
Abstract
Background:
Identification and resection of the thyroid pyramidal lobe is important for thyroid cancer surgery in order to prevent interval cancer in residual thyroid tissue.
Purpose:
The purpose of this study was to determine how often a thyroid pyramidal lobe is found in patients with and without previous thyroidectomy and to optimise the protocol for identifying thyroid pyramidal lobes during routine thyroid ultrasonography.
Material and Methods:
In this prospective study, a total of 1579 patients who received routine thyroid ultrasound scans at a single centre were enrolled. A dedicated standard scanning protocol was established containing both static images of the anterior neck superior to the thyroid as well as a transverse cine loop starting from the isthmus to the hyoid bone. The presence and features of thyroid pyramidal lobes were evaluated and compared.
Results:
Detection rate of thyroid pyramidal lobes in patients without thyroidectomy improved from 39.5% (480/1215) to 49.7% (640/1215) with protocol adding cine-loop as compared to protocol without cine-loop. The cine-loops were particularly helpful in the detection of thyroid pyramidal lobes when it is separated from the main lobe or in thyroidectomy patients. By adding assessment with cine-loop into the dedicated protocol, we have further detected different pathologies occurring on thyroid pyramidal lobes including benign and malignant solid nodules and pseudo-nodules of Hashimoto’s thyroiditis.
Conclusion:
The addition of dynamic assessment with cine-loop increases the detection rate of thyroid pyramidal lobes. By paying attention to the thyroid pyramidal lobe in pre-operative diagnostic sonographic images, we can help to avoid incomplete removal of the thyroid gland during thyroidectomy.
Introduction
The thyroid pyramidal lobe (TPL) is an embryological remnant of the thyroglossal duct and is considered a normal component of the thyroid gland. 1 It may occur in various positions with different widths and lengths. 2
At the time of thyroid cancer surgery, an attempt is made to locate and resect the TPL. In patients who have undergone a total thyroidectomy, the TPL should not be visualised during post-thyroidectomy follow-up imaging scans.3,4 However, if the TPL is discontinuous, its presence may be overlooked. 4 The residual TPL left post-operatively may influence the results of post-operative serum thyroglobulin measurements in papillary cancer patients. 5 Furthermore, residual thyroid tissue may alter the outcome of radioactive iodine ablation because the radioisotope will preferentially target normal remnant thyroid tissue over malignant thyroid cells. 5 Importantly, the remnant TPL may be involved in any pathology that occurs in the main thyroid gland including cancer, thyroiditis, nodules and so on.6,7
The reported prevalence of TPLs varies from 12% to 75% in cadaveric and post-surgical pathologic studies.1,2,8,9 Recent multi-centre studies focusing on the prevalence and features of TPLs using ultrasound (US) have demonstrated that this variant is present in 39.5% of patients. 10 The sensitivity and specificity of US to detect pre-operative TPLs has been shown to be up to 81% and 79.2%, respectively. 9 These findings suggest that thyroid sonography is useful into detecting TPLs.9,11
Identification and resection of the TPL is important for thyroid cancer surgery in order to prevent interval cancer in residual thyroid tissue and ensure reliable follow-up with serum thyroglobulin. However, to the best of our knowledge, no optimised US protocol for the detection of TPLs has been reported to date. The purpose of this study was to optimise the protocol to assess for TPLs during routine thyroid sonography.
Material and methods
Study design
This study was approved by the Research Ethics Board (REB) of our institute, and all participants gave informed written consent.
A prospective single-centre study was undertaken between June 2015 and May 2016. All patients who were scheduled for routine thyroid US scans were enrolled, including patients with previous partial and total thyroidectomy or previous neck surgeries. Both inpatients and outpatients were included in the study. There were no exclusion criteria.
Dedicated thyroid US protocol
The presence of a TPL on real-time US was defined as follows: accessory thyroid tissue with the same echogenicity as the main thyroid gland protruding from the upper margin of the isthmus, right or left thyroid lobe, regardless of continuity with the main thyroid gland.
A dedicated scanning protocol was established, and teaching sessions were given to all the sonographers in the US department. The scanning protocol includes both still images of the superior isthmus area (including visible TPL) and transverse cine-loop images starting from the isthmus to the hyoid bone. In the cases of post-thyroidectomy, the scanning protocol is still images of the superior thyroid bed and transverse cine-loop images starting from the surgical bed to the hyoid bone. Thyroid sonography was performed with a high-resolution US instrument (IU22; Philips Healthcare, Andover, MA, USA) equipped with a 17- or 12-MHz linear probe. By the end of scanning, preliminary tech note was provided by the sonographer. Two reviewers including a radiologist and a radiology resident retrospectively evaluated the presence and features of TPLs, such as the size, location and degree of continuity with the main thyroid gland by static images and cine-loop in the same patients retrieved from local imaging archiving and communication system (PACS) (Supplemental Figure S1). The reviews were performed independently, and discrepancies were discussed and consensus was reached between the two reviewers. The routine thyroid protocol is, however, described without cine as referenced in American College of Radiology (ACR) guidelines. 12
Statistical analysis
Continuous data including TPL length, width and isthmus width patient’s age were presented as mean ± standard deviation (SD), and categorical data including patient’s gender, types of TPL and history of surgery were presented as n (%). The comparative analysis of clinical variables and imaging findings utilised either the chi-square test for categorical variables or the Wilcoxon rank sum test (non-parametric version) for continuous data. For example, the Wilcoxon rank sum test was used for comparing variables (width and length of the TPL) between the TPL groups with or without cine-loop. The chi-square was used for comparing variables (location, separation or continuity of the TPL) between the TPL groups with or without cines. The chi-square was used for comparing different demographics between TPL present and absent groups.
