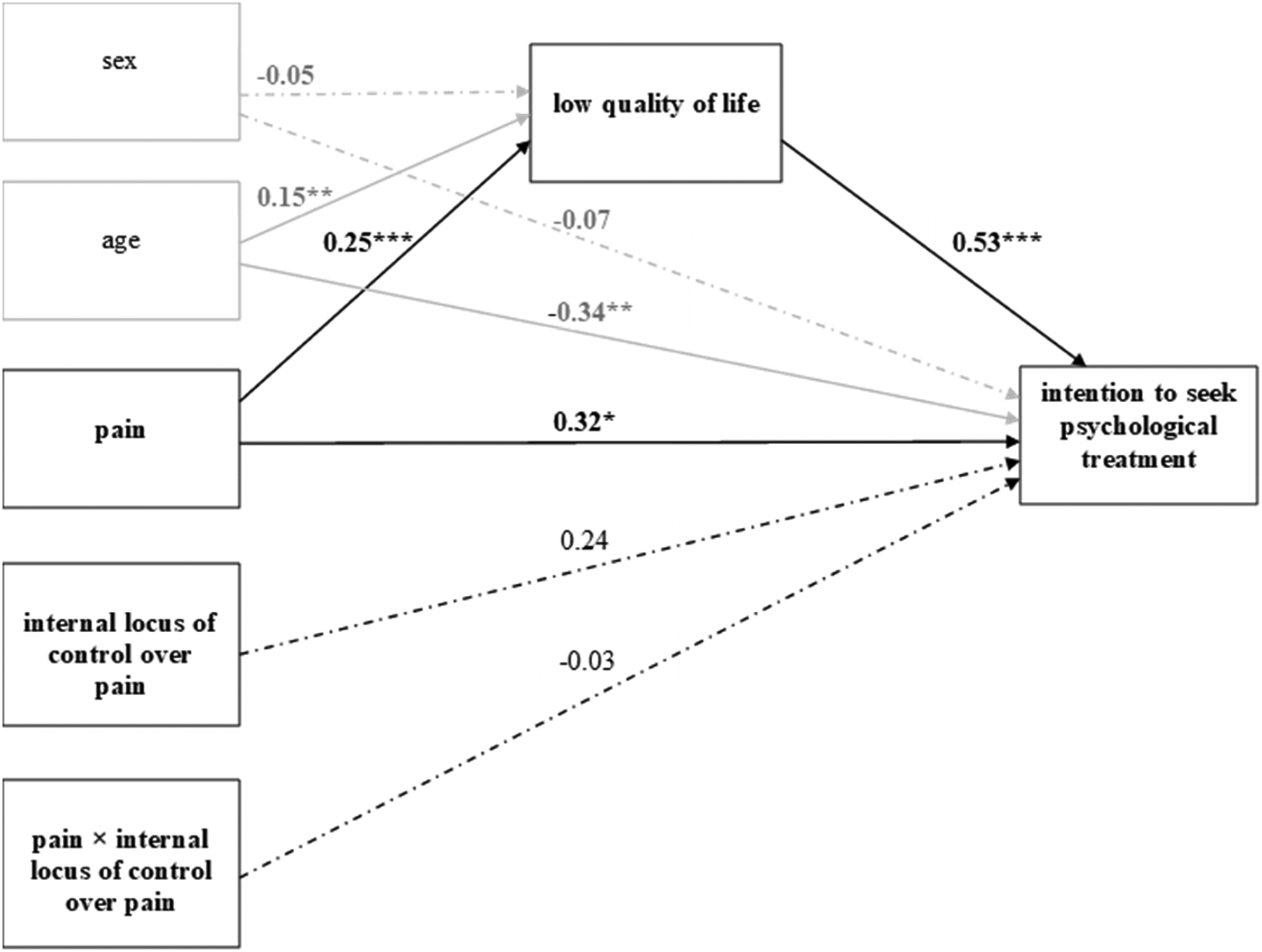
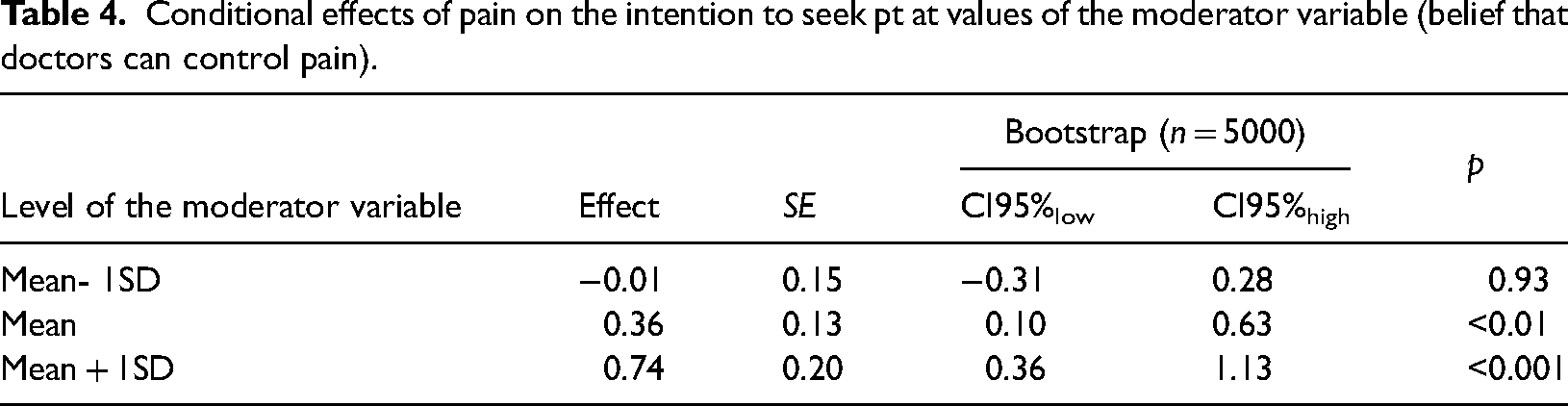
Two separate models were tested: In the first, the belief that doctors can control pain moderated the relationship between pain and intention to seek PT (Figure 1). In the second, the internal locus of pain control served as the moderator (Figure 2). Only the interaction effect of pain and the belief that doctors can control pain on the intention to seek PT turned out to be statistically significant (B = 0.38, SE = 0.11, CI95%low = 0.16, CI95%high = 0.60, p < 0.001). Specifically, the relationship between pain and the intention to seek treatment was significant at the “average” (Mean) and “above average” (Mean + 1SD) levels of the moderator variable, but not at the “below average” (Mean – 1SD) level of the moderator variable (see Table 4 for details).
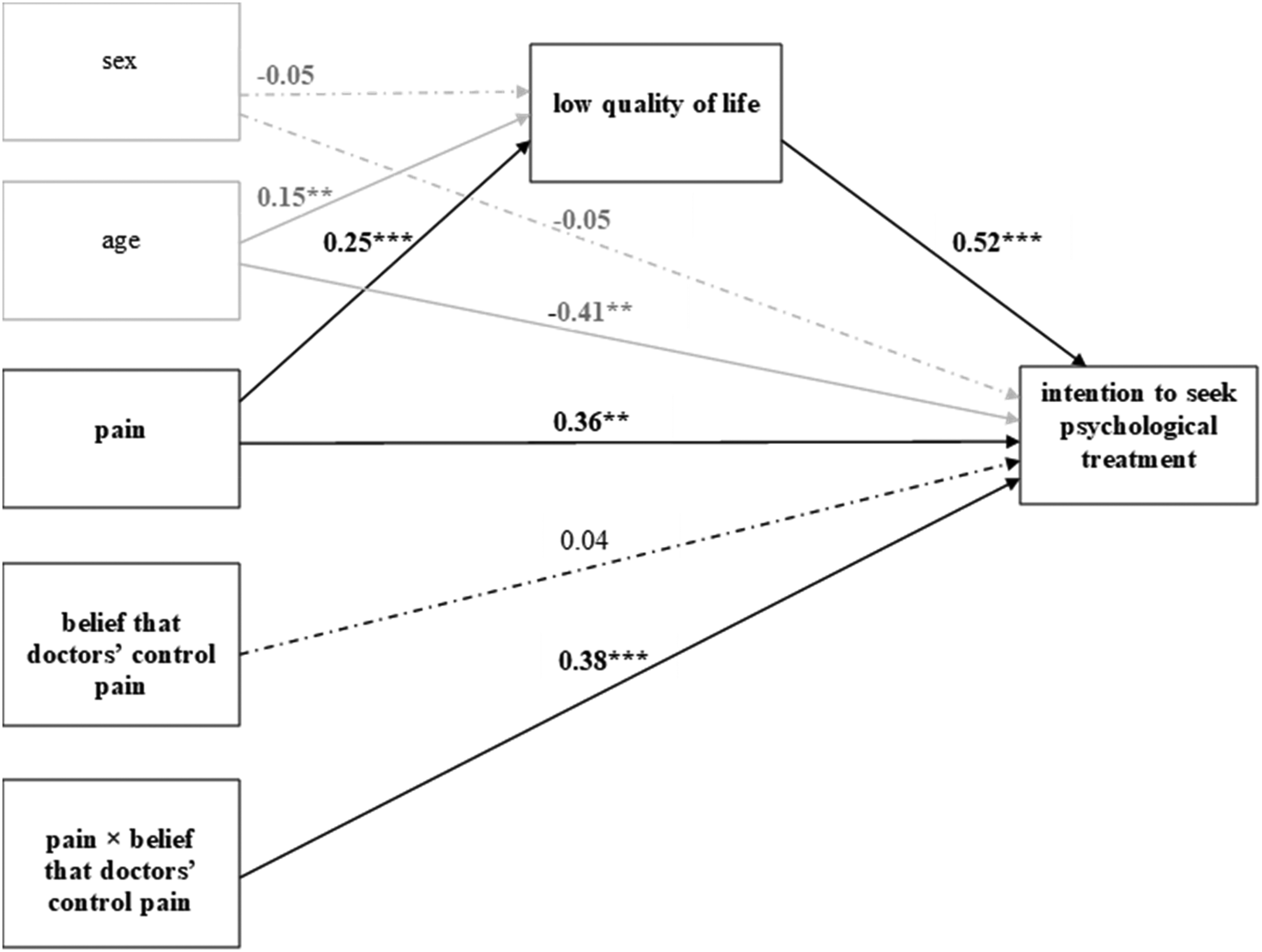
Pain, quality of life, belief that doctors have control over pain and intention to seek psychological treatment.
Pain, quality of life, internal locus of control over pain and intention to seek psychological treatment.
Conditional effects of pain on the intention to seek pt at values of the moderator variable (belief that doctors can control pain).
Discussion
To the best of our knowledge, this is the first study (a) to elucidate how CP patients who use PT for the management of their symptoms differ from CP patients who do not and (b) to address interactions between factors that are related to CP patients’ motivation to seek PT. The hypotheses were tentative