
Abstract
In the late 1950s and early-to-mid-1960s, Glasgow led the world in the development of diagnostic obstetric ultrasound technology, the result of fortuitous collaboration between key individuals advancing the application of an industrial technology. Originally used to detect flaws in metal pressure vessels, the obstetrician Ian Donald, during his military service, reflected on how ultrasound could benefit his own field. Donald involved the engineer Tom Brown to tackle the technical challenges. Brown, in turn, employed a young graduating industrial designer, Dugald Cameron, to address the design, aesthetic and ergonomic aspects of these early engineering prototypes. While previous accounts of these developments have rightly celebrated the medical, technical engineering and imaging achievements of this innovative technology, the discussion of the role of the creative design expertise which addressed serious ergonomic, aesthetic and production manufacturing shortcomings of the first prototypes has been less coherent. This article relates, through key drawings, extracts from witness statements and discussions with Cameron himself, the key design decisions and features resulting in the Sundén and Diasonograph machines, the latter being the world’s first commercial production-series obstetric ultrasound machine, deployed in Glasgow hospitals and beyond.
Introduction
Arguably the most important technological development to positively affect the health of women in the last 60 or so years has been diagnostic obstetric ultrasound. For a few short years in the late 1950s and early-to-mid-1960s, Glasgow led the world in its development. A unique collaboration between clinical obstetrics, engineering, electronics and industrial design expertise created the world’s first prototypes and production models of ultrasound scanners for obstetric scanning in Glasgow hospitals.
While previous accounts of these early developments have rightly celebrated the medical, technical engineering and imaging achievements of this innovative technology, much less has been said about the design expertise which addressed the serious ergonomic, aesthetic and manufacturing shortcomings of the first prototypes and which enabled the first commercially viable machines to be put into production.1–5
Then a young graduating industrial design student at The Glasgow School of Art (GSA), Dugald Cameron, in his first paid commission, worked closely with Kelvin Hughes’ engineer Tom Brown, transforming a brilliant innovation but a clumsy piece of technical apparatus into an elegant, usable and commercially viable manufacturing design. In so doing, Cameron played his own part, as a designer, in helping to revolutionize the clinical management of antenatal treatment and care in Glasgow and beyond.
Although engineering was a world-leading industry in the west of Scotland, industrial design (better known today as product design) as an academic discipline and a profession, was in its infancy in the UK in the late 1950s, concerned primarily with the aesthetics, ergonomics and usability of manufactured products. GSA was the first educational institution in Scotland to adopt this as a specific programme of study: Cameron, therefore, was one of the very first individuals trained as a designer to be working with industry in Scotland at this time.
To mark the 60th anniversary of the seminal paper by Donald, MacVicar and Brown, published in The Lancet in 1958, 6 Cameron was invited by GSA in 2018 to give the public lecture ‘Making Waves’ at the Royal College of Physicians and Surgeons of Glasgow. 7 In December 2018, given the renewed interest in this historic innovation, the Scottish Parliament also debated a motion during this 60th anniversary year, acknowledging the contributions of all involved. 8 These two key public events also helped fill in essential details in the story for GSA’s 2019 Ultrasonic Glasgow exhibition acknowledging and celebrating Cameron’s contribution. 9
Reconstructing the design story through the archive and from witness accounts
That Cameron’s contribution to these early developments is able to be accurately documented is due to a combination of fortunate circumstances. The author, as he had trained under Cameron in the 1970s and had remained in contact with him in the intervening years, was keen that the crucial role of the designer in this story was accurately recorded. Prior accounts of the design process are fragmentary and Cameron (born 1939) is the last surviving individual involved in this pioneering work able to provide a lucid and detailed account of the individuals involved and technical developments at that time.
In 2014, Cameron had donated his student portfolio to GSA containing his key drawings for the early Glasgow ultrasound machines. These were officially accessioned into the GSA Archives and Collections (reference number DC 091) in 2016. With Cameron’s assistance, with access to Cameron’s own personal library of photographs and to the drawings held at GSA, and through a review and selecting editing of previous accounts, a reconstruction of the full design story was made possible. Once Cameron’s key drawings had been identified, they were conserved and prepared for display forming the centrepiece of GSA’s Ultrasonic Glasgow exhibition and allowing, for the first time, the full set of Cameron’s drawings showing the evolution of the design to be seen in its entirety.
Pioneering medical obstetric ultrasound in Glasgow
Ian Donald (1910–1987) (Figure 1) trained in obstetrics and gynaecology in London. In 1954 Donald was appointed Regius Chair of Midwifery in Glasgow, a position he held until 1976. Donald had the brilliant idea of exploring the use of pulsed sonar in obstetrics while serving as a medical officer on the Hebridean island of Benbecula during the war when he became familiar with Radar and Sonar. Donald’s very earliest ultrasound investigations were on biological materials at Babcock & Wilcox, a Glasgow engineering company. His first experiments in Glasgow’s Western Infirmary were with an instrument of the Mark IV flaw detector type manufactured by Kelvin Hughes (a scientific instrument-manufacturing company established in the 19th century by Lord Kelvin). In due course, Donald would launch the new science of diagnostic medical ultrasound.
Ian Donald (1910–1987), Regius Chair of Midwifery at the University of Glasgow from 1954 to 1976. Photo reproduced by the kind permission of the British Medical Ultrasound Society.
Tom Brown (1933–2019) (Figure 2) was an engineer working at Kelvin Hughes. Brown’s detailed 1999 account of the technical development of ultrasound scanning techniques in Scotland 1956–1979 covers the origins of industrial ultrasonic testing for flaws in pressure vessels, the early experiments by Donald in the application of these machines in obstetrics, and the technical challenges in translating the ultrasonic ‘echo’ into useful imaging ‘information’. 1 Working at Kelvin Hughes, Brown built the first direct contact B scanner in 1956 (Figure 3). This was patented and was in clinical use later that year in Glasgow’s Western Infirmary. Brown then went on to build the first automatic scanner (Figure 4). More than two thousand patients were scanned in this way. The process of technical development was very closely linked to the clinical agenda resulting in early clinical payoff. Through the evidence generated by their results Donald, MacVicar (then registrar in the Department of Midwifery) and Brown alerted the medical profession to the possibilities of the use of ultrasound for diagnostic obstetric purposes in their landmark paper from 19586. Cameron has always been at pains to make it clear that ‘without Ian Donald it would not have happened but without Tom Brown it could not have happened’. 7
Brown, standing in front of the newly built contact scanner c. 1957. Photo reproduced by the kind permission of the British Medical Ultrasound Society.
