
Abstract
Objectives
Explore the lived experience of individuals managing and/or caregiving for someone with a chronic disease and their perceptions of developing a mindfulness program for stress reduction.
Methods
Sixteen participants with chronic disease and/or caregivers participated. Participants completed eligibility screening, demographic questionnaires, and semi-structured interviews (30–60 min each) online or by phone. Interviews (n = 16) were audio recorded, transcribed, and analyzed using thematic analysis and NVivo® 12. Survey data were analyzed using SPSS® 28.
Results
Four themes emerged: (a) Chronic disease management and stress—perspectives on life's stressors; (b) Stress reduction techniques/perceptions of mindfulness—knowledge and implementation of stress reduction practices and familiarity with mindfulness; (c) Mindfulness program acceptability, barriers, and facilitators—interest, barriers, and facilitators to attending; (d) Mindfulness program structure—logistics to increase access and appeal to diverse audiences.
Discussion
Mindfulness has the potential for addressing the complexities of stress associated with disease management. Targeting mindfulness programs for populations with chronic disease management and caregiving responsibilities should include: Consideration of group formats with participation limited to this population, structuring programs to overcome barriers (i.e., culturally appropriate location), and equipping members of the community being served as instructors to ensure culturally relevant instruction.
Introduction
Approximately 129 million adults in the United States have at least one chronic disease, 1 and 4 in 10 adults have multiple chronic diseases (multi-morbidity). 1 Each year, globally, chronic diseases account for 74% of all deaths. 2 Chronic diseases result in high economic and social costs. 3 Approximately one-fourth of US adults serve as caregivers to individuals with long-term illness or disability, 3 which aligns with data from other countries such as Canada and Israel and exceeds countries such as Australia and Japan. 4 Many of these caregivers are also managing their own chronic diseases, with over 40% having two or more chronic diseases and 33% reporting activity limitations due to physical, mental, or emotional challenges. 3 Overall, individuals managing chronic disease report a number of mental, physical, and social challenges, which include: psychological stress; anxiety; the impact of disease severity; treatment side effects; limited financial resources and other barriers to accessing care; barriers to effective clinician communication including dissonance between cultural beliefs and disease management practices; life transitions; balancing family and work demands.5–7 When individuals managing chronic disease are simultaneously caregiving, burdens on physical and mental health as well as financial, social, and personal resilience resources are multiplied. 8
Traditional self-management programs, developed to reduce medical costs and improve health, have shown promising outcomes for individuals with chronic disease. 9 These programs emphasize problem-solving, building a partnership with one's health care provider, decision-making, and increasing self-efficacy for a variety of health behaviors (e.g., exercise, communication with physicians).9,10 These programs often involve skills mastery, modeling, and social persuasion, but fail to address the complexity of multi-morbidity, the dual roles of self-management and caregiving, and the related psychological stress and anxiety.7,9,11 Given psychological stress and anxiety can trigger physiological reactions such as inflammation and dysregulation of the immune system, which can worsen health and disease management, 12 there is a need for programs addressing both the mental and physical health stressors experienced by individuals managing chronic diseases.
