
Abstract
Objective
Illness disclosure refers to when individuals with chronic illnesses make decisions to tell others about their disease. There is a lack of research on the complexity of disclosure among children and youth with chronic illnesses. We conducted a review of the literature to understand the process of disclosure among children and youth with chronic illnesses in the context of peer-based relationships.
Methods
A narrative review was completed using three databases. The search yielded 11 articles that utilized various research designs.
Results
Most of the literature was qualitative in nature. Most children and youth engaged in non-disclosure and concealment which is born out of fears of discrimination. Fewer children and youth engaged in unplanned disclosure, passive disclosure, partial disclosure, and open disclosure. Children and youth carefully consider who they are disclosing to and perceptions about other peoples’ responses strongly impact disclosure. Children and youth disclose verbally, behaviorally, and in written form. Disclosure is associated with both positive and negative effects, such as confidence, self-advocacy, and distress.
Discussion
Health providers and researchers should critically support disclosure and empower children and youth with the resources they need to be agents in their own disclosure decisions.
Introduction
In moral philosophy, the values of honesty and transparency are valued in many cultures. 1 With regards to disclosure and childhood chronic illness in North American and European countries, most of the literature has focused on when parents or physicians should disclose the condition to the child. Before 1948, chronically ill children were not given any information about their ailments due to a discourse of protectionism and the notion that any illness information could harm them. 2 With the growing child rights movement of the 1980s and the recognition that non-disclosure may be harmful to children, the disclosure discourse began to change. Best practice today recommends telling children about their illness in developmentally appropriate ways. 2
Unfortunately, the disclosure literature offers little guidance on the nature and process of chronically ill children and youth’s disclosure to peers. Thus, the disclosure literature is adultist, maintaining a primary focus on parents’ decisions. In this narrative review, we address these glaring lacunae in the disclosure literature by exploring how children and youth with chronic illnesses disclose their conditions to peers. The purpose of this narrative review is to investigate how children and youth with a chronic illness make decisions to disclose their diagnosis to their peers. Here, peers are understood to be individuals of similar age and/or developmental stages who share common spaces. 3
Childhood chronic illnesses can be considered as any illness that is incurable or lasts a duration of three months or longer, involves greater health services that extend beyond routine care, and limits functioning. 4 Despite increased survival, the rarity of childhood illness, and reduced mortality over time, these children may experience great hardship and psychosocial morbidity. 5 For instance, children and youth with chronic illnesses report experiencing social isolation, bullying, and reduced self-efficacy.5–7 These impacts are crucial to investigate since school-age children and adolescents are at a time in their lives when they begin to seek social acceptance and opportunities from systems outside of their family. 8 However, not all outcomes are adverse and positive outcomes such as resiliency and growth have also been observed. 9 Both positive and negative outcomes can have short-term and long-term impacts on children’s psychosocial well-being.
One process that heavily impacts the psychosocial wellbeing of children and youth with chronic illnesses is self-disclosure. Self-disclosure is a complex, dynamic, and continuous process in which individuals carefully select who, what, and how they tell others about their illness. 10 Factors such as time, setting, anticipated reactions, previous experiences, and the strength of friendship all play influential roles in whether and how children disclose their illness.11–13 Some of the reasons why youth choose to disclose their illness are associated with wanting understanding, acceptance, and support from those who have similar experiences. 11 On the other hand, the decision to withhold illness information includes fear of rejection and stigmatization.6,11–13 The literature illustrates a favor towards self-disclosure because it can result in psychosocial benefits which consist of sharing new identities, strengthening relationships, and maintaining self-esteem.11–13 Despite the importance of the existing literature, there is a lack of evidence on how children and youth with chronic illnesses engage in this complex process. Indeed, studying disclosure among children and youth is of critical importance given that disclosure is known to impact important interpersonal and intrapersonal processes, such as perceptions of acceptance, and stigmatization.4,14 The purpose of this narrative review is to understand how children and youth with chronic illnesses disclose their illness in the context of peer-based relationships.
