
Abstract
Objectives
To identify and describe the most relevant contextual factors (CFs) from the literature that influence the successful implementation of self-management interventions (SMIs) for patients living with type 2 diabetes mellitus, obesity, COPD and/or heart failure.
Methods
We conducted a qualitative review of reviews. Four databases were searched, 929 reviews were identified, 460 screened and 61 reviews met the inclusion criteria. CFs in this paper are categorized according to the Tailored Implementation for Chronic Diseases framework.
Results
A great variety of CFs was identified on several levels, across all four chronic diseases. Most CFs were on the level of the patient, the professional and the interaction level, while less CFs were obtained on the level of the intervention, organization, setting and national level. No differences in main themes of CFs across all four diseases were found.
Discussion
For the successful implementation of SMIs, it is crucial to take CFs on several levels into account simultaneously. Person-centered care, by tailoring SMIs to patients’ needs and circumstances, may increase the successful uptake, application and implementation of SMIs in real-life practice. The next step will be to identify the most important CFs according to various stakeholders through a group consensus process.
Introduction
There is a worldwide epidemic of chronic diseases (e.g., diabetes, obesity, Chronic Obstructive Pulmonary Disease (COPD)), due to a combination of an increasingly aging population, unhealthy lifestyle behaviours and life-prolonging medical treatments.1,2 In the European Union, chronic diseases affect approximately one-third of the population and have resulted in increasing demand on healthcare use and costs, affecting society as a whole. 3 Self-management is key in decreasing the high impact of chronic diseases on individuals, societies and economies. 3 Self-management can be defined as ‘what individuals, families and communities do with the intention to promote, maintain or restore health and to cope with illness and disability with or without the support of health professionals’.4,5 Drawing on this definition, self-management interventions (SMIs) are considered ‘supportive interventions that healthcare staff, peers or laypersons systematically provide to increase peoples’ skills and confidence in their ability to manage a long-term disease’.6,7 SMIs aim to enhance people's responsibility and active participation in the daily management of their chronic disease. 4 SMIs may consist of different components (e.g., monitoring, goal setting), delivery methods (e.g., remote, face-to-face), intensity and the self-management behaviours they aim to improve. 6 Previous studies show that SMIs can improve clinical outcomes as well as patient-reported outcomes like quality of life. For example, reducing HbA1C levels in type 2 diabetes mellitus (T2DM) patients, 8 reducing weight for patients with obesity, 9 reducing exacerbations and improving quality of life in COPD patients10,11 and decreasing hospitalization in heart failure (HF) patients. 12 However, a large variation in the success of SMIs has been observed. Understanding why, when and where SMIs work most effectively is crucial for the application and implementation of interventions.13,14 So far, we know that SMI's success can be influenced by factors on several levels (i.e., patient, provider, interaction, organization and system). 14 However, it is currently unclear how these factors hinder or facilitate the successful implementation of SMIs into practice. Understanding how these factors impact the effectiveness of SMIs for chronic diseases is thus crucial. Therefore, the objective of the present study is to identify and describe the most relevant contextual factors (CFs) from the literature that may influence the successful implementation of SMIs for patients living with one of the four most common chronic diseases: T2DM, obesity, COPD and HF.
Methods
Aim
The objective of the present study is to identify and describe the most relevant CFs that may influence the successful implementation of SMIs for the four chronic conditions: T2DM, obesity, COPD and HF. 6 In this study, CFs are defined as a set of characteristics and circumstances that surround the implementation effort and may hinder or facilitate the successful implementation of intervention into practice. This definition is based on previous work on CFs.13,14
This study is part of a project called ‘Comparing the cost-effectiveness of SMIs in four high-priority diseases in Europe’ (COMPAR-EU). COMPAR-EU aims to identify, compare and rank the most effective and cost-effective SMIs for adults living with T2DM, obesity, COPD and/or HF. 6
Design
We conducted a qualitative review of reviews, allowing the findings of separate reviews to be compared and contrasted. We followed the most up-to-date methodological guidance from the Cochrane Collaboration and used the PRISMA checklist. This included, amongst others, formulating research question(s), detailed inclusion criteria, a structured search process to locate and select relevant existing reviews and a formal process of data extraction followed by means to summarize and present the data.15–18
Search strategy
We searched four electronic databases (PubMed, Embase, PsycINFO and Cinahl) using Medical Subject Headings and plain text. We used the same search blocks as in our previous study to identify publications on self-management, 19 combined with two additional search blocks for this study (see Appendix A: Tables 1–4). The search period was from 2010 to 2021.
Eligibility criteria
The inclusion criteria we applied are reported in Box 1.
The following inclusion criteria were applied:
The article is written in English. Participants have diagnosed diabetes mellitus type 2 (or if it is a mixed population of diabetes mellitus type 1 and diabetes mellitus type 2 patients at least 80% has diabetes mellitus type 2), heart failure, obesity or COPD, or if it is a mixed population of chronic diseases at least 80% must be diagnosed with the aforementioned diseases. Age of the intervention's target population is >18 years. The targeted population of the intervention is patients or (informal or formal) caregivers. Type of article is any kind of review (e.g., systematic, qualitative, meta-synthesis) concerning CFs influencing the implementation of self-management (interventions).
