
Abstract
Cancer causes inflammation as it progresses through healthy tissue. The differentiation of tumoral growth from the surrounding inflammatory change is paramount in planning surgeries seeking to preserve function. This retrospective study aims at illustrating how a careful use of imaging (computed tomography (CT)/magnetic resonance imaging (MRI)) can help to draw the line between infiltration and inflammation. Out of 72 cases of parosteal osteosarcoma in our institution we selected 22 which had pretreatment imaging, and out of those, 14 that had both MRI and CT. Using Fisher’s exact test, we evaluated the performance of each technique on accurately diagnosing medullary tumor infiltration, using histological analysis as a gold standard. All cases (14/14) demonstrated medullary abnormality on MRI, but only 6/14 (42.9%) demonstrated abnormality on CT. The 8/14 cases with MRI abnormality but no CT abnormality (57.1%) showed inflammation with no tumoral cells present on histological analysis. In the cases where the two examinations showed medullary abnormality (6/14) histology demonstrated tumoral infiltration. MRI demonstrated high sensitivity and negative predictive value, but low specificity and low positive predictive value and accuracy (P=1). CT demonstrated high sensitivity, specificity, high positive and negative predictive values and accuracy (P = 0.000333). MRI is highly sensitive for the detection of medullary abnormality but lacks specificity for tumor invasion. Correlation with CT is recommended in all cases of positive MR to add specificity for tumors. The adequate use of the two imaging methods allows to differentiate between inflammatory change and tumoral infiltration in POS, relevant for surgical planning.
Keywords
Introduction
It is now an established concept that inflammation and cancer share a tight bond and are mutually inter-related. Virchow, in the middle of the 19th century, 1 had already observed that cancer appeared linked to chronic inflammation, based on the fact that some irritating substances cause tissue injury and therefore trigger a reparative or healing response. This response develops thanks to the recruitment of inflammatory cells, ultimately resulting in the enhancement of cell proliferation to repair the damaged tissue. 2
The microenvironment of tumors plays a very important role in the tumoral process, involved in cell proliferation, the survival of tumor cells as well as their migration. In some cases, the basis of the cancer generation resides in the chronic reparative status, with continuous cell proliferation in an environment rich in inflammatory cells and activated mediators (chemokines, cytokines), growth factors and degradation products and agents. These may cause DNA damage and result in the selection of certain lines of mutated cells that take advantage of this proliferative-inflammatory status and their methods of recruitment to thrive, to invade, to migrate and to metastasize. One of the features of tumor progression, mediated by growth factors secreted by macrophages, is the process of angiogenesis. 3 Examples of this situation are the development of colon cancer in ulcerative colitis or Crohn’s disease, or hepatocarcinoma in the context of hepatitis C infection. 4
Similar to this type of cancer generation process, in its course of invasion, tumoral proliferation causes tissue damage, which subsequently generates and boosts inflammatory response. 2 Inflammatory cells may be a double-edged sword, with a counterproductive effect on the tumor, and pose a genuine defense, trying to suppress growth and proliferation. Cancer is associated with inflammation, but also causes inflammation, as it progresses through healthy tissue.
The differentiation of tumoral growth from the inflammatory change that accompanies it is paramount in planning treatment in cases where surgery seeks to preserve function. An example is the planning of resection of brain tumors: the amount of removed tissue, independent of the tumor itself, affects the prognosis.
How can imaging techniques help in the planning in these cases?
Physiopathologically, the destruction of tissues induced by tumoral inflammation results in the release of the water contained in cells (edema). At the same time, the tumoral advance favors angiogenesis. These pathophysiological processes are easily detectable with some imaging techniques. Another example of the need to preserve function becomes evident when tumoral processes advance through bone tissue. Conservative approaches to surgery (e.g. salvage of a limb) may improve the quality of life of the patient.
Previous studies demonstrated that many properties and types of cells within bone and its microenvironment contribute to tumor-induced bone disease. 2 Cell destruction triggers the release of factors that favor further tumoral growth 5 and the destruction of normal bone through several mechanisms, including angiogenesis. Therefore, inflammation also occurs in bone.