Methods
Rationale for a narrative review
It is important to conduct a narrative review of literature given the propensity of narrative reviews to capture rich, story-like information on the intricacies and nuances of peer-based relationships.15,16 Indeed, the potential for rich narrative and storying of the literature may be lost by reliance on more formal review types, such as scoping reviews or systemic reviews. The narrative-review type has the potential to capture the subtleties, nuances, and complexity of disclosures in the context of peer-based relationships. Additionally, this review type is incredibly useful when trying to synthesize diverse disciplines and methodological traditions. 16
Search strategy
The search strategy was developed and guided by workshops, research team discussions, meetings with a librarian, and reading other narrative reviews. These practices resulted in the use of three databases which included MEDLINE, PsycINFO, and EMBASE. These databases were found on Toronto Metropolitan University’s Library and Archives webpage and were chosen to encompass the clinical and psychological viewpoints of the research purpose. Initially, we aimed to investigate the disclosure practices that occur among children with cancer. Due to the extremely limited results, we had to re-evaluate our research purpose and expand our search to include all chronic illnesses and the youth population. A set of keywords were used for our search including, disclosure, chronic illness, child, adolescent, youth, peer, and friend. The keywords were chosen to gather articles that capture most if not all aspects of the research purpose. Cancer was also a keyword. Although we revised our original purpose, we still wanted to search for cancer-specific articles, as they are of particular interest. The keywords were combined with the conjunctions ‘and’ or ‘or’. The database code of truncation (*) was also used to gather relevant articles in a single search. For example, one of our searches was disclos* AND (chronic illness* or chronic disease* or chronic condition*) AND (peer* or friend*). Additionally, filters were applied to narrow the search criteria. These filters consisted of articles written in English and specified age categories. These categories slightly differed in each database. Generally, we used the age category filters of child, adolescent, and young adult, which resulted in an age search range of 0–29.
Screening process
The screening process was completed by the first author. The author documented the searches that were used and articles of interest. These documents were shared in regular meetings with the second author where we discussed major decisions and any questions we had regarding the process of developing and writing this review. The inclusion criteria was developed prior to conducting the search and readjusted along the way. This criteria consisted of articles that: (1) were peer-reviewed and full-text; (2) written in the English language (3) were published after 2000; (4) had participants with chronic illness; (5) had participants under the age of 25; and (6) were focused on disclosure among peers. Given that childhood chronic illnesses are rare and recruitment into studies is extremely challenging, the application of age-specified filters, and our desire to stay close to the child population, we wanted to maintain an inclusive definition of children and youth, up until the age of 25 years. 17 The existing literature consists of many articles that provide recommendations on when and how parents should provide children with developmentally appropriate information about their chronic illness. 18 Children as young as three years old may be able to understand their illness although they may regard death as reversible. However, we found a lack of empirical guidance on when children are able to disclose their condition to peers. Indeed, the lack of developmentally appropriate disclosure guidance for young children may speak to the underdeveloped disclosure literature.
We operationalized the concept of disclosure as a process in which individuals carefully navigate who, what, where and how they tell others about their illness. This study was inclusive of various research approaches including, qualitative, quantitative, mixed-methods and reviews of literature. All other publications that did not fit this criterion were excluded. We undertook a thematic analysis of the final pool of selected articles following the steps outlined in previous scholarship.16,19 First, the main findings from each study in the 11 articles were extracted into a table. These findings were coded using a numeric indicator. Then, common numeric indicators were grouped together into larger themes that were common across all of the studies. After the seven themes were generated, we ensured that each theme was conceptually distinct from other themes so that data in that category represented a novel or unique theme. We verified the themes based on developing consensus with the research team.
Selecting articles
A total of 1552 articles were found regarding disclosure practices among peers (Figure 1). This number decreased to 1213 after removing duplicate articles using the Mendeley reference manager software. To determine whether the remaining articles were relevant to the study, both the title and the abstracts were read. Those that were not related to the research purpose were removed. All, but 50 articles were excluded from the search. For the remaining articles, the full article was read to determine whether the articles met the inclusion criteria and provided sufficient information relating to our research purpose.
