
Abstract
This research proposes a unique cable-driven two-degree-of-freedom wrist exoskeleton robotic device for Range of Motion (ROM) exercises related to Carpal Tunnel Recovery (CTR). A transportable platform for hand support powered by two actuators and a nonwearable sensing system comprised the basic, user-friendly design of the proposed exoskeleton robotic device. A specialized assist-as-needed control was installed to make the necessary movements with the robotic device. Transferring the data to the exoskeleton for rehabilitation, the control approach was combined with a computer vision system that imitated the therapist's wrist motions. Utilizing a computer algorithm, hand landmarks were produced to mimic the therapist's wrist movements. A total of 20 participants (Male: 55 % and Female: 45 %) were involved in the experimental procedure. High-accuracy ROM readings were obtained: 87.5 % for flexion, 90.0 % for extension, 92.5 % for ulnar deviation, and 90.0 % for radial deviation. In the conventional method, the healthy persons have a ROM for wrist flexion and extension of 71.6° and 63.0°, respectively, but Carpal Tunnel Syndrome (CTS) patients have a reduced ROM of 49.4° and 38.9°. Healthy participants have ulnar and radial deviations of 45.6° and 27.0°, respectively, while CTS patients have lower values of 28.7° and 20.1°. Using an exoskeleton, healthy people exhibit ROM flexion and extension of 64.9° and 59.0°, compared to 42.9° and 34.5° in CTS patients. This pattern is also shown in the ulnar and radial deviations, which are 44.1° and 25.6° for healthy individuals and 27.1° and 18.9° for CTS patients, respectively. These findings demonstrated the validity of the measurement techniques, which is crucial for clinical evaluations and rehabilitation plans.
Introduction
One of the most common musculoskeletal conditions, Carpal Tunnel Syndrome, also known as CTS, affects millions of individuals globally. CTS is characterized by numbness, tingling, and pain in the hand and arm. It is brought on by compression of the median nerve as it passes through the wrist's carpal tunnel. 1 Repetitive hand and wrist motions, typical in some daily activities and vocations, are linked to the syndrome. The demand for efficient rehabilitation and therapy strategies to reduce symptoms and regain hand function is growing along with the incidence of CTS.
Conservative measures, including rest, splinting, and anti-inflammatory drugs, are among the traditional therapies for CTS. More invasive techniques include corticosteroid injections and surgical carpal tunnel release. 2 Although these therapies have the potential to be beneficial, they frequently have drawbacks and possible consequences. Conservative therapies might only offer short-term respite, while surgical procedures come with dangers such as nerve injury, infection, and extended recovery periods. Furthermore, although postsurgical rehabilitation can be resource-intensive and frequently lacks standardization, it is essential for restoring complete function.
Physical therapy is the basis of nonoperative and postoperative treatments for CTS. It is expected to include exercises meant to boost wrist strength, flexibility, and generality of hand performance. 3 Nevertheless, it becomes a problem for patients to adhere to the required exercise patterns, and the success of these exercises depends mainly on the precise implementation of movements. For this reason, there are opportunities for rehabilitation enhancement through technological advancements, particularly in the robotics industry.
Recently, much interest has been in robotic-assisted rehabilitation, particularly for illnesses demanding precise and repetitive movements. Particularly, wrist exoskeletons are becoming increasingly popular as cutting-edge treatments for various hand and wrist conditions, including CTS. These tools ensure that exercises are done correctly and consistently by supporting, guiding, and augmenting wrist movements. Wrist exoskeletons can customize rehabilitation programs to meet the needs of individual patients by offering real-time feedback and customizable resistance levels. This could improve results and speed up recovery. 4
Comparing wrist exoskeletons to conventional rehabilitation techniques reveals several benefits. By improving wrist workouts’ accuracy and consistency, they can guarantee that patients execute actions accurately and effectively. This is especially significant during CTS therapy, as using the correct method prevents more nerve compression and accelerates the healing process. These devices can provide personalized rehabilitation protocols, which can be configured to modify the difficulty level based on the patient's progress. Rehab success depends on patient motivation and participation, which may be maintained with this individualized approach. Wrist exoskeletons can also help with remote rehabilitation, enabling patients to work out at home under the supervision of medical experts. Given the rising healthcare expenses and the demand for readily available rehabilitative treatments, this capacity is highly beneficial. Wrist exoskeletons can also reduce overall healthcare costs by minimizing the need for frequent in-person visits and improving rehabilitation accessibility for a larger population.5,6,7
Even though wrist exoskeletons show great promise for CTS rehabilitation, there is still a significant research void in this field. Although the use of robotic devices for general wrist rehabilitation has been the subject of numerous research, few specifically address CTS. Passive exercises under therapist guidance have received little attention in most wrist exoskeleton research, concentrating on improving active ROM exercises. Furthermore, rather than focusing on supervised, noninvasive techniques for mimicking therapist movements during ROM exercise, some research has focused on developing exoskeleton devices to aid with wrist flexion and extensions. In addition to flexion and extension, exoskeleton devices that can track ROM movements, such as ulnar and radial deviation are required. Since precise therapist tracking is essential for successful passive ROM exercises, developing these systems is difficult.
This research aims to close the current research gap by methodically assessing the efficacy of wrist exoskeleton robot-assisted passive exercises in optimizing rehabilitation for individuals with CTS. It seeks to create a robot exoskeleton tool for ROM exercises and evaluate the improvement of hand function and symptoms. Another study goal is to develop and validate standardized protocols for integrating wrist exoskeletons into preexisting CTS treatment frameworks. This research will aid in the creation of more efficient, approachable, and patient-centered rehabilitation techniques for CTS by defining precise standards and parameters for their application.
The rest of this paper is structured as follows: The existing methods and approaches currently used for exoskeleton-based CTS therapy are covered in the “Literature review” section. The development of the proposed exoskeleton robotic device and the data-gathering system is covered in the “Methodology” section. The analysis and findings are shown in the “Results and analysis” section. In the “Conclusion” section, the authors conclude the research with future directions.
Literature review
This section outlines the role of ROM in CTS rehabilitation, the use of robotic exoskeletons for rehabilitation, and the most recent studies in the field. Related studies were searched using IEEE Xplore, ScienceDirect, PubMed, Google Scholar, and other major academic databases. The scope of the review was limited to developments from the past five years (2019–2024), focusing on peer-reviewed conference papers, journal articles, book chapters, and other peer-reviewed materials.