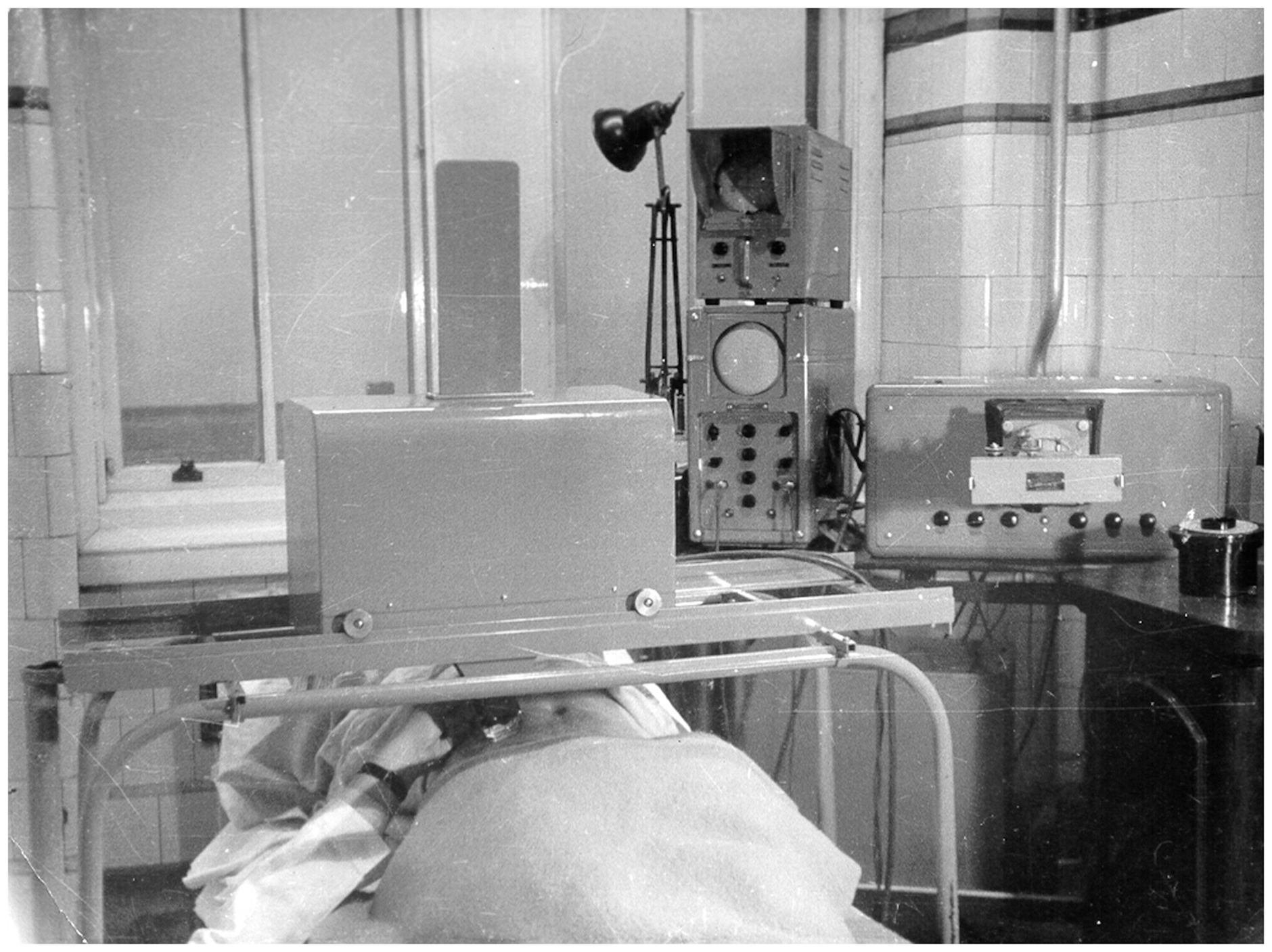
The first direct contact B scanner was patented and built by Brown in 1956. The University of Glasgow’s Hunterian Museum holds this scanner as part of its British Medical Ultrasound Society collection. Photo reproduced by the kind permission of the British Medical Ultrasound Society.
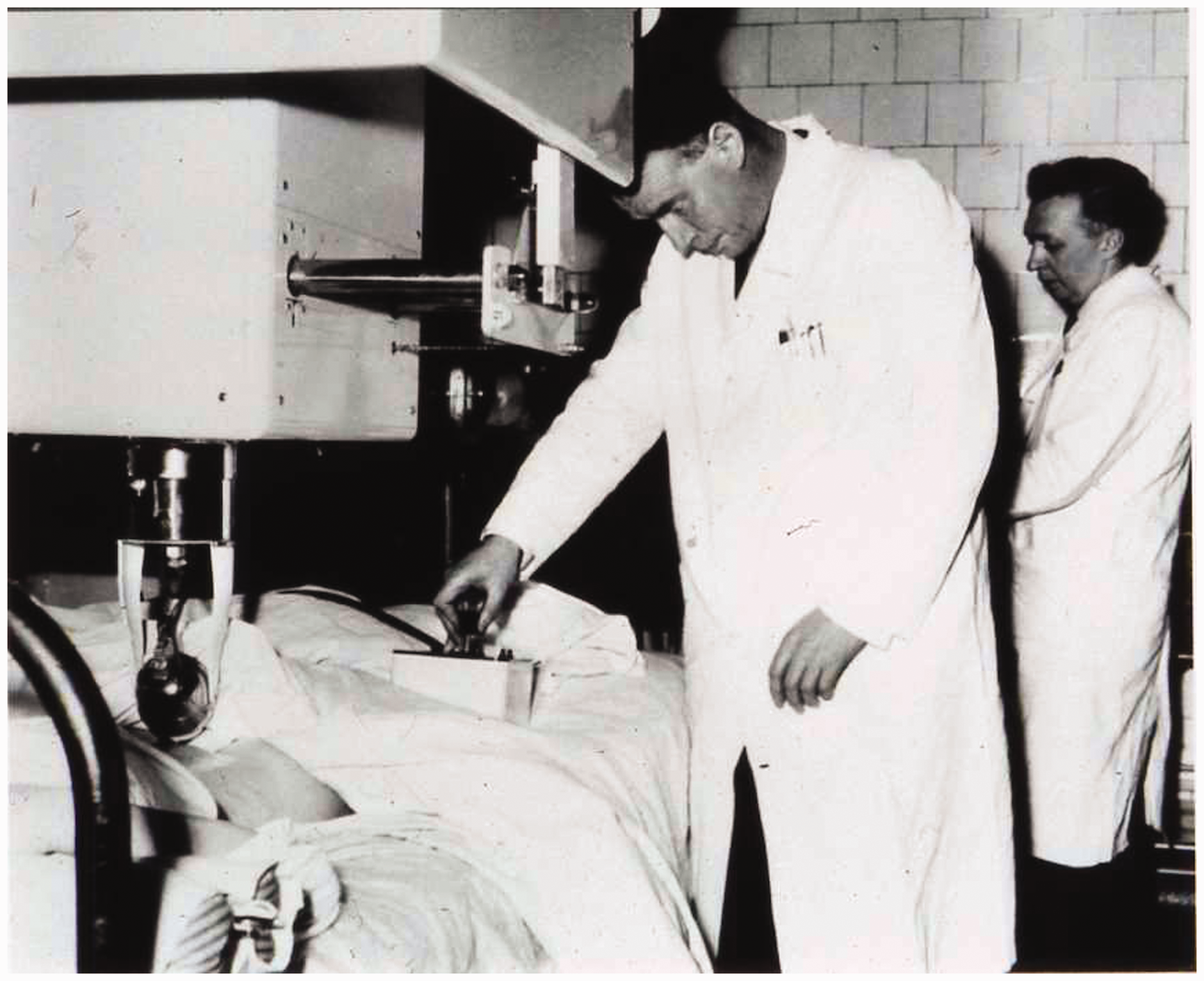
The automatic scanner being operated by Donald and MacVicar in the Glasgow Western Infirmary, c. 1960. Photo reproduced by the kind permission of the British Medical Ultrasound Society.