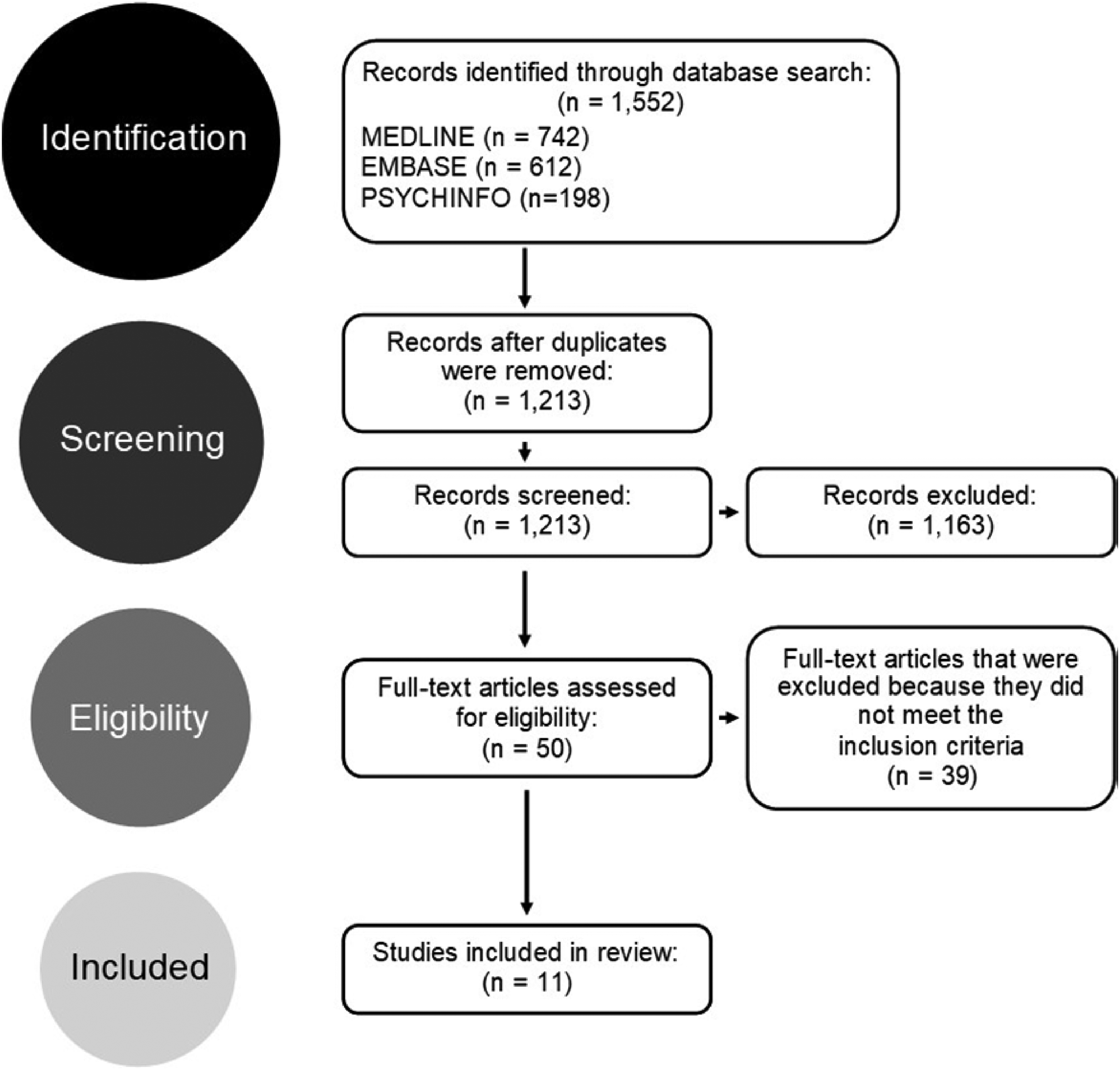
PRISMA flow diagram describing the selection procedure for this narrative review.