Research suggests incorporating mindfulness practices from Eastern contemplative traditions with Western cognitive-behavioral approaches 13 has the potential to address physical and mental health through improving stress resilience, reducing anxiety, coping with pain, and altering pathophysiologic processes involved in chronic disease.14,15 Mindfulness can be defined as nonjudgmental attention to the present moment. 16 It includes attention to sensations, thoughts, bodily states, consciousness, and the environment, while encouraging openness, curiosity, and acceptance. 13 Programs incorporating mindfulness practices have been associated with reductions in systolic blood pressure and inflammation, improvements in heart rate variability and immune function, and pain reduction.14,15 The use of these practices has recently increased and their application to chronic disease is not novel. For example, mindfulness-based stress reduction (MBSR) was developed 42 years ago and has been shown to reduce chronic disease-related stress.17,18 MBSR has been found to consistently reduce depression, anxiety, perceptions of pain, symptomology while enhancing coping and quality of life across a range of chronic diseases including cancer and fibromyalgia.19,20 Though the potential role mindfulness programs can play in chronic disease management has gained recognition, these interventions often target specific diseases and either patients or caregivers rather than addressing the broader needs of individuals managing multiple chronic diseases and roles (i.e., caregiver and patient).21,22
In the US, disproportionately higher rates of many chronic diseases and a higher prevalence of multi-morbidity have been reported within populations marginalized due to factors such as race/ethnicity, 23 gender and sexual orientation, 24 education, and socioeconomic status.25,26 These populations are also underrepresented in research on mindfulness interventions.27,28 Survey data show US mindfulness practitioners are on average White, female, college-educated, and older. 29 Barriers to participation in mindfulness interventions by individuals most impacted by chronic disease may include a lack of culturally relevant adaptation. 30 Thus expanding the reach of mindfulness programs and creating programs that both appeal and are applicable to individuals most in need requires community-engaged formative research. 31
This formative study used in-depth interviews with individuals managing chronic disease as well as caregiving. The study aimed to gain insight into mindfulness program development that reflects real-world conditions for populations who disproportionately experience health inequities and multi-morbidity.23,24 Given the study aim, we recruited and solicited input from a diverse population previously under-represented in mindfulness research to explore participant lived experiences with self-management and caregiving for chronic disease, related stressors, and stress reduction techniques, perspectives on mindfulness, and how to incorporate these factors into a culturally relevant mindfulness program.
Materials and methods
Participants and recruitment
Data were collected from 16 participants using semi-structured interviews from March 2020 until June 2020. Eligible participants were 18 years of age or older with a chronic disease diagnosis over 12 months for themselves and/or a family member. A study flyer was created and used to recruit participants. The recruitment flyer described the study as focused on “find[ing] out more about chronic disease stressors and how to help families deal with them.” Participants who wanted to discuss challenges they and their family face when dealing with a chronic condition were invited to participate. The flyer was shared by the study team with physicians as well as community and faith-based leaders who shared it with their networks (e.g., other physicians and leaders, congregation members, listservs, newsletter distribution lists) via email. Participants also shared about the study with their networks by word of mouth or sharing the study flyer. Interviews were originally planned to be in-person in Baltimore, MD; Madison, WI; and Memphis, TN, but were conducted virtually due to the coronavirus disease 2019 pandemic. With this transition, participation was no longer restricted by geography; however, participants primarily came through connections of study team members (BEH, KK) in Memphis, TN. These study team members have a long history of partnerships with African-American communities in the area.32–35 They were able to leverage their connections within healthcare systems and faith-based organizations to recruit participants for this study.
Prior to recruitment, all research activities were approved by the Institutional Review Board at the University of Maryland (UMD), College Park (Ref: 1293258) and through reliance agreements with UMD Baltimore; University of Memphis; and the University of Wisconsin. All participants provided informed consent.
Data collection
The study flyer provided contact information for two study team members (RCP, BEH). Potential participants who reached out were given additional information about the study as needed then provided directions on how to complete an eligibility screener online or over the phone. Potential participants provided gender, age, education, average household income, chronic disease status for participant and family, length of time from diagnoses, and experience with meditation, mindfulness, and yoga. This information was reviewed by the study team and eligibility determined. No ineligible individuals were identified however two chose not to participate, and individuals who were eligible were emailed a consent form, which they signed and returned via email. Providing and returning consent forms by mail was also an option, but email was the primary choice of most participants. Once a signed consent form was received, a time and day were set to conduct the interview. Participants were provided directions on how to connect to the interview platform via computer or phone.
All interviews were conducted using the Cisco Webex platform (Version 41, Milpitas, CA) with audio only. Interviews were recorded and computer-generated transcripts produced, which were manually verified against audio recordings and notes by research team members. Interviews lasting 30–60 min were conducted by an interviewer, with a notetaker present to ensure accurate notes were taken should interviews fail to record. 36 Five research team members (BH, NW, SS, KR, RP) alternated as interviewers and notetakers.