since there has not been much research on the subject so far. In general, the predictions were confirmed. The obtained results suggest that the more intense pain individuals suffer and the lower QoL they experience, the more likely they are to seek PT. However, pain intensity seems to be associated with PT seeking only in CP sufferers who believe that doctors can control their pain.
The hypothesis that low QoL would mediate the relationship between high pain intensity and PT seeking was confirmed. Most of the studies so far have shown that the intensity of symptoms, whether pain or psychological distress, is associated with a tendency to seek medical or psychological help, respectively.17–21,44 These results were confirmed in the current study on CP patients regarding PT seeking; however, the results of this study suggest that low QoL may be partially responsible for the link between pain intensity and interest in PT. One of the reasons for this mediation might be the fact that low QoL involves decreased activity and lower mood – two of the most typical symptoms of depression 45 – and PT is often chosen as the main treatment for depression. 46 Another explanation could be that QoL decreases over time in CP patients 47 who seek PT. It is possible that starting PT earlier might prevent QoL from decreasing. 48 Further, longitudinal studies would have to be conducted in order to compare QoL in CP patients who started using PT soon after diagnosis against those who initially relied solely on medical treatment.
In the current study, two models were created in order to test alternative hypotheses about two different LoC beliefs. LoC is an individual's belief regarding the causes of one's experiences. Internal LoC characterizes a person who believes that there is a positive relationship between their behaviour and the outcomes they experience. On the other hand, people with external LoC believe that external sources, e.g., medical professionals, can control what happens to them. 49 Therefore, LoC is an important concept that helps to understand whether or how CP patients may try to control their symptoms. In our estimation, it was equally probable that an external LoC and that an internal LoC could predict PT seeking. The analysis of the two models constructed in order to test these hypotheses revealed that only CP patients who believed that doctors could control their pain (a form of external LoC belief) sought PT if their pain intensity was high and their QoL was low. No previous study has analyzed the moderating effect of LoC beliefs on the relationship between pain intensity, low QoL and PT seeking in CP patients. The results reported here are in accordance with some of the previous studies, in which external LoC was a positive predictor of treatment seeking in general.17,19,27 The moderating effect of external LoC might either mean that CP patients can be convinced by their medical doctors to try PT to aid with symptom management or that they believe in the power of pain specialists in general and therefore are more likely to seek help from PT providers.
