
Abstract
Introduction:
Cavernous haemangioma is the most common benign non-infiltrative neoplasm of the orbit. Most cavernous haemangiomas are intraconal and lateral in location.
Case report:
We present a rare case of a cavernous haemangioma with an unusual location in the supraorbital region of the orbit, presenting with soft tissue swelling.
Discussion:
Cavernous haemangiomas are the most common benign non-infiltrative neoplasms of the orbit and have a slowly progressive mass effect. A slowly progressive proptosis is the typical presenting symptom. Extraocular muscle impairment and impaired visual function are seen with large lesions and with lesions located at the orbital apex. Most cavernous haemangiomas are typically intraconal and lateral in location. Extraconal and medial locations are uncommon. Ultrasound, computed tomography and magnetic resonance imaging are useful imaging techniques for the evaluation of such tumours. Treatment of the tumour is surgical excision. Complete excision is generally accomplished as the tumour is well-encapsulated with relatively few feeding vessels.
Introduction
Cavernous haemangiomas are the most common vascular lesions of the orbit in adults, being commonly seen in middle age, with a female predilection. 1 They result from new formation of vessels, proliferation of tissue components of the vessel wall and hyperplasia of cellular elements ordinarily concerned with the genesis of vascular tissue. Over 80% of orbital cavernous haemangiomas are located within the intraconal compartment, most commonly in the lateral aspect. 2 Progressive painless proptosis is the usual mode of presentation, and acute presentations are rare. 3 We report an unusual acute presentation of a supraorbital, extraconal cavernous haemangioma presenting with soft tissue swelling.
Case report
A 45-year-old man presented with gradually progressive onset swelling in the supraorbital region of the left orbit for the past 4 months. He had not sustained antecedent trauma and did not provide any other significant medical history such as bleeding diathesis or drug intake. The swelling did not change in size with the Valsalva manoeuvre, coughing, straining or a change in head position. On examination, the best corrected visual acuity in both eyes was 20/20, N5. The right eye examination was unremarkable. The cornea and sclera were normal. General and systemic examination findings were normal. Haematological investigations did not suggest any bleeding disorder. He was given symptomatic treatment and advised to review after a week. When he returned 10 days later, the swelling remained the same.
Ultrasound revealed a well-encapsulated, compressible, echogenic mass lesion (approximately 2.8 × 1.7 cm in size) situated in the subcutaneous tissues of the supraorbital region in the extraconal space of the left orbit (Figure 1). On Doppler interrogation, the mass showed few vascular channels in the periphery (both arterial and venous channels) suggestive of a vascular lesion (Figure 2). Small low-flow feeding arteries were seen. The left globe was otherwise normal (Figure 3). The intraocular muscles and optic nerve sheath complex showed normal signal intensity. The patient was counselled for magnetic resonance imaging (MRI) of the orbits for further evaluation of the swelling; however, due to financial constraints, the patient was unwilling to proceed with this.
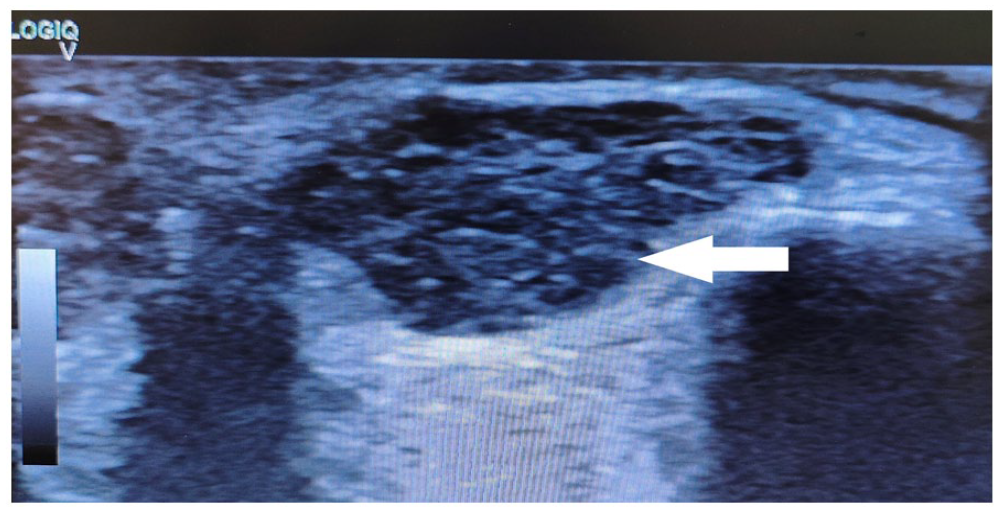
Ultrasound revealed a well-encapsulated, compressible, echogenic mass lesion (approximately 2.8 × 1.7 cm in size) situated in the subcutaneous tissues of the supraorbital region in the extraconal space of the left orbit.