Exercises involving ROM are essential for treating CTS, a condition in which the median nerve in the wrist is compressed. These movements improve wrist, finger, and forearm flexibility and mobility, which aids in function restoration, pain relief, and injury prevention. Passive ROM exercises, in which a therapist moves the patient's fingers and wrist to preserve joint flexibility and prevent stiffness, are frequently included in the early phases of rehabilitation. Active ROM exercises are offered to patients as their recovery advances to help them develop their strength and endurance. Exercises that stretch and glide the nerves are also helpful in relieving tension in the carpal tunnel and improving nerve mobility.8,9
A significant development in wrist rehabilitation is exoskeleton technology, which helps patients heal from operations, trauma, or neurological disorders. These tools improve strength, flexibility, and coordination by offering specific workouts, controlled resistance, and support. 10 They employ sensors and actuators for real-time feedback and modifications, ensuring precise and consistent therapy sessions—something traditional approaches might not provide. Integrating AI and machine learning makes personalized treatment planning and progress tracking possible. Despite obstacles such as cost and user adoption, research is still being done to increase affordability and usefulness.11,12
With their sophisticated, noninvasive techniques for tracking and directing healing, computer vision–enabled models are entirely changing the field of wrist rehabilitation. These models can quantify progress and spot discrepancies by capturing and analyzing wrist movements using cameras and depth sensors.13,14 Accurate feedback from this exact tracking increases patient motivation and enables more individualized treatment programs. Additionally, the technology facilitates remote rehabilitation, allowing patients to resume their activities at home while receiving real-time therapist feedback and supervision. 15 One such is BlazeHand, an interactive rehabilitation program that automates movement tracking and analysis and improves recovery timelines and outcomes by combining computer vision and machine learning.16,17
Several researchers in the field have engaged to provide solutions for the CTS using ROM and other exercising methods. Sustaining hand functionality is essential for day-to-day activities and overall well-being; diseases such as Duchenne muscular dystrophy can lead to disabilities. The goniometer is usually used to measure the ROM in the hands and wrists during rehabilitation. While less dependable than a goniometer, Nizamis et al.'s 18 evaluation of the Leap motion sensor's ability to detect active ROM showed promise for clinical applications. Eini et al. 19 evaluated the Camera Wrist Tracker when measuring wrist ROM in patients with distal radius fractures. They found that it had good reliability for extension and intermediate reliability for flexion.
Wrist exoskeletons assist in stroke and hand dysfunction rehab through high-intensity training but often fail to mimic natural movements. Zhang et al. 20 developed the HrWr-ExoSkeleton (HrWE) with bioelectronics and a hybrid design, enabling natural wrist motions and integration with other exoskeletons. Their platform, using surface electromyography signals, enhanced therapeutic outcomes. Jeong et al. 21 developed Soft Wrist Assist (SWA) using shape memory alloy to aid wrist motion. The SWA, lightweight and easy to apply, showed promising results in improving wrist mobility. Nikafrooz et al. 22 developed a cost-effective wrist rehab robot with three degrees of freedom (DOFs), aligning with anthropometric data to aid effective rehabilitation. Oblak et al. 23 introduced the Universal Haptic Drive for arm and wrist rehab, featuring ARM and WRIST modes and proportional force control. It proved reliable and repeatable in movement training. Soft exosuits can lessen worker fatigue and enhance motor abilities. A 3D-printed structure and cable-driven soft wrist exosuit were introduced by Chiaradia et al. 24 to improve comfort and force transfer. For loads up to 3 kg, it significantly reduced physical effort. A fabric pneumatic artificial muscle–powered wrist exosuit was introduced by Schäffer et al., 25 exhibiting controlled mobility along one and two DOFs. Its lightweight construction did not come without movement restrictions.
The demand for mobile exoskeletons has surged due to the rise in stroke sufferers. Prasad et al. 26 found a 4-cable design for rehabilitating the lower limbs in their simulation-based framework for cable-driven mobile exoskeletons. CADEN-7, a 7-DOF arm exoskeleton for everyday activities, was created by Perry et al. 27 Its design makes applications in virtual reality, therapy diagnostics, and rehabilitation possible. The portable forearm exoskeleton designed for rehabilitation and assistive purposes (FE.RAP) was introduced by Lee et al. 28 It uses a direct-drive mechanism to help with wrist movements and facilitate motion recovery for daily tasks. The CURER upper limb rehab exoskeleton was created by Qian et al. 29 and included modular actuators, VR training, and lightweight construction. It offered a broad ROM and regulated torque for efficient rehabilitation.
Ueki et al. 30 demonstrated a motion assistance robot with several DOFs as part of a VR-enhanced hand rehab system for flexion/extension and abduction/adduction, thumb opposability, and hand-wrist coordinated motions. The system with audiovisual VR instructions efficiently supported complex finger and thumb movements. In addition to stressing the benefits of exoskeleton-based stroke rehabilitation over conventional techniques, Frisoli 31 underlined important issues with upper limb exoskeleton design.
Robotic assistive devices have been helping people regain the function of their limbs for more than ten years. Ou et al.29,32 concentrated on developing a wearable exoskeleton to support bilateral task training and palm extension in hemiplegic stroke patients. The paralysis of the upper limb frequently requires caretaker support. Trotobas 33 concentrated on creating assistive orthoses and in-patient testing, and his hybrid hand and wrist orthosis showed promise. Future studies will focus on modular systems that combine orthoses and Functional Electrical Stimulation to provide flexible options. Numbness and pain may result from the palmar carpal ligament's pressure on the median nerve, which can enlarge. Most remedies are passive, such as braces. Zhu et al. 34 proposed a wearable, soft robotic sleeve that modifies wrist position to relieve CTS stresses in real-time.
With the tremendous progress of exoskeleton technology and the urgent need for efficient rehabilitation methods, this study attempts to maximize wrist exoskeleton robot-assisted exercises for carpal tunnel healing. Moreover, this aims to improve carpal tunnel therapy's accuracy, efficacy, and user experience by utilizing the most recent advancements in exoskeleton design and incorporating cutting-edge measurement techniques. There are still several shortcomings in optimizing carpal tunnel healing, even with the advances in wrist exoskeletons and rehabilitation technologies. Although some technologies, such as the HrWE, SWA, and several soft exosuits, have shown encouraging outcomes, more all-encompassing and patient-specific solutions that are easy to incorporate into regular rehabilitation practices are required. Many exoskeletons on the market now concentrate on general wrist and hand rehabilitation rather than addressing the particular difficulties brought on by CTS.
According to the current study, studies on the long-term effectiveness and patient adherence to exoskeleton-assisted therapy for CTS are still being determined. While most research assesses the short-term therapeutic results, there is a dearth of information regarding these solutions’ long-term viability and applicability in real-world contexts. Furthermore, there is a need for readily available, reasonably priced solutions that may be extensively used in various home and hospital settings.