All statistical significance was defined at p < 0.05. All statistical analyses were performed using the Statistical Analysis System (SAS) (version 9.4, SAS Inc., North Carolina State University, NC, USA).
Results
Demographics of patients included in the study
A total of 1579 patients who were scheduled for thyroid US between June 2015 and May 2016. A total of 1475 patients were included in the final analysis (104 patients were eliminated from the study due to poor quality of cine images). Among them, 17.1% (n = 252) of patients were male, and 82.9% (n = 1218) were female (Table 1). The TPL was present in 44.9% of the total population (Table 1). Interestingly, the TPL was more common in the female group as compared to the male group (46.4% vs 36.9%, p = 0.007) (Table 1). The mean age of the TPL group was 55.7 and group without TPL was 56.7. A total of 260 patients (14.7%) had undergone previous partial or total thyroidectomy. As expected, this group had much lower rate of detection (21.5% vs 49.7%, p < 0.001).
Demographics of patients included in the data set.
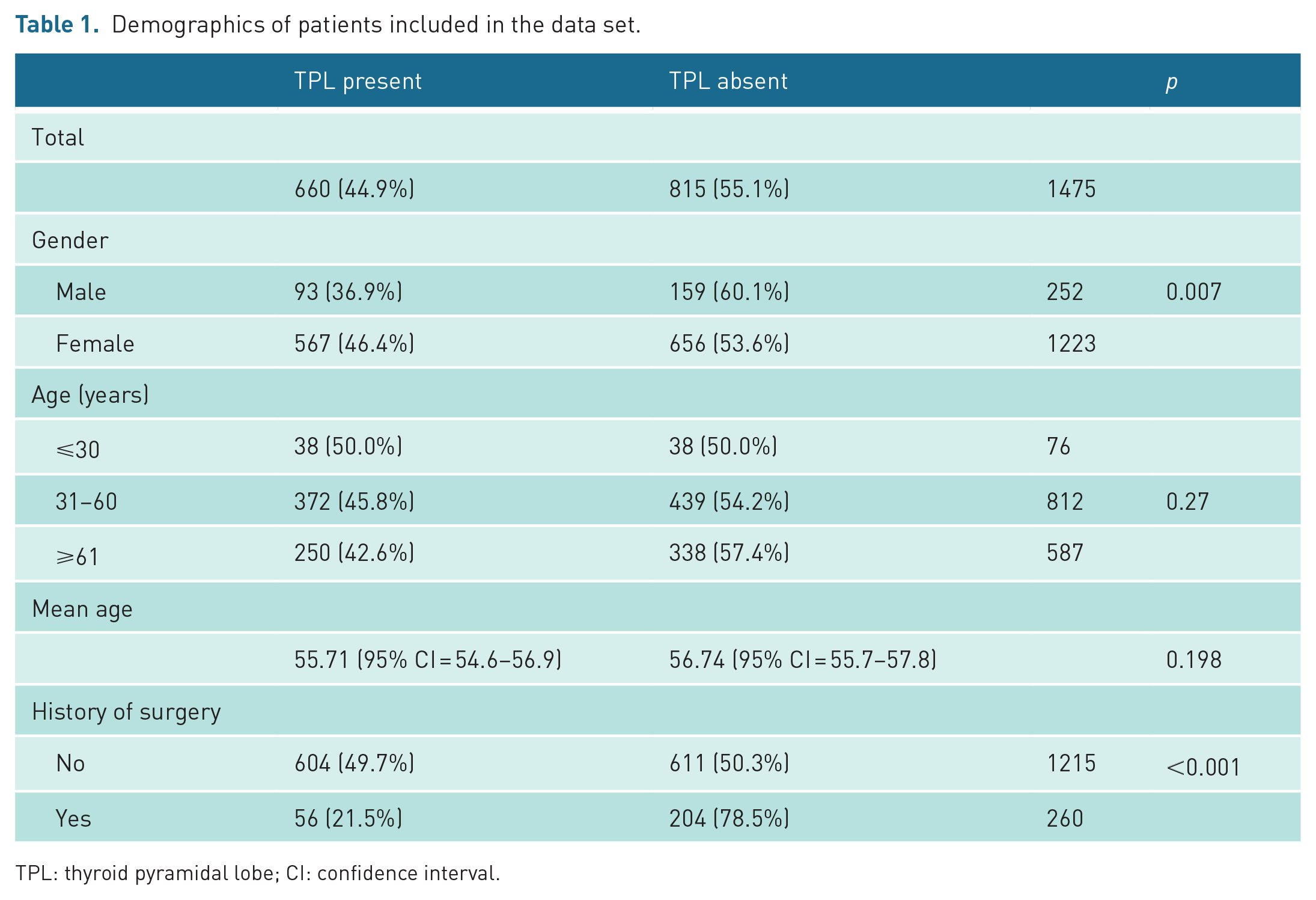
TPL: thyroid pyramidal lobe; CI: confidence interval.