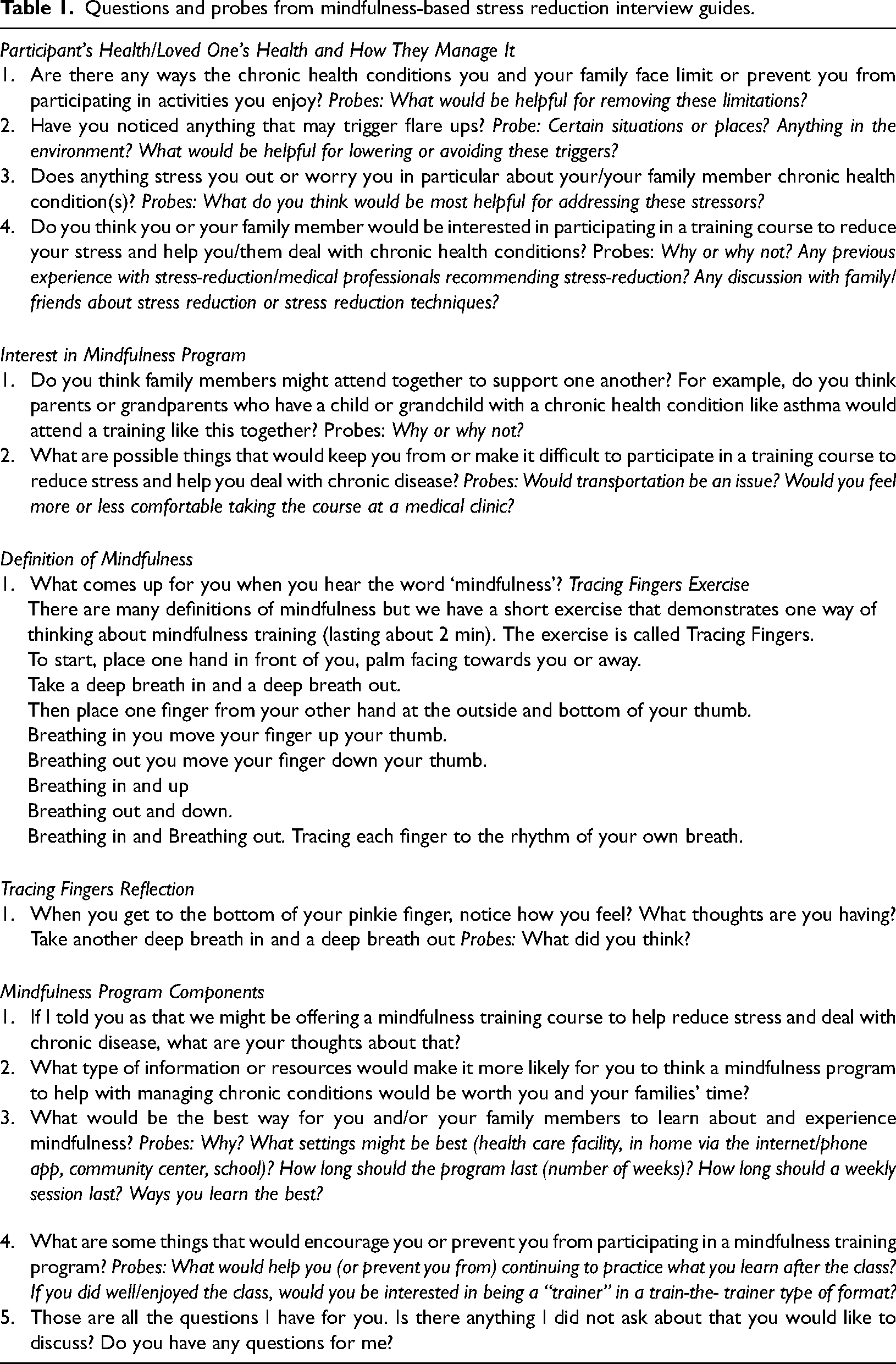
An interview guide maintained continuity across interviews (Table 1) and elicited participant lived experiences with self-management and caregiving for chronic disease, related stressors, and stress reduction techniques, perspectives on mindfulness, and how to incorporate these factors into a culturally-relevant mindfulness program. Open-ended questions and probes were used to guide participants through describing life stressors as well as their knowledge of stress reduction techniques and mindfulness. This was purposefully done to avoid prescribing standard research definitions of mindfulness to a community in which it may not resonate, which aligns with formative research and recognizing potential cultural biases that exist in defining life stressors and stress reduction.30,37 A brief mindfulness activity, “Tracing Fingers,” 38 occurred after participants were asked to share their understanding of mindfulness to demonstrate one definition of mindfulness and to provide a standard example before soliciting perspectives on how to incorporate mindfulness into a mindfulness program (i.e., methods of delivery, venue, session length). Upon completion, a $40 grocery store gift card was mailed to each participant as a “thank you” for their time.