This research seeks to close these gaps by creating a wrist exoskeleton tailored for carpal tunnel healing. Furthermore, it aims to improve the effectiveness and productivity of rehabilitation exercises by incorporating exoskeleton-enabled robotics. These devices include advanced assessment tools that help enhance natural wrist movements. The research seeks to close these gaps and offer a holistic, patient-centered approach to carpal tunnel rehabilitation optimization.
Methodology
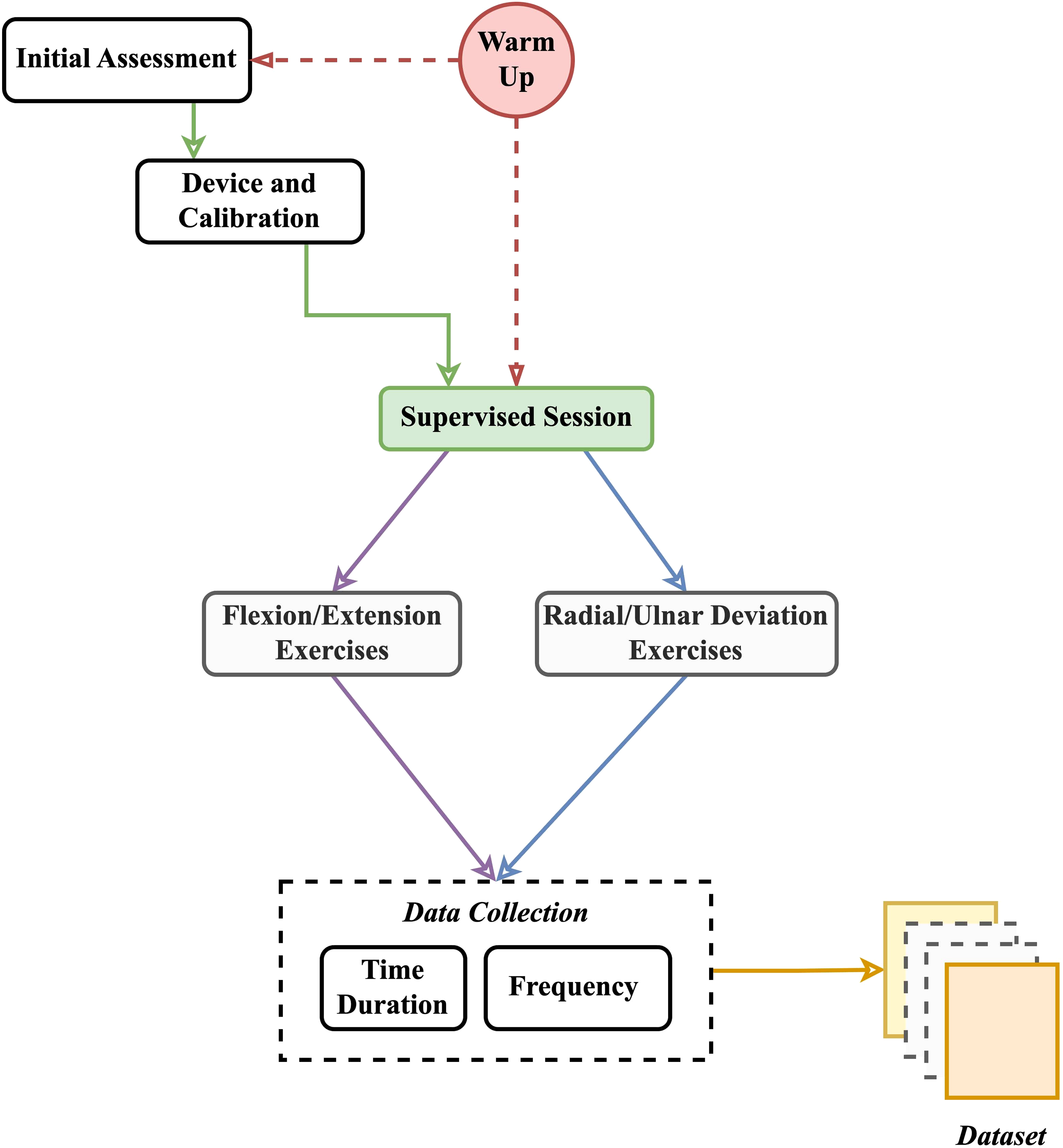
Several vital components came together to form the overall design of the proposed methodology, which allowed for effective wrist rehabilitation using an exoskeleton robot. The main parts utilized to simulate the exoskeleton system were wrist angle computation, angle communication to the controller, control wires, and therapist's hand movement detection. Each component was essential for the exoskeleton to guide the wrist precisely during its ROM exercises. Figure 1 shows the overall block diagram of the proposed exoskeleton robot system.

The architecture of the overall system.
Hand movement recognition was accomplished using advanced computer vision algorithms to comprehend the therapist's hand movements, ensuring accurate exoskeleton response. Afterward, the wrist angle calculation model used real-time processing to convert these motions into accurate wrist angles, providing secure and effective movements. In both natural and assisted rehabilitation scenarios, the exoskeleton's controller required prompt receipt of the computed angles. The controller instructed the motors to match the therapist's anticipated movements. Ultimately, control cables converted the impulses from the controller into actual motions. Therefore, their construction had to be exact and robust to ensure dependability. These components produced a well-working system that precision-guided the wrist through ROM exercises, facilitating wrist rehabilitation.
Mechanical design and dynamics
The goal of the cable-driven robot was to operate n DOFs with at least n+1 up to 2n cables, enabling the wires to respond to outside influences. The exoskeleton robot's workspace was constrained because the wires could only pull in the same direction. The relative positions of each cable attachment shifted as the cable pulled the limb to move, reducing workspace and altering tension efficiency while raising parasitic force.
Wires connected to two motors supply the force needed to move the CTS patient's wrist in the system. This cable-driven exoskeleton robotic device used four separate cables to provide two DOF movements. The motors were carefully selected and installed to simplify a range of wrist exercises and therapy routines. The robotic device's 30° to 80° flexion range offered plenty of flexibility for strengthening and rehabilitation workouts. The ROM supported for extension movements was 30° to 75°, which provided complete coverage of wrist motion in both forward and backward directions. With a movement range of 15° to 30°, the robotic device also allowed for radial deviation, which is helpful for activities that require moving the wrist toward the thumb.
Similarly, a 25° to 50° range supported ulnar deviation, which permitted the wrist to move toward the little finger. The exoskeleton robot's intricate design was developed to guarantee it can efficiently address therapeutic requirements while improving the user's wrist flexibility and strength. The exoskeleton robotic device was a flexible tool for physical treatment and recovery because it combines the precise control of the motors with the thoughtful arrangement of the wires to provide a complete solution for wrist rehabilitation.