Results
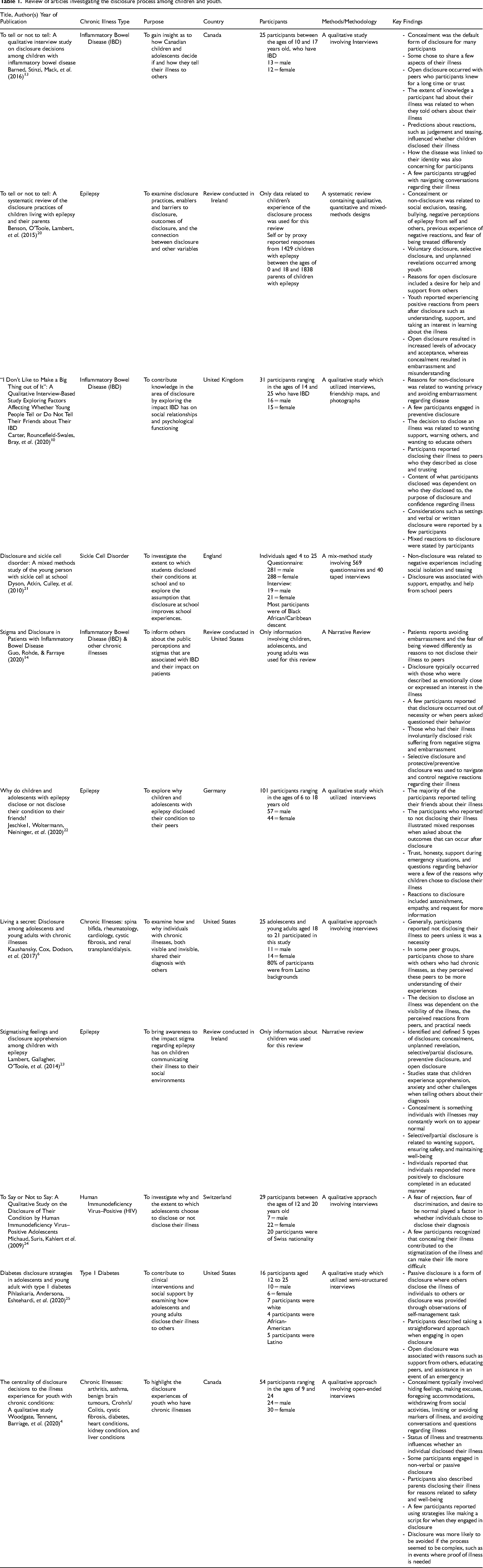
A total of 11 articles were identified to be eligible for this study (Table 1). These articles ranged from the year 2009 to 2020. The articles all aimed to identify how and why children, adolescents, and young adults disclosed their chronic illness to peers.
Review of articles investigating the disclosure process among children and youth.
Study design
Various research designs and methods were used to investigate disclosure among children, adolescents, and young adults. Qualitative studies were the most popular method (n = 7). These methods include semi-structured and structured interviews. Mapping of peer relationships, photographs, and a focus group were also used. Three out of the eleven articles (n = 3) found were reviews of literature. One article (n = 1) used a mixed-method approach to collect data.
Demographics
The inclusion criteria stated that articles must have participants under the age of 25 who have a chronic illness. A few exceptions were made. For example, although two literature reviews stated that they are examining children, adolescents and/or young adults, the age ranges were not specified. Due to the limited literature, the way these articles identified the audience in the studies that were discussed, and the richness of information that reviews can provide, we decided to include these articles. Most studies, excluding those that conducted reviews of literature, had samples that included roughly equal numbers of female and male participants. However, only four articles mentioned the ethnic backgrounds of their participants. In these studies, most participants were from African American and Latino backgrounds.
