
Abstract
Introduction:
This study aimed to explore the needs of newly qualified sonographers with respect to the requirements of preceptorship. This paper describes the first stage of research, with data obtained from a cohort of experienced preceptors. A second stage of research with data from newly qualified sonographers is pending synthesis with this work. The aim is to produce an evidenced-based tool to support departments in developing and implementing effective and robust preceptorship.
Methods:
Twelve experienced participants from eight trusts, with a range of clinical backgrounds and experience were recruited. Two focus groups were held with questions structured around known themes highlighted in current evidence regarding newly qualified sonographers. The interviews were recorded and transcribed, and the qualitative data were analysed using thematic analysis.
Results:
Four main themes with subthemes emerged. These were: (1) the gaps between qualification and proficiency, (2) the need for managerial investment and formalisation, (3) the preceptor and (4) tools to support the transition and prevent burnout. Frequency data and quotes are given as exemplars.
Conclusion:
Participants report that newly qualified sonographers require support in report writing, clinical reasoning and confidence, and this should be addressed within preceptorship while acknowledging individual needs. Managerial investment is essential in ensuring adequate support and protected time is available for important preceptorship activities, such as meeting for feedback and feedforward with opportunity to clearly document progression. Inadequate support may be damaging for the wellbeing of preceptor and preceptee and ultimately impact the standard of our ultrasound services and patient care.
Introduction
Preceptorship can be defined as a period to guide and support newly qualified practitioners to make the transition from student to autonomous practitioner and to further develop their practice. 1 There is evidence that a structured and robust preceptorship programme is essential in developing confidence and competence in newly qualified healthcare professionals and minimising attrition.1,2 Furthermore, preceptorship programmes are not only key to developing competencies but also essential in providing a safe and supportive environment for those transitioning to reflect and progress on their journey from student to autonomous practitioner.1–3 There is an existing body of evidence that suggests that newly qualified sonographers are unsupported during this critical and vulnerable period of their career4,5 and that there is a pressing need for sonography preceptorships.
With chronic escalating disparity between ultrasound service demand and provision6,7 alongside evidence of sonographer ‘burn-out’ and worsening rates of attrition,6,8,9 it is not unreasonable to speculate that the absence of informed, quality preceptorships may be a contributory factor for such troubling phenomenon. Furthermore, in professions with established preceptorship programmes, such as that of the Nursing and Midwifery Council’s (NMC) principles of preceptorship,1,3 the literature suggests that formal preceptorships are effective in increasing the quality of patient care by improving skills and competencies, retaining newly qualified staff and increasing job satisfaction1,3 with the caveat of ensuring adequate support is available for both preceptors and preceptees. 3 In the context of sonography practice, the timely publication by the British Medical Ultrasound Society (BMUS): Preceptorship and Capability Development Framework for Sonographers 10 provides useful guidance and framework for sonography preceptorship.
The overall aim of this study is to substantiate evidence for implementing effective sonography preceptorship and offer an insightful, evidenced base to bridge the gap between theoretical and practical strategies. There are two distinct phases of research: first, exploring themes on preceptorship and the needs of newly qualified sonographers through the lens of experienced preceptors and second, through data obtained from newly qualified practitioners regarding their needs and expectations. This paper outlines the results from the first phase of research. The objectives are to engage managers, preceptors and preceptees with the preceptorship process to support newly qualified sonographers in their practice, safeguard wellbeing, improve patient care and combat the alarming rate of sonographer attrition.6,8
Methodology
Ethical approval was obtained before commencement of this project. A collaborative research strategy was utilised to co-develop an evidenced-based preceptorship tool for newly qualified sonographers via engagement with stakeholders, appraisers and alumni beyond the classroom. The methodology incorporates a literature review of the current body of evidence regarding preceptorship to integrate and synthesise with the research findings. The first phase explores the views of stakeholders and preceptors, and the results of this study are discussed on their own merit. The findings will later be synthesised with the second phase for future publication.