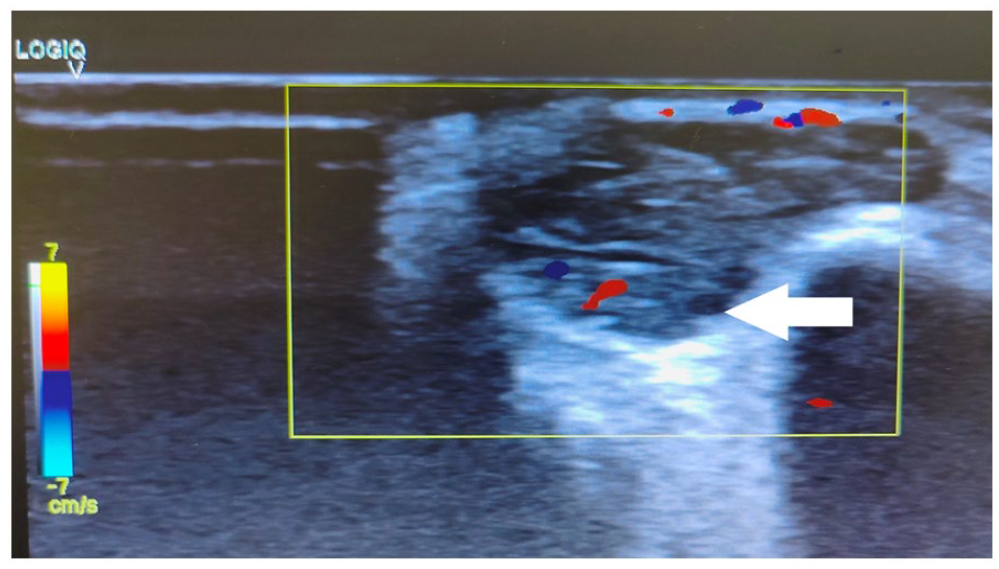
On Doppler, the mass showed few peripheral vascular channels (both arterial and venous channels) suggestive of a vascular lesion. All low-flow feeding arteries were seen.
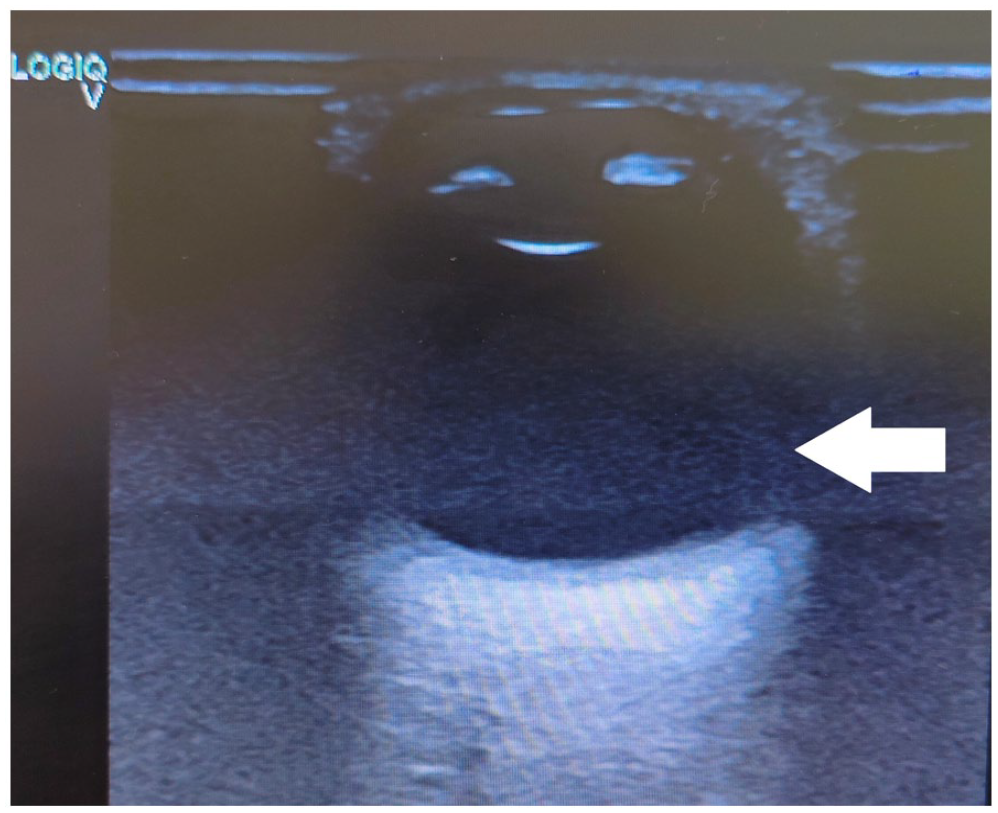
The left globe is otherwise normal.