Issues with early designs
The development of ultrasound devices for obstetric purposes faced many challenges, e.g. how to adapt the existing technology for its new purpose, how to match the apparatus to the perceptual faculties of the human user, how best to image the developing foetus in its mother’s uterus, and how to ensure the design of the equipment was acceptable, usable and commercially viable for manufacture. However, the design configurations of the early machines by Brown and Donald had proved problematic. Brown admitted to the crudeness and limitations of the prototype contact B scanner, essentially a test-rig built from government-surplus elements, ‘Meccano’™ sprockets and chains, and using a borrowed hospital bed table (Tansey and Christie,
3
p.13) Initially this allowed only transverse scans to be made, with the unfortunate operator - usually John MacVicar [Registrar] - guddling about underneath it in a most cramped and uncomfortable position, hardly conducive to good experimental technique. (Brown,
1
p.7) [He was] crouching at the bedside, reaching up under this infernal machine, trying to carry out a regular compound scan over the patient, while getting olive oil running up his arms, and bumping his head on the underside of the frame. Generally, it was an ergonomic catastrophe. (Tansey and Christie,
3
p.20)
The concept for the first commercial machine
After the contact and automatic scanners had been built by Kelvin Hughes, the Obstetrics and Gynaecology Department of the University Hospital in Lund in Sweden placed an order for a new machine. Brown had developed a proposal for its design, drawn up as an engineering drawing by one of Kelvin Hughes’ draughtsmen. In 1961 Cameron, then a fourth-year Industrial Design student at GSA, first came into contact with Brown and, due to his skills in perspective, presentation (through his airbrush technique) and production drawing and his training in aesthetics and ergonomics, was first asked to draw up Brown’s proposal for the Lund scanner. Figure 5 shows Cameron’s original sketch prepared from Kelvin Hughes’ drawing, and Figure 6 a perspective drawing developed from this, revealing that the design was highly problematic. Kelvin Hughes’ previous automatic scanner had a heavy and bulky box which hung over the patient in a way some patients found potentially menacing. Their current design continued that tradition. Cameron recalls:
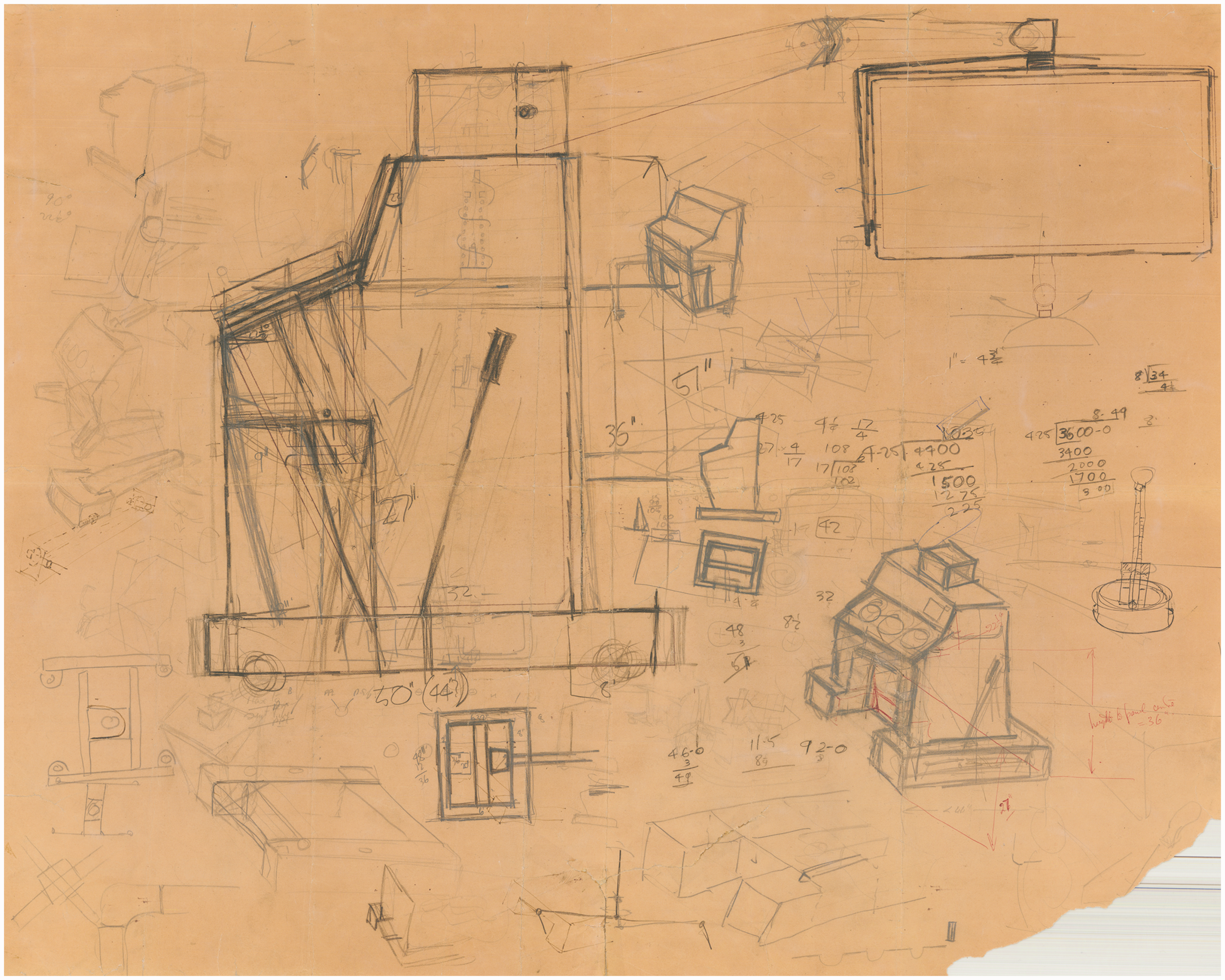
Cameron’s initial sketch visualising the original Kelvin Hughes’ concept for the Lund machine. The Glasgow School of Art, DC 091/3/1/1.
