
Abstract
Objective
Type 1 diabetes is one of the most common chronic conditions in young children and adolescents. During the period of adolescence, young people with diabetes often struggle with self-management and have compromised health-related quality of life. This often leads to familial conflicts affecting all family members negatively. The aim of this study is to provide qualitative insight into the everyday life of families with adolescents with type 1 diabetes.
Methods
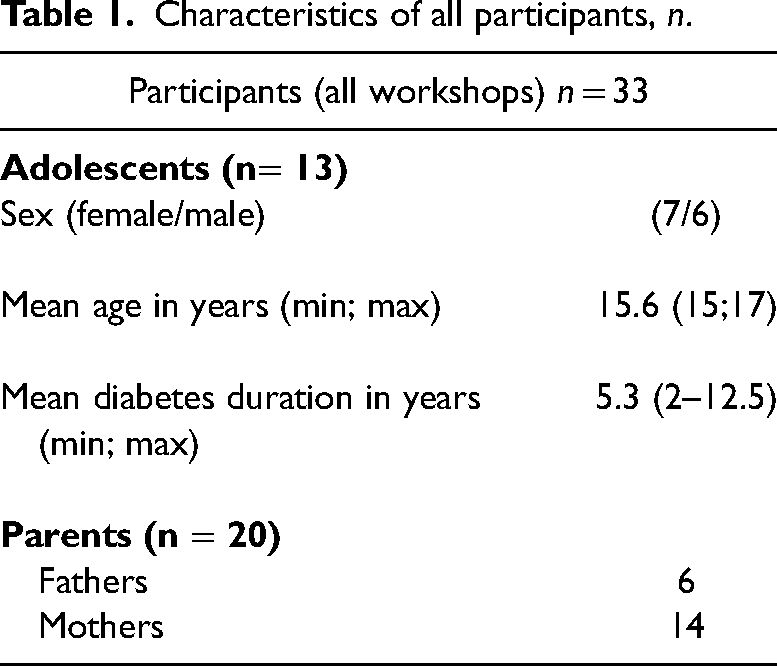
The data consisted of participatory family workshops conducted using interactive dialogue tools. The total number of participants was 33 (adolescents n = 13, parents n = 20). The adolescents were between 15 and 17 years. The data were analyzed using systematic text condensation.
Results
The results showed two main themes. The first theme, Diabetes-friendly and unfriendly social contexts, highlighted how the (dis)comfortability of disclosing diabetes was a significant factor in achieving optimal metabolic control. For parents, it affected their perception of social support. The second theme, incongruent illness representations among family members, dealt with the extended family conflict during the period of adolescence.
Discussion
Insights from our study could help healthcare professionals apply a family-centered approach minimizing family conflict and supporting metabolic control when consulting families with adolescents with type 1 diabetes.
Introduction
The prevalence of type 1 diabetes (T1D) is expected to increase worldwide. 1 The disease often debuts during childhood and is one of the most common chronic conditions in young children and adolescents.2–5 T1D is characterized by an absolute deficiency of insulin secretion. The pathology includes the presence of insulin antibodies, creating an autoimmunity that destroys insulin-producing beta cells. 3 The etiology is still unknown.2,3 T1D is universally dependent on management behavior, and failure to regulate blood glucose can result in macro and microvascular complications.6,7
The adult brain is capable of understanding and making choices in relation to the management of diabetes. The developing brain, however, may have difficulties, as it processes information more primitively. 8 Going through adolescence with T1D requires strict self-management discipline while balancing both cognitive and physiological changes.8–10 At the same time, adolescence is a period in which a natural distancing from parents takes place, as the adolescent establishes autonomy by challenging authority.5,10,11 For this reason, optimal management is often compromised during this phase of life, affecting glycemic control negatively. The implications of such structural changes often lead to the rearrangement of familial structures and routines.12–15 Epidemiological studies have shown that adolescence is the age group with the worst glycemic control. 4 Christie 8 suggested this being because adolescents begin to understand the complexity of the interacting mechanisms of their illness, but are not yet fully capable of understanding the longterm consequences of not being regulated, which compromises adherence to treatment.
