
Abstract
Objective:
This study aimed to investigate the correlation of Helicobacter pylori (Hp) infection with disease risk and severity of colorectal adenoma, also to explore the association of cytotoxin-associated gene A (CagA) positive (CagA+)-Hp infection with gastrin and ki-67 expressions in colorectal adenoma patients.
Methods:
There were 1000 colorectal adenoma patients and 1500 controls consecutively enrolled, then Hp infection status was determined by 14C urea breath test and rapid urease test. Also, serum CagA expression and gastrin expression of colorectal adenoma patients were determined by enzyme-linked immunosorbent assay. Ki-67 expression in adenoma tissue of colorectal adenoma patients was assessed using immunohistochemistry.
Results:
Hp+ rate in colorectal adenoma patients (623 (62.3%)) was more elevated than that in controls (814 (54.3%)). Multivariate logistic regression model analysis disclosed that Hp+ was an independent risk factor for colorectal adenoma. Additionally, Hp+ was positively associated with tumor size and high-grade intraepithelial neoplasia in colorectal adenoma patients. Also, serum gastrin expression and intratumoral ki-67 expression were higher in Hp+ CagA+ patients and Hp+ CagA− patients compared to Hp− patients, and they were also higher in Hp+ CagA+ patients compared to Hp+ CagA− patients.
Conclusion:
Hp infection positively associates with higher disease risk and worse disease conditions of colorectal adenoma, and CagA enhances the carcinogenicity of Hp in colorectal adenoma.
Introduction
Colorectal cancer, one of the most common cancer worldwide, ranks the third most prevalent cancer and the second leading cause of cancer deaths.1,2 According to a recent epidemiological survey, there were 1,800,977 new colorectal cancer cases and 861,663 colorectal cancer-related deaths in 2018.1,3 Colorectal adenoma (CRA) is the primary precancerous lesion of colorectal cancer.4-6 Therefore, exploring the risk factors for predicting CRA is critical for the prevention of colorectal cancer.
Helicobacter pylori (Hp) is standardized as a class I carcinogen of gastric cancer by the International Agency for Research on Cancer, especially for cytotoxin-associated gene A positive (CagA+) Hp.7-9 Recently, accumulating evidence revealed that Hp is not only a risk factor for gastric cancer, but also a factor presenting with a carcinogenic effect on other digestive cancers such as hepatobiliary and pancreatic.10,11 Considering the potential carcinogenic effect of Hp in these digestive cancers, we hypothesized that Hp might also contribute to the development and progression of CRA. However, several studies with small samples drew contradictory results with respect to the association of Hp infection with CRA risk; some studies discovered that Hp infection was associated with higher CRA risk, while some studies reported that there was no association of Hp infection with CRA risk.12,13 Hence, the role of Hp in CRA carcinogenicity has not been fully clarified, which may be because most of these previous studies had small sample sizes, thereby generating low statistical power and leading to unconvincing results. Therefore, a large-sample-size study unveiling the role of Hp in CRA development and progression is urgently needed.
In this study, we enrolled 1000 CRA patients and 1500 controls to investigate the correlation of Hp infection with CRA disease risk and disease condition, and to explore the association of CagA positive-Hp infection with gastrin and ki-67 expressions in CRA patients.
Methods
Participants
Between January 2011 and December 2015, 1000 CRA patients who were treated at the Central Hospital of Wuhan and 1500 age- and sex-matched controls who underwent screening colonoscopy during a physical examination at the hospital were consecutively enrolled in this study. The screening criteria for CRA were (a) the diagnosis of CRA was based on conventional clinical, radiological, endoscopic, and histological examinations according to the World Health Organization (WHO) criteria; 14 (b) age above 18 years; and (c) complicated with chronic gastritis confirmed by esophagogastroduodenoscopy. The screening criteria for controls were (a) confirmed diagnosis of chronic gastritis by esophagogastroduodenoscopy examination; and (b) aged above 18 years. Both CRA patients and controls were excluded if they (a) previously underwent Hp eradication treatment, (b) had taken proton pump inhibitors, H2 receptor antagonists, antibiotics, and corticosteroids within the past 4 weeks; (c) had a condition complicated with autoimmune diseases; (d) had a history of malignancy or gastrointestinal surgery; and (e) were pregnant or lactating. Informed consents were collected from all study subjects, and the research project was approved by the Ethics Committees of the Central Hospital of Wuhan.