Screening
The process of retrieving, screening and extracting studies was applied for T2DM, and for the other three diseases combined. We first intended to do separate reviews for all four diseases, starting with T2DM. However, we decided to combine the other three diseases within a second review, based on the impression from the T2DM review that CFs were overall generic instead of disease-specific. All publications identified during the electronic database search were imported into EndNote. 20 Both title/abstracts screening and full-text screening were performed using Covidence. 21 Screening was performed by two independent researchers (for T2DM: MM and RP; for HF, obesity and COPD: MM and TR). For the full-text screening, calibration of extractors was done in two publications for T2DM (MM and RP) and in seven publications for HF, obesity and COPD (MM and TR). Disagreements were discussed until consensus, and doubts were discussed with a third experienced researcher (CW).
Extraction and analysis of CFs
Two reviewers (MM and TR) conducted extraction of CFs in the full-text papers and analyzed the data with MAXQDA 22 (i.e., software for qualitative data analysis) according to the seven domains of the Tailored Implementation for Chronic Diseases (TICD) framework (see below)13,23 and added CFs that did not fit the seven domains. Disagreements between the reviewers were discussed until consensus was reached. Doubts were discussed with a third experienced researcher (CW). The analysis was summarized in an Excel file and described (MM for T2DM and JN for obesity, HF and COPD).
TICD framework
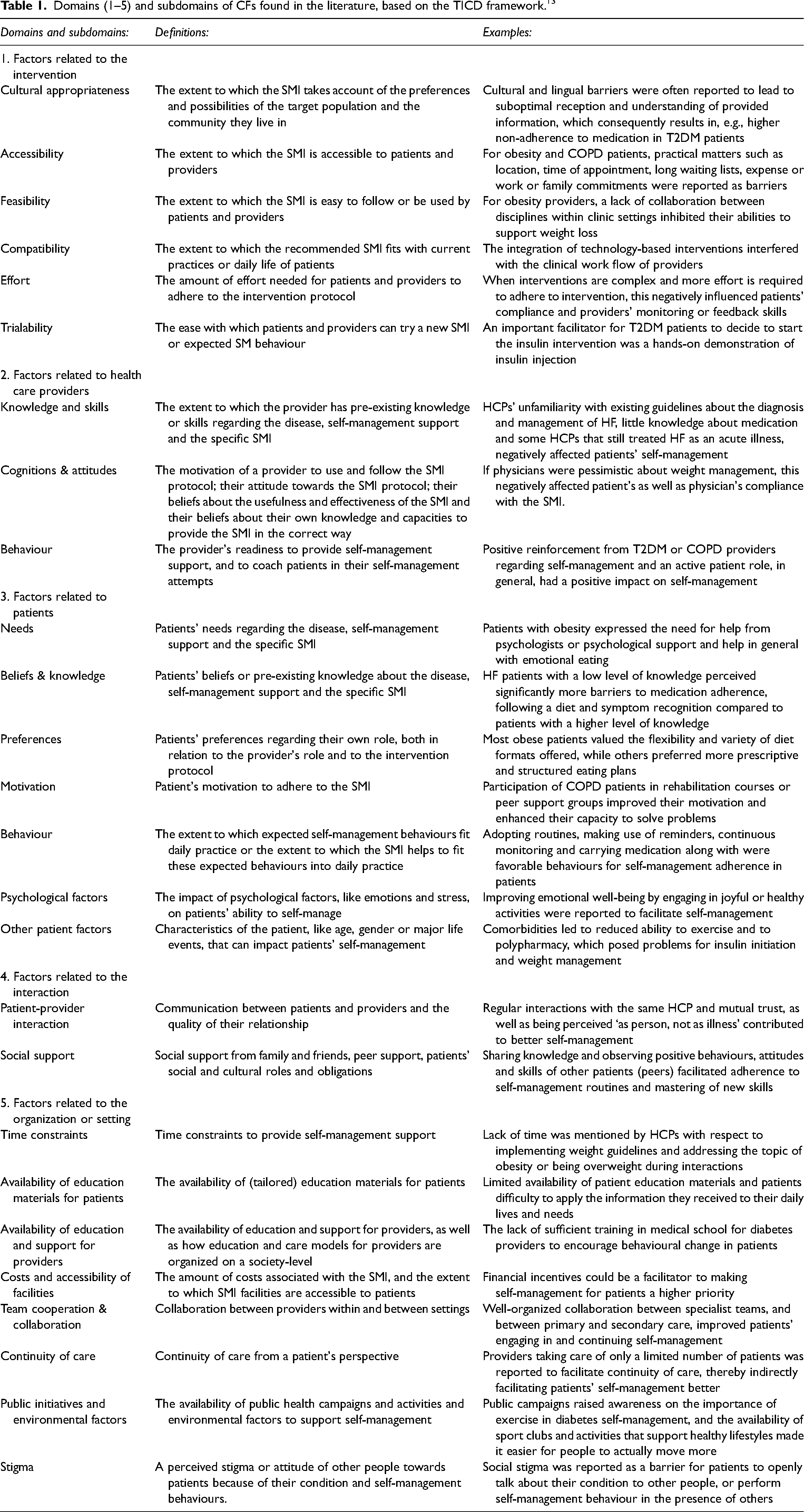
The TICD framework is a checklist for identifying potential determinants that enable or prevent improvements in healthcare professional practice. 13 The seven domains of the TICD framework include: (1) Guideline factors/factors related to the intervention (e.g., feasibility, accessibility of the intervention); (2) Individual health professional factors (e.g., knowledge, skills); (3) Patient factors (e.g., needs, preferences); (4) Professional interactions/factors related to the interaction (e.g., communication and influence); (5) Incentives and resources (e.g., financial incentives, available resources); (6) Capacity for organizational change/factors related to the organization (e.g., capable leadership, regulations); and (7) Social, political and legal factors (e.g., economic constraints, legislation). CFs in this paper are described and summarized according to the (sub-)domains of the TICD framework. We used one of the worksheets (i.e., Additional file 4), developed by the authors of the TICD checklist, to facilitate the use of the checklist and synthesize our data. This worksheet includes definitions, questions and examples of the checklist. 13 However, based on the literature findings (i.e., qualitative data analysis), some (sub)domains of the TICD framework were merged or added, or existing (sub)domains were altered to create a better fit for our findings. The domains 5, 6 and 7 of the TICD framework were merged into one domain: ‘Factors related to the organization or setting’, containing newly identified sub-domains. This resulted in a total of five domains for CFs: (1) Factors related to the intervention; (2) Factors related to health care providers (HCP); (3) Factors related to patients; (4) Factors related to the interaction between patients and HCPs; and (5) Factors related to the organization or setting. Table 1 provides an overview of the definitions of the (sub-)domains that we defined based on the CFs we found in the literature, as well as examples.