Multiple chronic illnesses
Various chronic illnesses were identified and investigated in the literature. The most common were inflammatory bowel disease (n = 3) and epilepsy (n = 3). Three studies focused on sickle cell disorder (n = 1), human immunodeficiency virus (HIV) (n = 1), and diabetes (n = 1). Two articles investigated chronic illnesses generally (n = 2). The illnesses investigated in these articles included arthritis, asthma, benign brain tumors, Crohn’s/colitis, cystic fibrosis, heart conditions, kidney conditions, liver conditions spina bifida, a rheumatologic disorder, and a condition requiring renal dialysis or transplant.
Main themes and findings
We found that disclosure is a complex process that encompasses many factors such as the reaction of others. Many claimed this process was one of the most challenging tasks they faced. 1 Seven themes about disclosure among peers emerged. These themes consist of: types of disclosure, who, how, what, when, reactions to disclosure, and potential outcomes (Figure 2). It should be noted that a few of these categories may overlap or be very similar to one another. The reason why there is some overlap is due to the incredibly nuanced and complex nature of illness disclosure, with factors such as time, setting, and relationships all impacting disclosure. However, it should be noted that each of the seven themes are conceptually distinct from every other theme and these differences will be discussed.
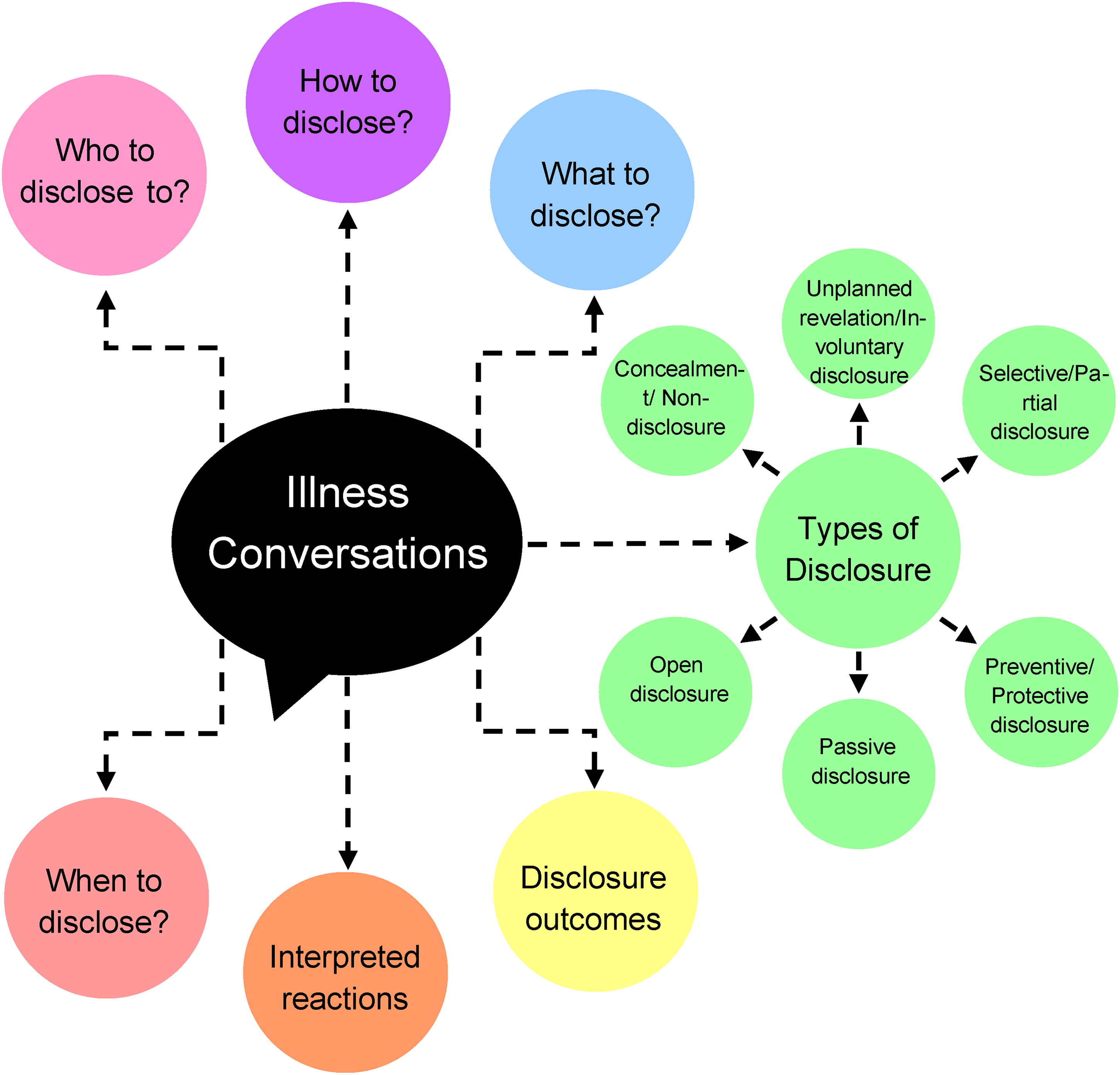
Concept chart illustrating the main themes that emerged from the review of literature.
Non-verbal disclosure occurs when peers notice a change in behavior within the individual with the chronic illness or when the individual engages in illness self-management tasks, such as taking pills.4,25 One research team reported that this method of disclosure can be problematic as it can lead to a lack of discussion and control regarding the information that is gained by their peers. 4 Passive disclosure differs from unplanned and involuntary disclosure because in involuntary disclosure, there is sometimes a “forced” reveal, such as parents disclosing without a child’s consent. In passive disclosure, the child is involved in the disclosure process and there is a purpose to the disclosure.
