
Abstract
Objective
This study was an attempt to shed light on the predictive role of intimate partner violence in adhering to treatment regimens in women with chronic illnesses.
Method
In a descriptive-analytical study, 400women with chronic illnesses in Bushehr were selected through convenience sampling. The data were collected by distributing a demographic information form and two questionnaires, including the intimate partner violence (IPV) questionnaire and the treatment adherence scale.
Results
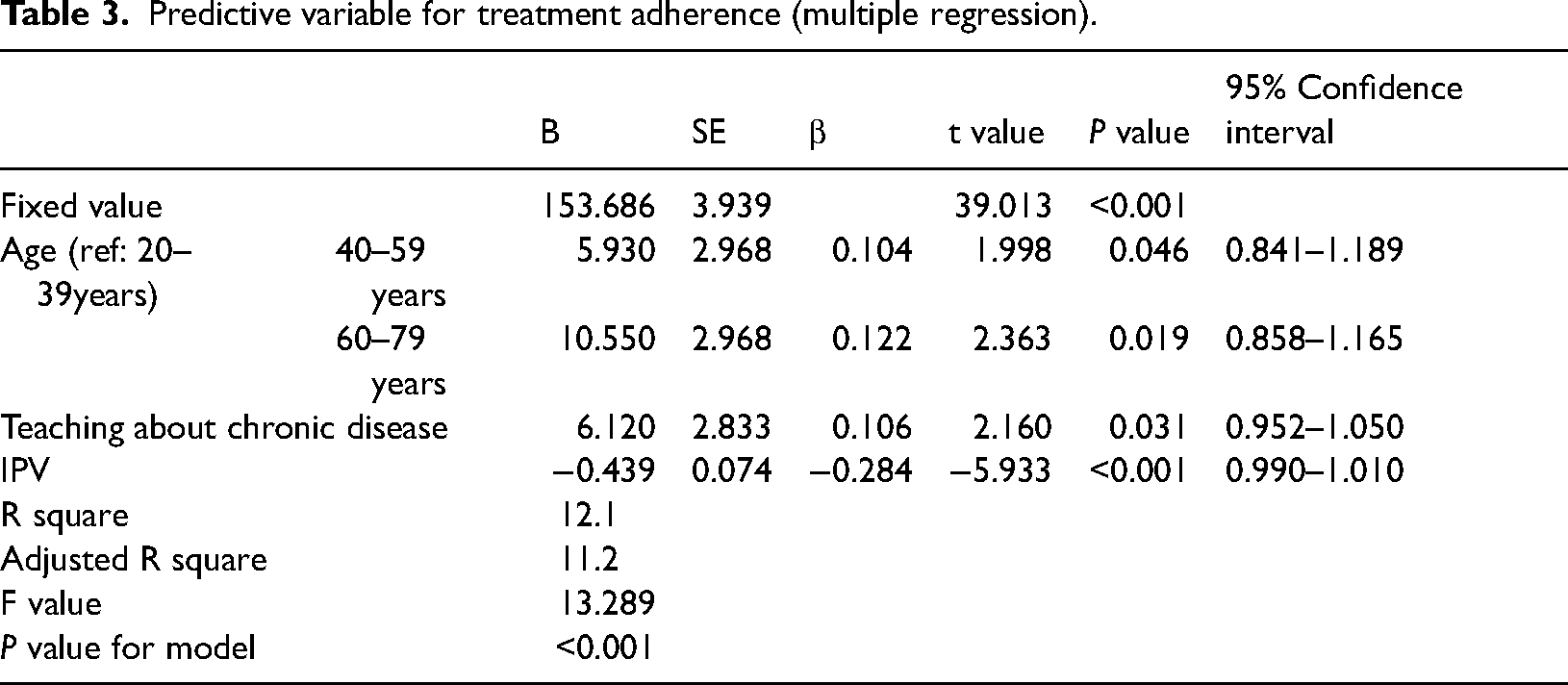
According to the results, the 40 to 59 years age group (P = 0.046, β = 0.104), the 60 to 79 years age group (P = 0.019, β = 0.122), and the group receiving education about chronic illness (P = 0.031, β = 0.106) showed a direct relationship with treatment adherence, while IPV (P < 0.001, β = 0.284) had a significant inverse relationship with treatment adherence.