The system used cables to actuate the hand, making it nonback-drivable. The wires were attached to the hand via a comfortably padded hand brace with a quick-release latch for easy emergency removal. Figure 2 shows the physical view of the exoskeleton robotic device. The setup demonstrated the wrist's secure yet easily adjustable attachment to the platform, facilitating efficient motion and manipulation.

Configuration of wrist placed on the moving platform with quick-release latch.
Cables run from the brace to the control box containing the two motors, positioned behind the user on the same side as the treated hand. The construction of the cable control mechanism is shown in Figure 3(a). The cables C1, C2, C3, and C4 are oppositely wound to achieve motion. C1 and C2 are wound clockwise and counterclockwise on separate slots in the same pulley, as are C3 and C4. This configuration allows for easy extension and contraction of the cables.
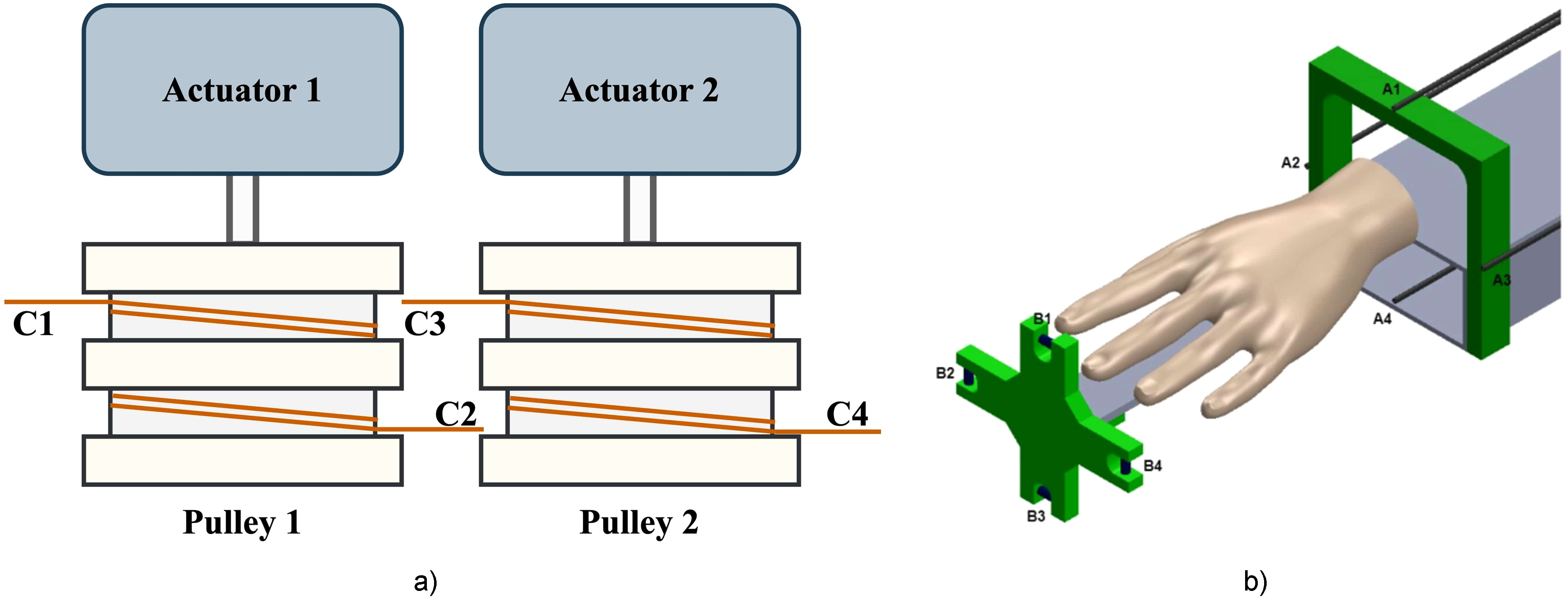
(a) The schematic of the cable drive system, (b) The exploded view of the robot: A1–A4 are four cable attachments of the forearm module, and B1–B4 are four cable attachments of the hand holder.
When the system was in operation, the power source motor continually rotated the gear motors. These geared motors disperse the mechanical power needed to create the necessary force in the wires by directly connecting to the cable reel. Different stresses were produced by the four cables connected to the four cable attachments B1−B4 on the hand holder through A1−A4 on the four extension arms (Figure 3(b)).
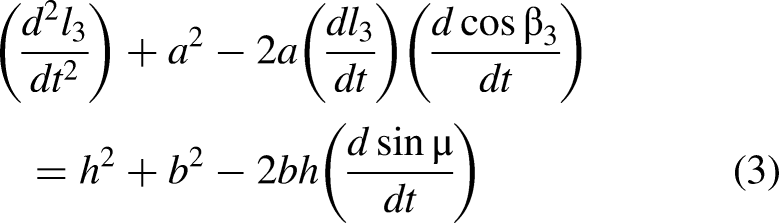
The dynamic representation of the radial deviation and ulnar deviation motion (horizontal plane) is shown in Figure 4(a), with l1 and l2 representing the lengths of the cables C1 and C2. The dynamic representation of the flexion and extension motion (vertical plane) is shown in Figure 4(b), with l3 and l4 representing the lengths of the cables C3 and C4.

(a) Dynamic representation of radial deviation and ulnar deviation motion on a transverse plane, (b) Dynamic representation of the flexion and extension motion on a sagittal plane.
According to the above schematic, the mathematical model for horizontal motion is described as equations (1) and (2):


Wrist motion tracking and control system
The therapist's wrist motion tracking and exoskeleton control system is an essential part of the exoskeleton robot for wrist rehabilitation, which is intended to aid in healing CTS via ROM exercises. This robotic device incorporated cutting-edge technologies to precisely monitor the therapist's wrist movements and support CTS patients for successful rehabilitation. Wrist motion tracking and closed-loop motor control are the two main phases of the motion control system's operation.
The MediaPipe hand movement recognition algorithm was used in the first stage to recognize hand movements from the therapist. With the origin at the geometric center of the hand, this advanced model finds 21 landmark spots on the wrist, each represented by x, y, and z-coordinates in actual 3D space (see the architecture of the MediaPipe hand model in Figure 5). The landmarks are essential for determining the plane of motion and wrist angles. In particular, wrist angles were calculated using the coordinates of landmarks 0 and 12, and the plane of motion was chosen with the aid of the landmark point's z-coordinate. Precise tracking of flexion, extension, radial deviation, and ulnar deviation was ensured by the accuracy of the MediaPipe model, which is necessary for focused rehabilitation programs.