The cine clips significantly improve the sensitivity of pyramidal lobe detection
Without cine-loop, the presence of TPLs was only detected and imaged by sonographers in 480 of 1215 patients without prior thyroidectomy (39.5%). However, detection rate of TPLs in patients without thyroidectomy improved to 49.7% (604/1215) by US practitioners after reviewing the cine-loop (Figure 1).
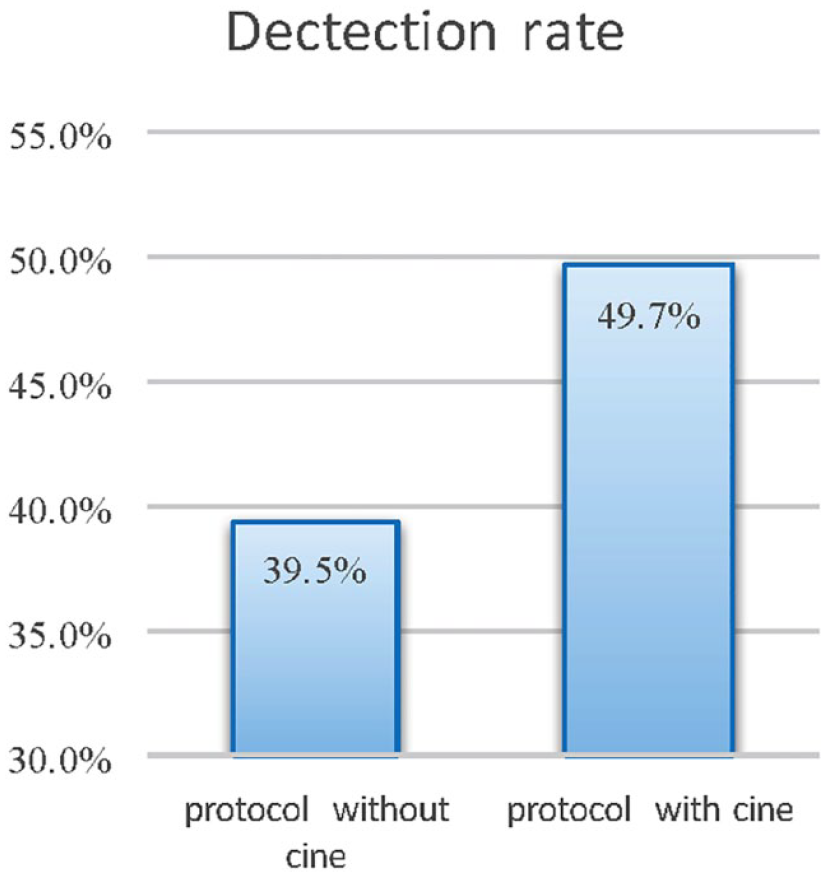
The detection rate of pyramid lobe is calculated with optimised scanning protocol with cine-loops versus standard thyroid protocol without cine-loops.
The sonographic features of TPL
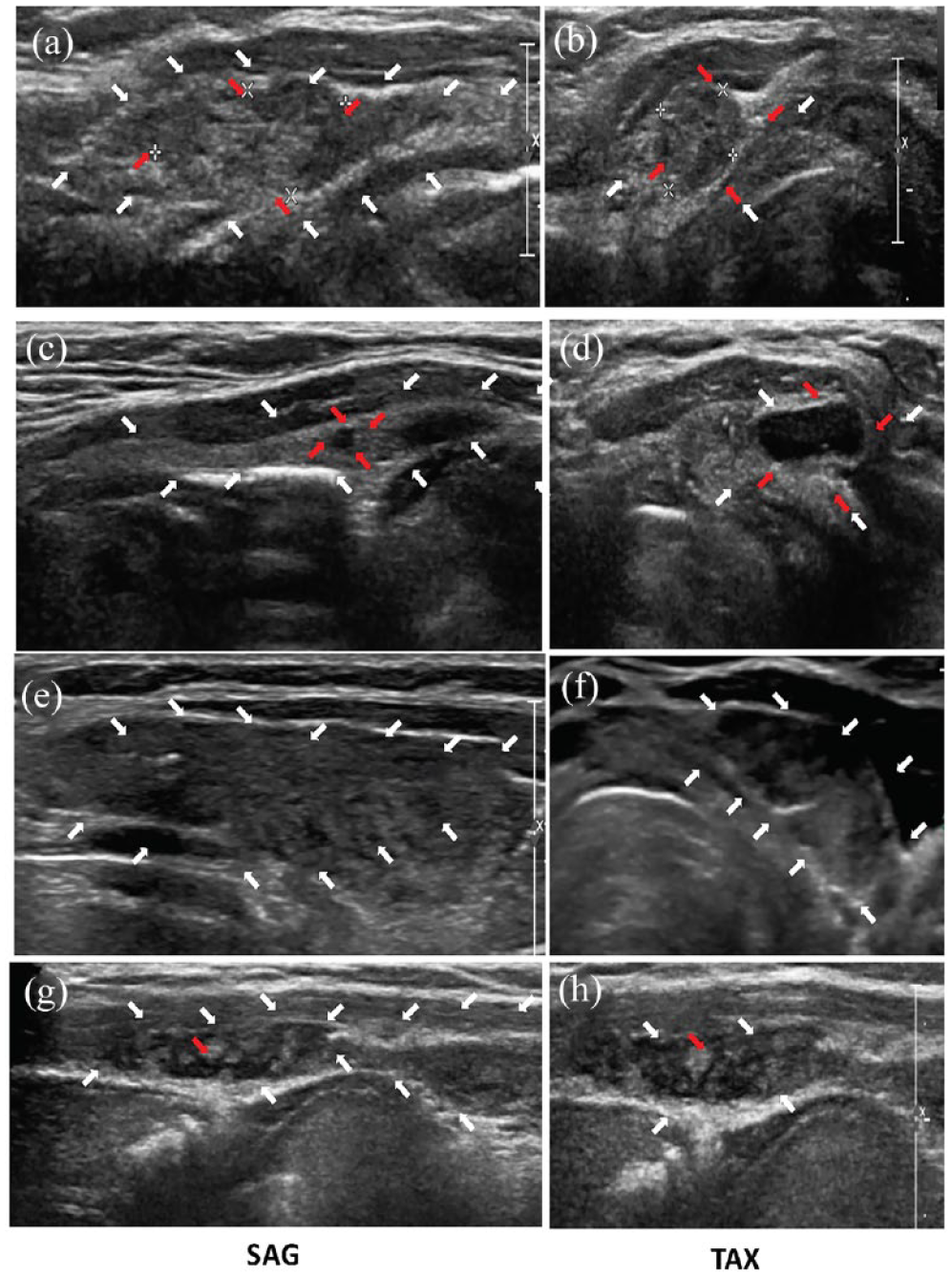
Transverse and sagittal two-dimensional (2D) sonographic images demonstrated different locations for TPLs. At assessment, 36.5% arose from the right side, while 49.4% arose from the left side. A further 8.2% arose