Conclusion
The results of the study showed that predictors of treatment adherence are IPV in women aged 40 and older with chronic illnesses, and receiving education about chronic illnesses. It is necessary for healthcare providers to consider barriers such as intimate partner violence when providing education in order to increase treatment adherence. To avoid nonadherence, managers and health planners should implement policies to increase the level of awareness of healthcare staff on how to manage care of women with chronic illnesses who are abused by an intimate partner and refer them to counselors and family helpers.
Keywords
Introduction
Chronic diseases have garnered considerable attention due to their high mortality rate and the disease burden.1,2 These diseases constitute the most important causes of death in the world. In Iran, chronic illness accounts for 63% of all deaths. 1 Correct diagnosis and effective treatment are substantially important for a longer lifetime and better quality of life in patients with chronic illness. 3 Most of these patients need behavioral changes including their diet plans, exercise regimes, proper use of prescription drugs, and reduction or elimination of risk factors such as smoking and stress. 4 In patients with chronic illnesses, achieving practical treatment outcomes and minimizing the effects of diseases, improving health outcomes, preventing further disability, increasing the quality of life, and reducing healthcare costs are highly contingent on the degree of treatment adherence.2,3 However, many of these patients do not adhere to the prescribed treatments. In developed countries, the reported treatment adherence stands at approximately 50% on average. 5 In Iran, the estimated treatment adherence is between 12.7% and 86.3%. 1 Treatment adherence is considered a major challenge for patients with chronic illnesses and has remained an unresolved challenge.1,4
A set of factors (not just one single factor) determine the patients’ ability to closely adhere to the treatment recommendations. Interpersonal interactions along with the degree and method of the support received can affect treatment adherence. 6 Family is the first and most important support platform for patients, and spouses are typically the first ones who act as a source of support in times of crisis.7,8 Hence, close relationship with parents, siblings or friends generally does not make up for the lack of strong relationship with one's spouse and cannot prevent depression and stress in patients at difficult times in life. 7 Studies often refer to the supportive role of the spouse in treatment adherence.7–9 However, they have not paid attention the effect of spouses on treatment adherence, as they may not only do not support but create a stressful and unsafe environment by their violent actions.
Studies have examined the role of stress and anxiety in treatment adherence, as well as the role of the spouse and his behavior, especially intimate partner violence (IPV), as a stressor that may ultimately affect treatment adherence, a factor which has been largely overlooked. IPV is a behavior that is recognized as a cultural and health issue, 10 and has short-term and long-term consequences for the physical and mental health of women and their families. 11 Regardless of geographical constraints, economic development, and education levels, domestic violence is a major global public health concern that affects women of all ages. 12 According to the estimates by the World Health Organization in 2017, one out of every three women in the world (approximately 35%) experiences physical, mental, or sexual violence during her lifetime. 13 Based on 31 studies conducted in Iran, the rate of IPV in various cities of Iran varies, where the prevalence of domestic violence has been estimated at 66%, with 70% in the eastern and southern geographical regions, and 59%, 62%, and 75% in the central, northern, and western regions of Iran, respectively. 14 The inability of female victims of IPV to cope with problems can lead them to pursue unsafe coping strategies such as unhealthy behaviors including drug or illegal medication abuse, smoking, and drinking. 15 Therefore, it seems necessary to study the effect of the spouses of chronically ill patients on treatment adherence, where they may not only do not support them but may create a stressful atmosphere in the house and adversely affect the mental-emotional state of women. The first important step in designing interventions is gaining adequate knowledge of the role of IPV in adhering to treatment in the lives of the victims. Moreover, the lack of knowledge of the factors determining adherence can lead to failure in coping with this phenomenon. Therefore, understanding and identifying the influential family factors are important and can be a practical guide for policy makers, managers, and clinical nurses in developing support plans, interventions, approaches, and new strategies. Therefore, the present study was conducted to analyze the role of IPV as a predictive indicator in adhering to treatment in women with chronic illness.
Method
Study design and participants
The present paper was a cross-sectional correlational study conducted in 2019 to 2020. The study population included women suffering from the most prevalent chronic illnesses in Iran based on the most recent statistics provided by the Center for Controlling Non-Communicable Illness, which include cardiovascular diseases, dyslipidemia, diabetes, and hypertension. 3 The participants were selected from patients referred to hospitals, cardiologists’ offices, internal medicine specialists’ offices, and general healthcare centers. As the distribution rate and the number of participants referred to doctors’ offices and hospitals are not known, the convenience sampling technique was used. Considering the sample size for regression analysis, which requires selecting 10 to 30 participants per predictor variable (n = 10–30k), 30 participants were selected for each predictor variable. 16 Since there was just one main predictor variable, all the main demographic variables were also included in the set of potential predictors. Approximately, 300 participants were considered in the end with a maximum of 10 predictor variables. Considering the probability of a 30% drop in participation, 400 samples were finally considered. Finally, out of 400 women who had agreed to participate in the study, all 400 completed the questionnaires.