The MediaPipe model (a) human hand skeleton view, (b) MediaPipe hand landmarks model, and (c) Architecture of the MediaPipe hand, adapted from Google Research. 35
The process for determining wrist angles of therapists for efficient therapy in the healing of CTS is shown in Figure 6. It comprises measuring the radial and ulnar deviation using the vertical axis angle (θ) (see Figure 6(a)), measuring the flexion and extension using the horizontal axis angle (μ) (see Figure 6(b)), and discussing the geometric principles involved in these calculations (see Figure 6(c)). While the μ examined flexion and extension by comparable slope calculations in the vertical plane, the θ assessed ulnar and radial deviations by calculating the slope between important wrist landmarks in the horizontal plane. Both measurements relied on vector geometry and exact trigonometric relationships for accurate wrist movement monitoring and control. With the help of this exacting process, the exoskeleton could precisely modify cable tensions, allowing the wrist to move through its prescribed ROM for the best possible rehabilitation.

(a) Therapist's vertical axis angle (θ) measurement (radial deviation and ulnar deviation), (b) Horizontal axis angle (μ) measurement (flexion and extension), and (c) Methodology of the angle calculation geometry.
The angle line, with a slope m, is represented by the equation
Next, the magnitudes of these vectors were determined. The magnitude of the vertical vector is
A similar method was applied to flexion and extension, which take place in the vertical plane. The main differences lie between the direction vectors and the reference line orientation. The system must consider the wrist's rotation along with an additional axis for these movements, but the basic ideas of magnitude determination, vector dot products, and slope calculation stay the same.
A serial connection was then used to transmit the exact angle data of the exoskeleton's control system. Using this data, the control system modified the tension in the wires that propel the wrist's movement. To ensure that the wrist gets to the proper position, the control system, for example, will increase the tension in the cables responsible for flexion if the computed angle indicates that further flexion is required. On the other hand, the system will modify the cable tension to achieve the desired amount of flexion or extension. Moreover, a six-axis motion tracking sensor (MPU-6050) built into the closed-loop control system continuously tracks the location and movement of the user's wrist. Because of this sensor's real-time feedback, the control system was developed to change the wrist holder's position quickly. This feedback loop was essential to retain precise and responsive control and guaranteed that the wrist movements corresponded precisely with the targeted ROM exercises.
A closed-loop control system guarantees precise tracking and adjustment of the user's wrist movements for the wrist rehabilitation exoskeleton robot systems. To determine the transfer function of the system, we utilized the feedback sensor (H(s)), the controller (C(s)), and the plant or exoskeleton mechanism (P(s)). Figure 7 shows the architecture of the closed-loop control system of the exoskeleton robotic device.

The architecture of the control system.
The transfer function of the system is shown in equation (5):



Transient response for step unit with PID controller.
The following metrics were obtained from the transient response analysis: a rise time of 0.19 s, representing the time needed for the system's output to climb from 10 % to 90 % of the ultimate steady-state value. This suggests that the system responded to changes in input rather quickly. The system settled rather rapidly, as evidenced by the 1.26-s settling time—the time needed for the output to stay within 2–5 % of the final steady-state value following a disturbance or step input. The system's transient response peak value exceeded the final steady-state value by 11.4 %, resulting in a percentage overrun of 11.4 %. According to the total closed-loop stability study, the tuned PID controller ensured system stability.
Experimental procedure and data collection
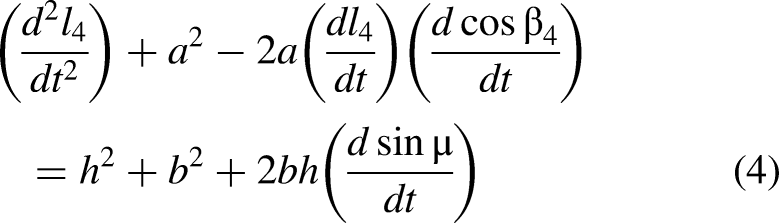
By combining sophisticated hand movement recognition, accurate control systems, and extensive data collection, the research aims to close the research gap and provide solid evidence for the advantages of exoskeleton robotic devices for rehabilitation therapy in CTS management. This experimental procedure outlined a systematic approach to evaluating the effectiveness of wrist exoskeleton robot-assisted passive exercises in optimizing CTR. Figure 9 shows the proposed experimental and data collection procedure.
Experimental procedure and data collection methodology.
The initial step in the experimental process was to find volunteers diagnosed with CTS. To guarantee that the study is relevant and practical, these individuals were chosen by predetermined inclusion criteria. Data on age, gender, height, weight, Body Mass Index (BMI), and grip strength were gathered during the initial data collection.
The second step included a thorough baseline evaluation of each participant's wrist functionality. This examination used standardized equipment (grip dynamometer, goniometer) to gauge the wrist's strength, ROM, and intensity of CTS symptoms. These assessments were a benchmark for assessing how well the passive exercises using an exoskeleton work. After the baseline examination, the exoskeleton robotic device was calibrated to each participant's unique wrist size and ROM. Calibration was essential for the device to function correctly and offer the proper support during the exercises.
The third step involved a regular warm-up regimen performed at the start of each session to prime the wrist for upcoming movements, minimize injury risk, and improve performance. The supervised exercise sessions concentrate on particular wrist movements, such as the exercises for flexion and extension and radial and ulnar deviation. The same therapist worked with all individuals throughout data collection to maintain consistency in wrist rehabilitation therapy and exercise routines.
Results and analysis
The primary objective of this research is to gather and compare wrist ROM measurements for flexion, extension, radial, and ulnar deviation between a group of participants with CTS and a healthy. A total of 20 participants (55 % of male and 45 % of female) were voluntarily involved in the experimental procedure. This section discusses the results and analysis of the proposed system to determine how CTS affects wrist functionality and mobility. Initially, the system captured the therapist's handwrist movements using a vision system, as shown in Figure 10.

Graphical user interface (GUI) of the vision-based wrist angle extraction system (left: angle variation of the ulnar and redial motion, right: angle variation of the extension and flexion motion).
Participants in the flexion and extension data collection held each position for 15 s, four times. Sensors recorded the actual wrist angle, and computer vision technology was used to measure the intended angle. This technique produced accurate wrist movement tracking and dependable analytical data. Figure 11(a) shows the control group's wrist flexion and extension variations. Participants were instructed to repeat the process four times, holding each position for 15 s for radial and ulnar deviation. A sensor was used to measure the actual wrist angle, and computer vision was used to estimate the ideal angle. This method made it possible to accurately compare the desired and actual wrist movements. Figure 11(b) demonstrates the variation of the control group's wrist radial and ulnar deviation.