Domains (1–5) and subdomains of CFs found in the literature, based on the TICD framework. 13
Research Ethics Committee
See Declarations.
Results
Flow charts
For T2DM 540 publications were identified for screening, of which 335 duplicates were removed. Overall, 205 titles and abstracts were screened, resulting in 65 publications eligible for full-text screening. Twenty-one studies met the inclusion criteria and were included (Figure 1). For obesity, HF and COPD, 389 publications were identified for screening, of which 134 duplicates were removed. Overall, 255 titles and abstracts were screened, resulting in 69 publications eligible for full-text screening. Forty publications met the inclusion criteria and were included (Figure 2).
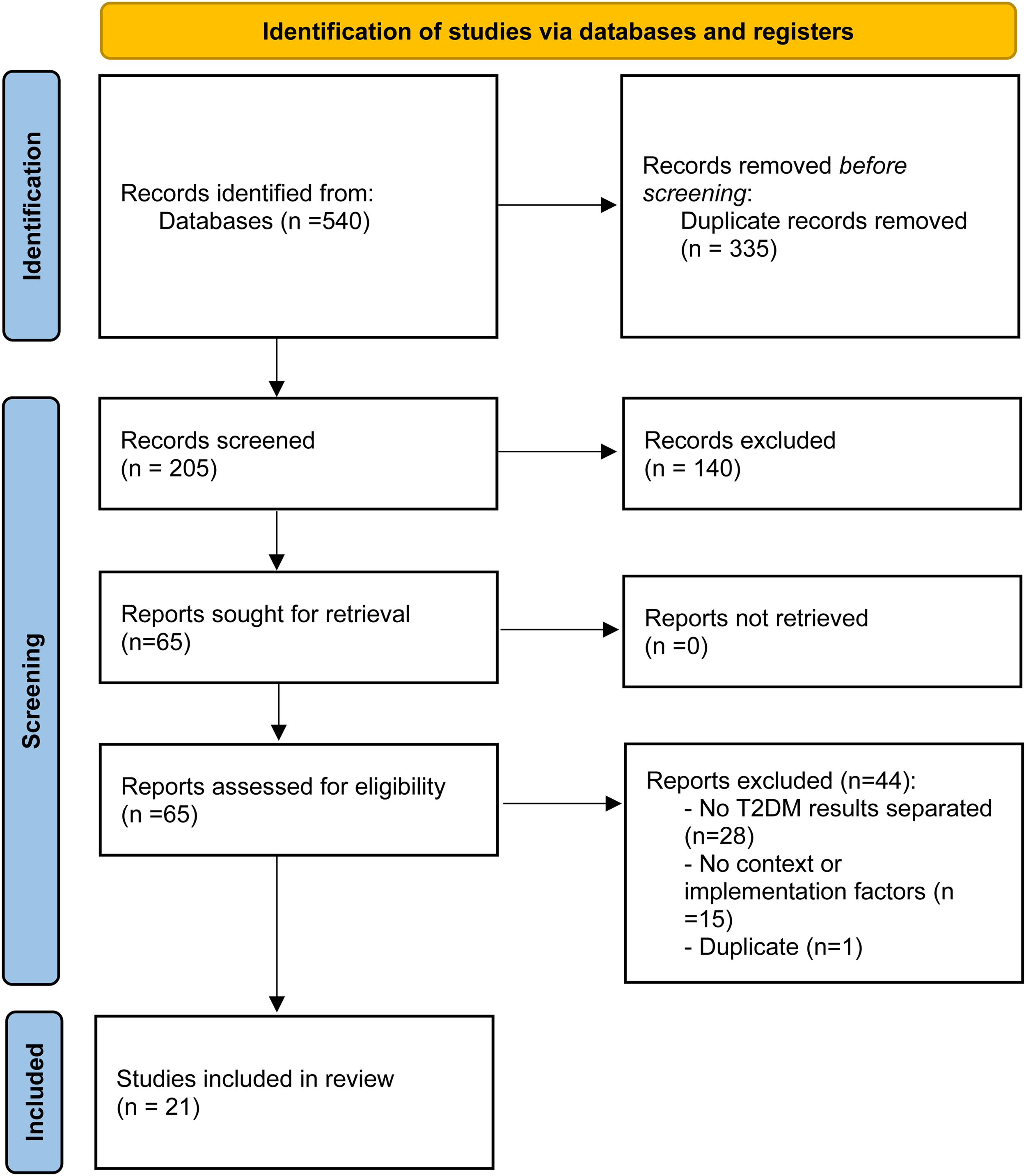
PRISMA 18 flow chart: A qualitative review of reviews for T2DM.
