
Abstract
In order to compare the curative effect of the Da Vinci surgical system (DVSS) with laparoscopic surgery (LS) or open surgery for colorectal resection, literature search was conducted in PubMed, Excerpt Medica Database (Embase), and Cochrane library up to January 15, 2016. Odds ratio (OR) and weighted mean difference with their corresponding 95% confidence intervals were used as effect size for evaluation of different outcomes. In total, 10 studies consisting of 2767 patients were included for the meta-analysis. As a result, there were no significant differences between DVSS and LS/open surgery in the long-term oncologic outcomes (p > 0.05). However, DVSS achieved a significantly lower length of hospital stay and estimated blood loss (EBL), but a longer operation time. Moreover, DVSS showed a significantly reduced conversion to open surgery than LS (OR = 0.19, 95% confidence interval: 0.08–0.48). Subgroup analysis indicated that DVSS had different results in rectal adenocarcinoma and colon cancer subgroups on outcomes of conversion to open surgery and operation time. DVSS is superior to LS/open surgery in length of hospital stay and EBL, but needs longer operation time. Long-term outcomes of DVSS are comparable with the other approaches. From long-term perspective, DVSS has an equivalent effect to the other two techniques.
Introduction
Colorectal cancer (CRC) is the third most common cancer in the world, and the main curative treatment is surgical resection. The minimally invasive surgery (MIS) has been applied into the treatment of CRC. Increasing evidence has supported that MIS approach is more advantageous compared with the conventional open surgery. 1,2 Since 1988, when laparoscopic surgery (LS) was introduced, it has been widely accepted in the field of general surgery, such as colorectal resection. 3,4 Reportedly, LS is superior to open surgery with regard to many aspects such as quicker recovery and reduced duration of hospital stay. 5 In spite of the feasibility, the application of LS in CRC is limited due to anatomical complexity and the narrow pelvic cavity. 6
Robotic surgery is an advanced technique of MIS. It was first used in 2000, and since then many robotic surgery devices have been developed, such as the Da Vinci surgical system (DVSS), which is the newest and widely used one. 7 Theoretically, robotic surgery has obvious advantages over LS, such as the greater precision, lower error rates, and the decreased bleeding. 8,9 However, other researchers indicate that robotic surgery is comparable with LS in the short-term perioperative outcomes and believe that LS could not be substituted with robotic surgery. 10,11 A previous meta-analysis compared the effects of laparoscopic hysterectomy with and without robot assistance. Five indexes were evaluated in this study, including operative time, conversion to open surgery, length of hospital stay, estimated blood loss (EBL), and postoperative complications; and the investigators found that robot-assisted laparoscopic hysterectomy had a shorter length of hospital stay and reduced conversion to open surgery numbers and postoperative complications than traditional laparoscopic hysterectomy. 12 This study might provide evidence for the benefits of robot-assisted surgery to some extent. However, long-term outcomes such as survival and recurrence were not involved in this study.
With regard to CRC, several studies have been carried out to compare the efficiency of robotic surgery, LS, and open surgery. However, controversial results are presented. With regard to long-term outcomes, Ghezzi et al. demonstrate that robotic total mesorectal excision (RTME) achieved a significantly reduced local recurrence rate (LRR) compared with open surgery mesorectal excision, 13 while similar effect on the 2-year disease-free survival (DFS) is found among open, laparoscopic, and robotic surgery. 14 Regarding short-term outcomes, it is found that robotic surgery and LS have a significant shorter length of hospital stay than open surgery, and robotic surgery is more advantageous over LS with regard to time for resumed soft diet and length of hospital stay. 14 On the contrary, another study observes a comparable conversion rate, length of hospital stay, and postoperative morbidity between RTME and laparoscopic total mesorectal excision. 15 To resolve these inconsistencies, we conducted this meta-analysis to comprehensively evaluate the efficiency of DVSS on CRC treatment, compared with LS and open surgery. Considering that there were too many studies that investigated the short-term outcomes, we mainly focused on the long-term outcomes. Meanwhile, to provide comprehensive evaluations, relevant short-term outcomes in the included studies were also extracted.
Methods
Search strategy
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines for meta-analysis of randomized control trials (RCTs), 16 studies from PubMed, Embase, and Cochrane library were retrieved until January 15, 2016. The key terms of the literature search were “DVSS,” “CRC,” “rectal cancer,” “colon cancer,” and “long-term outcomes.” The searching strategies were “Da Vinci” or “Davinci” or “robot,” “CRC” or “rectal cancer” or “colon cancer,” and “laparoscopic” or “open.”