from the midline (ML) (Figure 2). More interestingly, in 1.7% of patients, the pyramidal lobe arose from both lobes, and in 4.2% of patients, the pyramidal lobe could shift from one side to the other (Figure 2). Cine-loop imaging demonstrated that some of the pyramidal lobes were actually mobile under probe pressure (data not shown).
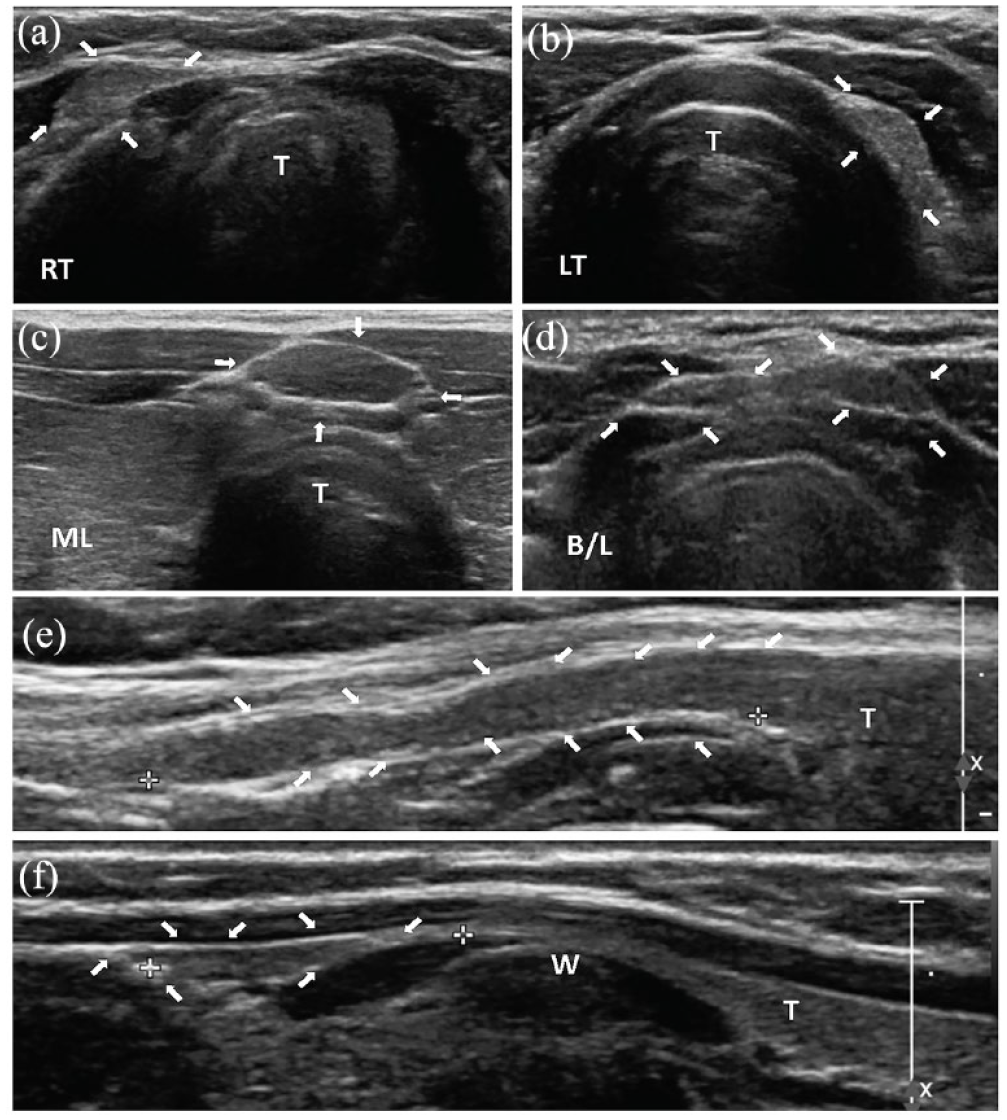
Cross-section (a–d) and sagittal (e and f) 2D sonographic images showing different locations of pyramidal lobe. (a) RT, (b) LT, (c) midline (ML) and (d) bilateral (B/L) lobes, (e) example of pyramidal lobe which is continuous from isthmus or either side thyroid lobe and (f) example of pyramidal lobe which is separated from main thyroid lobes. An extreme thin waist is often seen sonographically that occurs over the thyroid cartilage as indicated by W. T represents the thyroid gland.
