
Abstract

Blinding (or masking) is considered pivotal for many clinical trials to prevent elements of bias and to prevent potential confounding. In a ‘blinded trial’, for a period of time, the intervention group allocation and/or other healthcare information is not disclosed to the participant, the investigator, the outcome assessor, other members of the site team, members of the central team, statisticians and/or combinations of these roles. Many blinded trials employ placebos or sham interventions which, in the case of some treatments, need to be produced or amended on site, or brought in. The decision to implement blinding should not be lightly taken as this has considerable practical and resource implications.1–6
Many healthcare settings now use electronic health record (EHR) systems, with government aspirations to be paper-light and improve healthcare green footprint. 7 Access for patients to pertinent aspects of the EHR (‘patient portals’) is increasingly common in primary care settings and is developing in secondary care settings. This is good for patient autonomy, even if initially read-only.
Without careful consideration, information in the EHR may inadvertently allow elements of unblinding. For example, access to certain blood test results in the EHR could inadvertently reveal the treatment allocation to blinded staff or participants. This may be because of the treatment’s mode of action or a common side-effect (such as renal function change). In another setting, an early phase healthy volunteer study may give all participants the investigational treatment and blind them only to the allocated dose so that self-reporting of any side-effects is not informed by dose-related expectations. The dose needs to be visible to relevant staff but must be withheld from the participant in the EHRs. In addition, in a trial where the local pharmacy production unit makes up the active treatment while the placebo is imported, allowing all site staff to see in the EHR whether the production unit had been involved could effectively break the blind. Participants and relevant staff need to be protected from these results if they are to stay blinded.
Large, phase III trials, which might cost industry tens of millions of dollars, enrol multiple sites, internationally, in order for their treatment effects to be generalisable. Participating hospitals will use a variety of EHR systems, each with their own, local implementation and likely varying in their ability to restrict data access. Trials employing blinding crucially depend on outcome events being reported without bias. Rather than promoting high-quality research, EHRs designed poorly could delay, harm and, worse, invalidate research findings.
This is therefore an emerging and critical issue to tackle, especially for large-scale phase III or small-scale, rare disease trials where confounding could invalidate a treatment approach very early. These issues are raised by new technology predominantly because EHRs designers have deliberately focused on collation of data rather than on how it might need to be segregated. Healthcare settings must consider the needs of research when implementing a new EHR system and each EHR manufacturer needs to make it easy to enable appropriate new restrictions and controls to be applied by site teams.
In Table 1, we propose a series of simple actions that should be taken in general and for each trial at the implementation stage, prior to recruitment, and periodically thereafter. We anticipate that a ‘blinding matrix’ should be developed, including for implementation by local EHR team (see Supplemental Tables). The groups for the matrix should reflect the role groups available in the site’s EHR, the labelling of which may vary greatly across EHR systems and hospitals. Completing the matrix may require the central trial team to liaise with the local EHR team directly to ensure a correct mapping. If blinding cannot be well implemented, a site should not participate.
Actions for trials employing blinding.