Inclusion and exclusion criteria
The search was conducted by two independent investigators. If disagreements occurred, a discussion with a third investigator was required to reach a consensus.
Studies were included if they meet the following criteria: (1) the study was a controlled clinical trial or a RCT; (2) participants in the studies were patients with CRC or rectal cancer or colon cancer; (3) the experimental group was treated with DVSS in colorectal surgery, while the control group was treated with traditional LS or open surgery; (4) the studies provided sufficient information involving long-term oncologic outcomes, such as local recurrence, overall survival (OS), DFS, and disease-specific survival (DSS); (5) the study was an English publication.
The exclusion criteria were as follows: (1) the studies were non-original literature, such as reviews, letters, conference abstract, and plans; (2) the studies were duplicated publications; (3) data in the studies were insufficient to obtain the long-term oncologic outcomes; and (4) the studies were case series that only provided data about DVSS but not about control.
Data extraction and quality assessment
According to the aforementioned criteria, two investigators independently extracted the following data from each eligible study: first, author name, date of publication, study type, study region/country, disease type, case distributions in DVSS group and control group, age and sex of study subjects, sample size, study outcomes, and follow-up time. During data abstraction, the discrepancies were resolved by discussion with a third investigator. Meanwhile, qualities of the included studies were assessed using the QUADAS (University of Bristol, England) checklist (http://www.ncbi.nlm.nih.gov/books/NBK35156/), including 11 items that could be answered with “yes,” “no,” or “unclear,” respectively.
Statistical analysis
Long-term oncologic outcomes were the primary outcomes in this study, such as local recurrence, 3-year OS, 3-year DFS, 5-year OS, 5-year DFS, 5-year DSS, and 5-year LRR. Secondary outcomes were postoperative data, such as length of hospital stay, complications, and readmission; and operative data, such as operation time, EBL, conversion to open surgery, and protective stoma. Odds ratio (OR) and its corresponding 95% confidence interval (CI) weres used as a measure of effect size to calculate the pooled result for dichotomous variables (e.g. local recurrence, 3-year OS/DFS, 5-year OS/DFS/DSS/LRR, complications, readmission, conversion to open surgery and protective stoma), while weighted mean difference (WMD) and its 95% CI was used as the effect size for continuous variables (e.g. operation time, EBL, length of hospital stay). The heterogeneity across studies was examined by the Cochran’s Q statistic and the I2 statistic. 17 The value of p < 0.05 or I2 > 50% indicates a significant heterogeneity, and the random effects model was used with the method of DerSimonian. 18 Otherwise, the fixed-effects model was applied (p > 0.05 and I2 < 50%) with the inverse variance method. 19
For the outcomes that involve multiple outcomes, the publication bias was determined by Egger’s test, 20 and p < 0.05 indicates a significant publication bias. In addition, for all the above outcomes, sensitivity analysis was performed to evaluate the influence of a single study. If a reverse result is presented after removal of a study, it suggests that pooled results are instability.
The statistical analysis was completed using Cochrane Collaboration Review Manager 5.3 software (http://ims.cochrane.org/revman) and Stata 12.0 software.
Results
Eligible studies
The study selection process is depicted in Figure 1. Through preliminary screening, a total of 641 articles were selected (PubMed: 337, Embase: 274, and Cochrane library: 30), of which 292 were excluded because they were irrelevant and 167 were excluded due to duplicated publications. For the remaining 182 articles, through abstract reading, studies that did not meet with the criteria were further excluded, including 66 non-RCTs (e.g. reviewers, conference abstracts, and letters), 43 case series containing no controls, and 31 articles not involving DVSS. Then the remaining 42 articles were subjected to full-text examination and the following studies were further eliminated, including 24 articles without long-term oncologic outcomes, seven studies irrelevant to the comparison of DVSS versus LS/open surgery, and one plan. Finally, 10 eligible articles 5,11,13 –15,21 –25 were included in the present meta-analysis.