Questions and probes from mindfulness-based stress reduction interview guides.
Data analysis
Descriptive statistics (Table 2) were calculated for demographic variables, personal and family member health status and experience with a meditation using IBM SPSS® Statistics Software (Version 28.0). Interviews were analyzed using NVivo® 12 (Q. S. R. International Pty Ltd). A thematic analysis approach was used to identify emerging themes across all semistructured interviews. 39 The thematic analysis process included: Becoming familiar with the data, initial coding, creating themes, and reviewing and defining themes. 39 Saturation of primary themes was reached after the completion of 16 semi-structured interviews (i.e., no new information was being gleaned from the interviews). 40
Demographics of participants (n = 16).
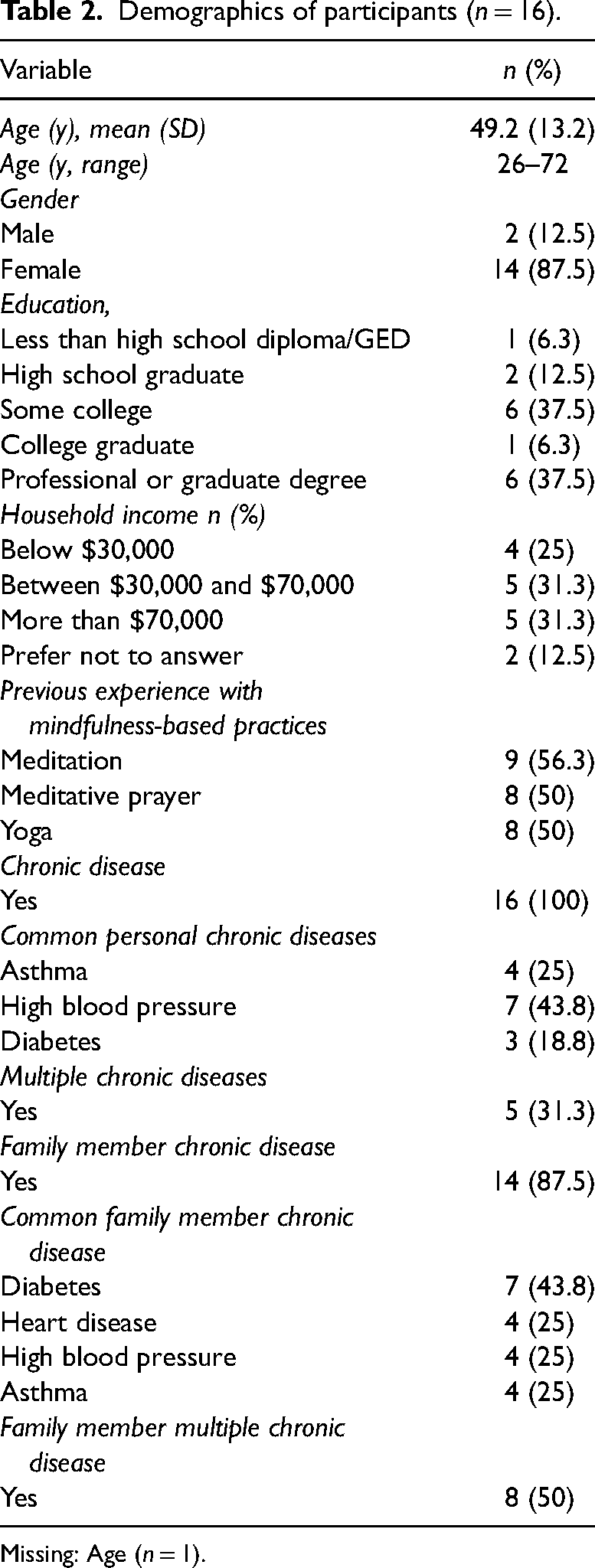
Missing: Age (n = 1).