Data collection
Demographic characteristics and clinical features of CRA patients and controls were documented after enrollment, including age, gender, body mass index (BMI), smoke status, drink status, chronic complications (diabetes, hypertension, hyperlipidemia), and family history of colorectal cancer. Also, the tumor features of CRA patients were recorded, including tumor size, number of nodules, presence of a pedicle, pathologic types of CRA, and grade of intraepithelial neoplasia (IEN).
Hp detection
Hp infection status was determined by 14C urea breath test (UBT) and rapid urease test (RUT). The values of 14C UBT ⩾100 dpm/mmol were considered positive, and the values <100 dpm/mmol were considered negative. In addition, biopsies of gastric mucosa were collected from CRA patients and controls by esophagogastroduodenoscopy for the screening of gastric cancer after they signed informed consents, and the biopsies were used for the RUT. In our studies, when the 14C UBT and RUT were both positive, a diagnosis of Hp positive (Hp+) was established, whereas when both tests indicated negative results, the patients were defined as Hp negative (Hp−).
Determination of serum CagA and gastrin
Blood samples from CRA patients and controls were collected in serum separation tubes and were centrifuged at 1000 g for 10 min at room temperature after spontaneous coagulation of 30 min, then the separated serum samples were stored at −80°C until analysis. Serum CagA and gastrin levels of CRA patients were measured by human CagA enzyme-linked immunosorbent assay (ELISA) kit (CUSABIO, Wuhan, China) and human gastrin ELISA kit (CUSABIO), respectively, according to the manufacturer’s protocol. In addition, each sample was tested in triplicate. The optical density (OD) of each sample was determined using a microplate reader setting at 450 nm. OD sample/OD negative ⩾2.1 patients were defined as CagA+; and OD sample/OD negative <2.1 patients were defined as CagA negative status (CagA−).
Immunohistochemistry for Ki-67
Immunohistochemistry (IHC) was used to detect the expression of proliferation-associated antigen Ki-67 in adenoma tissue obtained from CRA patients. Briefly, paraffin sections were dewaxed and rehydrated, followed by antigen retrieval via microwave heating, then the slides were rinsed in phosphate buffered saline (PBS). Then the sections were incubated with 3% H2O2 solution at room temperature for 10 min to block endogenous peroxidase, then washed with PBS. The sections were blocked with goat serum at room temperature for 15 min, followed by the removal of blocking solution through the PBS washing. Next, the sections were incubated with a mouse anti-human Ki-67 monoclonal antibody (Abcam, Massachusetts, USA) at 37°C for 60 min. Afterward, the sections were incubated with horseradish peroxidase-conjugated Goat Anti-Mouse IgG H&L antibody (Abcam, Cambridge, MA, USA) at 37°C for 30 min. Subsequently, 3,3′-Diaminobenzidine (Sigma, St. Louis, MO, USA) was used for the chromogenic reaction, which was followed by a hematoxylin and eosin counterstain. Finally, the sections were dehydrated through an alcohol gradient, clarified in xylene, mounted in neutral resin, and observed by light microscopy. Ki-67 positive cells could be identified by the appearance of brownish-yellow or brown granules in the cell nuclei. The percentage of positive cells represented the relative expression levels of the Ki-67 protein: 10 highly magnified visual fields (10 × 40 magnification, with no overlap) from each tissue section were randomly selected. 15
Statistical analysis
The statistical analysis was performed by SPSS 18.0 software (IBM, Chicago, IL, USA), and figures were plotted by the GraphPad Prism 7.02 software (GraphPad Software Inc., San Diego, CA, USA). Data were displayed as mean and SD, or count (percentage). Comparison between two groups was determined by the Student’s t-test, the Chi-square test, or the Wilcoxon rank sum test, and comparison among three groups was determined by one-way analysis of variance (ANOVA) followed by multiple comparisons with Bonferroni correction. Factors that were related to the CRA risk were determined by the stepwise forward multivariable logistic regression. All tests were two-sided, and a value of P <0.05 was considered statistically significant.