Conventional computed tomography (CT) is unable to reliably distinguish edema from soft tissue masses within the bone medullary, but at the same time is a superb tool for the evaluation of tumoral matrix in bone tumors. Positron emission tomography/CT has high sensitivity for the detection of the presence of tumor, but low spatial resolution for the accurate definition of lesion margins. Magnetic resonance imaging (MRI) without contrast is sensitive to the detection of medullary abnormalities; however, due to the pathophysiology of tumor spreading in the bone, edema and tumor infiltration is indistinguishable in some cases. Dynamic-enhanced MRI has the capability of discerning between edema (linked to cellular destruction) and angiogenesis (linked to tumor progression), based on the time that enhancement is detected. Vascularized regions enhance earlier than edematous regions. However, in some cases, regions of edema may contain slow-flowing capillaries, and contrast may be visible at early stages, 6 a situation that can paint an equivocal picture. Dual-energy CT is a promising tool, with some studies demonstrating its ability to discern inflammatory infiltration and tumor infiltration in animal models. 7
Our aim is to illustrate how the careful use of imaging tools can help to draw the line between tumoral infiltration and inflammatory-edematous change, providing information to assist in surgical planning.
Illustrating the possibility to draw the line with a case series study: parosteal osteosarcoma
Parosteal osteosarcoma (POS) is an uncommon malignant bone tumor usually arising from the posterior cortical of the distal femur, comprising 4% of all osteosarcomas (OS). 8 POS arises from a juxtacortical location and usually occurs in the metaphyses of long bones. 9 Even if it is histologically low grade, it can present medullary involvement. 10 The rate of medullary involvement is reportedly 18% in Grade-1 lesions, 25% in Grade-2 lesions, and 43% in dedifferentiated lesions. 8
To assess medullary involvement before surgery, CT and MRI are the best techniques. MRI is more sensitive than CT for the characterization of medullary bone abnormalities 11 ; however, these abnormalities sometimes consist of edema, and not tumoral infiltration. If infiltration is present, this could change the surgical treatment and local recurrence, and therefore have an impact on survival. 12
On the other hand, if reactive edema is mistaken as tumor infiltration, more aggressive surgeries might be performed, with an increased rate of complications, morbidity, and impact on the patient’s life.
Our aim is to compare medullary involvement visible on CT and MRI with histological analysis, to assess the accuracy of each technique to determine true tumoral extension.
Material and methods
We retrospectively reviewed 72 cases of POS treated at our institution from 2003 to 2015, and selected those patients that had had CT or MRI with a reported finding of medullary abnormality and who had subsequently been submitted to surgery. Patients that had not been found to present medullary abnormality on CT or MRI, or had not been treated surgically, were excluded from the study.
A total of 22 patients out of 72 (8 men and 14 women; mean age 29.6 years old; range 9–53) had pretreatment imaging (CT/MRI) positive for medullary abnormality. All imaging was reviewed by two musculoskeletal radiologists. Medullary abnormalities on MRI appeared as a hypo-intensity on T1-weighted images and hypo- or hyperintensity on T2-weighted fat suppressed (T2 FS) images. CT medullary abnormality was defined as a homogeneous region of sclerosis.
All 22 POS cases were treated surgically and the specimens were analyzed histologically by two expert pathologists. Out of the 22 patients with positive medullary findings, 21 had CT and 15 MRI. Fourteen patients had both CT and MRI, and were included in the study. Fisher’s exact test was applied to evaluate the performance of each technique.
Results
Fourteen of the 22 cases had CT and MRI. Of the 14 cases with CT and MRI, 14 had medullary abnormality on MRI (100%). Only 6 showed medullary abnormality on CT (42.9%).
In a histological examination of tumoral extension, the cases that showed an abnormality on MRI but not on CT (14 − 6 = 8) only showed thickened trabeculae, fatty marrow, and hypervascularization of the bone marrow, with no tumoral cells present. In the cases where the two examinations showed medullary abnormality (6 cases on CT, given that all 14 cases showed abnormality on MRI), the medullary abnormality was confirmed as tumoral cell infiltration.