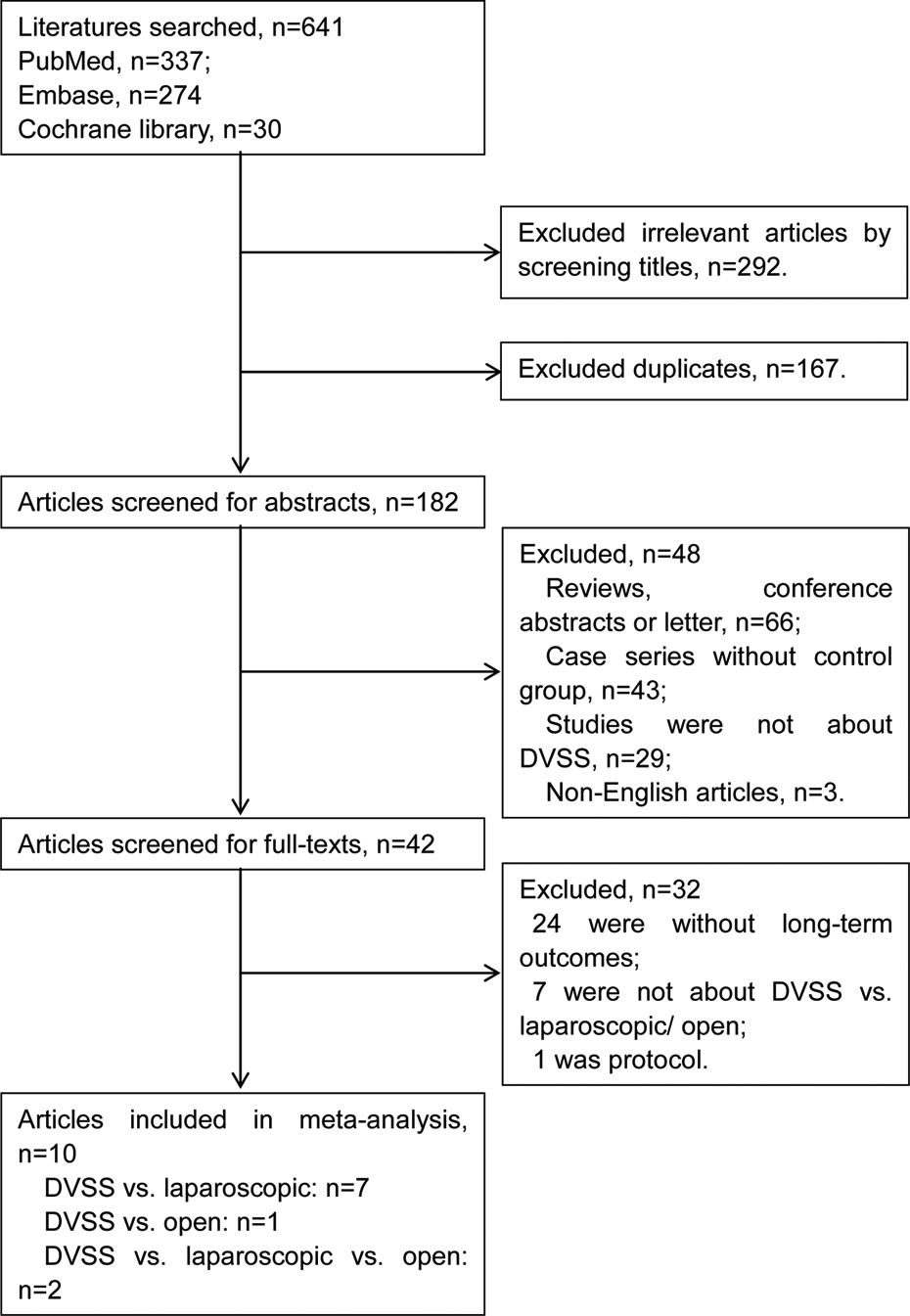
Flow chart of study selection.
Characteristics of eligible studies and the quality assessment
Characteristics of the included 10 studies are shown in Table 1. There were a total of 2767 patients, including 1005 cases in DVSS group, 1066 cases in LS group, and 696 cases in open surgery group. These studies were published from 2013 to 2015, and the majority of the patients suffered from rectal adenocarcinomas.
Characteristics of the included studies.

DVSS: Da Vinci surgical system; TME: total mesorectal excision; ISR: intersphincteric resection; M: male; F: female; m: months; y: years.
Result of quality assessment indicated that all the included studies provided information about the detailed case resources, inclusion criteria, and time for inclusion, and the overall quality was high (Table 2).