After written informed consent and proper psychological counselling, the patient was taken to the operating theatre for excision of the lesion. The tumour was excised using an anterior supraorbital incision approach (Figures 4 and 5). Histopathology confirmed the diagnosis of cavernous haemangioma. The post-operative period was uneventful. The patient was discharged subsequently and followed up after 1 month of surgery, which showed complete resolution of the swelling.
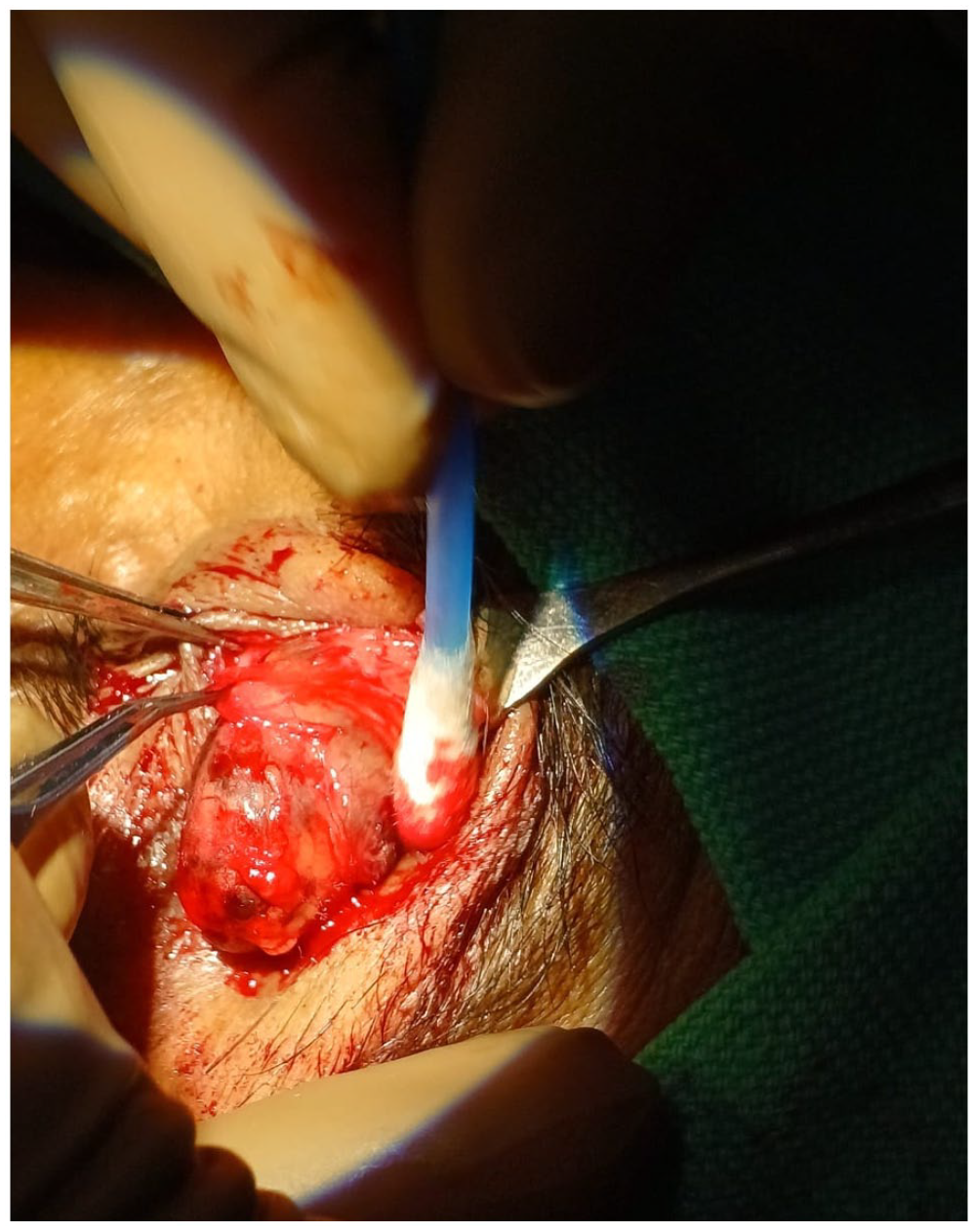
The tumour was excised using an anterior supraorbital incision approach and excision of the mass.