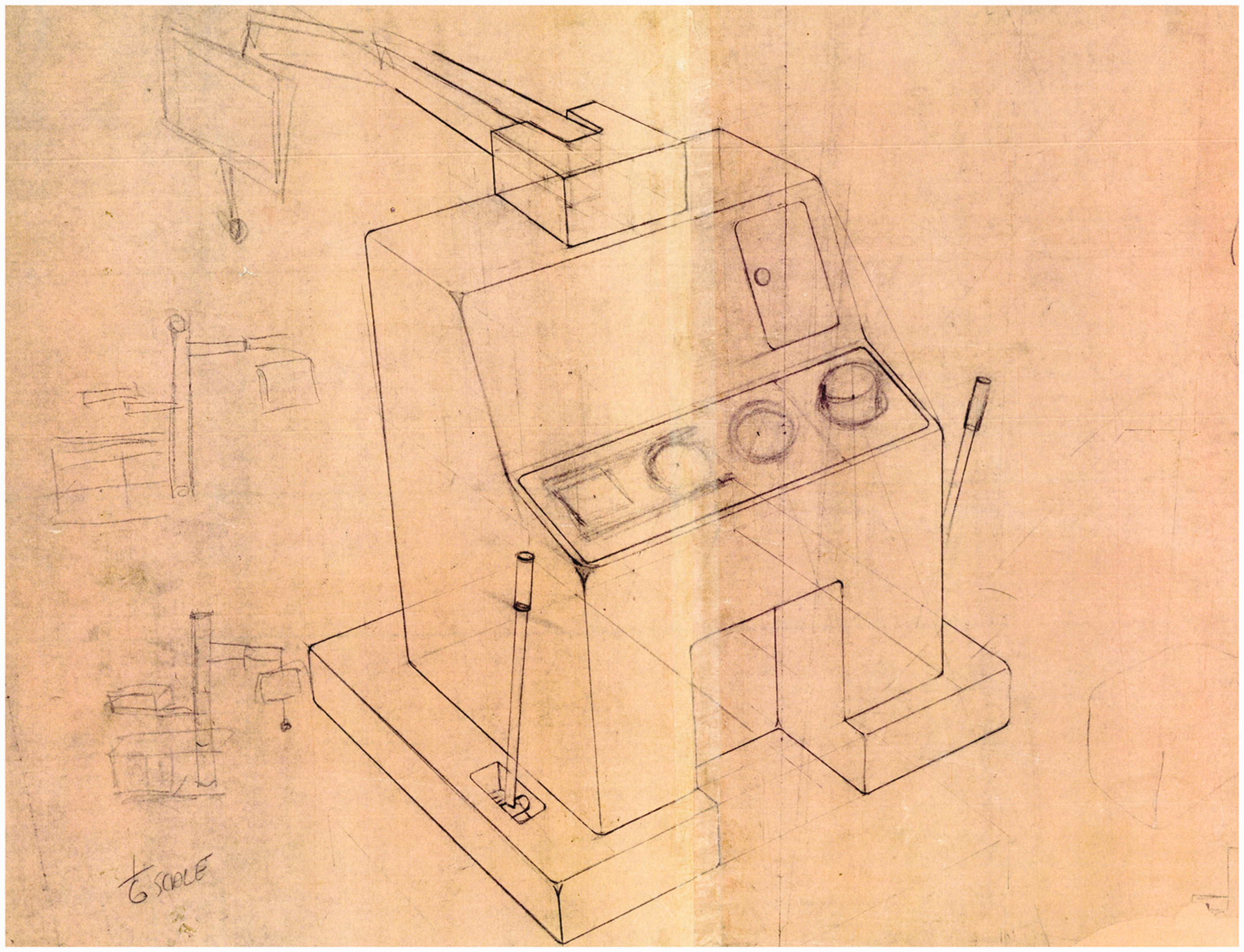
A dyeline print of Cameron’s perspective visualising the original Kelvin Hughes’ concept for the Lund machine. Note the smaller sketches on the left-hand side which were Cameron’s own ideas for the way this should be designed, leading to his own design for the Sundén machine (in Figures 7 to 9). The Glasgow School of Art DC 091/3/1/2.
That was my attempt to give a three-dimensional view of what that machine was going to look like’. ‘I remember saying that I thought it looked like a gun turret and that it was thoroughly inappropriate for pregnant ladies. This was the design drawing: Tom [Brown] and I were arguing over how to make it so that it could be used by a seated or a standing doctor, but we determined, in fact, that you couldn’t. It was useless for both, and therefore on that ergonomic basis this was not the right configuration for the machine’. (Tansey and Christie, 3 p.22)
The Sundén machine
In Figure 6, of notable interest are the small, faint sketches on the left which show the genesis of Cameron’s concept for improving Brown’s design, to be developed into the design which later came to be known as the Sundén machine. Cameron explains: I knew nothing whatever about the whole business, but had a desire to make the thing ergonomically better so that the approach to the patient was better and that the doctors would find it easier to use. (Tansey and Christie,
3
p.22) On the left [of the drawing] are the two sketches where what we thought we ought to do was to separate out the patient, the doctor, and the machine and try and put these three things in a better ergonomic relationship with one another, so that the doctor would actually be on a level with the patient and seated. (Tansey and Christie,
3
p.22) [this had] … a central stem with things growing out of it, including a desk for the operator, doctor typically, and a place for them to keep all their bits and pieces. And be level with the patient, so not looking down on the patient. (The History of Modern Biomedicine Research Group,
10
p.3) That showed the basic relationship of a desk for the doctor in which he could keep the various bits and pieces, including the olive oil when needed. The machine could be rotated in different ways so that it was very handy and the doctor could speak to the patient very easily. (Tansey and Christie,
3
p.23) We had a lot of discussions about how to make it, but in fact it was made from a proprietary system called Widney Dorlec 52, which was then adapted a bit and I had a lot of arguments about that. In fact, in retrospect, it was the right way to do it, because you didn’t want to waste time on a lot of other things in concentrating on seeing if the thing would work. (Tansey and Christie,
3
p.23)
Cameron’s presentation drawing for the Sundén machine. Photo reproduced by the kind permission of Dugald Cameron.