Trustworthiness of findings was established by ensuring credibility, confirmability, dependability and transferability in data collection and analysis. 41 Analytic and interdisciplinary triangulation (e.g., psychology, behavioral science, epidemiology) aided credibility through: (a) two trained coders developing a codebook with input from a third researcher who aided in data collection, (b) reaching mutual consensus on identified themes (i.e., inter-coder agreement), and (c) incorporating perspectives and data interpretation from multiple scientific disciplines.42,43 Confirmability and dependability were aided by a detailed audit trail of data collection and analytic procedures. 43 Descriptive data (e.g., personal chronic diseases) were collected to enhance the transferability of our findings to similar populations. 41
Results
Among 16 interviews, participants had a mean age of 49.2 years (SD = 13.2, range = 26–72) and were mostly female (n = 14; 88%). Compared with 38% of the US population, 44 44% (n = 7) had a college degree or more education, and had a household income less than $70,000 (n = 9; 56%) comparable with the median US household income of $67,521 in 2020. 45 All participants reported at least one chronic disease with 31% reporting two or more (n = 5), and 88% reported one immediate family member with at least one chronic disease (n = 14) and 50% with multiple diseases among family members (n = 8). The most commonly reported personal chronic diseases were: high blood pressure (n = 7; 44%), asthma (n = 4; 25%), and diabetes (n = 3; 19%), with diabetes (n = 7; 44%), heart disease (n = 4; 25%), high blood pressure (n = 4; 25%), and asthma (n = 4; 25%) reported for family members. Most participants reported experience with mindfulness-related practices: meditation (n = 9; 56%), meditative prayer (n = 8; 50%), and yoga (n = 8; 50%). Race/ethnicity was not queried; however, most participants gave information that allowed for racial/ethnic identity to be determined, with most identifying as African American.
Qualitative themes
Identified themes that reached saturation were: chronic disease management and stress; stress reduction techniques and perceptions of mindfulness; mindfulness program acceptability, barriers, and facilitators; and mindfulness program structure.
Chronic disease management and stress
This theme provides insight into the ways stress and stress management manifested in participants’ lives as individuals managing disease and caregiving for someone managing disease. Within this theme, all participants (n = 16) spoke about various ways they manage their personal or family member's chronic disease using physical activity, diet, pain relievers, therapy, or other practices. Participants also described how their personal or immediate family member's chronic disease impacted efforts to manage their condition and life activities (n = 9). Some activities that were limited included sleeping, exercising, outdoor activities, and travel.
In addition to limiting life activities, participants acknowledged disease management techniques can also induce stress. Participants reported monitoring symptomology (n = 5) and accessing appropriate resources (n = 2) enhanced disease management but created additional psychological stress. Additional stressors described included attempts to avoid triggers (e.g., pollen for asthma attacks) (n = 6), hearing about community members dying from the same disease (n = 2), and having a chronic disease people cannot see (n = 3). Participants who also were caregivers described being unable to control the situation (e.g., disease, symptoms) for their loved one (n = 4) and the challenge of finding time for adequate self-care as additional stressors (n = 6).
Stress reduction techniques and perceptions of mindfulness
Some participants (n = 10) described receiving recommendations to engage in stress reduction from a variety of sources (e.g., physicians, family members). Some of these techniques included journaling, counting backwards or other breathing techniques, taking days off, and practicing yoga.
Participants also described volunteerism (n = 4), social support (i.e., support groups, friends) (n = 7), hobbies (n = 3), and outdoor activity (n = 3) as sources of stress reduction. Interestingly, caregiving was described as a stressor (e.g., lack of time for self-care and inability to control the disease for their family member as described above) and a stress reducer (n = 3). It helps to, like, have something else to be focused on or, you know, just something somebody else to care about. (Participant 4)
Four participants described the stress reduction that came from finding they were not alone in the situation via support groups or social networks; however, the social support was not without challenges. Participants qualified that “you have to be open to it”, and social support should be provided nonjudgmentally (n = 2), and in a culturally appropriate way. For example, participants (n = 5) noted an expectation that stress and disease management should remain private (we don't like to open up about our conditions) with outward appearances betraying no sign of stress or disease (we don't want to let people know that we're not in control of situations), which could limit actively seeking support as well as overtures of support.