Post-operative tumour image.
Discussion
Haemangiomas (benign vascular neoplasms) are classified as capillary and cavernous. A capillary haemangioma usually presents in the first year of life and often increases in size for 6–10 months before slowly involuting. Cavernous haemangiomas are the most common benign non-infiltrative neoplasms of the orbit and have a slowly progressive mass effect. 1 They are usually present in the second to fourth decades of life and are more frequent in females.2,3 A slowly progressive proptosis is the typical presenting symptom. Extraocular muscle impairment and impaired visual function are seen with large lesions and with lesions located at the orbital apex. Clinically, these tumours are soft and do not change in size with the Valsalva manoeuvre, coughing, straining or a change in head position.4,5 Most cavernous haemangiomas are typically intraconal and lateral in location. Extraconal and medial locations are uncommon. A cavernous haemangioma of the orbit, which typically presents as a slow-growing tumour with gradual onset of symptoms, usually causes a mass effect, due to an increase in the volume of the orbital contents. The patient may present with a painless, slowly progressive bulging of the globe. A reduction in visual acuity and the presence of visual field defects are manifestations of a mass effect or pressure on the optic nerve and surrounding vasculature. Diplopia may occur due to extraocular muscle dysfunction. Lagophthalmos due to extraocular muscle dysfunction or nerve involvement results in exposure to keratopathy, keratitis and corneal perforation. Pupillary dysfunction is sometimes noted due to the involvement of neural structures within the orbit. Ultrasound, computed tomography (CT) scan and MRI are useful imaging techniques for the evaluation of cavernous haemangiomas. Angiography is rarely required. 6 The tumours are round to oval in shape with well-defined borders and a specific ‘honeycomb’ pattern of alternating weak and strong echoes corresponding to their structure, with flow demonstrated with colour Doppler interrogation although they may also demonstrate a negative Doppler phenomenon, which is attributable to the stagnant blood within the vascular spaces. 7 CT scan shows discrete lesions with varying degrees of enhancement. On MRI, the lesions are homogeneous, isointense to muscle on T1 weighted images and hyperintense to muscle on T2 weighted images; however, our patient did not give consent for the MRI. Histopathology reveals a fine capsule that surrounds a tumour consisting of large endothelium-lined channels with abundant, loosely distributed smooth muscle in the vascular wall and stroma. Treatment of the tumour is surgical excision. Complete excision is generally accomplished as the tumour is well-encapsulated with relatively few feeding vessels. However, in our case, it only presented with a swelling in the supraorbital region without any extension to the orbit. Such an unusual location in the supraorbital region and extraconal location has not been described to date, which makes this case a rare entity.
Conclusion
Supraorbital cavernoma is a rare but important cause of swelling in the supraorbital region. Although many cases are described in the literature for the intraconal location, an extraconal location in the supraorbital region is rarely described, making this case a unique entity. This differential diagnosis should always be included for any swelling in the supraorbital region of the orbit.
Footnotes
Contributors
Dr. Sandip Maheshwari.
Data availability
The data sets analysed are available from the corresponding author on request.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Nil.
Informed consent
The patient’s signed consent form is available from the author on request.
Permission from patient(s) or subject(s) obtained in writing for publishing their case report
Yes.
Permission obtained in writing from patient or any person whose photo is included for publishing their photographs and images
Yes.
Confirm that you are aware that permission from a previous publisher for reproducing any previously published material will be required should your article be accepted for publication and that you will be responsible for obtaining that permission
Yes.
Guarantor
Dr. Sandip Maheshwari.