Two semi-structured focus groups were conducted virtually via Microsoft Teams™ and facilitated by the authors over a 2-day period. Participants were recruited from a potential pool of 80 appraisers and stakeholders within departments across the Southwest of England during a sonographer appraiser study day at our site, and participants who volunteered were purposively selected to represent preceptors from a range of professional backgrounds and locations in the Southwest of England. Purposive sampling of the volunteers, although recognised as being associated with bias, 11 allowed the authors to collect views from a diverse ultrasound workforce. The final representation encompassed 12 preceptors from eight different trusts, with experience ranging from 4 years to 20+ years. The sample included nine radiographers, one nurse, one clinical vascular scientist and one midwife sonographer. Participants held a range of clinical specialisms, including general medical ultrasound, obstetrics and gynaecology, musculoskeletal, head and neck, vascular, paediatric and interventional studies.
Each focus group comprised six participants and lasted approximately 120 minutes. The participants were asked a range of open-ended questions pertaining to themes previously recognised as pertinent to the preceptorship of newly qualified sonographers. These were: transition, role-development, and maintaining competencies and credibility. 5 The data collection during the focus groups was iterative in nature with emergent themes identified and discussed further. The data were organised, anonymised and analysed using NVivo 10™ software and a thematic analysis framework. Initially, codes were generated and common patterns within them were identified to generate themes and subthemes. Both transcripts were independently coded by a single author with all codes, subthemes and themes shared with the co-author for validation and scrutiny. Frequency distribution analysis was also carried out to explore whether keywords or phrases occurred more frequently than others, thus allowing for triangulation of the data and further contextualisation of the relevant findings. The results were shared with the participants prior to seeking publication to allow for any feedback of the findings and interpretation, with peer debriefing recognised as a criterion for credibility in qualitative research. 12
Results
The thematic analysis resulted in four main themes and twelve subthemes, shown in Figure 1. Relevant frequency data are shown in Figure 2.
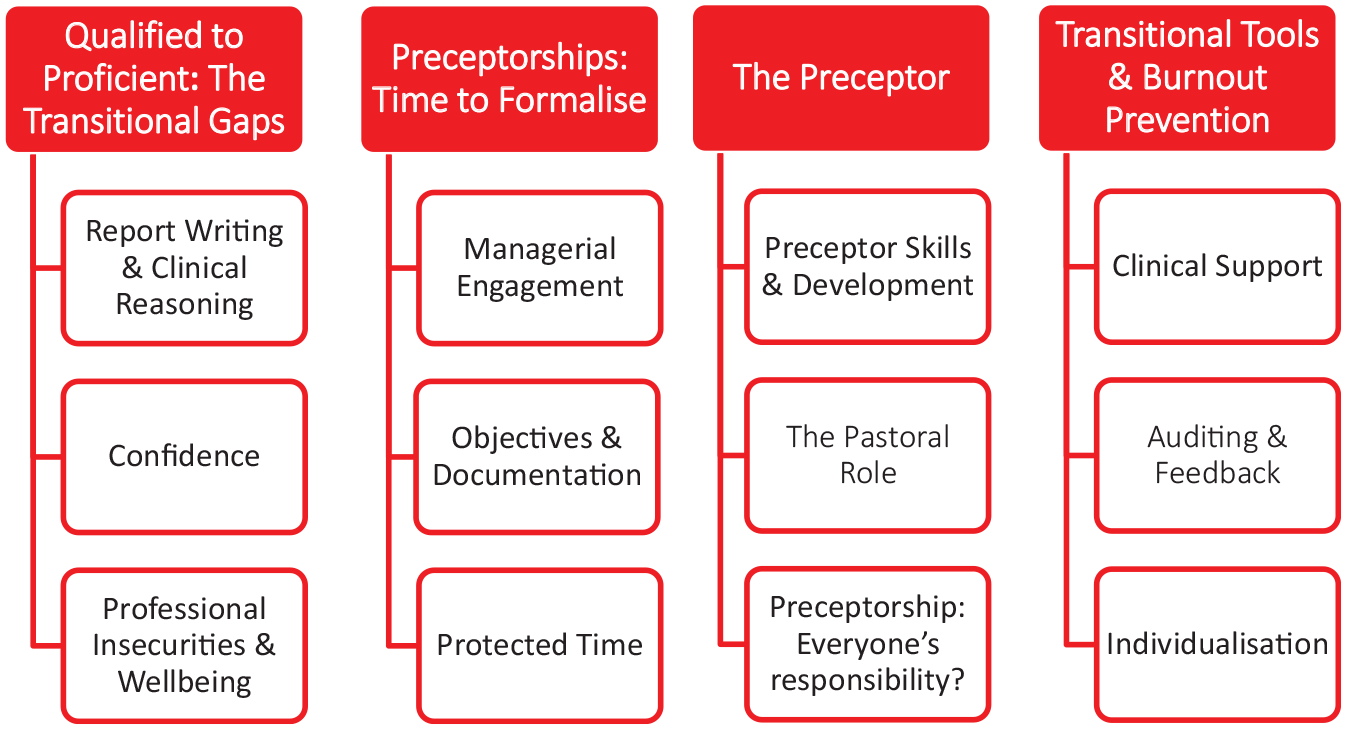
Four main themes and 12 subthemes.