Quality evaluation of the included studies.a
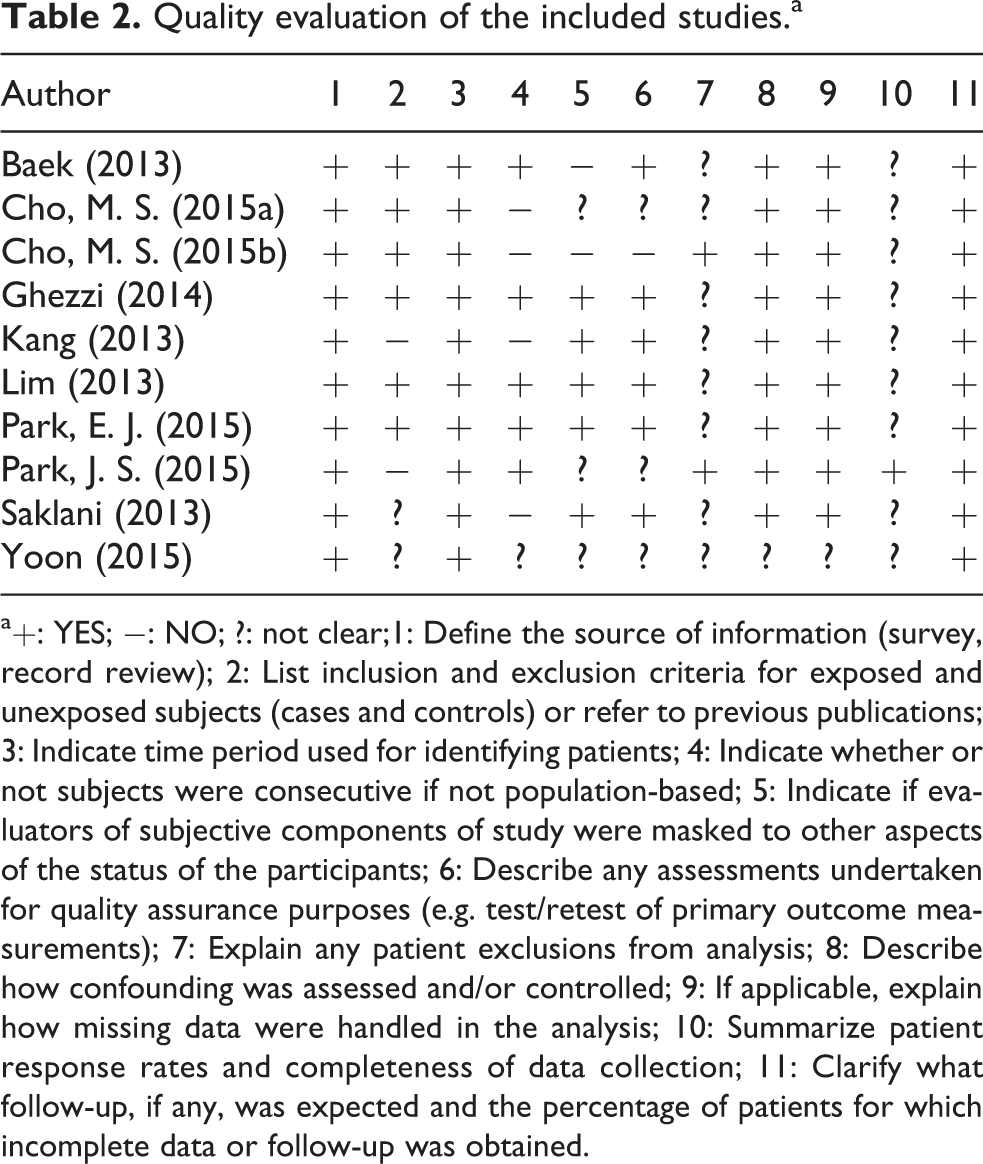
a+: YES; −: NO; ?: not clear;1: Define the source of information (survey, record review); 2: List inclusion and exclusion criteria for exposed and unexposed subjects (cases and controls) or refer to previous publications; 3: Indicate time period used for identifying patients; 4: Indicate whether or not subjects were consecutive if not population-based; 5: Indicate if evaluators of subjective components of study were masked to other aspects of the status of the participants; 6: Describe any assessments undertaken for quality assurance purposes (e.g. test/retest of primary outcome measurements); 7: Explain any patient exclusions from analysis; 8: Describe how confounding was assessed and/or controlled; 9: If applicable, explain how missing data were handled in the analysis; 10: Summarize patient response rates and completeness of data collection; 11: Clarify what follow-up, if any, was expected and the percentage of patients for which incomplete data or follow-up was obtained.