MRI demonstrated high sensitivity (100%) for the detection of medullary abnormality, but had low specificity (0%; no true negatives), with low precision (low positive predictive value, 40%), and a high false discovery rate (60%). Accuracy was low (40%). The high negative predictive value was high (100%) (P=1). CT demonstrated high sensitivity (100%) and high specificity (100%), with high precision (positive predictive value 100%), high negative predictive value (100%), and high accuracy (100%) (P = 0.000333)
Discussion
The prognosis in POS is better than in conventional OS, with a 5-year overall survival rate of 65%–96%. 13 Given the overall good prognosis and the frequently limited local extension of the tumor, surgical treatment options can range from marginal resection to wide resection. The incidence of local recurrence has been demonstrated to be strictly related to the adequacy of surgical tumor margins. 14
Poor prognostic factors in POS include incomplete excision and the presence of tumor dedifferentiation. 10 A potential cause for incomplete excision is intramedullary extension. Some authors found no connection between medullary involvement and dedifferentiation 13 ; others reported a higher rate of higher tumor grades. 9 This consideration suggests that invasion into the medullary cavity is a sign of tumor aggressiveness. Medullary involvement has been described in 52% of dedifferentiated POS, 15 and in some cases where telangiectatic differentiation was present. 16
The diagnostic modalities to study POS medullary involvement are MRI and CT. MRI (water sensitive and T1 sequences) is the most sensitive modality to evaluate medullary abnormalities, and therefore, to potentially expose infiltration. 17 However, medullary abnormality may merely represent edema due to inflammatory change associated with tissue damage. CT is not sensitive to the detection of edema in the medullary, but it is sensitive to the detection of bone texture abnormalities, which are typical for the progression of osteosarcomas (osteoblastic tumors). 11
In our series, the CT-positive cases for medullary invasion (6/6 cases) demonstrated a region of dense sclerosis abutting the medullary (Figure 1). When retrospectively evaluated on MRI (6 out of 14 cases where MRI was positive for medullary abnormality), these regions appeared as predominantly low in signal intensity on both T1 and T2 FS images. In the remaining 8 cases, MRI demonstrated abnormality, consisting of hypointensity on T1 sequences but hyperintensity in T2 FS sequences. This correlated to thickened trabeculae, fatty marrow, and hypervascularization of the marrow in a histological analysis (Figure 2).
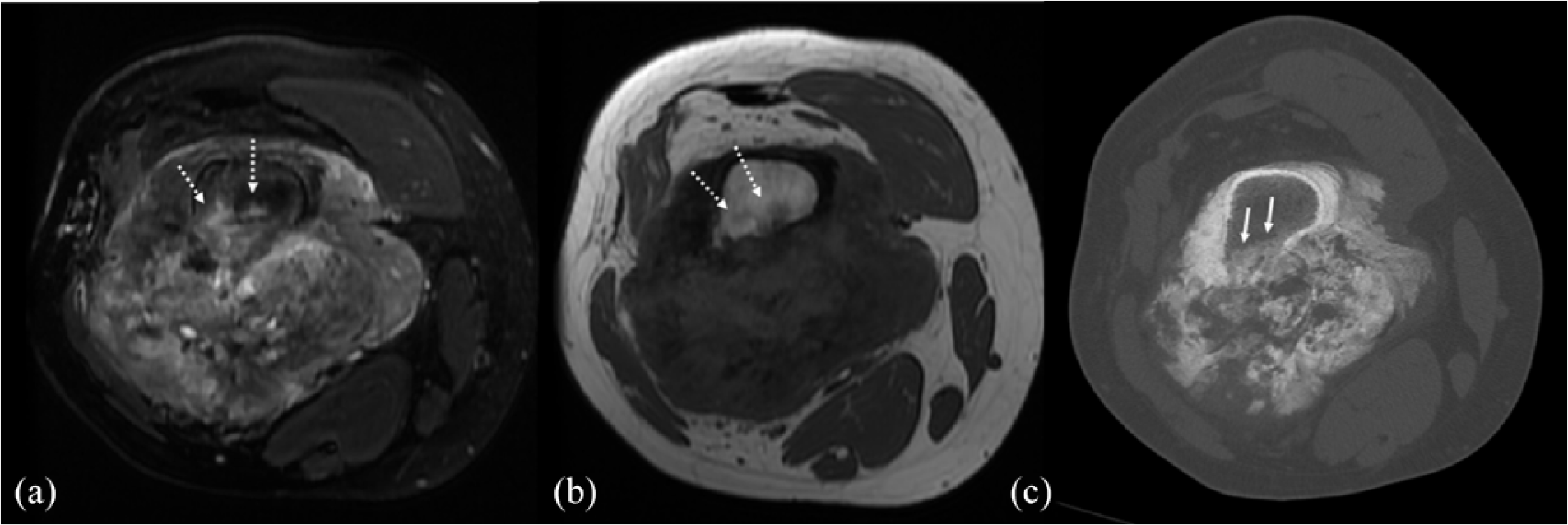
Positive tumoral infiltration. (a) T2 FS axial image demonstrates hyperintensity in the medullary, adjacent to the parosteal location of the tumor (dotted arrows). The cortical is breached. (b) T1-weighted image demonstrates mild hypointensity corresponding to the hyperintense region on T2 FS (dotted arrows). (c) CT at this same level demonstrates a geographical region of sclerosis in the medullary, corresponding to the hyperintense region on T2 FS and hypointense region on T1 (solid arrows). Histology was positive for tumoral infiltration in this area.