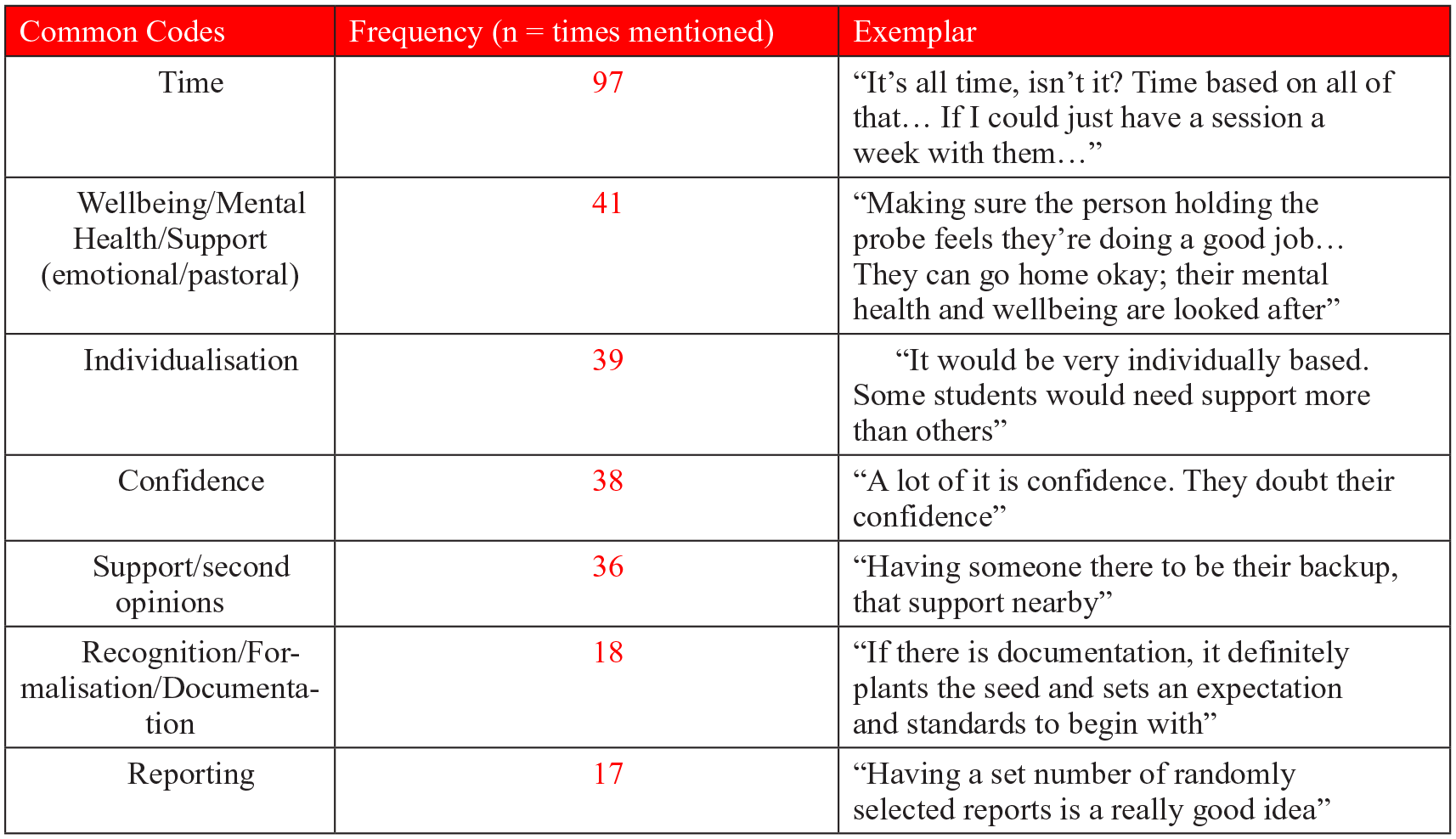
Frequency data of common codes, which informed the thematic analysis.