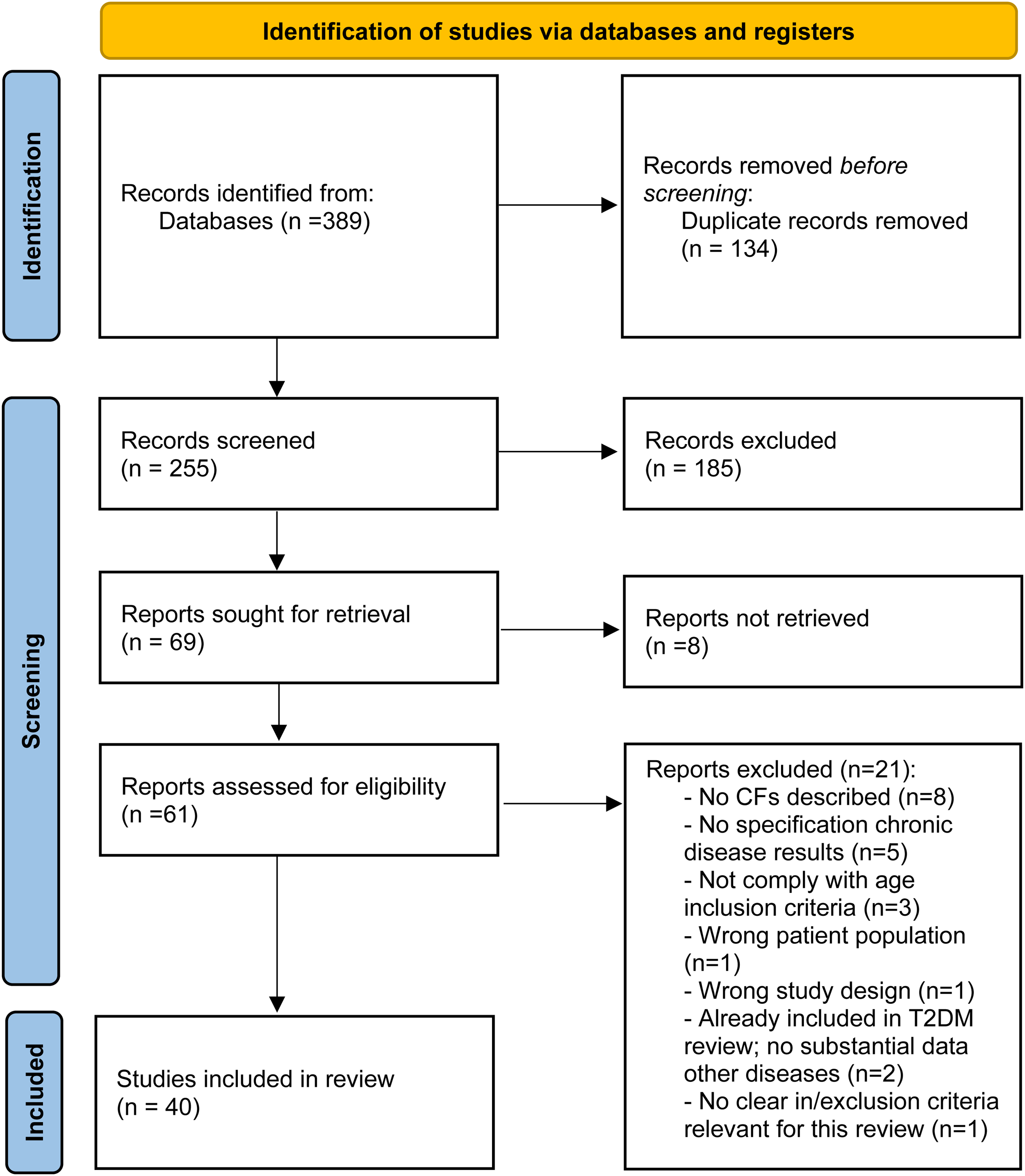
PRISMA 18 flow chart: A qualitative review of reviews for obesity, HF and COPD.
Study characteristics
Most included studies in the reviews were from the USA or the EU/the UK. Since not all reviews reported on the included countries or reported ‘multiple countries’, no exact numbers can be reported. Most reviews included studies with only patients (n = 37), of which six were on specific patient groups (e.g., minority groups, bariatric surgery patients). Fifteen reviews included patients and other stakeholders; six reviews reported only on HCPs, and three reviews reported only on caregivers. A detailed description of the included reviews is presented in Appendix B (Tables 5 and 6).
Contextual factors for the successful implementation of SMIs
Based on the included reviews, a great variety of CFs was identified (see Table 1 for CFs definitions and examples). Most of these CFs were on the level of the patient, the HCP and the interaction level, while less CFs were obtained on the level of the intervention and higher organizational and national structures. The CFs described below are related to all diseases. Examples are given for only one or two diseases to limit the amount of information, and differences are highlighted.