With in situ glands, 85.3% of pyramidal lobes are continuous from the isthmus or either side of the thyroid lobe, while 14.7% of them were separate from the main thyroid gland. In the later situation, an extreme thin waist is often seen sonographically that occurs over the thyroid cartilage (Figure 2). A schematic diagram showing different locations of pyramidal lobes is illustrated in Figure 3.
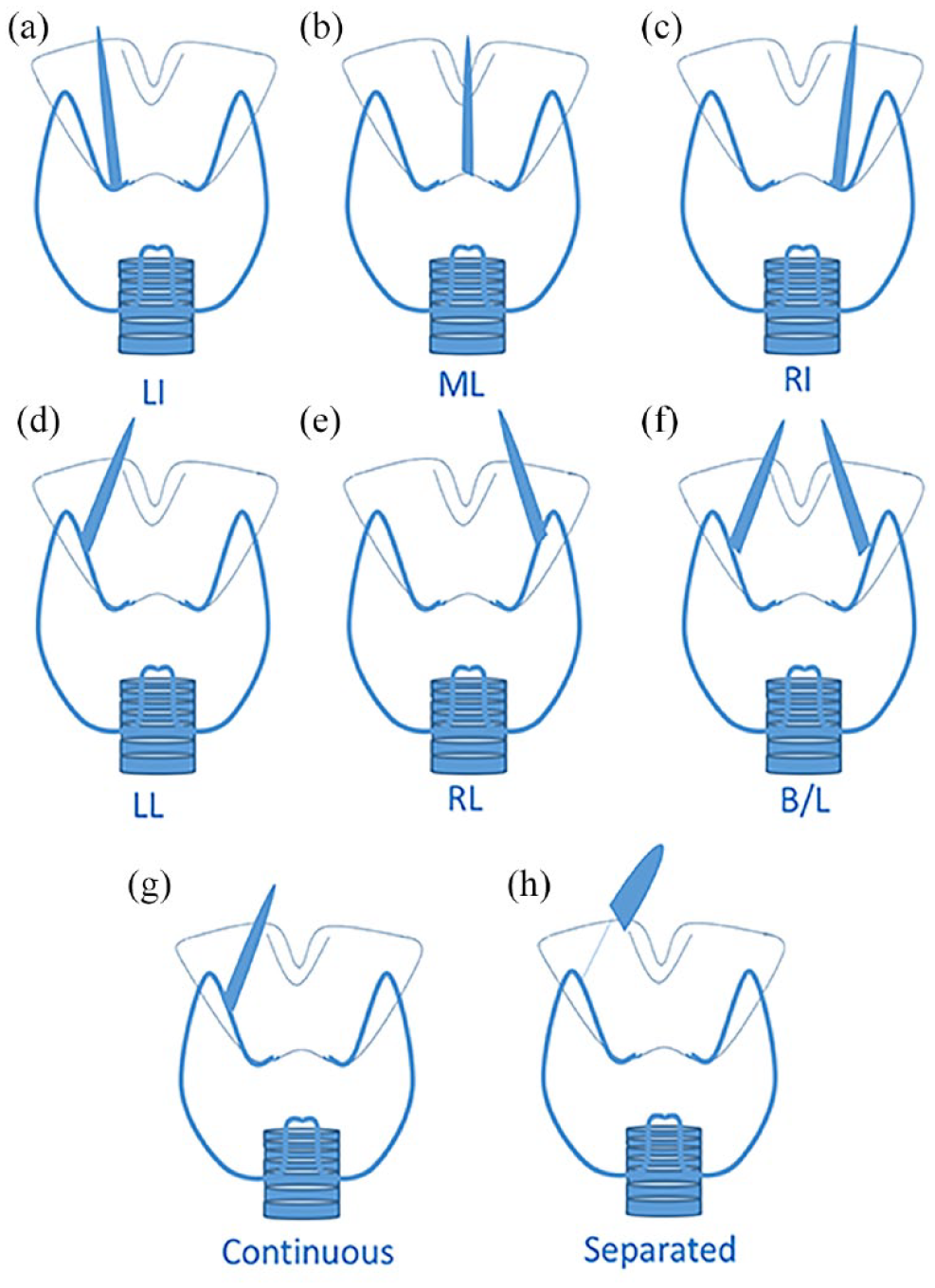
Schematic diagram showing different locations of pyramidal lobe, and its percentage of total population. (a) RT-isthmus, (b) LT-isthmus, (c) midline-isthmus (ML), (d) RT-lobe, (e) Lt-Lobe, (f) bilateral lobes and (g) and (h) continuous and separate from main thyroid lobe. In the later situation, an extreme thin waist is indicated that occurs over the thyroid cartilage.