When moving from the broader context of stress reduction to defining mindfulness, nearly all participants (n = 15) stated they were familiar with the term. Their definitions were sometimes couched in terms of what is required for the practice of mindfulness (e.g., “it's a lifestyle,” “responsibilities,” “your whole soul and body”) or benefits of mindfulness practice (e.g., “getting the mind to settle down or rest,” “awareness,” “understanding your situation,” “being fully present,” “being thoughtful”).
The “Tracing Fingers” activity
38
(Table 1) was an important tool in providing all participants with an example of a mindfulness practice. Participants (n = 15) used positive descriptors (e.g., “feels good,” “feel less heavy,” “cool”) and/or noted common mindfulness benefits such as awareness, decrease in heart rate, increased focus, enhanced breathing, pain relief, and a clear mind. Several (n = 8) participants described it as “relaxing” as well as noted its potential for reducing stress and/or interest in future use. My mind was focused on my hand and nothing else, so at that particular moment … It was like everything else was of no concern just what you told me to do. So, my knee right now it's hurting, but what you told me do just then, I didn’t feel the pain in my knee because I was listening to you and what you told me to do. (Participant 10)
Mindfulness program acceptability, barriers, and facilitators
When introduced to the concept of a mindfulness program to help with reducing the stress of chronic disease management, all participants (n = 16) expressed interest. However, a variety of barriers that might impact attendance were raised including: “just not wanting to do it,” “schedule,” and “time.” However, the most frequently mentioned factors that could impact attendance were transportation issues (n = 8) and class location (n = 8). Some participants described public transportation (e.g., buses running on time) and not owning a personal vehicle as potential barriers to attending a mindfulness program. Additionally, when asked about appropriate settings for implementing a mindfulness program, some participants (n = 3) spoke of settings such as hospitals and faith-based organizations (i.e., churches) not being comfortable settings for all individuals. … some folks won’t go, because it's at a church and I think it's the same thing with the hospitals. You know, we have people that literally fear a hospital or going to the doctors. So I would eliminate that by maybe putting it in the community. (Participant 11)
Participants (n = 6) advocated for the inclusion of techniques for long-term habit development and mindfulness retention techniques. Participants also noted engagement in a mindfulness program would depend on the benefits, including: intangibles (n = 4) (i.e., seeing “improvement” and “helping me deal with my stress”) and tangible items (n = 8) (i.e.,“incentives” or “swag"). I think after three weeks, I don’t see no improvement where I have to, you know, cause I don’t want to take pain pills for the rest of my life … If it would lower my pain pill usage, that would be enough for me. (Participant 10)
… you’ll get a gift card that helps people to say, okay, I got five more classes to go. I can do this …. (Participant 6)
Mindfulness program structure
Participants commented on how best to structure a mindfulness program to appeal to a diverse audience. Class format suggestions included a hands-on approach (n = 2), virtual or at-home (n = 6), or a combination of formats (n = 4). Except for one participant, nearly all participants (n = 15) were interested in attending a mindfulness program with a friend or family member. Several participants highlighted that a group-based program “works better together” and would provide “camaraderie” or “support.” I would definitely extend it to my family. I think all families, you know, people who go through it should have family support. (Participant 5)
Participants (n = 13) brought up class timing to balance the participant burden with gaining information. While no consensus was reached on when and how long the mindfulness program should be, the most frequent recommendations were 30-min to one-hour (n = 6) or one and a half-hours to two-hour sessions (n = 3) offered weekly or bi-weekly (n = 5) for three (n = 2) or four to eight weeks (n = 4). even if the information is beneficial, anything over thirty minutes, you sort of start to lose people nowadays…– (Participant 9)
When asked who should teach the mindfulness program, a few participants (n = 2) said they wanted an “expert” or “someone who has been trained,” with a participant noting they preferred either “someone who has been professionally trained” or “someone who has walked in my footsteps.” Most participants (n = 10) were interested in a train-the-trainer model, in which lay persons with chronic diseases were trained to teach the mindfulness program. Thus, increasing the relevance of mindfulness programs may require it to be community-led. … You can reach so many more people. If you have people this, you know, the boots on the ground, and they're in their community, and they're at their church and they're able to kinda share that information. (Participant 11)
Discussion
The goal of this study was to explore participants lived experiences with self-management and caregiving for chronic disease, related stressors, and stress reduction techniques, perspectives on mindfulness, and how to incorporate these factors into a culturally relevant mindfulness program. Participants presented a complex lived experience that often involved managing multiple chronic diseases for themselves and their family members. Though stress reduction techniques and mindfulness were familiar to most, experience with traditional mindfulness programs (e.g., MBSR) was limited. Participants expressed interest in attending a mindfulness program, and provided unique insights on perceived benefits, barriers, and important structural components necessary to develop an acceptable program.