Study outcomes
Primary outcomes
Long-term oncologic outcomes were the primary outcomes, including local recurrence, 5-year LRR, 3-year OS/DFS, and 5-year OS/DFS/DSS.
DVSS versus LS
Due to the absence of significant heterogeneity (p > 0.05, I2 < 50%), the fixed-effects model was utilized for evaluations of the above seven outcomes. The pooled results indicated that DVSS showed an increased recurrence (local recurrence: OR = 1.23, 95% CI: 0.70 to 2.18, Figure 2(a); 5-year LRR: OR = 1.41, 95% CI, 0.81 to 2.44, Figure 2(d)) and reduced OS (3-year OS: OR = 0.75, 95% CI, 0.40 to 1.41, Figure 2(b); 5-year DSS: OR = 0.84, 95% CI, 0.52 to 1.34, Figure 2(g)) compared with LS, however, all without significant differences. For each outcome, there did not detect any significant publication bias across the studies (Egger’s test: p > 0.05).

Forest plots of long-term oncologic outcomes between DVSS and laparoscopic surgery. (a) local recurrence; (b) 3-year OS; (c) 3-year DFS; (d) 5-year; (e) 5-year OS; (f) 5-year DFS; (g) 5-year disease-specific survival. DVSS: Da Vinci surgical system; OS: overall survival; DFS: disease-free survival; LRR: local recurrence rate; DSS: disease-specific survival.
DVSS versus open surgery
Two studies reported the long-term outcome comparisons between DVSS versus open. Significant heterogeneity was observed for the evaluation of 5-year LRR (p = 0.01, I2 = 84%), thus a random-effects model was used to calculate the combined results. By contrast, for the remaining outcomes, the fixed-effects model was applied due to obvious homogeneity. As a result, although DVSS was superior to open surgery with reduced 5-year LRR (OR = 0.51, 95% CI: 0.06 to 4.41, Figure 3(a)), increased 5-year OS (OR = 1.48, 95% CI: 0.86 to 2.52, Figure 3(b)), and 5-year DSS (OR = 1.34, 95% CI: 0.78 to 2.32, Figure 3(d)), the differences were not statistically significant.
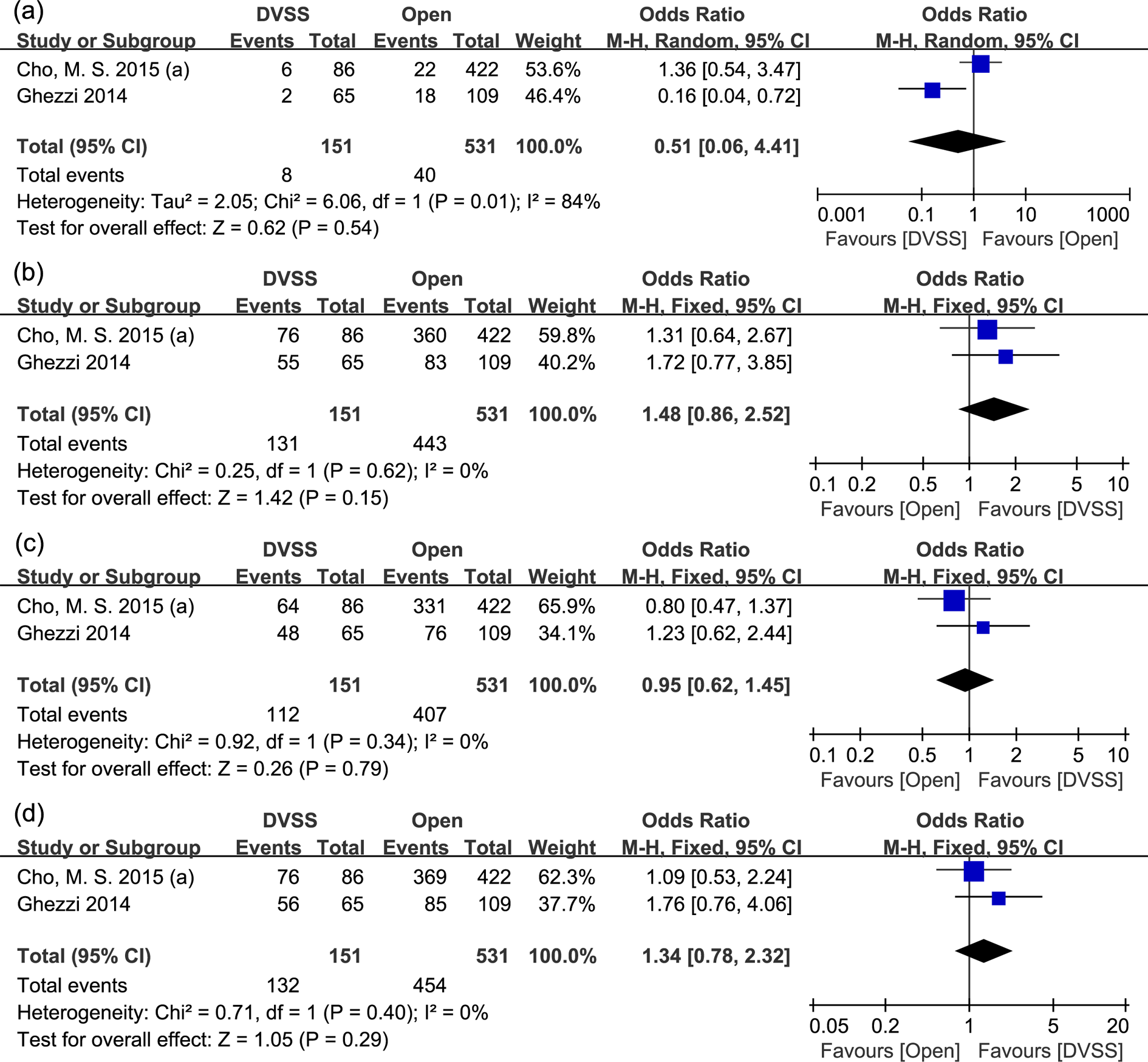