Similarly,
Discussion and analysis
In our study, concealment and non-disclosure was the most common disclosure practice among children and youth with chronic illnesses even in the presence of a robust social support network of friends.6,13,22 This builds on existing literature because concealment was found to occur in many ways as has been reported in other studies, such as hiding identifiers of illness and withholding illness information.4,23 Children with chronic illnesses may choose to conceal their illnesses to avoid bullying. 26 Further, in late childhood and adolescence, the most pressing developmental concern is acceptance by a peer group. 8 If youth feel that disclosure will threaten acceptance in a peer group, they may also resist disclosure. The disclosure process was also perceived as an exhausting task.4,10,25 Researchers and clinicians should try to understand how fatigue, perceptions of difference, and peer acceptance threaten disclosure and be sensitive to these disclosure burdens. Efforts to reduce disclosure burdens should also be made. Disclosure interventions with youth may also help to promote more insight into the complexity of these decisions.
Forced, involuntary, and unplanned disclosure was also reported in our study. This is a novel finding as it categorizes disclosure practices discussed in the literature that held common factors of forced or involuntary actions. Sometimes, unplanned, forced, or involuntarily disclosure occurs when a third party, like a parent, discloses on behalf of their child without the child’s consent.20,23 In addition to promoting discourses of childism that devalue children’s competence to make decisions, forced disclosure might undermine youth’s agency and lead to embarrassment.27,28 Researchers and clinicians may consider making themselves aware that stigma and embarrassment stem from forced and involuntary disclosures. Unless it is absolutely necessary to ensure the child’s safety, efforts should be made to avoid forced and unplanned disclosures unless done in consultation with youth.