Previous research has highlighted associations between psychological stress and chronic disease. 12 Consequently, mindfulness programs may be particularly beneficial as they have shown promise addressing physiological aspects (e.g., blood pressure, pain management) of certain chronic diseases,14,15 and have been associated with stress reduction benefits for caregivers of individuals with chronic disease.21,46 However, much of the research exploring these benefits has focused either on managing a chronic disease 14 or on caregiving.21,46 Our participants described a complex web of balancing comorbidities along with chronic disease management strategies (i.e., monitoring symptoms, being active) for themselves and family members, which contributed to high levels of stress.
Most participants were familiar with aspects of mindfulness and found the Tracing Fingers exercise to be a positive experience. However, almost none had previous experience with traditional mindfulness programs (e.g., MBSR). This may reflect our participant population, diverse in socioeconomic position, mostly residing in the Southern US. Prior research suggests that mindfulness programs are more commonly attended by non-Hispanic White, affluent, individuals in the Western US 29 with culturally relevant adaptations needed to encourage use among more diverse populations. 30 All participants in this study were interested in attending a mindfulness program and provided suggestions for creating programs that are more acceptable and accessible to individuals managing chronic disease and caregiving. This community and other communities should continue to be engaged throughout the development and implementation of mindfulness programs to increase the inclusion of holistic and culturally relevant management strategies.22,30
Program development suggestions from participants in this study provide insight into ways to promote and structure mindfulness programs for optimal engagement. 22 Participants noted the need to overcome barriers (i.e., location, transportation) when attending a mindfulness program. A few participants spoke of implementing the program in a community setting as opposed to a church due to concerns over it being a deterrent. Faith-based settings are often suggested as a preferred location for health-related programs for Latino, African American, and rural populations, especially in the Southeastern US.47–49 However, other studies have reported hesitation by community members to attend faith-based programs due to concerns churches are opposed to non-congregation members attending or try to “convert” members. 34 In addition, studies have noted the need to address religious concerns (e.g., beliefs) related to mindfulness programs when using faith settings.49,50 To help overcome barriers related to transportation and logistics of attending a program no matter the location, previous researchers have recommended providing support in the form of travel reimbursement, child-care, and a meal. 51
Participants felt a group format would work well, which is consistent with previous mindfulness program designs. 18 Group formatting is a way to provide social support, which is a common construct within multiple behavior change theories. 52 This suggestion also aligns with the participant discussion of social support as a stress reducer. A group format, open only to participants managing chronic disease, would provide a space where participants may feel more comfortable being open about their situations. Individuals with chronic disease and caregivers could attend together, facilitating the sharing of knowledge, accountability, and reducing the burden of finding respite care to attend. However, these considerations should be balanced with recognition of needs particular to caregivers that were voiced by participants, including challenges of self-care and being unable to control situations for their loved one. Offering a variety of group sessions is an option for meeting the needs of individuals with complex disease management roles.