Forest plots of long-term oncologic outcomes between DVSS and open surgery. (a) 5-year LRR; (b) 5-year OS; (c) 5-year DFS; (d)5-year DSS. DVSS: Da Vinci surgical system; OS: overall survival; DFS: disease-free survival; LRR: local recurrence rate; DSS: disease-specific survival.
Secondary outcomes
Postoperative data
DVSS versus LS
In this comparison, three outcomes were involved including length of hospital stay, complications, and readmission. Fixed-effects model was used for all the outcomes (heterogeneity: p > 0.05, I2 < 55%) except for the length of hospital stay (heterogeneity: p = 0.04, I2 = 55%), which used a random-effects model. The combined result indicated that DVSS had a significantly reduced length of hospital stay compared with LS (WMD = −1.14, 95% CI: −1.69 to −0.58, p < 0.01, Figure 4(a)). With regard to the other two outcomes, the results were comparable between two groups (p > 0.05, Figure 4(b) and (c)). For each outcome evaluation, there was no obvious publication bias (Egger’s test: p > 0.05).

Forest plots of postoperative data between DVSS and LS/open surgery. (a) length of hospital stay (DVSS vs. LS); (b) complications (DVSS vs. LS); (c) readmission (DVSS vs. LS); (d) length of hospital stay (DVSS vs. open surgery); (e) complications (DVSS vs. open surgery). DVSS: Da Vinci surgical system; LS: laparoscopic surgery.
DVSS versus open surgery
In this comparison, two outcomes, length of hospital stay, and complications, were involved. A random-effects model was used for length of hospital stay calculation (heterogeneity: p = 0.01, I2 = 55%), while a fixed-effects model was used for complications (heterogeneity: p = 0.41, I2 = 0%). As expected, DVSS obtained a lower length of hospital stay than open surgery (WMD = −3.98, 95% CI: −6.12 to −1.84, p = 0.0003, Figure 4(d)). On the contrary, difference between the two groups was not significant with regard to complications (OR = 0.77, 95% CI: 0.54 to 1.09, p = 0.14, Figure 4(e)).