Results
Participants’ characteristics
Mean values of age were 61.4±16.2 and 56.9±13.4 years in CRA patients and controls. The numbers of male and female patients were 592 (59.2%) and 408 (40.8%) in CRA patients, and 872 (58.1%) and 628 (41.9%) in controls (Table 1). There were no differences in age (P = 0.238) or gender (P = 0.596) between CRA patients and controls. However, both the percentage of patients with hyperlipidemia (286 (28.6%) vs. 305 (20.3%); P < 0.001) and the percentage of patients with family history of colorectal cancer (181 (18.1%) vs. 168 (11.2%); P < 0.001) were increased in CRA patients compared to the controls. Other clinical characteristics are depicted in Table 1.
Characteristics of participants.
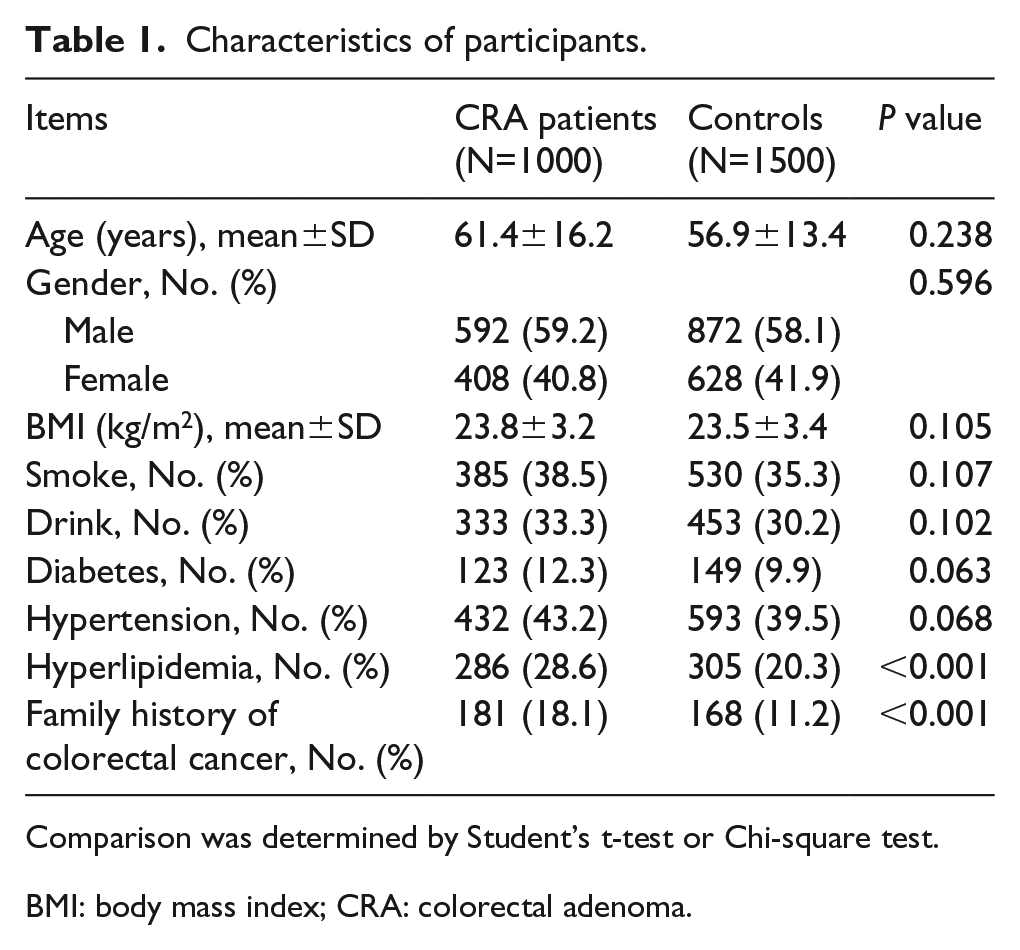
Comparison was determined by Student’s t-test or Chi-square test.
BMI: body mass index; CRA: colorectal adenoma.
Comparison of Hp+ rate between CRA patients and controls
The numbers of Hp+ patients were 623 (62.3%) in CRA patients and 814 (54.3%) in controls (Figure 1). The Chi-square test revealed that the Hp+ rate in CRA patients was higher than that in controls (P < 0.001).