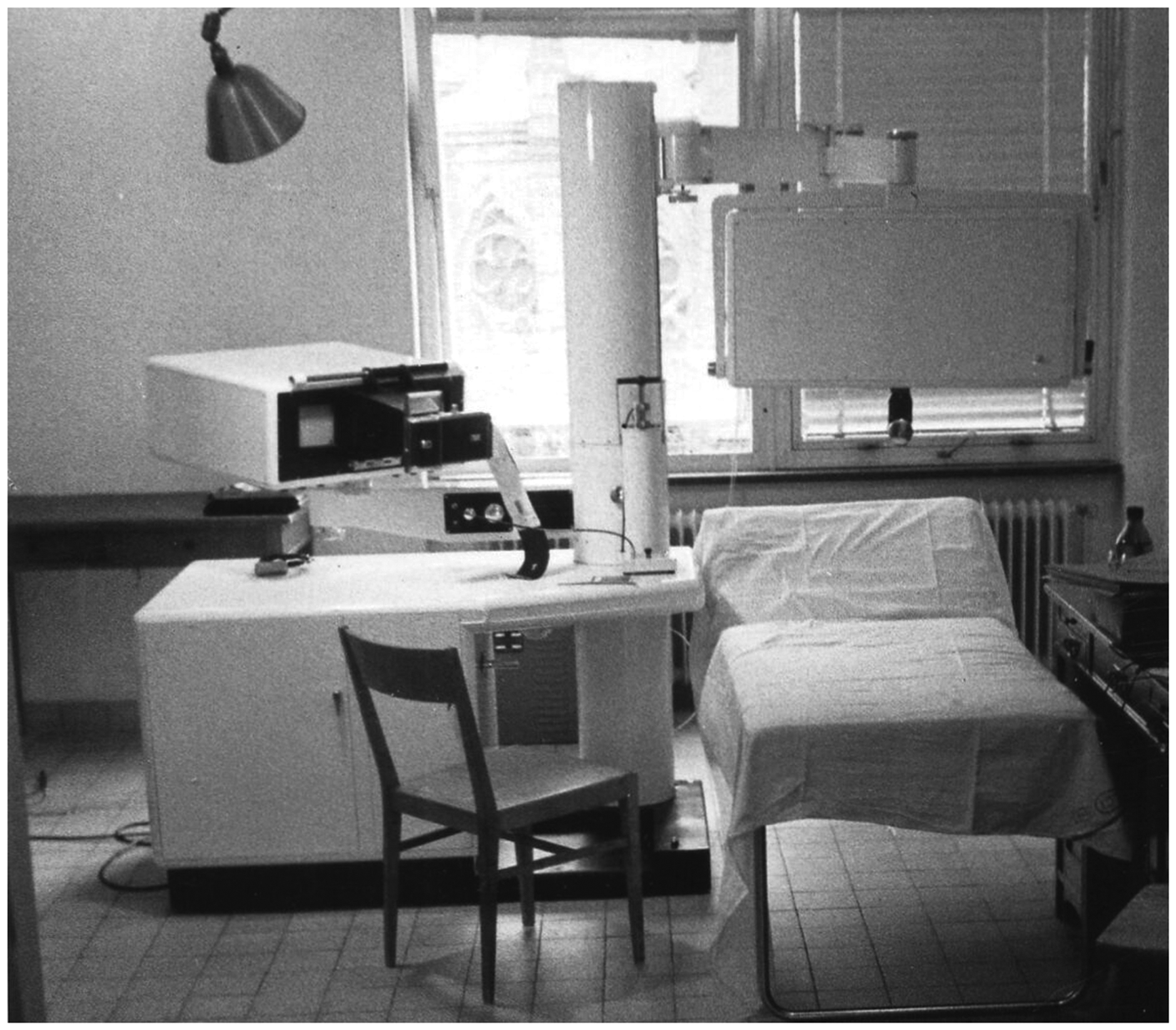
A photograph of the original Sundén machine in use in Lund in 1962. Photo reproduced by the kind permission of Juliet Ross.
A multiple view of the original Sundén machine showing movement of the scanning head. Photo reproduced by the kind permission of Dugald Cameron.
The Diasonograph
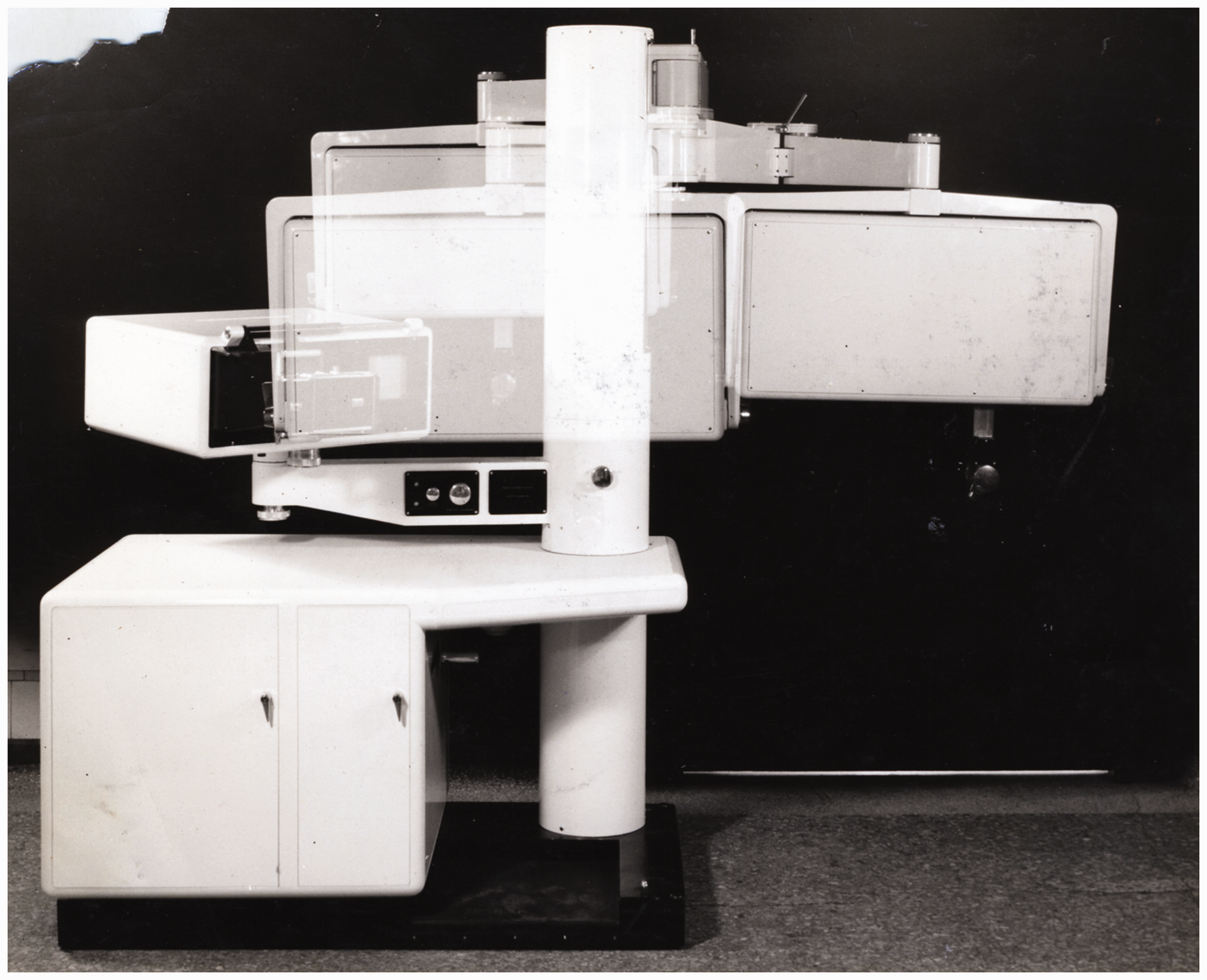
The Sundén scanner was designed and developed as a prototype but it was