From qualified to proficient: the transitional gaps
Report writing and clinical reasoning
The first theme explores the difficulties encountered by newly qualified sonographers during the transition period as understood by the participants. Report writing and clinical reasoning was widely discussed by both groups: A very big one . . . is not knowing the significance of what they see. I find often that newly qualified staff want to report everything – S3. (Reporting) is a fundamental aspect of preceptorship. It’s very different, being asked to write reports under direct supervision to suddenly being asked to do them autonomously, that’s one of the big areas I found newly qualified sonographers have needed support with – S7.
Confidence
All participants agreed that confidence is an obstacle for preceptees, partly due to the culture shock of making decisions without the oversight of an experienced sonographer. This subtheme is arguably explanatory of the above ‘gaps’ in proficiency, with autonomous reporting and clinical decision-making secondary to one’s experience and confidence in their own ability: If they have an event early on in their list which knocks their confidence, they get into this confidence spiral where they then ask about everything, even if, ordinarily, they would have known – S1. One day you’re the student, the next day you’re qualified . . . It’s a fear factor as well . . . They doubt their confidence – S2.
Professional insecurities and wellbeing
Professional insecurities and wellbeing overlaps widely with the subtheme of confidence, which is attributable to the fear of making mistakes, missing pathology, or feeling like a burden when interrupting sonographers for support. It is perceived by the preceptors that newly qualified sonographers are at particular risk of feeling insecure in their practice and developing associated mental health issues, and poignant anecdotal discussion of a struggling preceptee emphasised this: She really did lose so much confidence and mentally she developed a lot of anxiety . . . It’s been about building that up and knowing when to ask for help, or not being afraid to ask for help – S9. The thing with mental health and newly qualified sonographers is there’s a real nervousness about making the wrong diagnosis, about missing something . . . It’s a demon that can really destroy your mental health and your career – S7. It’s very much a mental health space, the preceptorship year – S10.
Preceptorships: time to formalise
Managerial engagement
There was overwhelming support for a formalised preceptorship contract or memorandum of understanding to exist between management, preceptors and preceptees to enable a structured and protected programme. There is heterogeneity in practice among trusts, each devising their own approach with varying parameters, some with little or no managerial support. One preceptorship was devised by a student, with activities performed in the staffs’ own time, and in another department, difficulties arose in achieving trust-level approval due to a lack of recognition for sonography practice: We’re a small group of midwife sonographers and our manager isn’t a sonographer, so although they’re very supportive, they don’t get what we’re doing . . . We have a kind of a package, which one of the students designed in 2018 because there was nothing . . . So, a memorandum of understanding would be essential for us – S12. It was tricky, because the preceptorship department wouldn’t recognize it as a preceptorship because we were already registered staff . . . We weren’t being supported because theoretically these were already diagnostic radiographers or midwives – S1.
While some participants raised concerns around available funding for preceptorship periods, or how robust such contracts would be in the reality of pressurised departments, the potential advantages of accountability, enforceability, measurability and mitigating burn out and attrition are hugely desired: Having that scaffolding is really helpful in busy NHS environments because you’ve got documentation to take to your managers and say ‘we should be doing this every four-months and we haven’t done it for eight, QSI are coming . . . So, we should get our act together’ . . . Anything like that is helpful to evidence why it’s important – S1. For any formal preceptorship to work, you absolutely need buy in from the manager. It needs to be understood that it’s a two-way street . . . It’s not just beneficial for (the preceptee) but if that newly qualified sonographer burns out, the manager loses that member of their team – S7.