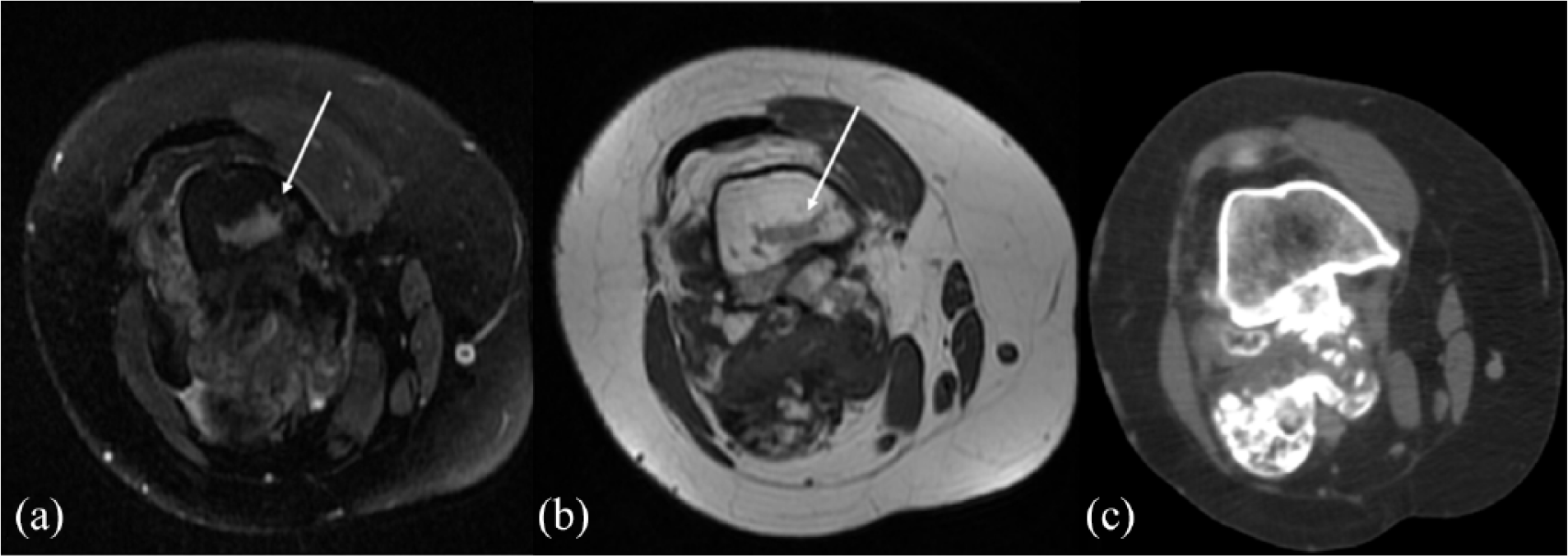
Negative tumoral infiltration. (a) T2 FS axial image demonstrates hyperintensity in the medullary, adjacent to the parosteal location of the tumor (solid arrow). Note how the posterior cortical appears thin and indistinct, with adjacent tumor mass. (b) T1-weighted image demonstrates a hypointense region corresponding to the hyperintense region on T2 FS (solid arrow), and demonstrates the existence of a tumoral mass attached to the cortical. (c) CT at this same level does not demonstrate any abnormality. Histology was negative for tumoral infiltration in this case, demonstrating only thickened trabeculae, fatty marrow and increased vascularity in this region.
The presence of ossified matrix in the medullary is a sign of tumor infiltration. Edema, as the manifestation of inflammatory change, does not correlate with tumor extension in our series. When MRI showed abnormalities in signal intensity in T2 FS but CT did not show medullary abnormality (ossified matrix), histology revealed no medullary involvement.
A similar histopathological aspect was found by another group 18 demonstrating the unique feature of a case report of a POS which mimicked medullary involvement by secondary remodeling of the cortex underlying the tumor. The concept that the tissue abutting in the medullary canal in POS does not always represent tumor infiltration was first presented by Okada et al. 8 who found no association between local recurrence and medullary involvement. Later, Lewis et al. 14 concluded that focal medullary involvement did not necessitate the resection of the entire segment of the lesion.