The inclusion criteria included having suffered at least 6 months from one or several types of chronic illness, 9 absence of neuropsychiatric disorders and debilitating physical disorders, no abuse of psychotropic drugs, full hearing, ability to speak, married marital status, and a completed written informed consent form. The exclusion criteria also included failure to complete the research scales, withdrawal from the study after completing the questionnaires, and failure to understand the questions of the questionnaire despite the explanations provided by the researchers.
Instruments
The data gathering tools included the demographic form, the IPV questionnaire, and the treatment adherence scale. To measure IPV, the researchers used the intimate partner abuse questionnaire by Mohseni Tabrizi et al. 17 This questionnaire consists of 26 statements based on the five-point Likert scale with answers ranging from always to never. The score range for this questionnaire is 26 to 130. The psychometric analysis of this questionnaire was performed by Mohseni Tabrizi et al. 17 In the present study, the internal consistency of the questionnaire was confirmed with a Cronbach's alpha of 0.90.
The second questionnaire was the treatment adherence scale developed by Seyed Fatemi et al. 18 which is composed of 40 statements. It is based on a six-point Likert scale and range from completely agree (5) to completely disagree (0). The score ranges from 0 to 200. The psychometric analysis of this scale was conducted by its designers. 18 In the present study, the resulting Cronbach's alpha value was 0.93.
Data collection
Upon receiving the ethics approval from the ethics committee in Bushehr University of Medical Sciences, Iran (IR.BPUMS.REC.1398.009), the researchers submitted an introduction letter to the mentioned centers, and hence, the sampling was conducted. The researchers explained to the study participants about the study's objective, rights, confidentiality, and the method of data collection. Informed written consent to participate in the study was obtained from each study participant. Thereafter, the demographic information questionnaire, the domestic violence questionnaire, and the treatment adherence scale were completed by the participants.
Data analysis
The data was analyzed in SPSS v.19 statistical software after data gathering. First, the distribution of the quantitative data was assessed using the Kolmogorov–Smirnov test. Simultaneous univariate and multivariate regression analyses were performed to determine the factors associated with treatment adherence. For the multivariate regression, the variables that were associated with adherence in the univariate regression were included in the analysis. The linear regression hypotheses were formulated, and the significance level was below 0.05 in all cases.
Results