Living with poorly regulated diabetes affects the individual on a wide range of health parameters. Studies have shown that, on a cognitive level, poorly regulated diabetes can affect quality of life. 4 Physiologically, hormonal levels affect disease parameters leading to overall poorer somatic health. 16 Psychosocially, associating positively with peers is important and seems to influence the decision-making process in self-management, distress, negative moods, and negative self-image/confidence—all of which are factors that affect poor glycemic control.11,17,18 One quantitative study revealed how the age group of emerging adults (18–25) rated themselves as having the lowest Health-Related Quality of Life (HRQOL) compared to other age groups. 19 This was confirmed by Fischer et al. 20 who looked at adolescents and young adults aged 7–27, showing how increasing age is a significant determinant of low rates of HRQOL and low ratings of HRQOL correlated with poorly regulated blood glucose. In contrast, a study by Laffel et al. 21 showed how the quality of life among children and adolescents with diabetes aged 7–17 is the same as that among controls; however, discrepancies in HRQOL were seen in reports of diabetes-specific family conflict. This finding suggests that diabetes-specific family conflict could cause the low ratings of HRQOL seen in multiple studies within the age group of emerging adults.19,20 Thus, to increase the quality of life, there is a need for interventions focusing on reducing diabetes-specific family conflict. This is important, as evidence indicates that reducing diabetes-specific family conflict also improves glycemic control during the period of adolescence and further into adult life.9,15
Families with adolescents with T1D have been investigated previously. However, most studies have been quantitative14,21,22 or focused either on very wide age groups (4–17 years)14,20,21 or on emerging adults age (18–25 years). 9 We see a gap in that not enough qualitative research has been conducted on families with adolescents in the age group of 13–18 years. Investigating family dynamics in a narrower age group of adolescence could aid healthcare professionals (HCPs) in facilitating diabetes management in families more effectively and from an earlier age, possibly even preventing the low HRQOL ratings and poor glycemic control seen in the later period of adolescence and early adulthood.19,20
Our study aims to provide qualitative insights into life with T1D from the perspectives of both parents and adolescents (ages 15–17). We have utilized the concept of illness representations by Leventhal 23 to analyze data looking into the influence of social context and incongruences in illness representations among, respectively parents and their adolescents. We found incongruences in identity, perceived consequences of threat caused by diabetes, the threat's causal mechanisms and coherence in the perception of illness. 23 Our findings contribute with knowledge to the development of a family-centered approach that HCPs working in pediatric clinics can apply when consulting with families with adolescents with T1D.
Methods
Sampling and recruitment
Empirical data were gathered through three interactive family workshops with parents and their adolescents with T1D. Participants were recruited by HCPs during regular clinical visits. If families showed an interest, HCPs mediated contact between the participants and the research group. The research group then contacted the families, providing relevant information about the workshop and what participation involved (Table 1).
Characteristics of all participants, n.
Research methodology—Workshops
We used workshops as a method to enhance the participants’ own interests relevant to the domain in question while producing empirical data. 24 Throughout the workshop, we used dialogue tools from The Family Toolbox 25 to facilitate peer-to-peer dialogue. The exercises included storytelling about time of diagnosis, drawing a line on the floor and asking participants to place themselves on the line to indicate how much space diabetes takes up space in everyday life and selecting picture cards/quotes to describe experiences with different types of support. Because The Family Toolbox 26 was originally designed to target people with type 2 diabetes, 25 the exercises were adapted to families with T1D, excluding picture cards and quotes specifically related to type 2 diabetes. The workshops consisted of two main sections. First, the families were gathered in a large group, with the purpose of facilitating communication across the participating families. Second, participants were divided into separate groups of parents and adolescents. This was done to enhance peer-to-peer communication. All three workshops followed the same agenda and were facilitated by the researchers (DG and MVI). Each workshop lasted around 2 hrs and was audio-recorded. The transcribtion was made verbatim by SH.