Only a third of the participants had experience with PT. It has been shown before that PT may not be very popular among CP patients despite all the evidence that it may be helpful in treating CP. 50 Evidently, public education on the psychological aspects of pain is needed for PT to be perceived as more effective and acceptable. 51
There were significant differences between CP patients who had and had not tried PT. Patients from the first group were significantly younger and suffered from more intense pain than the other group. These results corroborate earlier findings on other populations in terms of symptom severity19–21,44 but not age, although some studies showed that older age is associated with a more positive attitude towards PT seeking.32,52 It is possible that among CP patients the relationship between age and attitudes towards PT is reversed. On the other hand, age did not predict PT seeking among the participants who had no previous experience using it. Similarly, a meta-analysis of studies conducted on lower back pain patients who were seeking treatment revealed that age was not associated with care seeking. 17 In the population of CP patients, it seems, therefore, that age does not predict treatment seeking, whether psychological or otherwise. It is possible that younger CP patients have a more positive attitude towards PT than older ones. They may be more aware of the psychological dimension of pain and the effectiveness of PT. Another explanation may lie in the “well-being paradox.” According to research, 53 older CP patients may have a higher level of mental well-being than younger ones despite suffering from CP (and, therefore, probably, a lower need for PT). Attitudes toward seeking PT may also play a role in whether or not CP patients will consult a psychologist. Unfortunately, some CP sufferers may be afraid of social rejection due to being identified in their society as a person suffering from a mental disorder if they seek PT. 54 Even if they want to seek PT, their physical mobility issues may prevent them from doing so if online therapy is unavailable.55,56
CP patients who declared having experience with PT were also more likely to use various coping strategies than patients who have never tried PT. There might be two reasons for this difference. A generally more active approach to dealing with one's problems might include PT seeking as a coping strategy. Otherwise, the tendency to use coping strategies might have developed as a result of PT.
Some of the advantages of this study are the large size of the sample and the proportion of men and women, which is similar to the proportion in the population of CP patients. One of the limitations of the present study is the fact that it was conducted online. Therefore, it is probable that elderly people were underrepresented in comparison with the population of CP patients. Furthermore, the self-reported diagnoses were not confirmed with medical documentation because of online security measures. Differentiating persistent CP conditions from cyclic ones and checking if it influences any of the other factors we assessed was therefore not possible. Future research should take these limitations into account and perhaps focus on data obtained from hospitals where detailed diagnoses will be available, and the age bias avoided. The cross-sectional character of the study means that some confounding variables might have been ignored; however, most of the studies on large samples of CP patients conducted to date have been cross-sectional.57,58
To conclude, our results show for the first time what characterizes CP patients who seek PT for the management of their symptoms and what psychological factors are associated with it. Intense pain and low QoL motivate CP patients to seek PT if they also believe that doctors can control their pain. This association might be interpreted as (a) an opportunity for medical professionals to diversify the therapeutic methods they can offer to CP patients and (b) a suggestion that PT might be included in the therapeutic process sooner, before pain becomes very intense and QoL drops.
Typically, CP patients seek medical treatment first; only when that treatment has failed are they offered other kinds of therapy, including PT. 29 This may suggest that PT is sought only as a treatment of last resort, an approach that certainly does not take full advantage of the benefits that PT may offer.11,12,14 One of the reasons may be the cost and limited access to high-quality psychotherapy, even in developed countries.59,60 Another is perhaps a lack of awareness in the general population that pain is not only a medical problem. 61
Despite the evidence that PT may be helpful in treating CP, it might not be very popular among CP patients.26,50 The way to escape this vicious circle may lie in the trust CP patients place in their medical doctors. It might be the responsibility of doctors to direct patients to use PT. This would not only be beneficial for the patients and would likely improve their condition, but it could also reduce the pressure placed on medical professionals as the sole clinicians responsible for managing patients’ CP symptoms. Multidisciplinary pain management programmes are often recommended for CP patients,62–64 but PT is not always included in them. 65 Perhaps putting more emphasis on PT as an integral part of CP care would improve patients’ QoL and increase the chances of successful pain management.
Footnotes
Acknowledgements
The authors would like to thank Kazimierz Sedlak, PhD, for encouraging us to conduct the study.
Contributorship
DF, EB, PB, JK and JB researched literature and conceived the study. DF, JB and JK were involved in protocol development, and gaining ethical approval. JK was involved in data analysis. DF wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from The Research Ethics Committee at the Institute of Psychology, Jagiellonian University, Kraków, Poland (approval number KE/41_2021).
Funding
This study was funded by the Pain Medicine Foundation, Poland. PB was supported by the National Science Centre, Poland (grant number 2016/23/B/HS6/03890)
Guarantor
PB
Informed consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.