Operative data
DVSS versus LS
Four outcomes were contained in this comparison, including operation time, EBL, conversion to open surgery, and protective stoma. Random-effects model was applied for operation time (heterogeneity: p < 0.01, I2 = 90%) and EBL (heterogeneity: p = 0.44, I2 = 55%), whereas fixed-effects model was used for the other two outcomes (heterogeneity: p > 0.05). The pooled results indicated that compared with LS, although DVSS achieved a significant longer operation time (WMD = 35.48, 95% CI: 6.04 to 64.92, p = 0.02, Figure 5(a)), the EBL (WMD = −19.50, 95% CI: −34.47 to −4.53, p = 0.01, Figure 5(b)), and conversion to open surgery (OR = 0.19, 95% CI: 0.08 to 0.48, p = 0.0004, Figure 5(c)) were significantly reduced. Meanwhile, difference on the outcome of protective stoma was not obvious (p > 0.05, Figure 5(d)). No significant publication bias was detected for all of these outcomes (Egger’s test: p > 0.05).

Forest plots of operative data between DVSS and LS/open surgery. (a) operation time (DVSS vs. LS); (b) estimated blood loss (DVSS vs. LS); (c) conversion to open surgery (DVSS vs. LS); (d) protective stoma (DVSS vs. LS); (e) operation time (DVSS vs. open surgery); (f) estimated blood loss (DVSS vs. open surgery). DVSS: Da Vinci surgical system; LS: laparoscopic surgery.
DVSS versus open surgery
Operation time and EBL were involved in this comparison, and the former used a random-effects model (heterogeneity: p = 0.02, I2 = 82%), while the latter applied a fixed-effects model (heterogeneity: p = 0.87, I2 = 0%). Likewise, DVSS also achieved a significant longer operation time (WMD = 74.97, 95% CI: 41.29 to 108.66, p < 0.001, Figure 5(e)) but a lower EBL (WMD = −146.17, 95% CI: −191.21 to −101.13, p < 0.001, Figure 5(f)) than open surgery.
Subgroup analyses
In the comparison of DVSS versus LS, subgroup analysis stratified by CRC types, colon cancer and rectal adenocarcinoma, was performed, and the long-term oncologic outcomes, postoperative data, and operative data were evaluated in these two groups, respectively.
For the outcome of length of hospital stay, DVSS was obviously advantageous than LS in both rectal adenocarcinoma (WMD = −1.25, 95% CI: −2.03 to −0.47, p = 0.002) and colon cancer (WMD = −0.89, 95% CI: −1.71 to −0.07, p = 0.03) subgroups (Figure 6(a)).

Forest plots of operative data between DVSS and LS in colon cancer and rectal adenocarcinoma subgroups. (a) length of hospital stay; (b) conversion to open surgery; (c) operation time. DVSS: Da Vinci surgical system; LS: laparoscopic surgery.
With regard to the outcome of conversion to open surgery, DVSS achieved a better result than LS in rectal adenocarcinoma subgroup (OR = 0.17, 95% CI: 0.06 to 0.46, p = 0.0005), but a comparable result with LS in colon cancer (p > 0.05) subgroup (Figure 6(b)).
For operation time, DVSS took a longer time than LS in colon cancer subgroup (WMD = 37.79, 95% CI: 19.35 to 56.22, p < 0.001, Figure 6(c)). However, in rectal adenocarcinoma subgroup, there were no significant differences between these two approaches (p 0.05, Figure 6(c)).
With regard to the other outcomes, there were no significant differences between DVSS and LS in both of the subgroups (p > 0.05).
Sensitive analysis
For all outcomes in the comparison of DVSS versus LS, there did not present any reverse result after eliminating any study, suggesting a reliability of this meta-analysis (data not shown).