not pursued as a production design. However, with further design work, the Sundén machine became the prototype for the Diasonograph, the world’s first commercial production scanner (Figure 10). Brown provides the rationale for the production model:
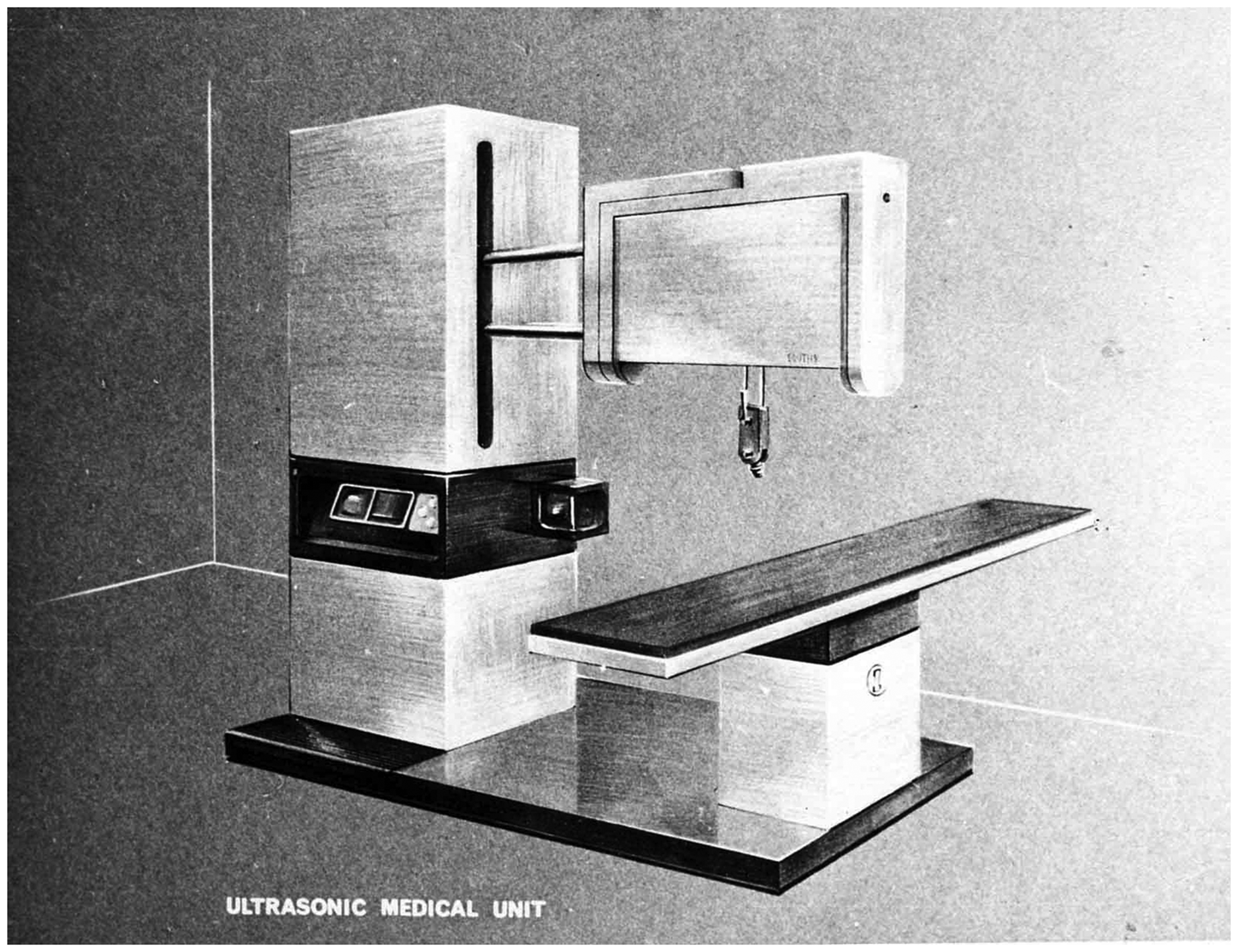
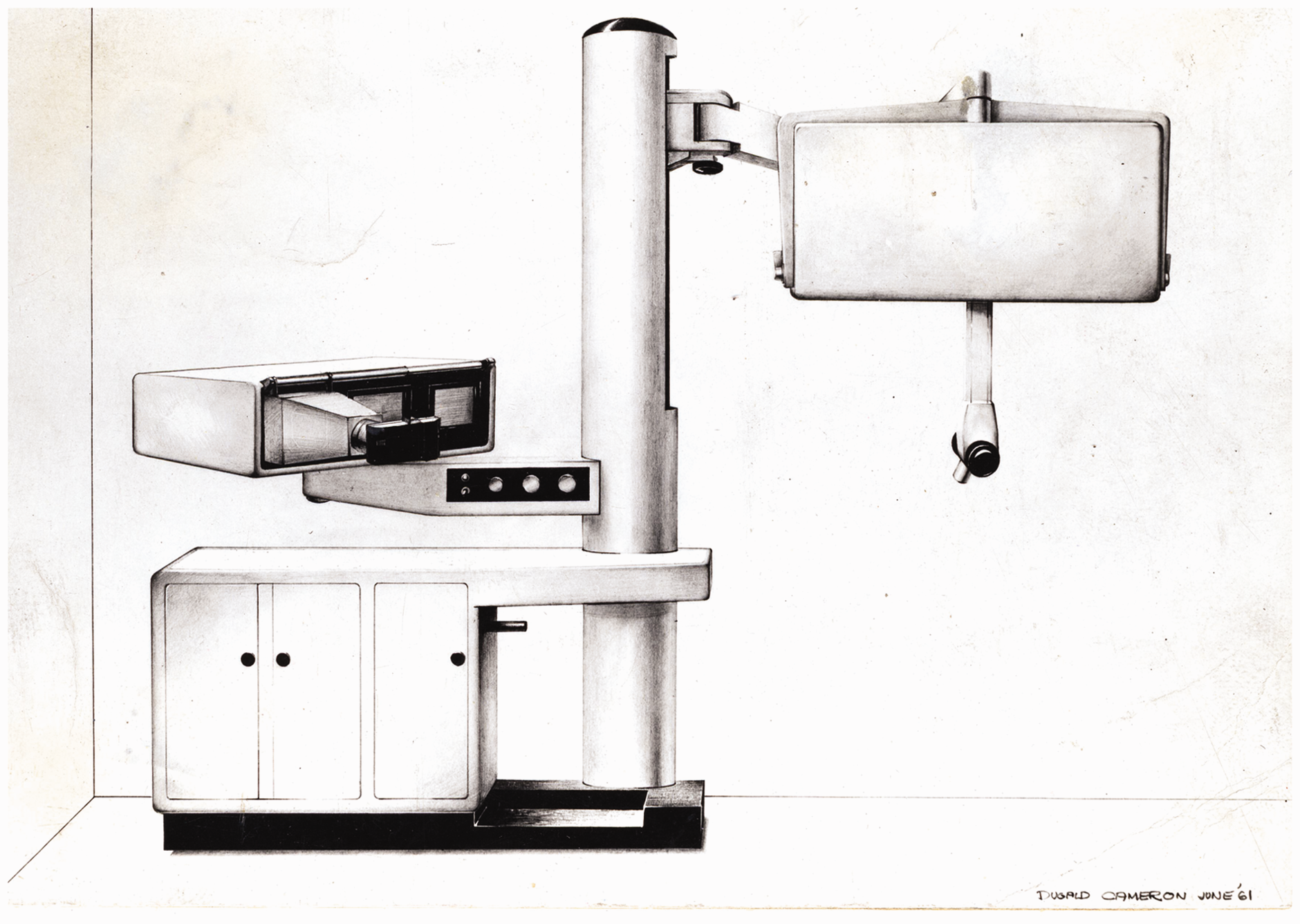
Cameron’s presentation drawing of the Diasonograph. Photo reproduced by the kind permission of Dugald Cameron.