Ethical considerations
The study was conducted in compliance with the Helsinki Declaration, approved by the Danish Data Protection Agency (Rec. No.: 1-16-02-606-18) and processed by the Regional Committee on Health Research Ethics. Prior to the study, participants signed a written consent form indicating their agreement to participate on a voluntary basis. This agreement was based on information about the purpose of the study, the participants' anonymity and their right to withdraw at any time. As all adolescents were under 18, their written consent was obtained through their parents.
Data analysis
The analysis was based on Systematic text condensation, a tool for systematically classifying and coding themes Identified in qualitative data. 27 Systematic text condensation is a step-by-step process enabling the condensation of large amounts of data into meaning units, from which themes are developed. The analysis included the following steps: 1) reading through all transcripts to get an overall impression; 2) development of meaning units by identifying and sorting data from themes to codes; 3) encoding themes to meaning—“condensation”; and 4) synthesizing meaning-creating descriptions. The primary analysis was conducted by LNJ and SH while engaging DG, PS, and MVI in the consensus around identified meaning units. All quotes and identified themes were translated from Danish to English by SH.
Findings
The main findings of the present study showed that social context and incongruences in illness representations had a major impact on the daily lives of the family members participating in the workshops. The first theme, Diabetes-friendly and -unfriendly social context, played a great role in the (dis)comfortability of disclosing diabetes, which, in the case of adolescents, could hinder optimal metabolic control, and for parents, could affect their perception of receiving social support. The second major theme, Incongruent illness representations among family members, contributed to explaining the extended family conflict during the period of adolescence, thus providing insight into the difficult balance between autonomy and control affecting the parent–child relationship during this period.
Diabetes-friendly and -unfriendly social contexts
Social context covers both peer relationships and social settings, such as the classroom, sports, and friends’ houses. Social context was found to play a major role in the adolescents’ lives. The extent to which diabetes was included in the adolescents’ everyday lives varied. Social context and norms were major contributors to the disclosure of diabetes, and because social context could be perceived as either “diabetes friendly” or “diabetes unfriendly,” diabetes management behavior was typically adjusted to perceptions of the social context. One adolescent explained that it felt normal to measure blood glucose and take insulin at a friend's house, but not at school, the reason being that the friend's parents were “totally cool” about it. However, at school, management behavior drew unwanted attention and was therefore difficult to maintain. It was evident how contextual the degree of perceived “normality” of diabetes was, and how important it was for the adolescent to have an autonomous choice regarding how comfortable she/he was with disclosing diabetes: “It depends on where you’re at, because if you’re at someone's house; because it's your friend's house, and you know them and have been there many times, then their families also know that you have diabetes and stuff like that, and then it's all natural that you measure your blood sugar and do all the managing. Then there are other places where it's not as natural” (Adolescent girl, 15 years)
The aspect of “normality” in relation to the disclosure of diabetes became evident in the next quote, where the adolescent was doubtful about how to integrate diabetes into his everyday life with peers. He expressed a strong fear of becoming a burden to hi fellow classmates because of his diabetes: “ I just think I’m a bit scared about the thing about how to tell them. I don't want to be the one saying things like: ‘hey wait for me because I’m different” (Adolescent boy, 16 years).
The two quotes illustrate how a specific social context can become a determinant of whether diabetes is perceived to be part of the “normal” everyday picture of the adolescent's life. On the one hand, in the first quote, the friend's house is perceived as a “safe space” to disclose diabetes because management behavior was “normalized.” On the other, as illustrated in the second quote, environments such as school, where “normality” did not include diabetes, determined the adolescent's self-management behavior, which changed to become more hidden.