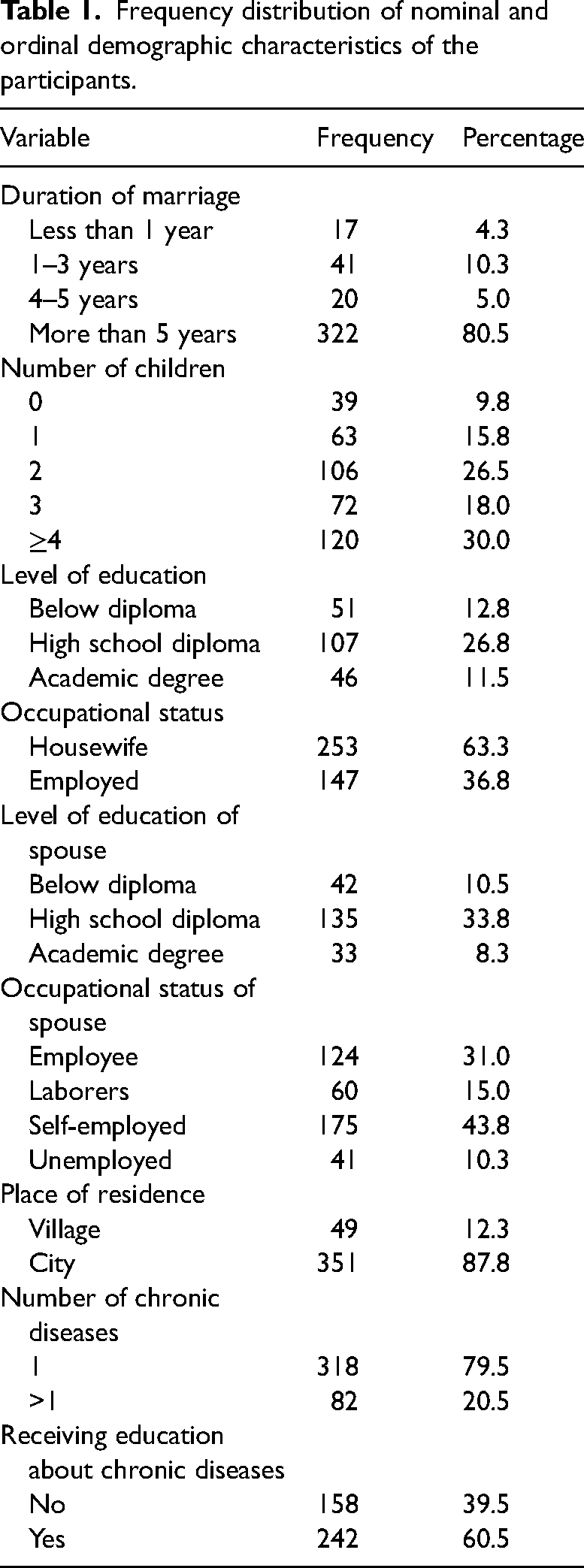
In this study, the data on 400 women with chronic illness was analyzed. In addition, 41.8% of the participants were below the age of 40 years, 46% were from 40 to 59 years old, and 12% were 60 years old or over. The mean and standard deviation of the disease duration was 4.63 ± 5.02 years. The demographic characteristics of the patients are also listed in Table 1.
Frequency distribution of nominal and ordinal demographic characteristics of the participants.
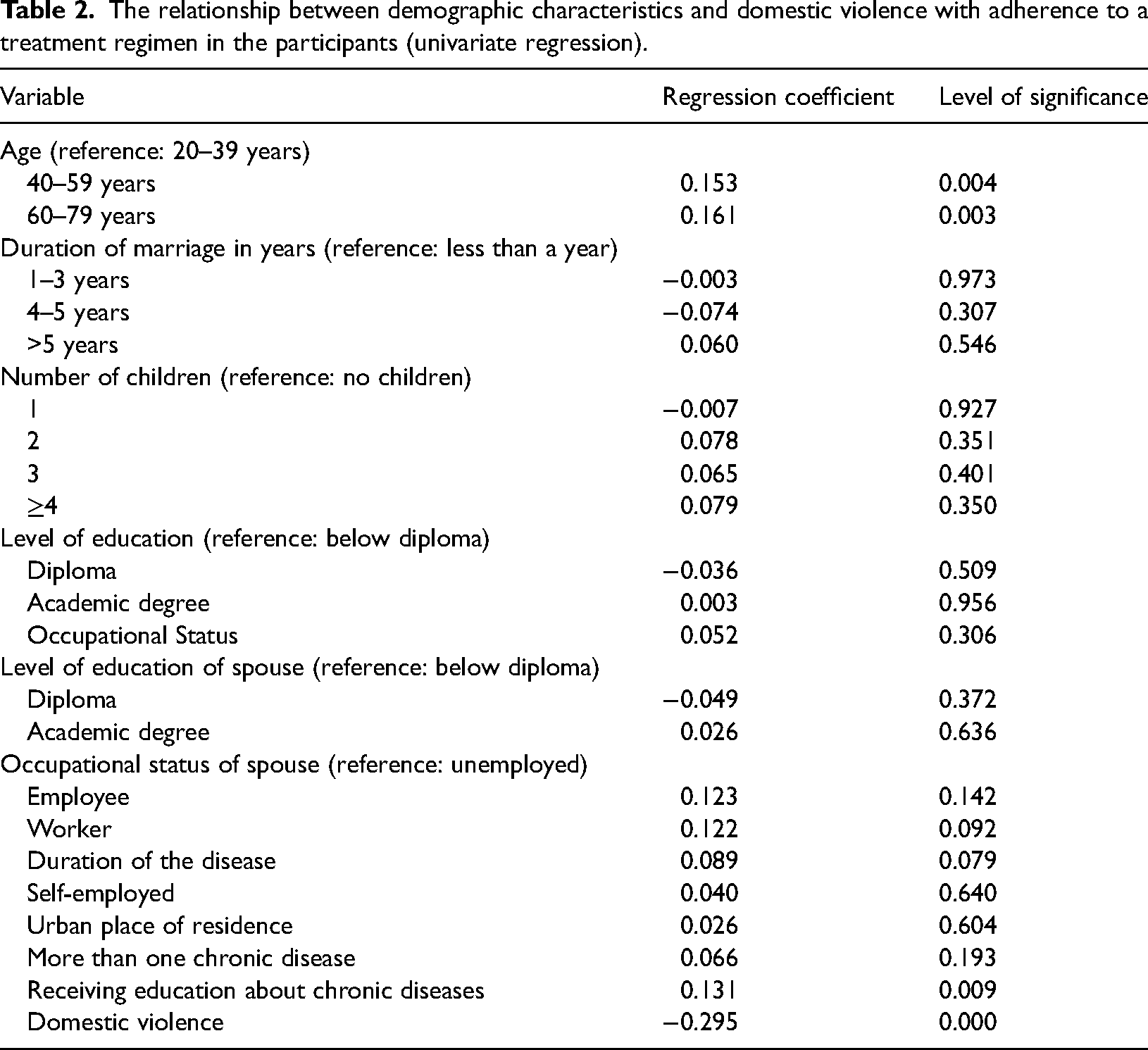
The univariate regression coefficients and the significance level of the demographic characteristics, as well as IPV and treatment adherence as the dependent variables are presented in Table 2. The variables that were related to treatment adherence in the univariate regression were included in the multivariate regression to carry out a more precise analysis of this relationship. The results of the univariate regression are presented in Table 3. As shown in the results, the age group of 40 years and over receiving education about chronic illness had a positive relationship with treatment adherence, while IPV had an inverse significant relationship with treatment adherence.
The relationship between demographic characteristics and domestic violence with adherence to a treatment regimen in the participants (univariate regression).
Predictive variable for treatment adherence (multiple regression).
Discussion
The overarching goal of this study was to analyze the role of IPV as a predictive indicator of treatment adherence in women with chronic illness. The results are indicative of the predictive and inverse role of IPV in treatment adherence in women suffering from chronic illnesses. The previous studies are mostly centered on the effect of IPV on treatment adherence in HIV-positive women. These studies have revealed that HIV-positive women who experience IPV are less likely to follow through their treatments.19–21 Although these studies are not similar to the present study with respect to the nature of the diseases, they are similar to the present study in terms of the consequences of exposure of ill women to an intimate partner's violence. Mathew et al. 22 indicated that women who experience IPV exhibit more unhealthy behaviors. Gass et al. 23 also argue that unhealthy behaviors such as smoking and drinking are more common in people suffering more domestic violence, while they opt less for health-related behaviors such as seeing a physician.