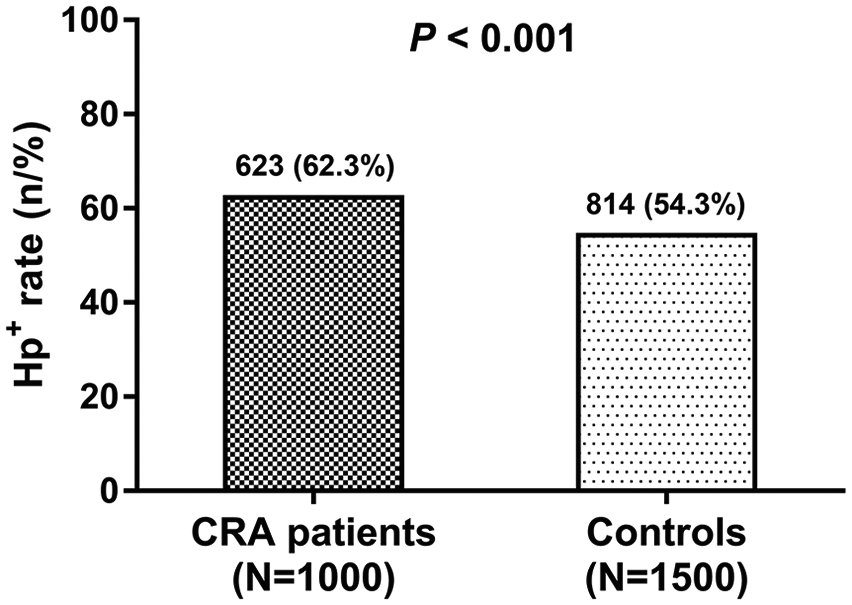
Hp+ rate in CRA patients and controls. Comparison of Hp+ rate between CRA patients and controls. Comparison between two groups was determined by the Chi-square test. P < 0.05 was considered significant.
Analysis of factors affecting CRA risk
Stepwise forward multivariate logistic regression model analysis was conducted to investigate factors affecting CRA risk, which disclosed that Hp+ (P = 0.032; OR = 1.17) was an independent risk factor for predicting CRA (Table 2). Meanwhile, hyperlipidemia (P = 0.024; OR = 1.38) and family history of colorectal cancer (P = 0.015; OR = 1.53) also independently predicted increased risk for CRA.
Stepwise forward multivariate logistic regression model analysis of factors affecting CRA risk.
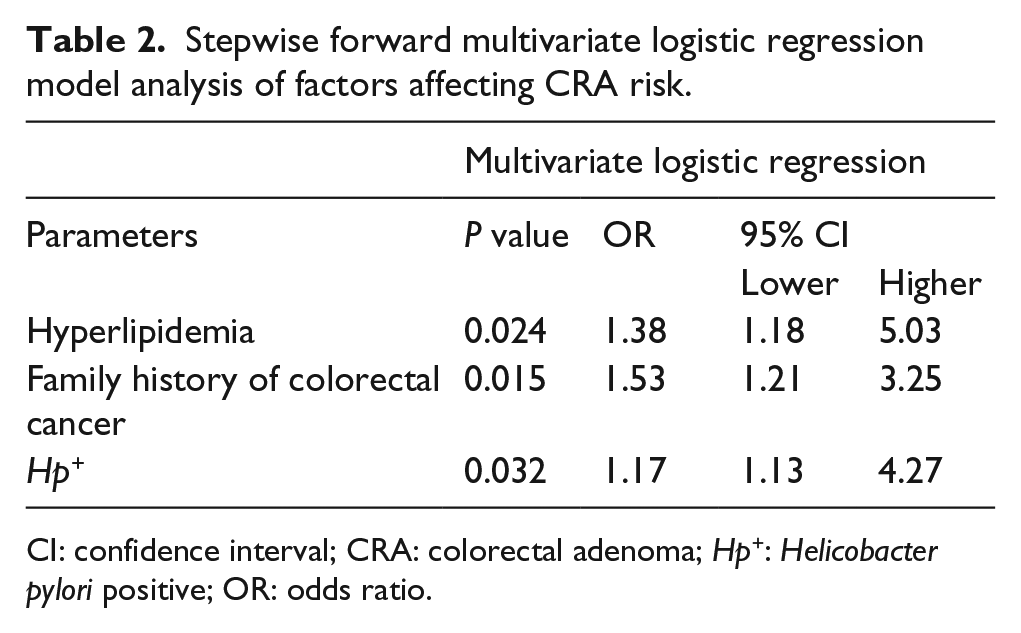
CI: confidence interval; CRA: colorectal adenoma; Hp+: Helicobacter pylori positive; OR: odds ratio.