The mechanical complexity involved in the ‘elbow-shoulder and wrist-joint’ mechanism in the Sundén machine was difficult to make. So when we came to think about a production machine, following the Sundén machine, the measuring frame which is a white box with a probe sticking out at the bottom was the same, however the mechanism for supporting it was simplified, and became a couple of bars that ran backwards and forwards inside a strong cabinet. So this was an attempt to make a cheaper Sundén machine. As it happened, it turned out to be far more slab-sided and heavy-looking than I wanted, or than Dugald wanted. (Brown, 1 pp.23–24)
The modular approach used in the Sundén machine was carried forward into the design for the Diasonograph where, if desired, the control unit could be positioned and used separately to the other elements. Cameron provides the design rationale for this machine, although the inclusion of the bed as an integral part of the machine was later discarded due to cost: This was to be the production version of the Sundén machine, and you see we were intending to make a bed for the patient as an integral part of that machine. The mechanics and the electronics of the thing were all separate. Indeed it was a modular construction. (Tansey and Christie,
3
p.22) … the configuration was split into the mechanics, which are the white bits, and the electronics, which were the grey bits. It was envisaged that the electronics, in fact, would be used on their own, so quite apart from sorting out the design of the machine ergonomically, in terms of patient and doctor, it was also sorted out in terms of mechanics and electronics. (Tansey and Christie,
3
pp.27–28) It actually took quite a lot of thinking about, because part of Tom’s [Brown] requirement to make it ‘doctor-proof’ was to make it very easy to use’. (Tansey and Christie,
3
p.28) The object was to enable the machine to be used by one person. The original design which Dugald produced had an examination couch which was operated from the control panel side of the console. That design was not put into production. What was put into production was a machine that had to be used by two people … one scanning and the other operating the controls – but it had to be possible in my view, and in our view, to operate the machine singlehandedly. (Tansey and Christie,
3
p.34)
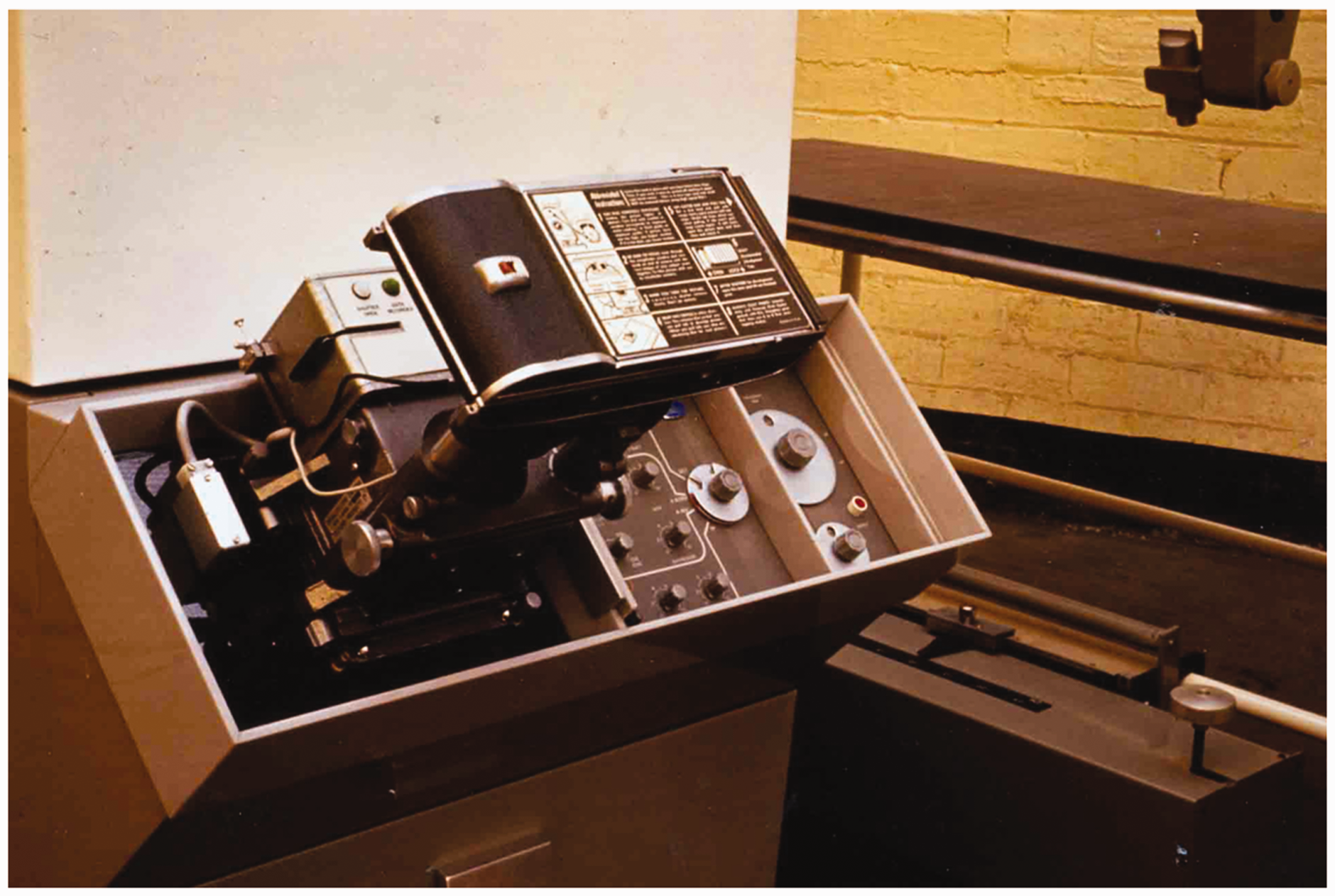
Cameron’s design for the Diasonograph’s console design with the three levels of control and polaroid camera. Photo reproduced by the kind permission of Dugald Cameron.
… the wee electronics unit could be used on its own. And I devised with them a means of controlling it. There were three levels of control. The primary control; you only needed to expose a couple of buttons here. The secondary control, which somewhat of a skilled operator could use, and the tertiary control, you pulled forward the panel in the front and you had access to all the adjustments and controls … And so there was a bit of ergonomics involved in that but it could be used on its own, and was indeed used on its own. And it was in white and pale grey, fashionable colours of the time. (The History of Modern Biomedicine Research Group, 10 p.3)
Nicolson and Fleming acknowledge the heritage of the industrial aesthetic (echoing Brown’s comment above) and its association with engineering quality and excellence: The original, elegant plan of the Sundén machine was considerably modified … the new scanner had a simpler, more linear layout. It was also bigger, its slablike sides and massive boxed superstructure proclaiming the factory’s industrial heritage. The Diasonograph was Clyde-built, at a time when that epithet still alluded to an admired tradition of heavy engineering. The scanner was certainly heavy, weighing approximately one ton. It rapidly acquired the nickname Dinosaurograph.