(a) Wrist flexion and extension of the control group, and (b) Wrist radial and ulnar deviation of the control group.
Evaluation of the desired and actual wrist angle of a control and CTS participant during the flexion and extension movement is shown in Figure 12. As shown in Figure 12(a), the peak average wrist flexion and extension angle for the control group were 67.6° ± 3.8° and 59.3° ± 2.3°, respectively. As shown in Figure 12(b), the peak average wrist flexion angle of 43.3° ± 3.3° and extension angle of 36.4° ± 4.2° were substantially lower in the CTS group. The statistical analysis demonstrated that these differences were significant (p < 0.05), suggesting that wrist flexion and extension are limited in CTS patients relative to the control group. This decrease in ROM highlights how CTS affects joint mobility and raises the possibility of functional restrictions. Figure 12(c) and (d) shows a segment variation during a flexion cycle. As shown in the graphs, the CTS group significantly reduced ROM flexion. The same observation is visible for the extension movement for the control and CTS group.
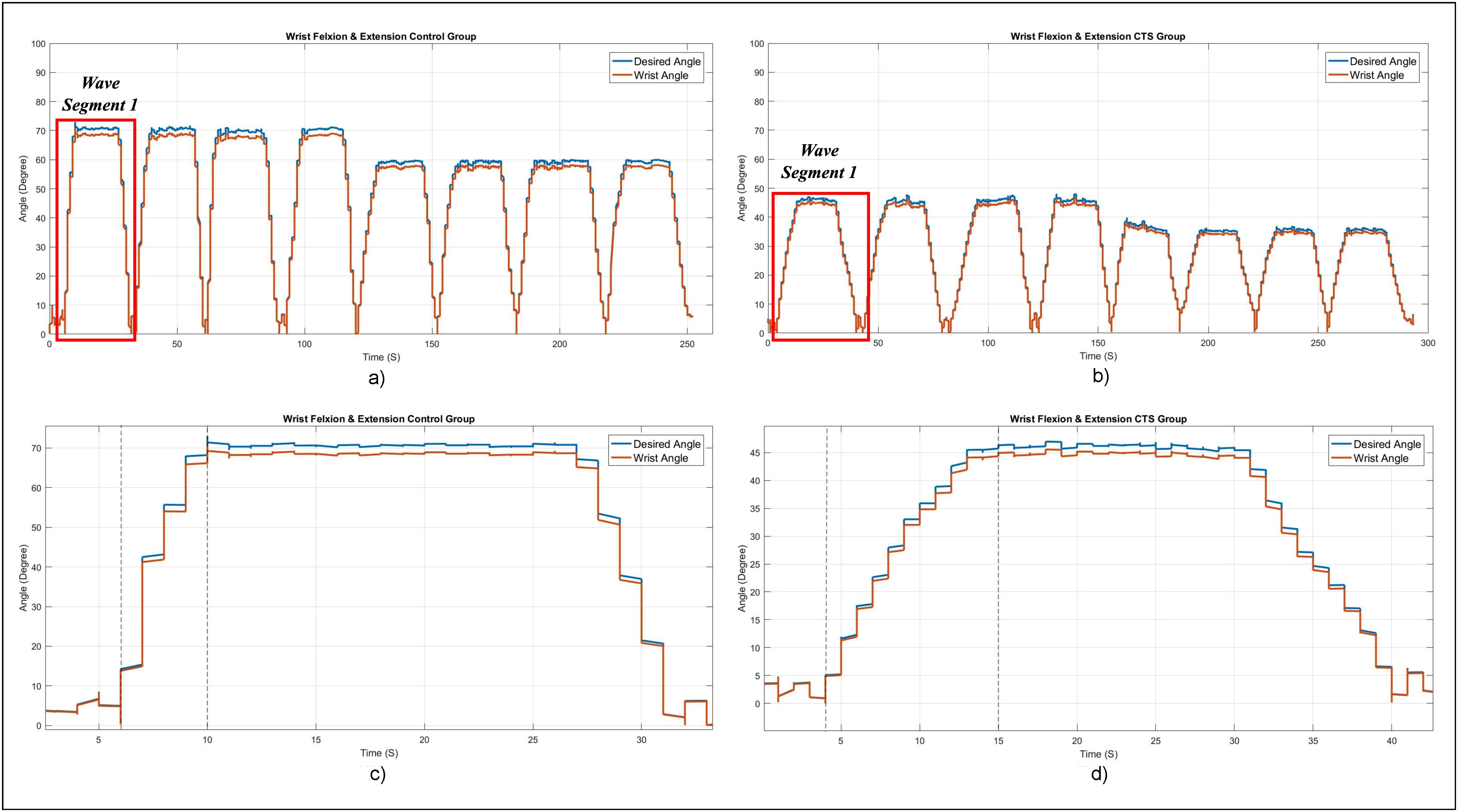
Variation of desired and actual wrist angle during flexion and extension of the (a) Entire exercise of the control group's test case, (b) Entire exercise of the CTS group's test case, (c) Expanded view of the first segment of the control group's test case, and (d) expanded view of the first wave segment of the CTS group's test case.
Figure 13 shows the variation of desired and actual wrist angles of the control and CTS group during ulnar and radial deviation movements. As shown in Figure 13(a), the peak average ulnar deviation and radial deviation angle of the control group were 44.7° ± 2.7° and 25.9° ± 2.1°, respectively. Figure 13(b) shows that the peak average ulnar deviation angle of 26.9° ± 3.2° and peak average radial deviation angle of 20.2° ± 2.8° were also considerably lower in the CTS group. The statistical significance of these discrepancies (p < 0.05) indicates that CTS limits wrist movement in the direction of the ulnar and radial sides. Individuals with CTS exhibit a restricted ROM, which exposes potential functional constraints and reflects the overall impact of the disorder on wrist mobility. These findings highlight the necessity for targeted treatment approaches to alleviate the movement limitations brought on by CTS. Figure 13(c) and (d) shows the control group's first-segment wave and the CTS group's fourth-wave segments during ulnar activity. As shown in the graph, a significant variation was observed in the CTS group, indicating that more therapy is required for recovery.