Factors related to the intervention
Cultural appropriateness
Reviewed studies suggest that it is important to consider whether the SMI is appropriate given the cultural background of the participants, for example, in relation to lifestyle, language or religion.24–38 For example, cultural and lingual barriers were often reported to lead to suboptimal reception and understanding of provided information, which consequently results in, for example, higher non-adherence to medication in T2DM patients.24,29,38 It can also inhibit access to health care services, such as issues with scheduling appointments, buying diabetes care products and attending education classes. 31
Accessibility
A large amount of factors was reported by reviews that can possibly influence accessibility in both negative and positive ways.39–43 For example, the use of telemonitoring was mentioned often to either improve or hinder accessibility. It was reported as a barrier when it increases patient anxiety, HCPs’ workload or threatens their professional identify, while it was described as a facilitator when it increases patient's ability for self-management.39,40,44 For obesity and COPD practical matters such as location, time of appointment, long waiting lists, expense or work or family commitments were reported as an access barrier.43,45,46 Another review described that case management was perceived by HF patients to facilitate access to overall care. 42
Feasibility
Especially feasibility barriers were found in the reviews for patients with T2DM.24,39,47,48 For example, the complexity of managing insulin has been associated with barriers that may lead to insulin non-adherence in patients with T2DM; that is, injection difficulties, patients failing to remember whether they have taken their insulin, difficulties in sustaining regular self-monitoring of blood glucose and adjusting insulin dosages due to its additional burden and painfulness, regimen inflexibility and the inconvenience of carrying an insulin pen with them and injecting regularly.47,48 Reviews including obesity, HF or COPD patients reported about feasibility barriers or facilitators related to technology.40,44,49–51 Especially, technology being too difficult to use for elderly patients.49,50 For obesity providers, a lack of collaboration between disciplines within clinic settings could inhibit their abilities to support weight loss. 51
Compatibility
When interventions do not fit with the current practices they pose a great challenge in terms of the magnitude of change required. For example, is the integration of technology-based interventions compatible with the clinical workflow of providers and does it fit in patients’ homes?39,50,52 Ensuring the fit of an intervention to the systems and regulations in practices will therefore aid the implementation of such interventions.
Effort
Several reviews reported that when interventions are complex, and more effort is required to adhere to intervention, this negatively influences patients’ compliance24,33,47,48,52 and providers’ monitoring or feedback skills.40,51 Frequent contacts allow for the repeated provision of emotional, psychological and social support, which can compensate for complexity and facilitate compliance. 48
Trialability
Several reviews reported that experience and hands-on practice of skills positively influences compliance with the SMI protocol and intervention outcomes.35,40,48,49,53 For instance, a review reported that an important facilitator for T2DM patients to decide to start the insulin intervention was a hands-on demonstration of insulin injection. 48 Hands-on practice for COPD patients to use telehealth equipment for remote monitoring was also reported as facilitator.40,49
No information was found in the reviews about the following sub-domains: the quality of the evidence supporting the intervention, the strength of the intervention, clarity and the source of the intervention. 13 However, since we focused on reviews instead of single, specific studies we did not expect to find this information.
Factors related to health care professionals
Knowledge and skills
Multiple reviews described examples in which HCPs’ lack of knowledge and skills influenced patients’ self-management behaviours.24,26,28,29,33,36,37,41,45,46,48,50,54–57 For example, a review reported about HCPs’ unfamiliarity with existing guidelines about the diagnosis and management of HF, little knowledge about medication and some HCPs that still treated HF as an acute illness, negatively affecting patients’ self-management. 37 A lack of providers’ communication skills is also considered an important barrier to successful self-management support.28,29,47,57 On the other hand, adequate knowledge and skills of HCPs, tailored communication skills and involving patients in decision-making can facilitate patients’ self-management behaviour.26,48
Cognitions and attitudes
Several reviews reported on the influence of aspects of HCP's cognition on self-management. However, cognitions and attitudes were reported differed per disease. The T2DM reviews focused on HCP's attitudes and self-efficacy with regards to medication treatment,24,57 while the HF reviews focused on HCP's attitude or self-efficacy towards telehealth, guidelines or case management.37,50 The obesity and COPD reviews described HCP's attitudes and self-efficacy towards weight management32,43,51,58,59 and COPD interventions36,40,46 in general. For example, if physicians are pessimistic about weight management, viewing it as too difficult for patients to achieve and sustain, this will negatively affect patient's as well as physician's compliance to the SMI. 58 Keeping track of patients’ weight, on the contrary, can make physicians less pessimistic. 32
Behaviour
Several reviews reported that HCPs’ behaviour influences the capacity to support self-management of patients and to provide feedback.24,32,41,48,54,58,60 For example, T2DM providers that are not inclined to engage patients in decision-making when planning treatment regimens or self-management were found to negatively affect patient adherence.24,48 This while positive reinforcement from T2DM or COPD providers regarding self-management and an active patient role, in general, have a positive impact on self-management.41,48
Factors related to patients
Needs
Few of the included reviews reported specifically on patients’ needs.39,43,53,61,62 For example, patients with obesity expressed the need for help from psychologists or psychological support and help in general with emotional eating, amongst others. 43 COPD patients expressed a need for information about their disease and care options, as well as the need for emotional support, as they mentioned being afraid to be alone during acute exacerbations. 62