A limitation to this study is that our case series is small, but POS is a relatively uncommon type of tumor. In our imaging evaluation, we did not use contrast or advanced MRI techniques, 19 which have been proven to be useful in the assessment of the progression of other bone tumors. 20
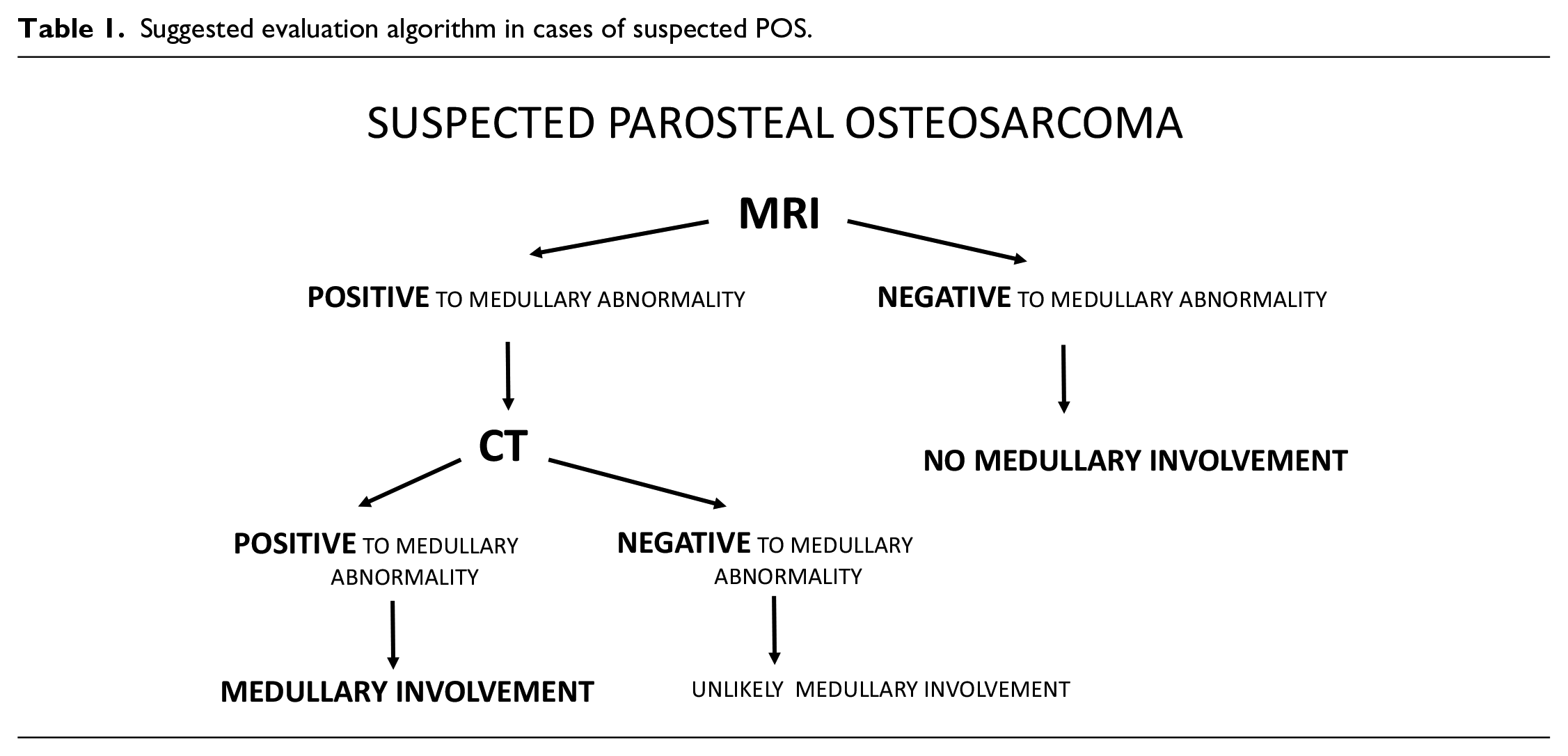
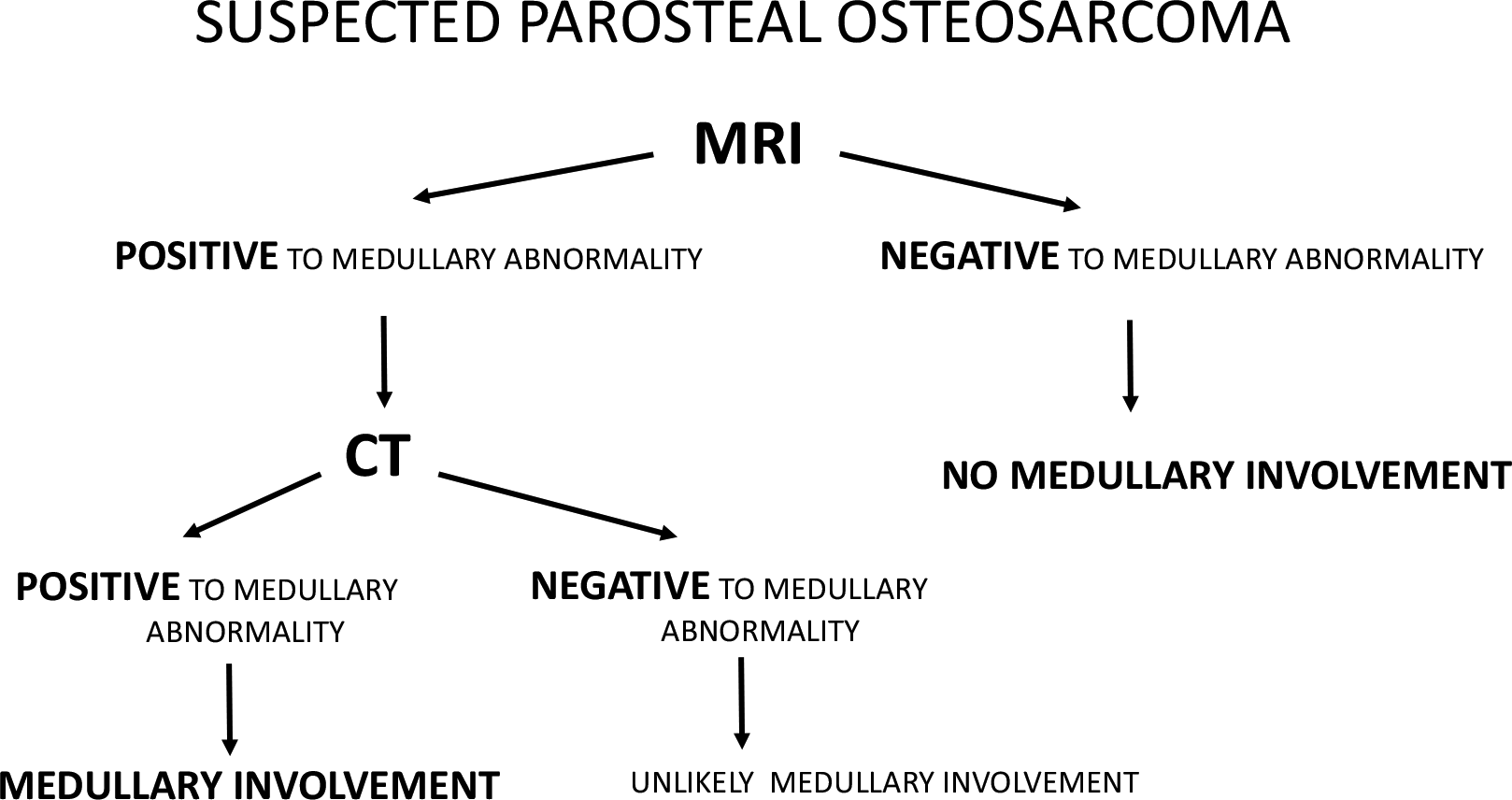
An accurate demarcation of the true extent of the tumor is useful in POS to avoid excessive bone resection and to improve functional results. Caution is required on the interpretation of medullary abnormality on MRI when studying POS. MRI is highly sensitive for the detection of medullary abnormality, but it lacks specificity for tumor invasion. Correlation with CT is recommended in all cases of positive MRI to add specificity for tumors. Table 1 suggests an evaluation algorithm in cases of suspected POS.
Suggested evaluation algorithm in cases of suspected POS.
The combination of MRI and CT allows for high accuracy in the determination of the true extension of tumoral infiltration in POS, with the possibility of assisting in the planning of conservative surgeries that avoid surgical morbidity.
Our results regarding POS illustrate the role of imaging in a relatively basic level as an already powerful tool to aid in the differentiation of pure inflammatory changes from true tumoral progression.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.