No consensus was reached on session frequency or length suggesting the need for flexible options. In general, participants recommended shorter sessions with less frequency (30-min to 1-h weekly or bi-weekly sessions for 4- to 8-weeks) than traditional mindfulness programs, which consist of 1.5–2.5-h weekly sessions for 8-weeks with a six-hour daylong retreat.18,53 In other studies, participants have expressed concern with the length of mindfulness programs as they may make it difficult to set aside time, conflict with busy schedules (e.g., child-care, work demands), and contribute to physical pain and impede concentration due to sitting for an extended period.27,51 Traditional mindfulness programs are taught by a trained professional, 18 but study participants expressed the importance of incorporating a train-the-trainer model. This model also aligns with the need for trainers who provide culturally relevant instruction 30 and participant views of volunteerism, social support, and caregiving/focusing on others as stress reducer. Few mindfulness interventions have incorporated this model, 54 limiting our understanding of its effectiveness. In other health promotion programming, training lay persons has proven beneficial through increased access to evidenced-based public health practices, program cost reduction, and targeted programs to meet community needs. 55 Similarly, participants in previous mindfulness programs have recommended incorporating individuals from the community to increase buy-in and targeting programs to the needs of the community through awareness of religious concerns, representation in teaching, terminology, and values.22,30
Study findings suggest future research is needed to better understand the influence mindfulness programs have on individuals with multiple stressors and complex living situations. Researchers wanting to engage individuals with chronic disease, caregivers, and diverse populations in mindfulness programs need to maintain community engagement throughout the development and implementation process to tailor programs to their specific needs while gaining knowledge on barriers specific to each population (e.g., transportation issues, location acceptability). Additionally, more research is needed to expand our understanding of the effectiveness of shorter, more flexible mindfulness programs,53,56 group-based programs, and the use of train-the-trainer or similar models when implementing mindfulness programs.
Limitations
Despite valuable findings, our research was not without limitations. Though we attempted to include as diverse a study population as possible, the pandemic influence on recruitment and study design highlighted the importance of leveraging existing community relationships to engage diverse participants. Saturation was attained for themes related to our study aim, but fewer participants of lower socioeconomic status and a small number of men participated (n = 2), which limits the transferability of our findings. In addition, convenience sampling may have introduced self-selection bias and self-reported patient characteristics may have led participants to report more desirable information (e.g., fewer chronic diseases). Finally, we did not collect information on participant race/ethnicity or rural/urban residential status; however, participants spoke of their race/ethnicity and community environment with interviewers. Participant perspectives and insights in this study were mostly representative of an African-American community, which may limit the transferability of our findings to other cultural groups.
Conclusions
Most study participants reported a personal chronic disease or a family member living with a chronic disease. Additionally, participants were familiar with mindfulness but did not have experience with traditional mindfulness programs, which aligns with the lack of diversity in current mindfulness research and practice. Unique findings regarding targeting programs included respecting time limitations (i.e., shorter sessions), having group-based programs, and incorporating a train-the-trainer model. Future mindfulness research and programming should consider: group formats limited to individuals managing chronic disease to address needs for social support from others in similar situations; with shorter and more flexible sessions than traditional programs, in settings that align with the community's views (i.e., location acceptability) and logistical needs (i.e., transportation); using a train the trainer model with community members to enhance culturally relevant instruction and for individuals managing chronic disease who reduce stress through volunteerism; and most importantly engaging individuals from the community who deal with the stressful and complex situation of managing chronic illness for themselves and others simultaneously.
Footnotes
Acknowledgments
The authors express our sincere appreciation to the participants of this study for sharing their valuable insights and time.
Contributorship
BEH, KER, SJS, AJS, MLR, CM, and RCP designed the overall study, developed protocols, data collection materials, mindfulness exercise, and interview guide; KK, BEH developed recruitment materials and advertised to potential participants; NTW, BEH, KER, SJS, and RCP conducted interviews; NTW, SM, and RCP cleaned transcripts; NTW, BEH, and RCP coded data and wrote; NTW, BEH, KER, SJS verified analysis; KER, SJS, AJS, SM, KK, CM, and MLR reviewed and edited manuscript; RCP obtained funding and provided project oversight, All coauthors contributed significantly, reviewed the article, and agreed to submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All research activities were approved by the Institutional Review Board at the University of Maryland (UMD), College Park (Ref: 1293258) and through reliance agreements with UMD Baltimore; University of Memphis; and the University of Wisconsin.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health, National Center for Complementary and Integrative Health # K18AT010207-01
Guarantor
The guarantor of this manuscript is Robin C. Puett.
Informed consent
All participants provided informed consent.