Sonographic features of the TPL that may hinder detection
The cine-detected TPL group were more likely separated from the thyroid lobe (26.1% vs 11.4%, p < 0.001). The TPL was shorter in length (1.53 vs 2.02 cm, p < 0.001) and smaller in width (1.80 vs 2.27 mm, p < 0.001) in the group only detected by cine (Table 2 and Figure 4). Interestingly, the width of the isthmus is also smaller in the cine-detected TPL group (2.57 vs 3.09 mm, p = 0.004) (Figure 4(b)).
TPL feature comparison between the cases seen with cines or without cines.
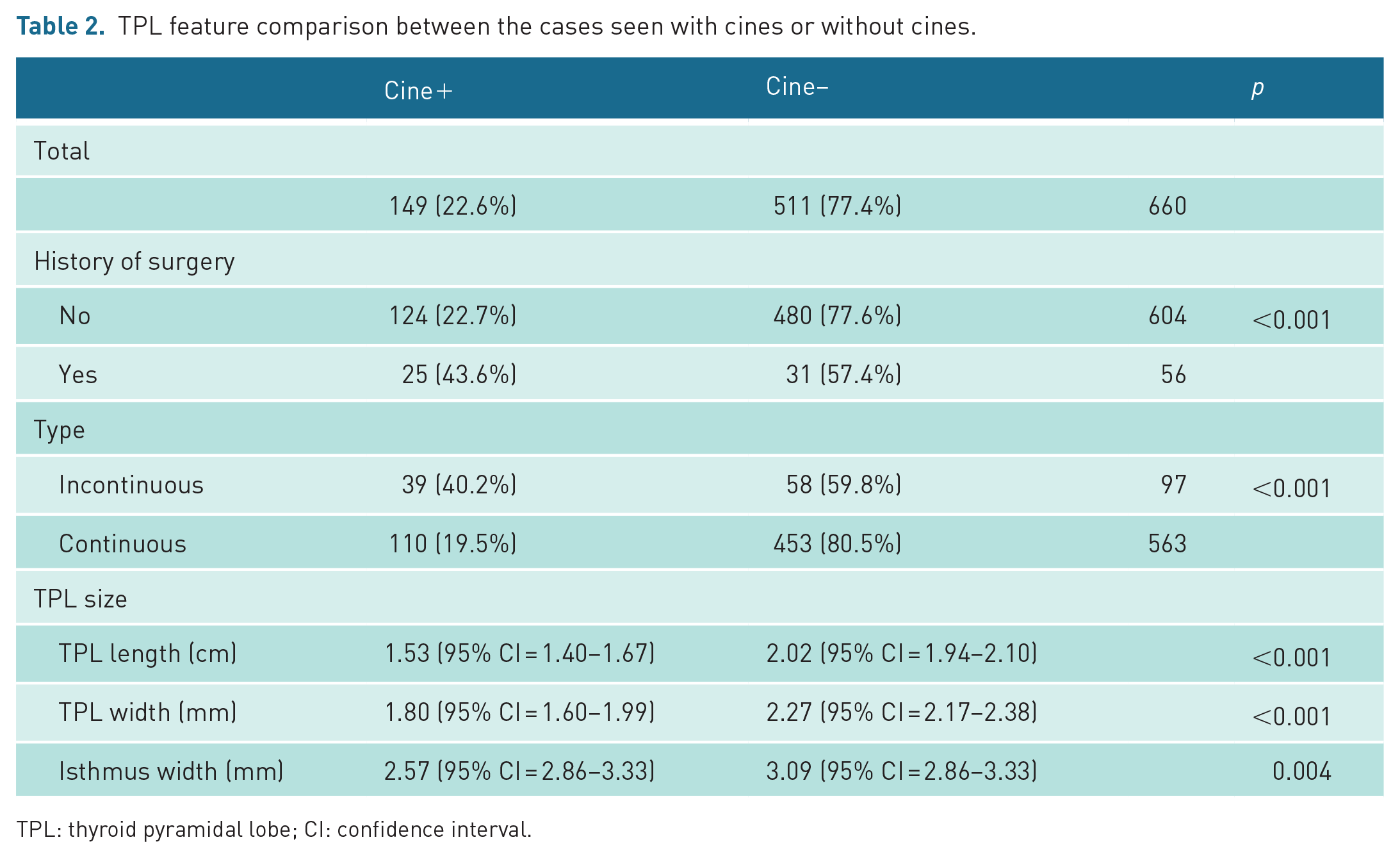
TPL: thyroid pyramidal lobe; CI: confidence interval.