Studies have pointed to the role of family support in treatment adherence. 9 Studies have also indicated that the spouse is the most important source of support.8,9,24 Husbands who are violent to their wives are not only unsupportive but also adversely affect health-improving behaviors such as treatment adherence in various respects. IPV of any kind can cause stress and anxiety in a victim of violence and can make her living environment unsafe. 25 A patient may feel more stressed than a healthy individual for being ill and IPV can increase their stress. Kretchy et al. 26 showed in their study that stress prevents adherence to medication in patients with blood pressure. The economic aspects of intimate partner abuse including obsessive controlling over the household expenses, not paying for the expenses and providing enough money for one's wife, and controlling a woman's income can adversely affect the access of a victim of violence to the requirements for treatment adherence such as buying medication, healthy nutrition, etc. in addition to causing stress to her. In a study of patients with tuberculosis (TB), over 80% of the participants mentioned financial struggle as a reason for their lack of treatment adherence. 27 The results of a meta-analysis also showed that a better financial standing can contribute to more treatment adherence. 28 Isolating a woman and preventing her from socializing with her family and friends, which are other examples of IPV, can help explain and interpret the effect of IPV on treatment adherence. Chronically ill women, who are not allowed to socialize with other people or even with their families, and are prevented from leaving their houses, will certainly have fewer opportunities to benefit from support of their family, brothers, sisters, and friends, and even have difficulties meeting with their healthcare providers, especially in countries like Iran, which still suffer from lack of community-based care. As regards the mechanism and the effect of IPV on reduced treatment adherence in women with chronic illness, perhaps the decreased sense of coherence in the victim might also play a role. If family members do not react to each other's needs and concerns, a sense of responsibility and solidarity will not emerge in the family. As a result, the problems can affect the patients’ ability to accept and manage their diseases. 29 Bergman et al. 30 studied patients with myocardial infarction and reported that the sense of coherence plays an important role in disease management and life after myocardial infarction. Given the adverse effect of IPV on treatment adherence in women with chronic illness, healthcare providers including physicians and nurses must specifically recognize this important factor that affects the treatment process in addition to diagnosis, pathophysiology, and treatment of the disease. Screening women with chronic illness that are exposed to intimate partner violence, referring women who have been abused by their intimate partners to the appropriate counselors and adding family-based education to the treatment regimen of these women can help reduce IPV and increase treatment adherence.