Discussion
In the present meta-analysis, we included a total of 10 studies, and the pooled results indicated that there were no significant differences between DVSS and LS/open surgery, in the aspects of long-term oncologic outcomes. However, DVSS achieved a significantly lower length of hospital stay and EBL, but a longer operation time, than LS/open surgery. In addition, DVSS showed a significantly reduced conversion to open surgery, compared with LS. Subgroup analysis suggested that DVSS reduced the length of hospital stay in both rectal adenocarcinoma and colon cancer subgroups; however, results on outcomes of conversion to open surgery and operation time were different in these two subgroups. Previously, a systematic review of RCTs indicates that for CRC treatment, long-term outcomes of LS are similar to open surgery, such as incisional hernias occurrence and reoperations for adhesions (p > 0.05). 26 However, studies that involve comparisons of these outcomes between DVSS and LS/open surgery are limited or the data are unavailable. A study compares the efficiency of robotic assisted and the standard LS for the treatment of rectal cancer and finds that there is no significant difference on 3- and 5-year LRR between two methods. 27 In addition, for rectal cancer, no significant differences were observed in 5-year OS (92.8% vs. 93.5%, p = 0.829) and DFS (81.9% vs. 78.7%, p = 0.547) as well as LRRs (2.3% vs. 1.2%, p = 0.649) between robotic and LS operations. 22 In the present study, we included the eligible studies as possible as we can and divided them into different comparisons (DVSS vs. LS; DVSS vs. open surgery). The pooled results suggested that there were no significant differences between DVSS and LS/open surgery on local recurrence, OS, and DSS, suggesting that from the long-term perspective, effects of DVSS might be similar to the conventional LS or open surgery. With regard to the operative data, consistent with our results, a previous meta-analysis found that DVSS took a significant 39 min longer surgery time than conventional LS for colorectal resection (MD = 39.42, 95% CI: 14.99 to 63.84). 7 Likewise, another study confirms the increased operative time using DVSS, compared with open surgery. 28 Having the computer-assisted robotic arms, DVSS device allows the operation on body with a very small incision, 29 which enables more precise dissection than conventional LS, 30 and this might be the reason it needs a longer operation time. The practical disadvantage that DVSS needs two surgeons might be another causative factor for the longer time, because it spends more time for the tacit cooperation between the one working at the operative table and the other from the console. 31
Although DVSS prolongs the surgery time compared with LS or open surgery, it has several beneficial effects for patients. In rectal carcinoma, a meta-analysis indicates that the convention to open rate is lower for robotic assistance than the traditional LS (OR = 0.31, 95% CI: 0.12 to 0.78), which is consistent with our results in rectal adenocarcinoma subgroup (OR = 0.17, 95% CI: 0.06 to 0.46), but the EBL is not different between the two approaches. 32 This result seems inconsistent with our findings, however, we should note that in Ortiz-Oshiro’s study, there were only two authors who reported the relevant data regarding EBL, 32 which might cause publication bias. Boggi et al. provide positive evidence that laparoscopic robot-assisted total pancreatectomies significantly reduce the mean blood loss compared with open total pancreatectomies (220 vs. 705 mL, p = 0.004). 33 Likewise, another study finds that the median EBL is significantly lower in comparison with that of minimally invasive (including laparoscopic-assisted vaginal, total laparoscopic or DVSS hysterectomy) versus open endometrial cancer staging procedures (100 vs. 300 mL, p < 0.0001). 34 Moreover, Yu et al. show that DVSS is significantly associated with lower length of hospital stay and blood loss than open surgery and LS. 28 In our subgroup analysis, DVSS achieved a shorter length of hospital stay in both rectal adenocarcinoma and colon cancer subgroups. These collectively support the advantages of DVSS than LS or open surgery.
Subgroup analysis indicated that DVSS significantly reduced conversion to open surgery in rectal adenocarcinoma subgroup but not in colon cancer and DVSS had a significant longer operation time than LS in colon cancer but not in rectal adenocarcinoma. These suggested that CRC type might be a causative factor for heterogeneity.
Despite the fact that we performed a comprehensive meta-analysis involving numerous outcomes, and the sensitive analysis indicated a relative precise result, several limitations remained. First, significant heterogeneity was detected for evaluation of several outcomes such as operation time, length of hospital stay, and EBL, which might cause deviation of the true results to some extent. The heterogeneity might derive from the inevitable factors, such as different operation level between different surgeons, varying health care level in different regions, and different disease severe degree of the enrolled patients. Second, as aforementioned, our major concern was long-term outcomes. Although several short-term outcomes in the included studies were also taken into consideration, we did not use “short-term outcomes” as a key search term from the initial retrieve. Thereby, potential eligible studies with regard to short-term outcomes might be missed. Third, the sample size was still small and more RCTs with large-scale patients are needed to provide potent evidence of our findings.
In conclusion, DVSS is superior to LS or open surgery in control of length of hospital stay and EBL but needs longer operation time. However, from long-term perspective, DVSS has an equivalent effect to the other two techniques. CRC type might be a factor for heterogeneity. More RCTs with large amount of samples are required to confirm our results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.