4
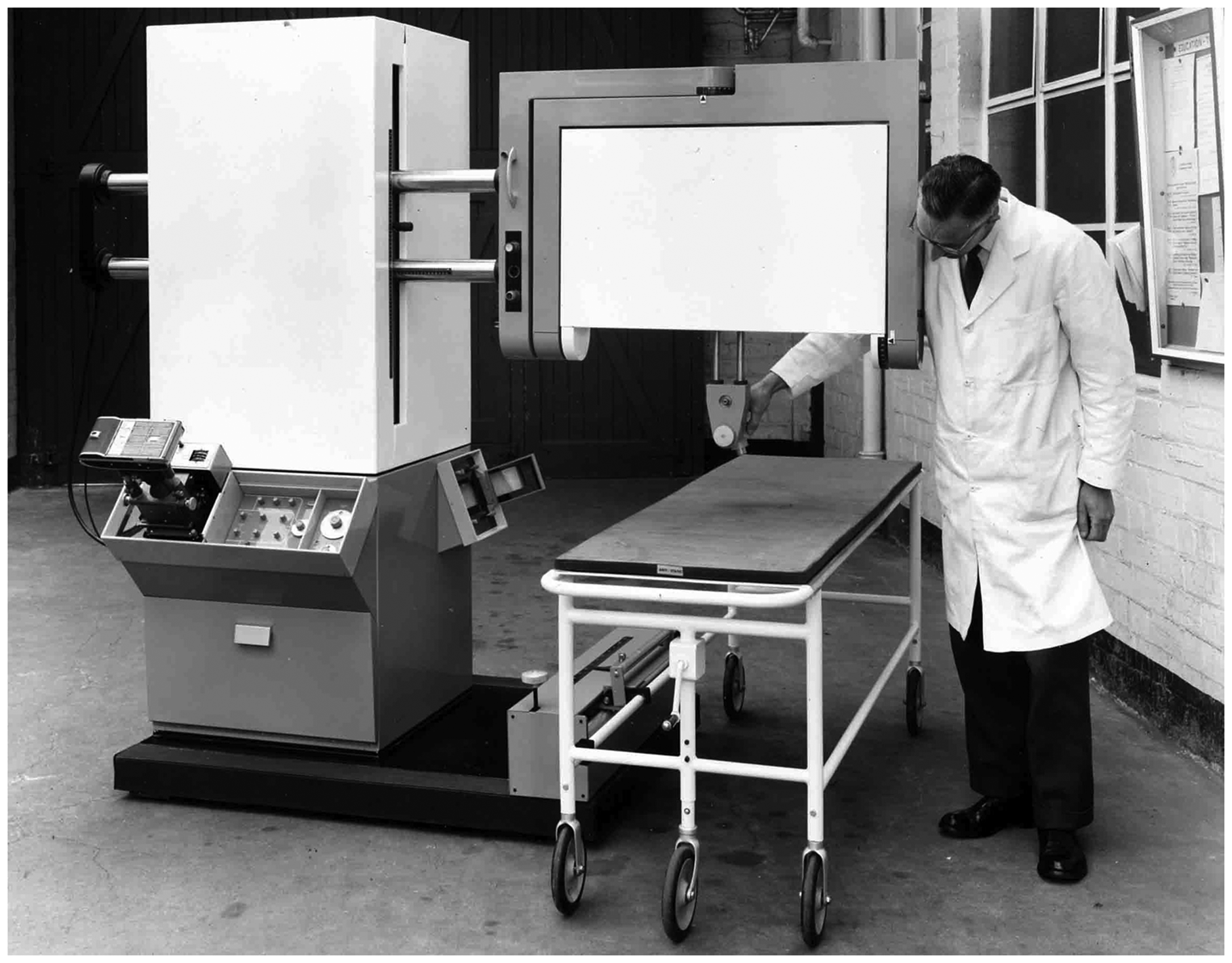
The first Diasonograph, built at Kelvin Hughes at Hillington, c. 1964. Standing beside it, to add scale, is Arthur Johnson, one of the draughtsmen involved in the project. Photo reproduced by the kind permission of Dugald Cameron.
We were due to get a Design Award, one of the very first ones, for the Diasonograph. Unfortunately, when the evaluation team came up to see it the actual machine was covered in notes and whatnot and I think Professor Donald was showing the full range of its activities and it frightened the life out of them. In fact, had it been a nurse or someone using it, we perhaps would have got the Design Award. There was a lot of early ergonomic thinking that went into the design, particularly for the design of the Sundén machine, which preceded the Diasonograph. (Tansey and Christie, 3 p.28)
Subsequent developments
Cameron began his design consultancy work with Kelvin Hughes at Hillington in 1961 with the Sundén machine while in his Diploma year and continued his work with them on the Diasonograph and some industrial flaw detectors. However, Cameron’s involvement with Kelvin Hughes at Hillington ended when they were closed down in 1966 shortly after a patents issue.
The design and production of later models of the Diasonograph and other obstetric ultrasound machines, without Cameron’s further involvement, was continued by Nuclear Enterprises, based in Edinburgh, until the 1970s. However, Cameron’s involvement with obstetric ultrasound was briefly revived when Brown started to develop the Multiplayer/3D scanner at Sonicaid in the 1970s.
Unfortunately, no models of either the Sundén or Diasonograph machines designed by Cameron are now in existence. However, Glasgow’s Hunterian Museum holds the first contact scanner as a part of its British Medical Ultrasound Society collection and an automatic scanner is held, along with a number of later machines (developed at Nuclear Enterprises in Edinburgh), in Glasgow Life’s collection at its Museums Resource Centre at Nitshill.
The designer’s vision
What is remarkable is that Cameron’s key design decisions for the Sundén and Diasonograph machines were determined and communicated, at that time, with no more sophisticated a technology than a pencil or pen assisted by simple drawing instruments on paper or tracing paper through different drawings of different types – freehand, presentation or ‘technical’ (manufacturing) drawings. Robertson, Reader in Material Cultures of Drawing, Design History and Theory at GSA, appraises Cameron’s achievement, referring to his disciplined training in observational drawing and through ergonomic exercises resulting in his profound understanding and respect for the human body, and becoming fully sensitised to the ‘human in design’. 11 Ergonomics and product (or industrial) design, as we understand this today, were young disciplines at the time of these developments.
Through the inspection of Cameron’s work, one can appreciate the vital contribution made by the emerging profession of product design to the functionality and operation of these early medical obstetric ultrasound machines in 1960s Glasgow. Cameron’s exemplary design work helped transform the early engineering test-prototypes of Donald and Brown into attractive, user-friendly and, for the first time, commercially viable production machines.
Footnotes
Acknowledgements
ASM expresses his deepest gratitude to Prof Dugald Cameron for his kind assistance.
Contributors
ASM researched and conceived the study, and provided the article to Prof Dugald Cameron to review and verify the accuracy of the account.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was granted by The Glasgow School of Art Ethics Committee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by the Royal Society of Edinburgh, Arts & Humanities Small Research Grant and by a Glasgow School of Art Research Development Grant.
Guarantor
ASM.