Beliefs and knowledge
In general, inaccurate health beliefs and lack of knowledge amongst patients have been reported as important barriers to adequate self-management and the ability to learn new behaviour.24–26,33–35,41–43,46,49,50,53,55–57,62–68 For example, HF patients with a low level of knowledge perceived significantly more barriers to medication adherence, following a diet and symptom recognition compared to patients with a higher level of knowledge. 65 The presence of negative fatalistic beliefs can lead to passive behaviour in patients who believe that they are not able to influence outcomes of their condition.26,29,39,69 In contrast, positive beliefs such as patients’ belief that self-management leads to improvements in their health and quality of life strongly encourages long-term adherence.26,30,31,63 Health beliefs were reported to often be related to past experiences, as well as the information sources used by the patient, attitudes of other people, cultural and religious beliefs and education.24,61
Preferences
A wide variety of patient preferences regarding treatment and self-management were reported.25,28,34,42,49,50,56 Some patients want a lot of help or information from their HCP, while others want to do it themselves and/or prefer not to receive much information to minimize their anxieties about their condition.24,25 For example, a review showed that most obese patients valued the flexibility and variety of diet formats offered, while others preferred more prescriptive and structured eating plans. 51
Motivation
Patients’ motivation was reported as a key determinant for self-management adherence, such as engaging in physical activities and medication adherence, or web-based interventions.24,25,29,33,39,46,53,55,56,59,63,70,71 For example, patients participating in weight loss interventions reported that being continuously monitored by a professional motivated them to adhere, 63 as well as the sense of belonging to a group of people who share similar issues and characteristics. 59 Participation of COPD patients in rehabilitation courses or peer support groups improved their motivation and enhanced their capacity to solve problems. 56
Behaviour
Adopting routines, making use of reminders, continuous monitoring and carrying medication along, amongst others, are favorable behaviours for self-management adherence in patients.53,56,61,70,72 On the other hand, behaviours of intentional non-adherence were reported, including adjusting doses or not taking medication (timely), due to inaccurate beliefs or to avoid side-effects.24,26,29,57,61
Psychological factors
Psychological factors and emotions can both impair or enable patients’ self-management. For example, positive thinking, acceptance of the condition, perceived self-efficacy and empowerment were associated with more motivation and better engagement in self-management.24,26,28,40,44,70,71 In addition, improving emotional well-being by engaging in joyful or healthy activities was reported to facilitate self-management.26,51 Negative emotions, such as fear of complications, stress, helplessness, guilt, anxiety and depression, compromised people's participation and adherence in self-management activities.24,26,30,31,43,47,48,50,51,53,57,59, 61,62,64,68,70–72 However, fear of dying or hospitalization was also found to sometimes result in seeking professional help or raising adherence.24,53,55
Other patient factors
Several patient characteristics can impact their ability to self-manage. For example age,48,67 gender,26,38,73,74 cultural background,33,47,63,69,74,75 being part of a minority group, 63 technical skills, 39 language, 39 health literacy, 39 socioeconomic status,26,48 occupational circumstances,57,70 comorbidities,24,26,33,41,48,50,51,57 physical or cognitive impairments24,41 and major life events such as pregnancy, divorce or house moves. 70
Factors related to the interaction
Patient–provider interaction
The communication between patient and provider and the quality of their relationship were described in multiple reviews as impacting patients’ self-management behaviour.27,28,32,34,36,43,47,48,50,54,58–60 Both can be influenced, amongst others, by a provider's communication skills and expertise,24,27,34–37,43,46,47,66 patient characteristics,24,25,27,32,34–36,43,47 conflicting views of care,24,26,43,47,74 and (a lack of) continuity of care.25,28,34,37,43,51,56,59 Examples of communication skills that have a positive effect on patient's ability to self-management are showing empathy, active listening, providing emotional support and non-judgmental communication.25–27,31,43,61 Moreover, regular interactions with the same HCP and mutual trust25–28,31,43,51,56,59,61 as well as being perceived ‘as person, not as illness’ contribute to better self-management.24,25,42,43,47,50 Barriers include HCPs providing incomplete or irrelevant information, a lack of shared decision-making, a mismatch between patients’ and providers’ expectations and beliefs, and conflicting advice between different providers.32,43,58
Social support
Receiving (no) social support from friends, family, work colleagues or peers was often reported to influence self-management significantly. Social support may include emotional (e.g., showing concern, offering reassurance), physical (e.g., assistance with managing tasks, helping with food preparation) and instrumental support (e.g., financial support).30,31 In general, support from family or friends increased patients’ self-efficacy, motivation and commitment to lifestyle changes, and it encouraged treatment adherence. Sharing knowledge and observing positive behaviours, attitudes and skills of other patients (peers) can also facilitate adherence to self-management routines and mastering of new skills.24–26,28,33,35,39,41,50,51,54–56,60,67,68,70,71,73,75,76 However, family, friends and peers may also exert a negative influence on patients’ self-management behaviour when they are not supportive.26,28,29,33,38,47,51,68,69,71,73–76 Although social and cultural roles and obligations that patients take upon themselves may in some cases act as a facilitator to self-management, they are more often reported as a barrier.29,30,55,56,69–71,73,76 For example, combining managing the household or childcare with self-management was often experienced as a challenge for patients, since the needs and desires of their family members may clash with their self-management. 76
No information was found about the subdomain: ‘communication and influence’. 13 The sub-domains ‘team processes’ and ‘referral processes’, in the original TICD framework part of the domain interaction, are included in the organizational and setting domain in this review.