On the other hand, passive disclosure encompasses similar disclosure actions as involuntary disclosure. However, this form of disclosure is distinguished by its voluntary purpose. 4 For example, for very young children, passive disclosure may occur via body language or knowledge that was shared a long time ago by parents before the child is able to remember. 25 Further, in the absence of formal disclosure, peers or others may infer a non-verbal disclosure through observing a child with a chronic illness consuming pills, for example. Even though passive disclosure was not a common strategy, it is still very important for clinicians, parents, and academics to be aware of it. Given the lack of open discussion about the child’s illness and the potential for miscommunication, this kind of disclosure may be very problematic. Clinicians and researchers may consider developing resources for youth with chronic illnesses to have a more empowered role in the disclosing process. More critically, it is imperative that important stakeholders be aware of the importance, meaning, and power of non-verbal communication and body language. 29 For non-verbal children with chronic illnesses, body language might be a very important communicative act.
Preventive and protective disclosure occurred in 6 articles, whereas selective disclosure was discussed in 4 articles. This builds on the existing literature because previous evidence found that these forms of disclosure occur when individuals carefully manage the information they give others.4,10,13,14,20,23 For example, protective and preventive disclosures can occur in classrooms to help peers know what to do in an emergency. 14 On the other hand, selective disclosure may occur to gain support and combat stigmatization and rejection. More critically, one of the benefits of these types of disclosures is that it provides the ill child with a degree of control over what and how much to disclose. Indeed, a sense of mastery and control is important in the context of chronic illness. 30 Health providers should make themselves aware that controlling the narrative may empower youth with a sense of agency. Educators should try to work with families to make these teachings and learnings as supportive as possible for youth.
Open disclosure was reported in 8 articles. This builds on the existing literature because previous studies show that open disclosure occurs with an ethos of transparency and honesty. 16 Open disclosure may also occur in an effort to express the “true” self or to gain access to academic accommodations.4,10,14,20–22,25 Those in educational settings trying to facilitate academic accommodations for young people with chronic illnesses should do so with respect, dignity, and confidentiality in an empathic way.
Our review found that the audience context for disclosure has a significant impact on whether these youth disclose. This builds on the existing literature because previous studies found that youth tend to disclose to long-term friends and family who they trust and who appear to have an interest in their condition.6,10,13,22 Given that many young people with chronic illnesses may lack access to friendship quantity and quality with characteristics such as friendship warmth, more efforts might be made toward ensuring that these youth actually have the peer resources available to them so they can safely disclose their illness. 31
Our review found that youth choose to disclose in person, in writing, or behaviorally, while also carefully considering the context and the timing of the disclosure.4,6,10 Additionally, depending on the purpose of disclosure, youth may disclose information about treatments and feelings regarding the illness. This builds on the existing literature because it provides insight as to what children and youth disclose and how they decide and prepare for disclosure. As the internet era continues to flourish and more blogs and websites are available to particular illness groups, this might potentially increase the likelihood of potential disclosures in written form online. 32 Indeed, in our anecdotal observations, young people with chronic illnesses are choosing to disclose on social media platforms like TikTok and Instagram. Future researchers might investigate whether written disclosures are perceived to be easier versus face to face disclosures.
Our review found that children and youth also appear to disclose several months into the process of developing intimate relationships with others. 10 Disclosure thus does not happen quickly. Youth are also more likely to disclose after they have accumulated knowledge about their own illness.6,13 In this regard, health providers and researchers might consider empowering youth with the educational resources they need to disclose. Health providers should also be aware that long-lasting friendships characterized by trust and reciprocity create the optimal conditions for disclosure.
Our review found that the likelihood of disclosure is strongly impacted by how youth imagine others to react.4,13 Previous investigations have not found this high degree of interpersonal engagement with the Other when making disclosure decisions. In this regard, our finding on the importance of interpersonal communication in the disclosure process for chronically ill children, is novel. Youth carefully consider the audience and their potential reaction before making disclosure decisions. Health providers should be cognizant of the masterful interpersonal communication skills that youth have when thinking about the disclosure process.
From our review, it is evident that disclosure has both positive and negative outcomes. This is a novel finding because this review provides an overview of outcomes for different types of disclosures.4,6,10,14,20,21 Health providers must consider both the positive and negative implications of disclosure before uniformly or uncritically encouraging patients to disclose. Indeed, despite the fact that honesty and transparency are heralded as virtues in many Euro-western cultures, disclosure does not always appear to be in the best interest of health. 1 If disclosure results in more harm to a child, it may not be the ethical course of action to take.