When including the perspective of the parents, a similar influence of social context was seen. It was emphasized, especially by mothers, how they did not feel understood by the welfare system regarding support in handling their child's diabetes, which resulted in a perceived increased burden caused by diabetes. Parents also expressed how it was difficult to find peer support in their nearest social relations, such as at work or with friends. The impact of and frustration with this was expressed by one mother: “Well, now it's not because I have to feel, or any of us parents have to sit and feel sorry for ourselves or wait for other people to do so. I just think that when you’ve had a difficult time, and you tell your colleagues about it, or family or something, I sometimes feel it's difficult to get the understanding you really need during the hard times when everything is extra difficult’ (Mother).
Parents expressed feelings of isolation and deviation from colleagues and peer relations because their child had diabetes. This was further emphasized in a quote by a mother talking about how difficult she felt it was to gain support from her surroundings: “It can be difficult to get the precise understanding you need.” In contrast, one mother's happiness and relief about having a friend who was also a “diabetes mother” substantiated the significance of support through social “diabetes-friendly” relations: “When I get the chance to talk to someone, like this other ‘diabetes mother’ I know, I feel like the weight is taken off my shoulders. I can hear some of the same concerns and things I go through. Just by sitting here today, I feel all elevated” (Mother).
The above quotes show how social context also affected the burden of diabetes for parents. Social context contributed to determining the perceived “normality” of diabetes. The parents’ feeling of support in handling diabetes was, for the majority, dependent on the degree of understanding and support received from the social system and their everyday social relations at work and/or at home. This indicated that feeling abnormal or misunderstood increased the burden of having a child with diabetes. Such insights are in line with findings among adolescents, illustrating variations in how “diabetes friendly” a social context was perceived to be.
Incongruent illness representations among family members
The concept of illness representations was developed by Leventhal. 23 It conceptualizes the different components influencing individuals’ perception of their illness. According to Leventhal, 23 these components are beliefs regarding illness identity, cause of illness, control, consequences, and duration/timeline beliefs. Leventhal claimed that these components make up illness representations. In our study, we found that the illness representations among adolescents and those among their parents were rarely aligned. This became evident as the general characteristics of adolescence, such as the need for autonomous decision-making, often conflicted with parents’ perception of their child's responsibility for diabetes management. When the adolescents were asked about how much responsibility for illness management they perceived to have, most adolescents did not have the motivation to allocate time and effort to prioritizing diabetes management in their everyday life. However, the adolescents were eager to take full responsibility for the remaining elements of their teenage life without diabetes. Incongruence in the level of perceived adequate responsibility and in fear of the consequences of diabetes between parents and adolescents was observed very frequently: “I actually forget that I have diabetes and then when you get reminded or think about it and talk to your parents about it, you think ‘okay, F*** I will die sooner’ or ‘I will get a lot of other diseases’” (Adolescent boy, 16)
As the above quote depicts, the adolescents showed their awareness of the importance of diabetes management in preventing the later onset of complications. However, the fear and perceived susceptibility to complications had not been internalized but rather seen in a projection of their parents’ fear. Therefore, the adolescents’ motivation to adhere to management routines was often based on their parents’ fear, which resulted in a lack of consistency in management behavior.