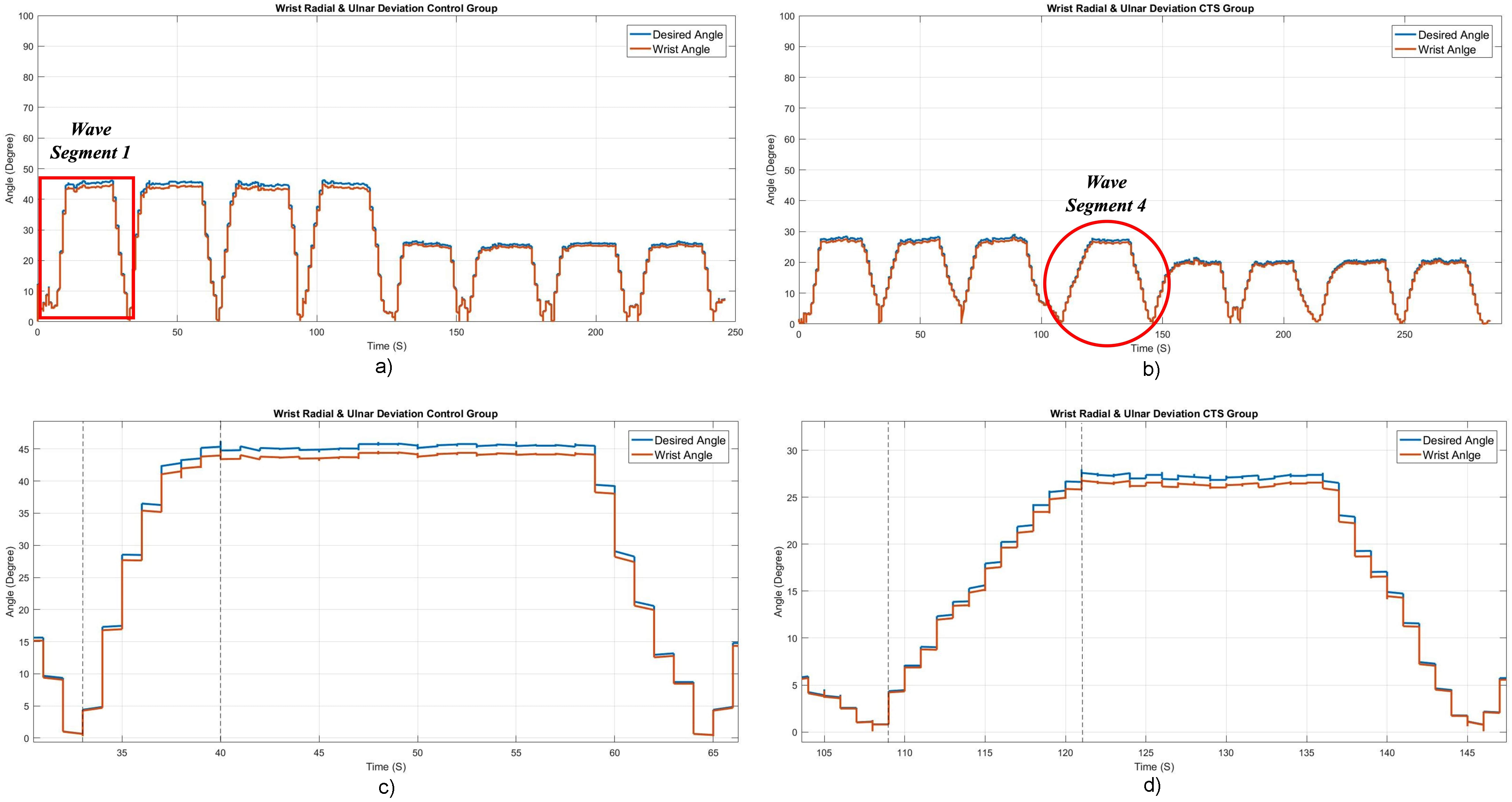
Variation of desired and actual wrist angle during wrist radial and ulnar deviation of the (a) Complete experiment of a control group test case, (b) Complete experiment of a CTS group test case, (c) Expanded view of the first segment of the control group experiment, and (d) Expanded view of the fourth segment of the CTS group experiment.
Figure 14 shows the speed variation during the ROM exercise for the control and CTS group. The data gathered showed significant variations in wrist ROM and movement speed between the CTS and control groups. The CTS group demonstrated decreased ROM and slower movement speeds, highlighting the effect of CTS on wrist functionality and mobility. These results emphasize the necessity of focused therapies to increase wrist mobility and lessen functional restrictions in CTS patients. The study's conclusions were made more valid by the precise and trustworthy measurements made possible by applying sensor and computer vision technologies. Despite the variations in the ROM, examining time-based graphs provided additional evidence for the consistency of wrist movements in the two groups. Overall, the study offers insightful information about how CTS affects wrist mobility and the possibility of using robot-assisted exercises to help affected people recover and regain better wrist function.

Speed variation during the complete experiment of a test case from (a) Flexion and extension of the control group, (b) Flexion and extension of the CTS group, (c) Ulnar and radial of the control group, and (d) Ulnar and radial of the CTS group.
Table 1 summarizes the angle and speed variation during a ROM experiment using the exoskeleton device. The table indicates that the angle variation for ROM activity in the healthy group is more significant than in the CTS group. Notably, the speed of CTS is considerably slower than that observed in healthy individuals. The peak speed of flexion and extension of the control group was 39.3 °/s, while 16.8 °/s showed in the CTS group; 17.1 °/s were observed during the ulnar and radial activities in the control group, while 3.7 °/s were observed in the CTS group.
Average angle and speed variation during the ROM exercise using the exoskeleton device.

Table 2 shows a sample dataset of individuals grouped by age, gender, BMI, grip strength, and CTS status. Using a traditional and an exoskeleton method, it measured their ROM across four movements–flexion, extension, ulnar, and radial deviation. Participants range in age from 41 to 69 years, representing both men and women. Their BMI varies from 16.9 kg/m² to 34.9 kg/m², indicating different body compositions. Grip strength ranges from 2 kg to 30 kg, and the participants’ CTS status was labeled as CTS = 0 (healthy) and CTS = 1 (CTS patients).
Sample of experimental data for conventional method and exoskeleton method.