Objectives and documentation
In departments with established preceptorship programmes, a key factor was having objectives and timelines in which a graduated transition can be achieved. Those who described such approaches were met with approval and interest, and although there were variations in the described timelines, it was mostly felt that such objectives should have flex for individualisation – a repeated subtheme that is addressed in theme 4: The first month they are supernumerary and doubled up with an experienced sonographer, and then months two and three, they have independent lists with extended time slots . . . They then have four to six months of 20-minute slots with an extra slot at the end, as needed – S3. A year, to do 30-minute appointments, then after the year, go to 20-minute appointments and have an audit . . . But it’s an individual thing, you don’t want to destroy people’s confidence but if they achieve it earlier then they should be encouraged – S11. Transparent documentation processes are considered an essential aspect of formalising preceptorships for measurability, reflection, and in providing an evidence base: A competency style document would be helpful, like, what you would expect a post-year qualified sonographer to have achieved – S1. (Regular meetings) must be clearly documented. If there are any issues, you can see if there’s a pattern . . . If you have a personality clash, you must be careful that it doesn’t look like you’re discriminating . . . You can see that you’ve documented everything fairly and if needed, you’ve got an escalation plan – S6.
Protected time
Protected, non-clinical time was an exceptionally strong theme throughout both focus groups. A key component of formalisation is agreeing non-clinical time with management to allow preceptors and preceptees to meet, discuss progression and address issues, despite the short-term loss of scan capacity. Furthermore, a recognised programme should allow for alterations in practice, such as lengthened appointment times and inclusion of reporting breaks to support preceptees: They come to us at the end of the list, and it’s gone 5 pm, it would be better if we could have a session set aside, once a week, to do that – S9. It’s important for how valued the preceptor and preceptee feels in the activity they’re doing . . . It’s not just time, but properly protected time, that isn’t going to get kicked to turf every time somebody’s sick – S1. I don’t think it’s valued enough . . . I’m quite fortunate because I’m the lead, so I decide, but if you’re not the lead, you’re at the mercy of the managers and I don’t think people realize how important it is – S4.
The preceptor
Preceptor skills and development
While it is unanimously agreed that preceptors must be capable sonographers who advocate good practice, they should also be patient, possess good people skills and able to give constructive criticism. Furthermore, some speculate that the development and training of preceptors should not be overlooked: It would have to be someone experienced, but also with good people skills – S1. We once had an assessor who was critiquing something but they forgot to put any positives in. They got so engrossed in it . . . It’s got to be constructive – S5. It would be helpful to have access to how to give feedback . . . Presumably, education is evidence based the same way that healthcare is. So, there’s different models of how you feedback – S1.
Opinions were divided on who the preceptor should be, whether it is the same person who supported the individual during their training period, or someone new, however, there was agreement that personality and interpersonal relationships are important: either in personality clashes or friendships, the dynamic of which may make open criticism difficult. The preceptor must therefore be selected carefully and transparently: The whole point of the preceptorship is that you are transitioning from student to newly qualified sonographer, so I think continuity with the same person is helpful – S8. It should be different . . . We all look through different lenses and if I were teaching someone, I might not have seen something that someone else would – S7. Personality clashes . . . We need to be open and honest about it – S3.
The pastoral role
The preceptor is acknowledged as needing good pastoral ability to support newly qualified sonographers through the difficulties of the transitional period, a role that relates to the subtheme of wellbeing and highlights the need for preceptors to be aware of pressures beyond the workplace; to nurture, support and offer reassurance: It’s not all about work, is it? There can be things happening outside of work that affect you, too. It’s needing somebody to understand that and support that – S10. We all know that practically, when everybody’s very busy, feeling that you’re being an interruption and a pest, which they’re absolutely not, is something we need to be aware of as preceptors – S7. It’s also developing the best personal relationship you can with them . . . In a way, the student picks their preceptor, because they feel like they can talk to them – S9.
Preceptorship: everyone’s responsibility?
The final preceptor subtheme addresses the support preceptors require and the importance of wider teamwork for the benefit of all involved. The unique pressures of the preceptor role were explored, and departmental engagement is perceived to be a helpful support mechanism: You can’t do everything. It’s too much for one person to have a responsibility like that . . . To not have any sounding board or somebody to talk about things with – S8. We do something very similar here and meet with fellow (preceptors) and talk about the difficulties that perhaps some are facing . . . You can draw on other people’s knowledge and experience – S5. I had sleepless nights worrying about (a preceptee). You get to a point where you think ‘I can’t manage this in myself. How are we going to do this?’ So, you must reach out. And then you must have a team approach, very much – S9.