Moreover, incongruencies were found in the components of timeline and control. The time perspective for when to begin taking diabetes seriously differed between parents and adolescents. The adolescents expressed a strong desire to be “normal” and not care about diabetes. This desire led to a tendency to ignore symptoms of poor metabolic control and reinforcement of the legitimacy of postponing worries about the onset of diabetes-related complications. Such a mindset can be seen in the following quotes from three adolescents talking about how they related to worries about complications: “Well… of course I have to make an effort to manage it, but I think that… for now I have to finish 9th grade” (Adolescent girl, 15)
“Yeah—you sort of hope, that the energy to manage will come at some point” (Adolescent girl, 17)
“Exactly, a point where you pull yourself together” (Adolescent boy, 16)
Further, the above quotes also illustrate how the adolescents acknowledged the consequences and wanted to adhere to treatment; however, the desire to “just be a teenager” and not have diabetes to care about seemed to overrule the rational motivation for adhering to treatment. This gives us an insight into the everyday life struggles of adolescents with T1D: They cannot concentrate solely on being adolescents, but also have the extra burden of an illness that requires daily management. It became clear that the adolescents were living with conflicting motives for self-management, which could help explain why adherence to treatment is limited during the period of adolescence. Such “duality” in motives for adhering to treatment was also seen in the quote below, where an adolescent was comparing the seriousness of diabetes to having cancer instead of setting a reference point of being disease-free. Changing the reference point of comparison to having another more serious illness like cancer legitimized downplaying the consequences of diabetes creating a space in which the adolescent did not have to worry about her diabetes: “But at the same time, I’m aware that I have to look at it from the positive side. I don't have cancer, and I’m not about to die. So I choose to sort of put it aside and say: ‘I do what I have to do, and then I’ll forget about it [the diabetes] because I don't think that it's that important’” (Adolescent girl, 15)
This example emphasizes the conflicting illness representations in the family. Perceptions of the seriousness and consequences of diabetes were clearly not aligned between the adolescents and their parents. For adolescents, “Not having cancer” became a reason for not thinking diabetes was “that important.” Having to manage diabetes seemed to further burden and stress the parent-child relationship, which led to a high level of in-family conflict. Parents had difficulties allocating management responsibilities to their adolescents. Parents’ need for control of diabetes management could be explained by them having been solely responsible for years. This often led to parents experiencing an internal conflict when they had to share some of the responsibility for illness management with their child, who was now becoming a young adult: “[…] ‘The worried mother’ I won't be able to let go of her no matter what. She's there all the time, even though I try to control her, and I try to play it cool, the worries are of course still there and I think they’ll keep being there, regardless of whether he is 16 or 32” (Mother)
Parents also expressed an associated feeling of not being “good enough” at regulating their child's diabetes when sharing the responsibility for illness management with their child. This showed how the all-encompassing parental need for illness control became a personal matter for the parent. Hence, diabetes regulation became a measure of parenting skills rather than a collaboration with the adolescent aimed at reaching a common goal:
“And even though he is very well-regulated and has some beautiful HbA1c levels, I still think ‘well, it could be better’” (Mother)
Further, parents’ need for control often had the consequence of the adolescent developing a compensative behavior, resulting in an even greater lack of responsibility, which could shift the focus of diabetes management away from regulation of diabetes to a conflict about how well diabetes was being regulated, causing parents and adolescents to compete about who is “right” and “wrong,” as determined by blood sugar levels: “Yeah, so this morning when I woke up, I saw that I had been low all night and immediately my mom had to show my dad and so on. “No way! Look how low you were last night!”, “Yes—no shit!” [the adolescent replies] Yeah so I think it's like- the fact that nothing happened… yeah, so that's just the way it is” (Adolescent girl, 17)
Based on these incongruencies of responsibility and consequences, it became evident that diabetes management in some families could be seen as a power game in the parent–child relationship. This was further seen in a quote, where the adolescent expressed feelings about her parents not trusting her management skills: “[…] And I will control it [the diabetes], because my parents can be hysterical from time to time and always be checking up on me - even though I actually manage it just fine”(Adolescent girl, 17)
Again, parents’ illness representations conflicted with the adolescents’ illness representations, leading to tensions in the adolescent–parent relationship.
Discussion
Among the families participating in the workshops, we found that social context played a role in whether environments were perceived as “diabetes friendly” or “unfriendly,” which determined how comfortable both the adolescents and the parents felt about disclosing diabetes in social contexts. The feeling of deviating from normality in a given context (e.g., at school, friends’ homes, or while doing sports) was often expressed as the main reason for not disclosing diabetes. Parents were also familiar with the feeling of deviating from “normality” because their child had diabetes. This was expressed through the repeated emphasis on the importance of having other “diabetes parents” as friends. Further, we found a large discrepancy in illness representations within the family, which gave insights into how diabetes management could become a power game in the parent–child relationship, leading to high levels of daily in-family conflict.