Our methodological evaluation is also a novel component of this review. Methodologically, it is evident that most of the studies on illness and disclosure are qualitative in nature or reviews of literature. This type of evidence is critical given the need to understand the complexity of disclosure and to build the evidence base. However, future researchers might also consider conducting more quantitative studies on illness disclosure to better grasp the conditions that give rise to disclosure or non-disclosure. The use of arts-based research may also be employed to better understand the emotional and affective components of disclosure.33,34
The reported age range in the literature of children and youth with chronic illnesses is extremely wide, ranging from 0 to 25. This might be because of recruitment challenges in studies on pediatric chronic illness. Despite this obstacle, identification of developmental and age differences could have provided more insight into the disclosure process among children and youth. With this being said, future researchers might also consider exploring illness disclosure among more narrow age ranges, such as 11 to 13 or 14 to 16 to identify these differences. Additionally, many studies stated the gender of their participants. However, only a few studies stated that gender did not make a significant difference in results. As with age, future studies should explore the role of gender on illness disclosure.
Recommendations for practice
Clinicians, academics, parents, educators, and other key stakeholders that work with chronically ill children should be aware that non-disclosure and concealment is a normative practice for these children and youth. Key stakeholders should avoid forced and involuntary disclosures and be aware that fear of difference and social exclusion is the main driver of non-disclosure. Critical stakeholders should reduce barriers to disclosure, encourage safe and inclusive spaces that are more likely to foster disclosure, consider disclosure interventions and supports, and ultimately support the autonomous disclosure agency of every child and youth.
Limitations
There were several limitations both in the existing literature and in our review. Although the narrative review of literature type is an excellent forum in which to engage in a rich, narrative-like storying of the data that is so necessary to document the complexity of disclosure, it does not engage in evaluating the evidence which is more characteristic of systematic reviews of literature. As well, there were limitations in the existing literature base in that disclosure literature is generally quite limited with the exception of children with cancer. The disclosure literature should expand in the future across many illness types. Furthermore, although there were international studies included in this review, we did not consider how cultural differences impacted the disclosure process.
Conclusion
Although there is some literature on self-disclosure, before this article, there was no peer-focused disclosure paper that captured the complexity and nuance of peer-based disclosure practices undertaken by children and youth with chronic illness. Indeed, narrative and storytelling about disclosure was made possible through the narrative review of literature type. We conducted a narrative review of literature on self-disclosure among children and youth with chronic illnesses using 3 academic databases. We found that concealment and non-disclosure was the most common form of disclosure and is born out of fear of judgment, ridicule, and bullying.6,13,22 However, involuntary disclosure, partial disclosure, and open disclosure were lesser practiced disclosure forms as well. The process of disclosure takes months and usually occurs in the context of close, intimate relationships.6,10,13,22 Youth heavily consider how they believe others will respond and thus disclosure is a highly interpersonal process. Disclosure is associated with both positive and negative health outcomes, such as acceptance and confidence, but also distress and stigmatization.6,10,14,20 Health providers and researchers should not uncritically support disclosure. Rather, they should aim to equip youth with the resources, skills, relationships, time, and abilities to make disclosure decisions that protect their agency, autonomy, and choices.
Footnotes
Contributorship
TP conducted the narrative review and wrote the 1st draft of the research report. FM contributed sections to the manuscript. RW, FM and TP reviewed and edited the manuscript. All authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Holland Bloorview Kids Rehabilitation Hospital Foundation. Additionally, Dr. Roberta Woodgate is supported by a Tier 1 Canadian Research Chair (CRC) in Child and Family Engagement in Health Research and Healthcare (CIHR - Canadian Research Chair- 950-231845).
Ethical approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Guarantor
TP