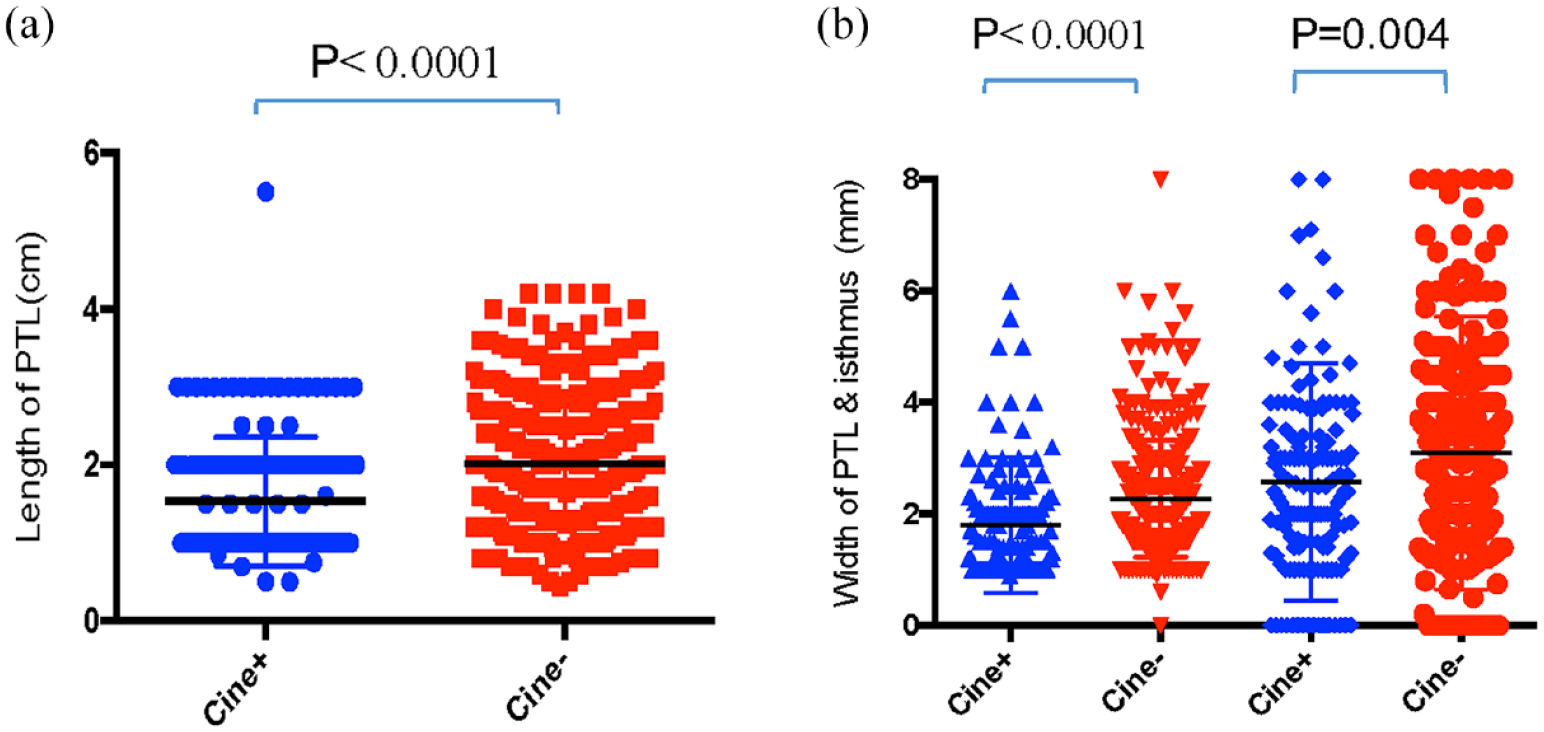
The sonographic features of thyroid pyramidal lobe identified solely by cine are compared to the ones identified by still images. The features include width and length of TPL and width of isthmus. Student’s t-test and the Wilcoxon rank sum test were used. The level of significance was defined as p < 0.05. The value of each feature was plotted as dots. Blue: only cine-detected TPL group. Red: still images detected TPL group.
US is a sensitive modality to detect various pathologies of TPLs
Using this dedicated scanning protocol, we have also detected the different pathologies that can occur in TPLs including benign and malignant solid nodules, pseudo-nodules of Hashimoto’s thyroiditis and thyroid cysts (Figure 5). Approximately 2% (10/660) of TPL cases were associated with abnormal sonographic findings present in our study cohort.
Different pathologies occurring on pyramidal lobe. (a) and (b) Goitre nodules as labelled by red arrows, (c) and (d) thyroid cyst (red arrows) on pyramidal lobe (white arrows), (e) and (f) Grave’s disease; heterogeneous hypoechoic-enlarged pyramidal lobe (white arrows) and (g) and (h) Hashimoto’s disease; echogenic pseudo-nodule (red arrows) on heterogeneous pyramidal lobe (white arrows).
Discussion
The routine thyroid protocol is described without cine-loop in the ACR guideline. 12 Our dedicated protocol with cine-loop has, however, improved the detection rate in patients without thyroidectomy from 39.5% (480/1215) to 49.7% (640/1215).