The impact of social context on diabetes disclosure and implications for management
Previous research on emerging adults (15–25 years) has shown how being young with diabetes involves a constant struggle of finding the balance between accommodating “normal” illness-free living while simultaneously managing diabetes.8–10,28,29 This was also supported in our findings, where “diabetes-friendly” environments were highly impacted by social context and peer relations. In line with this, literature mentioned how social relations can be both an obstacle and a source of emotional support.9,10 This ambivalence was also seen in our study. The dilemma of disclosing or not disclosing diabetes involved fear of stigmatization, on the one hand, and needing people around who were able to provide aid, if necessary (e.g., in the event of low blood sugar), on the other hand. Commissariat et al. 11 found that disclosing diabetes was perceived as conflicting with normalcy, which was described as a feeling of being differentiated from peers. Such elements were also present in our study, as the adolescents wanted to make decisions independent of their parents by choosing which social relations to involve in their diabetes-related behavior. Certain social contexts, such as at school with peers, were described as contributing to the feeling of abnormality that made diabetes an obstacle to feeling “normal.” Consequently, self-management came to be suboptimal, as blending in and not disclosing diabetes were more attractive than risking experiencing stigma when having to self-manage in front of peers. This finding may help explain why adherence to treatment is highly compromised during adolescence. If adherence is compromised, metabolic control will be affected negatively, 30 and past studies have shown how young people with T1D experience a deviation from their peers, resulting in compromised adherence to treatment.9,31,32 Moreover, our results show that parents experience the same alienation from their peers due to having diabetes in the family. Such a discovery increases the importance of handling stigma in the entire family as not only the person with diabetes is affected by stigma, but caregivers as well.
How incongruences in illness representations between adolescents and their parents contributes to family conflict
The second main finding of the present study was revealing the incongruences in illness representations among family members. Illness representations have often been measured quantitatively through validated questionnaires measuring the five dimensions of illness representations (identity, cause, timeline, consequences, and control/cure). 33 Our study contributes a qualitative perspective on the impact of illness representations on management behavior and family conflict. In our study, when comparing the illness representations of the adolescents and their parents, a discrepancy in the postponement of the fear of consequences, a lack of perceived illness management control, and an incoherent sense of illness chronology was seen. Prior studies have shown how caregivers believed that diabetes was more chronic and had a more negative impact than the adolescents themselves believed. 34 This was also seen in our study in the form of parents’ difficulty in trusting the adolescents with shared diabetes management responsibilities. A qualitative study on the psychosocial experience of anaphylaxis, a severe chronic condition, highlighted the importance of perceived control in developing a strong illness identity. The study showed how a lack of internalized perceived control led to the rejection of an illness identity and thereby compromised adherence to treatment. 35 In our study, the adolescents expressed a lack of control of management because their parents often took responsibility for metabolic control and perceived it as a measure of their parenting skills. A meta-analysis across somatic diseases by Hagger and Orbell 36 offers insights into how components of illness representations were related to coping strategies and health outcomes. A strong illness identity was positively associated with problem-focused coping strategies and positive health outcomes. Problem-focused coping strategies involved perceived control, a chronic timeline and believing in the seriousness of the illness. In our findings, the adolescents’ management behavior was mainly motivated by their parents’ fear of diabetes complications, which resulted in postponement of management behavior and relating diabetes to a reference point of more serious diseases (e.g., cancer). This contributed to a lack of perceived seriousness and control of illness, which, according to Hagger and Orbell, 36 are determinants of a weak illness identity, leading to poorer health outcomes (e.g., metabolic control). On these grounds, it could be hypothesized that parents’ need for control of their adolescents’ management prevents the adolescents from developing a strong illness identity, which the abovementioned literature has shown affects health outcomes negatively.36,37 This could help explain why levels of family conflict are highly elevated, and why adherence to treatment is compromised during the period of adolescence.4,9,30
Relevance to further research and clinical practice
The study was conducted in a narrow age group of adolescents between 15 and 17 years. Insights into this age group give HCPs a chance to focus on prevention strategies and to intervene and prevent the poor metabolic control observed in emerging adults. 9 Further, knowledge of the cause–effect relationship between socialization with peers and adherence behavior can assist HCPs in helping adolescents handle challenges involving social relations without compromising metabolic control. Nonetheless, our findings also indicate a need to help parents create a social support system with other diabetes parents to overcome the extensive burden of diabetes caused by the experienced element of abnormality in social contexts.