Transitional tools and burnout prevention
Clinical support
There are many clinical support mechanisms that can be included within preceptorship programmes to support newly qualified sonographers in their daily practice. Ensuring preceptees do not work off-site, are able to access second opinions when needed and have ample time within their scan lists is especially helpful: Having access to a qualified practitioner, so they have that support there. So, they’re not running a full list on their own. It’s well supported, with plenty of time – S2. A lot of that is centred around time management, feeling supported and whether the appointment times are appropriate – S11.
Auditing and feedback
Auditing scans and reports is a widely advocated preceptorship activity, included to varying degrees in the departments of all participants who follow a local framework. Dedicated reporting sessions offer valuable learning and development opportunities, with reporting, as addressed in the first theme, a specific hurdle for newly qualified sonographers. Feedback is extremely important and activities, such as auditing will be most effective if the preceptee has access to constructive outcomes and advice: We’ll audit their work at month one, three and six, to identify if there’s any gaps in their knowledge. There might be something that we’ve missed . . . Then we can address those needs by the time they have their six-month audit – S3. They’ve got to be safe; they’ve got to pass their audit. And I think, a certain number of cases before that time, they should be sitting down with somebody going through their reports – S11. Both groups were asked about encouragement of self-audit, and whilst this is not performed in departments, it was felt to be an excellent idea for promoting learning and development: That’s a brilliant idea . . . We used to do that with 1st trimester screening and the feedback I always got from sonographers was, ‘wow, that was so helpful’ . . . We need to do that more . . . They said when they were scanning the next session, in their minds they were going through the tick-sheet for the audit – S3.
Individualisation
While all participants recommend that preceptees are protected from the pressures of teaching and vetting, and some suggested that complex scans, such as inpatient work, should be introduced gradually, there was heterogeneity between the groups regarding preceptee involvement in extra-clinical activities. There was a consensus that recognition of individual ability and goals is therefore essential in preceptorships, as some will ‘fly the nest’ sooner and thrive in opportunities that could risk overwhelming others: It’s a really good idea to try and protect your newly qualified sonographers . . . They’re not allowed to teach at all until a year – S10. It must be individualized . . . We’ve had newly qualified students who welcomed being involved in departmental audits because it made them feel valued. It made them feel part of the team . . . They encouraged it and engaged in it. It does depend on the individual, doesn’t it? – S5.
Discussion
The four overarching themes of this study highlight: (1) the areas of proficiency requiring further support in newly qualified sonographers’ and the subsequent impact on wellbeing, (2) the pressing need for managerial engagement and formalisation, (3) the importance of the preceptor role, and (4) the preceptorship activities required to enable an effective process. The theme of ‘preceptorships: time to formalise’ illustrates the crucial need for managerial investment in implementing a successful preceptorship. There is strong emphasis on providing dedicated time, infrastructure, and documentation to ensure preceptorship is prioritised, and managers are in a good position to take ownership of this, having visibility of staffing capacity, workload, qualifications and experience within their department.
Offering protected time for preceptorship activities, such as feedback and audit, as highlighted in the fourth theme, would arguably allow preceptors to support preceptees in consolidating skills addressed in the first theme of reporting ability, clinical reasoning and confidence, all of which are vital components for safe and resilient ultrasound services 10 Practices, such as the described anecdotal evidence of preceptors using their own time to meet preceptees must be discouraged as this cannot afford the necessary time for meaningful preceptorship activity and arguably increases the risk of stress and burnout in preceptors and preceptees, with fatigue and longer working hours postulated as causes of sonographer burnout. 13
The recently published BMUS preceptorship and capability framework is a hugely welcome publication which, in view of the results of this research and the emphasis around the need for managerial support, is implored to be considered by ultrasound managers in the timely development of sonography preceptorships, the benefits of which are increased preceptee confidence and competence, professional development of the wider sonographic team, the preservation of team wellbeing and the delivery and resilience of safe, high-quality ultrasound services.2,10,13 Furthermore, our data are consistent with the wider allied health recommendations, with preceptorship guidance for psychological wellbeing practitioners 14 and NMC guidance 15 advising that preceptorships must have clear oversight with governance frameworks to monitor, evaluate and review.14,15 Therefore, there is emphasis on the importance of managerial investment and overarching responsibility of implementing preceptorships with rigour and due diligence.10,14,15
Themes on dedicated time for preceptorship activities, confidence, individualisation and wellbeing were the most frequently occurring within the focus groups, which is perhaps not only representative of such themes being pertinent to the preceptors’ views of, and needs within preceptorship, but also suggestive that such essential themes are inextricably linked, with sonographer wellbeing and development of confidence during the transitional period being directly, negatively impacted by the lack of personalised and protected time for effective preceptorship activities. There was no notable difference in data obtained from different clinical backgrounds.