In pre-operative patients, a pyramidal lobe may be an entirely incidental finding; however, it can be affected by the same range of pathologies as the remainder of the thyroid, and hence, it is important to recognise this normal variant on imaging. In current guidelines, the documentation of TPLs is not included in any imaging modality guideline. In addition, given the potential relevance in the pre-operative setting, the documentation of an existing pyramidal lobe on routine pre-operative thyroid ultrasonography may help to ensure complete resection at surgery. 1
Although there is a range in the incidence of TPLs recorded by US within existing literature from 21% to 58.1%,9,11,13,14 the largest study by Kim et al. 10 found an incidence of 39.5% in a multi-centre study. However, these studies only included pre-operative patients and a protocol without cine-loop. Therefore, our study compares favourably with the previous studies incident rate of 39.5% without cine-loop in patients without having undergone thyroidectomy.
Variations in the reported occurrence rates of TPLs in the literature may be attributed to differences in sonographer expertise. 10 In this study, a noteworthy number of TPLs were retrospectively identified on cine-loop images during a secondary review by radiologists, which had not been initially identified by sonographers. This finding points to potential differences in the training of sonographers and radiologists. In addition, we observed that a considerable number of small TPLs, especially those not connected to the isthmus, were initially missed in static images. Therefore, we strongly advocate for capturing cine-loops at the appropriate level, regardless of whether the TPL is detected during real-time scanning. This study also emphasises the importance of meticulous scrutiny when examining subtle findings and atypical configurations during secondary cine-loop reviews.
In post-operative patients, many case reports have suggested that the pyramidal lobe may be a site of recurrent disease.6,7,15–17 It is indeed challenging to assess the TPL in post-operative patients partially due to the lack of sonographic landmark ability post-thyroidectomy. In addition, the extensive post-surgical scaring can obscure the presence of TPLs. Interestingly, in our study, 22% of post-thyroidectomy patients (either partial or full thyroidectomies) had a visible pyramidal lobe detected with our dedicated protocol which could potentially increase the risk of recurrent or new pathology. The surgical intra-operative search pattern might contribute significantly to the wide range of reported TPL incidences (from 12% up to 75%).1,2,8,9 It is important for US practitioners to be aware of the importance of this normal variation, as it may be easier to recognise sonographically rather than intra-operatively. US practitioners should use a standard scanning protocol and include the presence or absence of the TPL in the formal report to ensure adequate surgical treatment.
We have also demonstrated that the same range of pathologies that occur in the remainder of the thyroid gland can also affect the TPL, including malignant and benign thyroid nodules and thyroiditis. In our cohort, approximately 2% (10/660) of TPL cases have been associated with either benign or malignant thyroid nodules. This detection rate of pathologies is higher than what has been documented in the available literature.
Our study has several limitations including a single-centre design. There may be different results depending on the professional background of the US practitioner. The current descriptive study also lacks the randomisation of groups to avoid the potential selection bias. The other pitfall of this study is that the false positive rate was not calculated since the consensus of a gold standard for the detection of TPL is not available in the literature. Also, not every patient in this study underwent surgery afterwards for TPL confirmation. In addition, for 204 patients with history of surgery and absence of TPL, it was not assessed if this had confirmed as having been removed during surgery.
We acknowledge the lack of computed tomography (CT) neck comparison in parallel to this study, although the current literature suggests no statistically significant differences between US and CT in the assessment of TPLs. 11 We also acknowledge possible limitations in implementing routine storage of cine-loops (i.e. data storage capacity of PACS, machine ability to take cine-loops, etc). Last but not least, reviews were not performed independently between the static images and cine-loops, which could potentially introduce reviewers’ bias.
In conclusion, our study suggests that pyramidal lobes are common normal variants, which can be accurately detected using US pre- and post-operatively. The detection is improved with cine-loop images. It is important to remember that incomplete resection of the pyramidal lobe may result in post-operative diagnostic and treatment dilemmas, including recurrence of the primary pathology. It is therefore important that radiologists and sonographers consider a standard protocol to detect and formally report them.
Supplemental Material
sj-tiff-1-ult-10.1177_1742271X231225047 – Supplemental material for Cine clips increase the detection of thyroid pyramidal lobe in routine thyroid sonogram
Supplemental material, sj-tiff-1-ult-10.1177_1742271X231225047 for Cine clips increase the detection of thyroid pyramidal lobe in routine thyroid sonogram by Yi Yan, Xiaoou He, Kai Hu, Jed Frankel, Jian Liu, Ashraf Goubran and Fern Karlicki in Ultrasound
Footnotes
Contributors
Y.Y., X.H., K.H. and F.K. were involved in the conception and design, literature search, data acquisition, data analysis, drafting of the initial manuscript and critical revision for important intellectual content. J.F., J.L. and A.G. were involved in data acquisition, data analysis and editing the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
This study was approved by the Research Ethics Board (REB) from University of Manitoba.
Permission from patient(s) or subject(s) obtained in writing for publishing their case report
Yes, every patient involved signed consent form.
Permission obtained in writing from patient or any person whose photo is included for publishing their photographs and images
Yes, every patient involved signed consent form.
Confirm that you are aware that permission from a previous publisher for reproducing any previously published material will be required should your article be accepted for publication and that you will be responsible for obtaining that permission
Yes.
Guarantor
F.K. is the guarantor of this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.