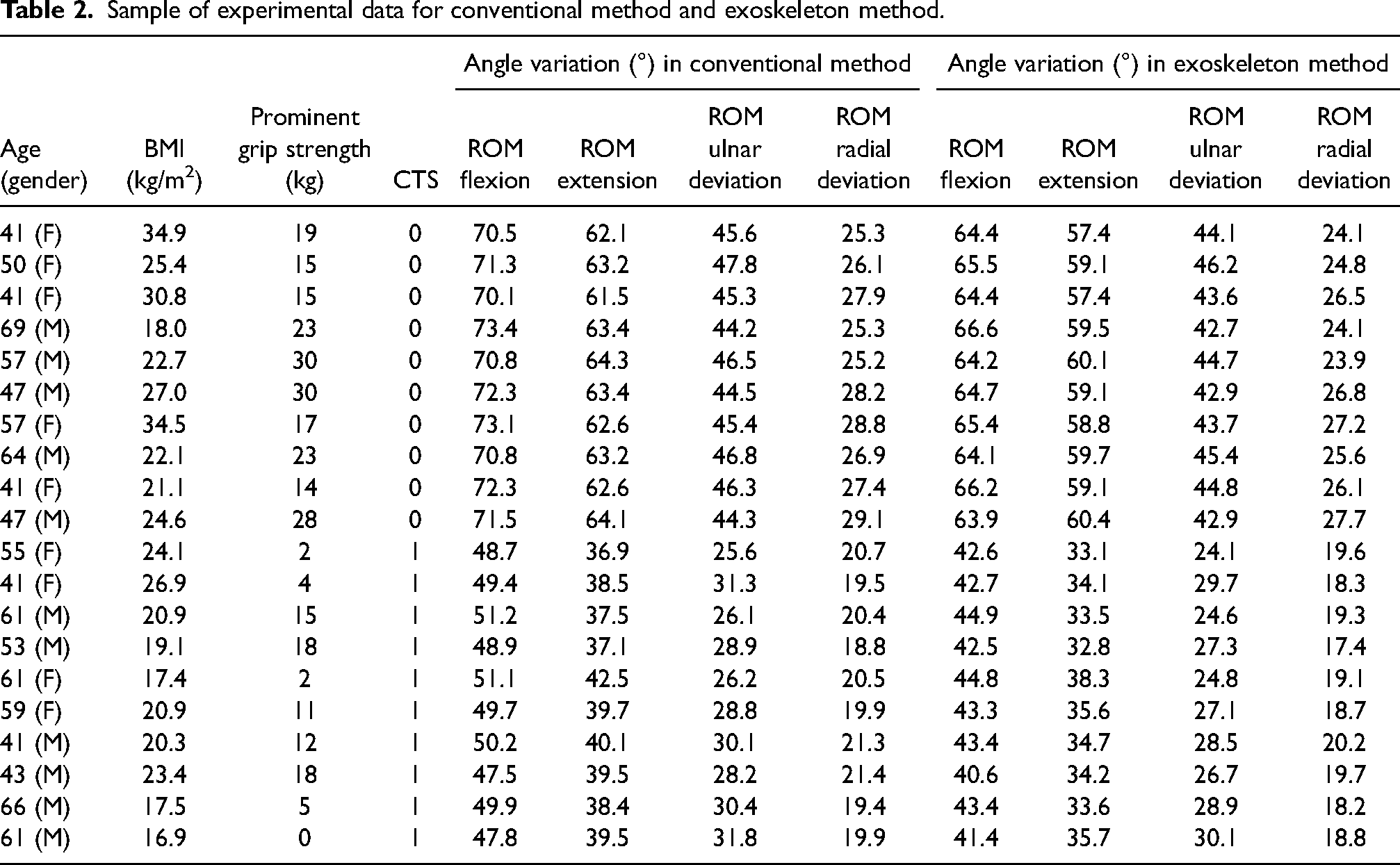
The table shows significant disparities in ROM measurements between the healthy group and CTS. In the conventional method, healthy participants have ROM flexion of 71.6° and extension of 63.0° in the wrist, but CTS sufferers have significantly lower values of 49.4° and 38.9°, respectively. Regarding ulnar deviation, healthy people have a 45.6° ROM, but CTS patients have 28.7°. Similarly, healthy persons have a radial deviation of 27.0°, compared to 20.1° in those with CTS. The exoskeleton robotic method confirmed this trend, with healthy persons having a ROM flexion of 64.9° and a ROM extension of 59.0°, against 42.9° and 34.5° in CTS sufferers. Furthermore, the ulnar deviation for healthy patients is 44.1°, compared to 27.1° for those with CTS, and the radial deviation readings are 25.6° and 18.9°, respectively. These results demonstrate the severe impact of CTS on wrist movement.
The exoskeleton method reduced stress on the wrist and surrounding tissues by restricting specific motions, particularly flexion and extension. This was crucial for rehabilitation or preventing the worsening of symptoms. The controlled constraints of the exoskeleton guarantee safe movement for patients recuperating from CTS or those with reduced wrist function, minimizing the chance of aggravating the condition. It was a valuable tool in therapeutic settings because it may restrict the full ROM. Still, the trade-off is a safer, more encouraging atmosphere for healing and long-term rehabilitation.
We measured the ROM for four critical activities in this study: flexion, extension, ulnar deviation, and radial deviation. As shown in Figure 15, the confusion matrix shows that the measurement methods were trustworthy and captured the ROM for every joint action. The 87.5 % ROM flexion accuracy reliably assessed the joint's bending capabilities. To be more precise, the ROM extension accuracy of 90.0 % demonstrates vital precision in determining the joint's straightening motion. The measurement's efficacy in capturing wrist movement toward the ulna is shown by its 92.5 % accuracy for ROM ulnar deviation, and its 90.0 % accuracy for ROM radial deviation validates a trustworthy evaluation of wrist movement toward the radius. The robustness of the techniques is demonstrated by the overall high accuracy of 90.89 %, which provides confidence in CTS rehabilitation through exoskeleton robotic devices using ROM exercises.

Confusion matrix of the experiment.
Conclusion
The study effectively shows that using robot-assisted exercises to improve CTR can significantly benefit from the revolutionary cable-driven 2-DOF wrist exoskeleton system. The device has proven to be a viable and dependable tool for wrist rehabilitation by mimicking healthy wrist motions and combining an intuitive design with sophisticated control strategies, such as computer vision algorithms and CTS exercises. The incredible accuracy of ROM measurements for different joint movements shows the device's potential in clinical examinations and rehabilitation regimens. Furthermore, the optimized PID controller guarantees the system's efficiency and stability, giving users’ confidence when using it for reliable and efficient wrist rehabilitation. The observations demonstrated the encouraging potential of advanced robotic technology in CTS sufferers’ therapy environments. The device worked well for rehabilitation because it increased wrist movement and accuracy. Its accurate measurements further validated its clinical applicability, suggesting that robotic systems may improve patient outcomes and rehabilitation plans. Subsequent efforts could concentrate on optimizing the apparatus, carrying out extended clinical studies, and investigating the incorporation of increasingly complex adaptive control systems to customize and improve the recuperation procedure.
Moreover, this study collected data and conducted experiments in a specific geographic area, namely Sri Lanka's Western Province. This localized strategy allowed for regulated and consistent data gathering within a well-defined population but may also present some restrictions. Future researchers who use this methodology may need to make changes, notably to the device's wobble angle settings, because ROM angles can vary between geographic regions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.