Factors related to the organization or setting
Time constraints
Time constraints were reported to hinder self-management support for patients. Time constraints included limited available consultation time and high workload of the provider,24,25,28,34,48,74 difficulty making appointments for patients, 34 and lack of time for follow-up and monitoring of patients. 37 For example, a lack of time was mentioned by HCPs with respect to implementing weight guidelines 58 and addressing the topic of obesity or being overweight during interactions, 32 and as a general barrier to behavioural change. 71
Availability of education materials for patients
The availability of patient education material was deemed important for self-management by both HCPs and patients in the reviews. Some reviews expressed concerns about the limited availability of patient education materials.46,57 Patients specifically valued information on the nature of the disease, its underlying processes in relation to the symptoms and its long-term consequences, as well as how medications work, the influence of lifestyle factors and management strategies. 24 However, some patients found it difficult to apply the information they received to their daily lives and needs. 69 Patient education materials need to be tailored to patients’ language, cultural background and health literacy.24,38,69,74
Availability of education and support for providers
In general, reviews reported that more professional education is necessary to keep the HCPs’ knowledge and skills to support the patients’ self-management up-to-date.25,28,46,47,50 For example, the lack of sufficient training in medical school to encourage behavioural change was mentioned by diabetes providers. 57 Absent, inadequate or delayed staff training was also reported as a barrier for HF patients to engage in self-management activities. 50 The availability of protocols and information technology (for long-term follow-up) in the organization could positively affect care and self-management.32,57
Costs and accessibility of facilities
Costs or accessibility of facilities can hinder or facilitate patients’ self-management. Costs include costs of the SMI itself, (non-)reimbursed care (out-of-pocket payments), costs of medication and associated costs of transport and health-promoting activities (e.g., buying healthy foods and attending exercise programs). Although most costs were reported as a barrier to self-management,24,28,29,33,39,41,43,45,47,49,54,55,60,69,73, 74,77 financial incentives could also be a facilitator to making self-management for patients a higher priority. 44 With respect to the accessibility of facilities, this includes for example translation services for those speaking a different language, 29 culturally appropriate physical activity facilities (such as gender-specific classes), 29 referral opportunities43,46,58 and technological access,40,50 amongst others.41,62,68
Team cooperation and collaboration
Mainly barriers are reported in the reviews related to a lack of team cooperation between providers and wide collaboration and integration of care to support patients’ self-management,28,50 as well as a lack of clarity with regards to professional roles (i.e., responsibility and coordination) within teams42,57 and lack of interdisciplinary working within clinical settings.51,58 On the other hand, well-organized collaboration between specialist teams, and between primary and secondary care, could improve patients’ engaging in and continuing self-management.28,47,57
Continuity of care
The importance of continuity of care was addressed by multiple reviews.25,28,34,37,43,51,56,59 For example, providers taking care of only a limited number of patients were reported to facilitate continuity of care, thereby indirectly facilitating patients’ self-management better. 28 A long-lasting, trusting relationship with their HCP could make patients more willing to accept and comply with being held accountable for their behaviour by their HCP. 25 Also, consistent staffing by knowledgeable HCPs that are aware of the intervention goals will facilitate implementation. 45
Public initiatives and environmental factors
The availability of campaigns and activities in the community to support self-management and environmental factors can influence self-management. For example, public campaigns could raise awareness on the importance of exercise in diabetes self-management, and the availability of sport clubs and activities that support healthy lifestyles will make it easier for people to actually move more.28,57 Facilitating environmental CFs are the presence of parks, clean air and a mild climate. 31 On the other hand, a lack of community safety or an unsafe environment (i.e., traffic and darkness) can be barriers to self-management.71,75
Stigma
Social stigma can be a barrier for patients to openly talk about their condition to other people, or perform self-management behaviour in the presence of others.26,32,47,56 For example, one review reported that many patients with T2DM are concerned to offend others by injecting insulin in public. 47 In an obesity review, it was addressed that the stigmatized attitude towards obese patients was especially apparent in the included papers focusing on patients with low incomes or those from a certain ethnic background, resulting in less frequent counselling of these groups. 32
No information was found in the reviews about social, political or legal factors. However, one review mentioned ‘inadequate supporting of policy and legislation’. 50
Discussion
Summary of main findings
Our qualitative review of reviews identified a great variety of relevant CFs for the successful implementation of SMIs across four chronic diseases. Most of these CFs were on the level of the patient, the HCP or the interaction level, while less frequently on the level of the intervention or the macro level. Although CFs are presented on different levels in this review, for the successful application and implementation of SMIs it is crucial to take CFs on several levels into account simultaneously.
We identified that person-centered care, which includes tailoring SMIs to patients’ preferences, needs and circumstances increases the successful uptake, application and implementation of SMIs in real-life practice. No differences in main themes of CFs across all four diseases were found, although examples per theme regularly differed per disease. For example, while several reviews reported on the influence of aspects of HCP's cognition on self-management which cognitions were reported differed per disease (e.g., T2DM reviews focused on HCP's attitudes towards medication treatment, HF reviews reported on HCP's attitude towards telehealth, guidelines or case-management). Finally, the included reviews did not report on CFs for all the domains and sub-domains of the TICD framework. 13 Especially CFs on the intervention level, organizational and national levels were reported less often. Although we did not expect to find many intervention-level CFs due to a focus on review studies instead of single studies, it is likely we do have an underrepresentation of CFs on the macro level. This does not mean that these intervention and macro-level CFs are not important or should not be taken into account when implementing SMIs.