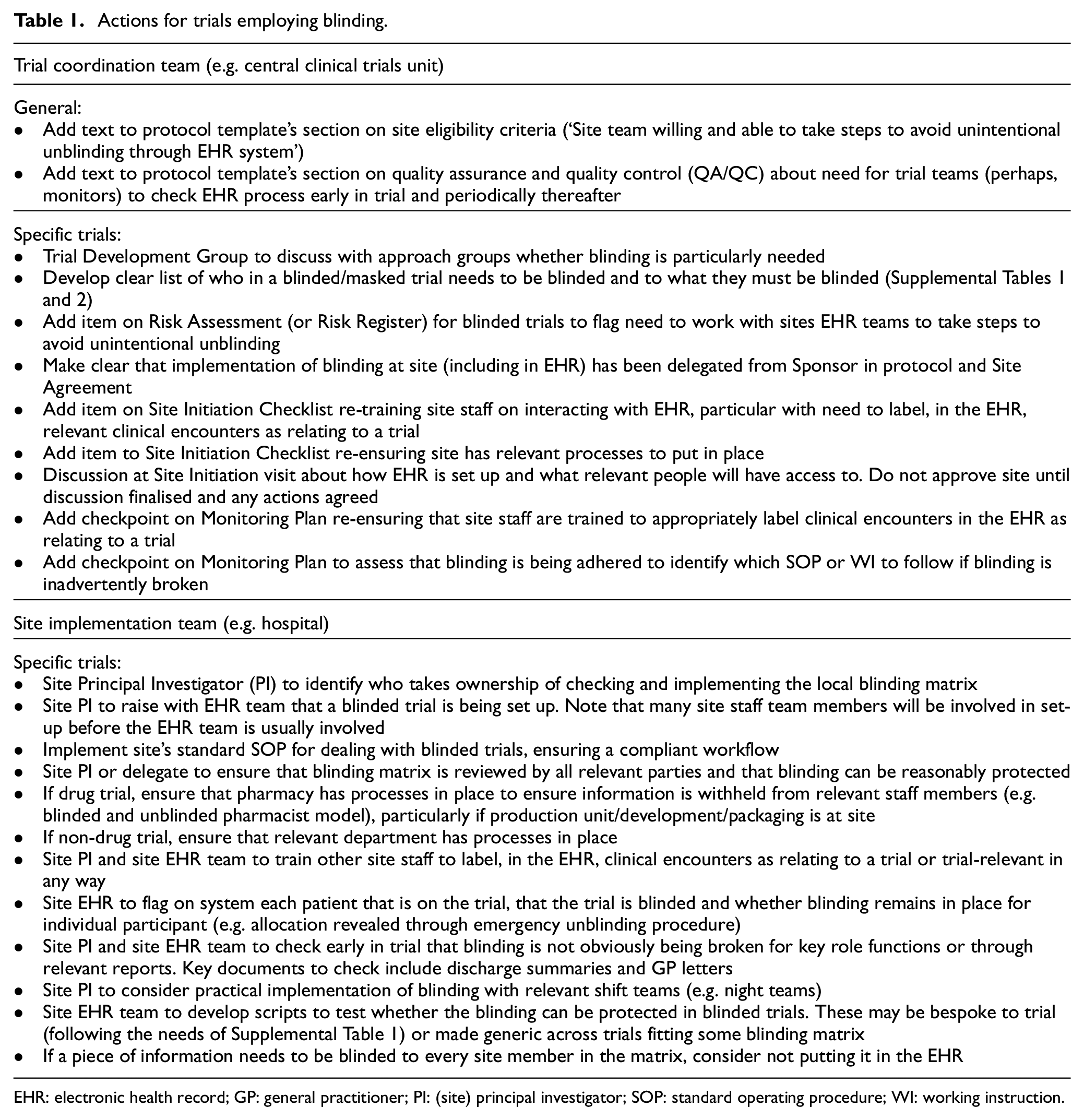
EHR: electronic health record; GP: general practitioner; PI: (site) principal investigator; SOP: standard operating procedure; WI: working instruction.
Maintaining blinding of treatment allocation can also be challenged in traditional, paper records. Although central and site teams should be more well-versed in addressing these, our tables may still prove helpful.
Groups and roles in EHR systems are complex and varied. These simple steps, employed for every blinded clinical trial, will help to protect clinical trials from the potential for inadvertent unblinding.
Supplemental Material
sj-pdf-1-ctj-10.1177_17407745211069985 – Supplemental material for Protecting blinded trials in electronic hospital systems
Supplemental material, sj-pdf-1-ctj-10.1177_17407745211069985 for Protecting blinded trials in electronic hospital systems by Matthew R Sydes, Wai Keong Wong, Ameet Bakhai, Nicola Joffe and Sharon B Love in Clinical Trials
Footnotes
Acknowledgements
The authors acknowledge Nafisah Atako, Stuart Braverman, Ferdousi Chowdhury, Celia St Claire, Debbie Ford, Sheena McCormack, Karen Sanders, Israel Serralvo-Caballero and Fiona Watson
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: M.R.S., N.J. and S.B.L. are supported by the Medical Research Council grant MC_UU_00004/08. W.K.W is supported by The National Institute for Health Research University College London Hospitals Biomedical Research Centre Grant: BRC3 IS-BRC-1215-20016.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.