Further, intervening to change and align illness representations in the family could minimize family conflict and increase adherence to treatment. Also, supporting HCPs in modifying their treatment approach from a disease-centered to a more person-centered individualized approach could lead to a more aligned diabetes management plan that allows the voices of all family members to be heard. The adolescents would be given more autonomy and thereby potentially assume responsibility for their diabetes. This would in return outweigh the incongruences between adolescents’ and their parents’ perceptions of management behavior, thus minimizing in-family conflict and increasing metabolic control during the period of adolescence. However, further intervention research, development, and testing is needed to more firmly establish if and how our results could have abovementioned impact.
Strengths and limitations
The use of workshops allowed all participants to be heard together as well as in peer groups with the adolescents and the parents separately. This format contributed with highly nuanced insights into the family dynamics and allowed peer reflections and sharing of experiences. As most literature on Leventhal's Self-Regulation Model of Illness 38 has used quantitative measures, our qualitative approach to exploring illness representations is, to our knowledge, the first of its kind in the area of T1D. Another strength is our narrow age group of 15–17 years, which allowed us to gain insights into themes of importance to this age group. One potential limitation is the risk that some participants held back sensitive information because the presence of other peers made them feel uncomfortable about disclosing personal matters in a group format. Another element to consider is the characteristics of the participants. We experience that participants agreeing to contribute to research are relatively resourceful, e.g., having supportive parents supporting the adolescents’ skills of regulation and thereby management of their diabetes. Further, our study population is fairly homogeneous, as all participants come from the same city. These factors should be considered if our findings were to be generalized to other populations. We suggest that such differentiations could be explored in future studies. The relatively few workshops conducted (three in total) could be a potential limitation of our study regarding the degree of transferability of the findings. However, as the total number of participants in the study was 33 (13 adolescents and 20 parents), and the themes emerging in the various workshops were similar, we estimated that data saturation had been reached.
Conclusion
The study provides insights into living with T1D during adolescence and into how T1D affects adolescents and parents in different ways. Our study contributes by illustrating the different perspectives on living with T1D among the various family members. One theme found to commonly affect all family members was the effect of social context on diabetes management and illness perception. On the one hand, some contexts were thought to “normalize” diabetes, which enhanced comfortability in disclosing diabetes. On the other, specific contexts contributed to participants’ feeling that diabetes is a burden, hence disclosure and level of management were naturally compromised in these social contexts. Another important finding was the emphasis parents placed on social support in having other parents of children with diabetes to talk to about frustrations and what was difficult for them. The other main theme, illness representations, contributed valuable insights into how diabetes is perceived differently among family members. By depicting and understanding the mechanisms underlying the divergent illness representations among family members, family conflict could be minimized, thus increasing the support of metabolic control.
Footnotes
Acknowledgments
All authors wish to thank the workshop participants. The authors value and respect the insights they shared, and the authors acknowledge the courage it takes to talk about sensitive experiences. The authors also thank the HCPs who helped recruit the participants.
Contributorship
Study design: MI, PS, DG; Data Collection: MI, PS, DG; Analysis: SH, LNJ; Writing original draft: SH; Writing feedback: DG, LNJ, PS, MI.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Danish Data Protection Agency (Rec. No.: 1-16-02-606-18) and carried out in accordance with the Declaration of Helsinki. According to Danish legislation, interview studies require no approval from an ethics committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
DG