In the present study, there was a direct relationship between older age and treatment adherence. It is also worth noting that the relationship between age and treatment adherence is weak. Several previous studies showed an increase in treatment adherence with age.1,24,31 However, Amininasab et al. and Algbbani et al. indicated that there is no relationship between age and treatment adherence.32,33 Uchmanowicz et al. 34 found that adherence decreases with age. A meta-analysis showed that although there is a relationship between age and treatment adherence, this relationship is weak. It seems that the difference in the results arises from the difference in the study population in terms of the type of care or training provided or even the difference in the research scales used. It is noteworthy that at any age, there are several factors that can affect treatment adherence. These factors cause the similarities between different age groups in terms of treatment adherence. For instance, young patients have a higher level of self-care ability than others because changes caused by ageing including reduced sight, hearing, and cognitive abilities of the patient lead to their inability to perform self-care activities. 35 Furthermore, young individuals may perceive the severity of a disease on a lower level. 2 Hence, intervention programs should be designed for any age based on the factors influencing treatment adherence.
The results showed that the education variable was also a predictor of treatment adherence and had a significant direct relationship with treatment adherence. This finding is in line with the studies of the effect of education on treatment adherence.4,8,36 A plethora of research supports the role of education in management of chronic illness, while it is also stressed that all approaches lead to a significant change in behavior. 5 Because behavior change is complicated and complex and a change in related knowledge, attitudes, beliefs, and behaviors has to also occur. 36 It is worth stating that despite the effect of education on treatment adherence, over one-third of the patients in the present study had not received any education about their illnesses, hence there is need for paying more attention to education by healthcare providers.
Limitations of the study
One of the important limitations of this study was the use of convenience sampling technique. Thus, it is suggested that random sampling be performed in the future studies. Given that this research is a cross-sectional study, it is affected by the limitations of cross-sectional research and the specified relationships should not be interpreted causally. This study was conducted in a research environment with geographical constraints and special sociocultural characteristics. In addition, the cultural and family contexts, and patriarchal beliefs of some of the women in this study hindered an accurate understanding of IPV. To wit, they might have considered many violent behaviors normal. Therefore, the results of the present study should be generalized to other societies and cultures with caution. Another limitation on this study concerns the collection of data using the self-report method. This could lead to sample-related biases, such as response or memory biases that may result in overestimation or underestimation.
Conclusion
The results of this study showed that IPV in women suffering from chronic illnesses is an inverse predictor of treatment adherence. Moreover, education about diseases improves treatment adherence. Screening women with chronic illnesses based on exposure to IPV, referring women exposed to IPV to the related counselors and adding family-based education to the treatment plans of these women might help reduce IPV and increase treatment adherence.
IPV often has a major psychological or physical impact on the lives of women and that can interfere with treatment adherence of women with chronic illnesses. Healthcare providers, especially nurses must pay attention to other risk factors for poor adherence. They can identify those patients who have suffered from IPV through screening and refer them to counselors and family helpers. In addition, it is highly vital that managers and health planners implement policies to increase the level of awareness of healthcare staff on how to provide appropriate care to abused female patients.
Footnotes
Acknowledgements
This study was conducted after obtaining a permit from the committee of research and ethics of Bushehr University of Medical Sciences (IR.BPUMS.REC.1398.009). Study objectives description, confidentiality participation and completing the consent form were considered. The authors hereby express their gratitude to the esteemed Vice Chancellor of the Research and Technology Department of Bushehr University of Medical Sciences and all the women who participated in this project.
Contributorship
RB and HV were involved in study design, PSN and TG in data collection, RB in data analysis including statistical analysis, PSN in manuscript (first draft), and HV and RB in data interpretation. PS and TG contributed to the development of the first draft. HK and RB performed critical revisions for important intellectual content and HKwas involved in study supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.