Comparison with existing literature
So far, few studies have systematically examined the complex relationship or association between CFs and the implementation of interventions. However, to our knowledge, none of these studies focused specifically on SMIs. For example, Kaplan 14 and Kringos 78 focused on the influence of CFs on the implementation of quality improvements, and Fleuren 79 focused on determinants for the implementation of innovations. Another study specifically focused on organizational- and system-level CFs that influence the implementation of shared decision-making. 80 Most comparable is the TICD framework that identified CFs to improve healthcare for patients with chronic diseases.13,23
Previous studies also reported that tailored (self-management) interventions can improve healthcare.13,23,81 For example, a recent study found that acting on the preferences of chronically ill patients with limited health literacy and building a solid relationship will enhance successful self-management. 82 However, the effect of tailored implementation is variable and tends to be small to moderate.81,83 An important issue raised previously is how to prioritize CFs and tailored interventions, as well as to explore the actual tailoring of SMIs in practice. 83 These previous findings are relevant for this study since as a next step we will prioritize CFs through a consensus process with different stakeholders, as part of the COMPAR-EU project. 6
Strengths and limitations
To our knowledge, this is the first qualitative review of reviews focusing on CFs for the successful implementation of SMIs, across the four chronic diseases in this review. It covers a wide range of both facilitators and barriers to the implementation of SMIs, and therefore, forms an insightful reference document for future SMI research. Another strength is that we compared five implementation frameworks79,80,84,85 before deciding on the TICD framework, 13 which fitted our data rather well. To create an even better fit we slightly adapted the framework based on our literature findings, e.g., by adding or altering CFs. Furthermore, the adapted domains for organization and setting (e.g., team communication and coordination, available education and recourses) are consistent with the findings of Scholl. 80 Therefore, we don't think we miss out on CFs because of our framework, except when not reported in the reviews (i.e., macro and intervention level CFs).
However, this review has also some limitations. Our review of reviews was dependent on the reporting, synthesis and quality of the previously conducted reviews; however, we included a large number of reviews across four diseases to overcome this shortcoming. In addition, we used current and robust methodological guidelines for our review.15–18 Another limitation is that most of the included reviews reported on patients or/and HCPs and not on macro-level CFs. This could be the result of our search strategy since we focused mainly on interventions targeting patients or/and HCPs. Thirdly, it was sometimes difficult to synthesize our data since several reviews reported on specific sub-populations in specific countries and it was not always clear if the CF was of importance in general or just for that population in that country. However, we have made several notes in our analysis to indicate this, for example: ‘In a population of Congolese and Zimbabwean migrant women living in South Africa, it was found that being away from home prevented them from making their traditional foods, which consisted of mostly plant-based meals, prompting them to compensate with fast foods’. 75 Finally, we focused on SMIs in general and did not search for specific SMIs (like ‘monitoring techniques’ or ‘motivational interviewing’). The focus on specific SMIs could have resulted in CFs more targeted to specific implementation aspects.
Implications for future research or clinical practice
This study is part of a larger project, called COMPAR-EU. 6 A next step of this project will be to identify the most important CFs according to various stakeholders through a group consensus process (i.e., Delphi study). Identifying disease-specific CFs will be part of this consensus process. Since the macro-level CFs were underrepresented in our review, we will pay specific attention to identifying (additional) higher level CFs by inviting managers and policy makers. The CFs will be part of the COMPAR-EU online platform (www.self-management.eu). This platform will provide support for policymakers, guideline developers, HCPs and patients to make informed decisions on the adoption of the most suitable SMIs and on which CFs to take into account given their own situation and resources. 6
Supplemental Material
sj-docx-1-chi-10.1177_17423953231153337 - Supplemental material for Contextual factors for the successful implementation of self-management interventions for chronic diseases: A qualitative review of reviews
Supplemental material, sj-docx-1-chi-10.1177_17423953231153337 for Contextual factors for the successful implementation of self-management interventions for chronic diseases: A qualitative review of reviews by Janneke Noordman, Maaike Meurs, Rune Poortvliet, Tamara Rusman, Carola Orrego-Villagran, Marta Ballester, Lyudmil Ninov, Ena Niño de Guzmán, Pablo Alonso-Coello, Oliver Groene, Rosa Suñol, Monique Heijmans and Cordula Wagner in Chronic Illness
Footnotes
Acknowledgements
The authors would like to thank all partners of the COMPAR-EU group.
Availability of data
The data are available on reasonable request by contacting the authors.
Contributorship
JN contributed to the design of the study and wrote the first draft of the manuscript. MM, RP, TR, CO-V, MB, LN, EN, PA-C, OG, RS, MH and CW contributed to the design of the study, reviewed the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The project coordinator (Avedis Donabedian Research Institute) requested the overall ethical approval for the project to our local Clinical Research Ethics Committee (CEIC) (the University Institute for Primary Care Research—IDIAP Jordi Gol). Ethical approval was granted in March 2018.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the European Union’s Horizon 2020 (grant number No 754936).
Guarantor
Nivel
Registration and protocol
The review was not registered. The research protocol is published previously: Ballester M, Orrego C, Heijmans M, et al. Comparing the effectiveness and cost-effectiveness of self-management interventions in four high-priority chronic conditions in Europe (COMPAR-EU): a research protocol. BMJ Open 2020; 10: e034680. 2020/01/22. DOI: 10.1136/bmjopen-2019-034680.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.