Individualisation is encompassed within themes of establishing personalised objectives, findings of which are consistent with the NMC’s principles of preceptorship, which state that activities should be agreed with the individual preceptee, and that preceptorship should vary in length and content according to the varying needs of each newly qualified practitioner.1,3 Additional consistent findings are the importance of interpersonal relationships, professional identity, the pastoral role of preceptors and the appreciation of mental wellbeing, with characteristics of being kind, fair, impartial, transparent, collaborative and prioritising individual mental and physical wellbeing all pertinent to the NMC preceptorship principles. 1 While themes around report writing and clinical reasoning are naturally unique to the sonography profession and therefore cannot be tangibly discussed in relation to nursing and midwifery outcomes, the results of the thematic analysis are congruent with the BMUS preceptorship framework with recommended activities of image review and audit, audit of report quality and the establishment of mutually agreed, prescriptive objectives and timeframes. 10
An arguable weakness of this study is that such themes are produced explicitly from the generalisations of preceptors only, however, the themes resonate with those identified within the available literature on the experiences of newly qualified sonographers and radiographers, who experience a ‘culture-shock’ when becoming solely responsible and autonomous in their role.5,16 Furthermore, work is underway to analyse and synthesise data obtained from the preceptee population during the second phase of research, alongside ongoing review of the most up-to-date literature, aiming to inform the development of a rigorous, evidenced-based tool to guide departments when considering their preceptorship model.
Strengths of the thematic analysis are the wide scope of inclusion criteria, which although was dominated by radiographic backgrounds was not limited to them, and the wide geographical scope of participation, with representatives present from several departments across the Southwest of England. Group discussion was encouraged to promote dialogical interaction and neither group encompassed more than eight participants to safeguard the quality of individual performance and interaction. 17
Conclusion
This research highlights the importance of formalising sonography preceptorships and the vital role that managers and preceptors play to ensure their success. The themes provide an insight into areas where newly qualified sonographers may need support in consolidating and enhancing their skills. Preceptorship programmes can be enriched for both the preceptee and the preceptor by encompassing activities, such as meetings, feedback and more importantly feedforward: by looking into the future, we can help nurture and develop skills in report writing and clinical reasoning, which will boost confidence and prepare preceptees for their continuing sonography career. A preceptorship programme should also be tailored to support the individual through mutually agreed and reviewed timelines and objectives.1,3,10
The potential benefits of a robust, formalised preceptorship include improved retention of staff, optimal patient care and a more confident and supported workforce. 16 To achieve this, we propose that preceptorships should also be implemented in a prioritised and measurable manner to ensure the process is effective and safeguards both preceptor and preceptee from risk of burnout and fatigue.2,6,10 Finally, by shining the light on preceptors, this research adds another dimension to the increasing empirical evidence reported in the literature on sonography preceptorships.
Footnotes
Acknowledgements
The authors thank NHS England (formerly HEE) for their financial support, and all participants for their involvement, engagement and enthusiasm.
Contributors
Rita Phillips.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by the NHS England (formerly Health Education England (HEE)).
Ethics approval
The University of the West of England (UWE) Faculty for Research Ethics Committee approved this study (REC: HAS.22.01.057). Guarantor: SA.
Permission from patient(s) or subject(s) obtained in writing for publishing their case report
Not Applicable.
Permission obtained in writing from patient or any person whose photo is included for publishing their photographs and images
Not Applicable.
Confirm that you are aware that permission from a previous publisher for reproducing any previously published material will be required should your article be accepted for publication and that you will be responsible for obtaining that permission
YES.
Guarantor
Siobhan Alsop.