Association of Hp infection status with tumor characteristics in CRA patients
Hp+ was positively associated with tumor size (P = 0.019) and high grade IEN (P = 0.025), but was not correlated with the number of nodules (P = 0.203), the presence of pedicles (P = 0.895), or pathologic types (P = 0.832) (Table 3).
Correlation of Hp infection status with tumor characteristics.
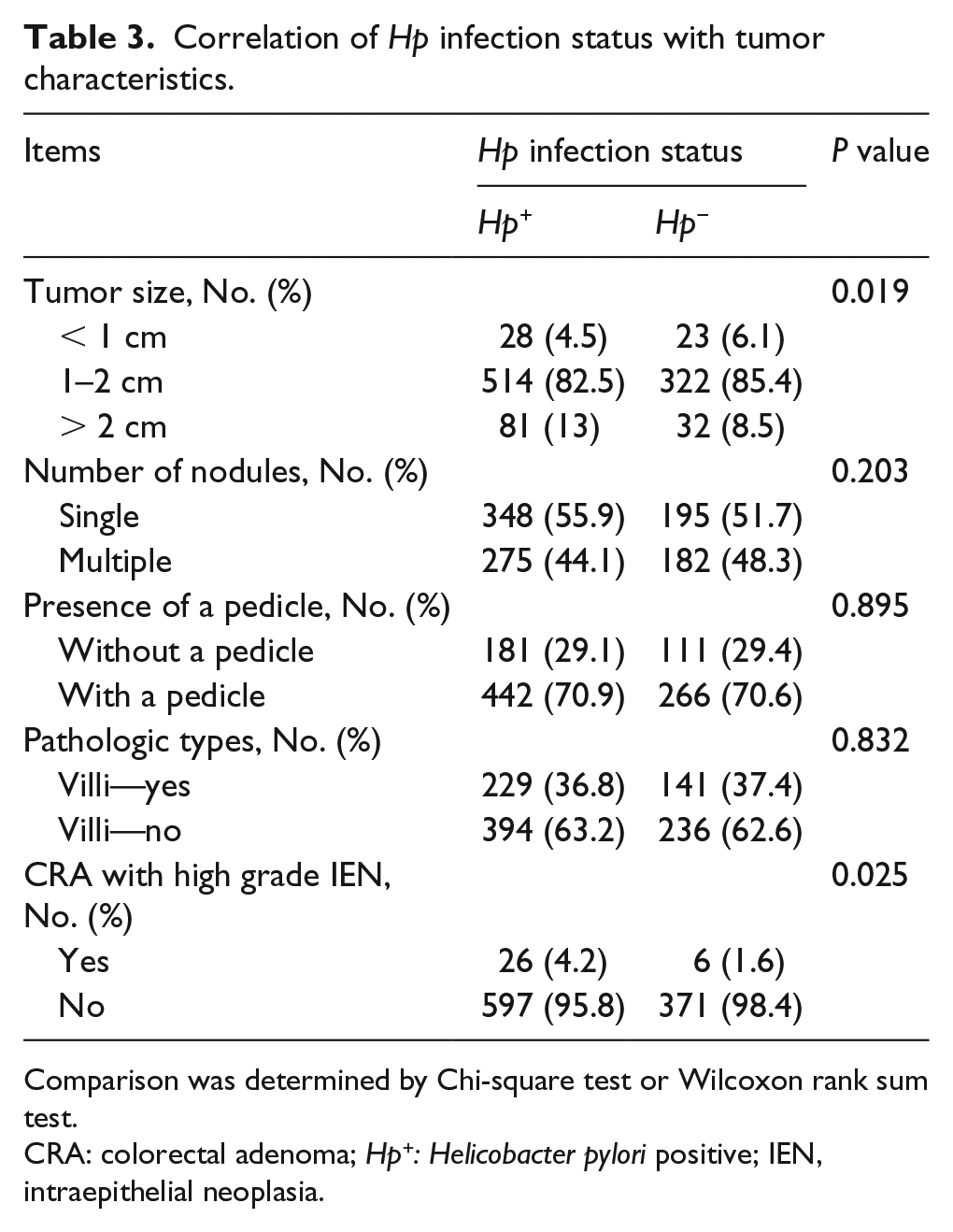
Comparison was determined by Chi-square test or Wilcoxon rank sum test.
CRA: colorectal adenoma; Hp+: Helicobacter pylori positive; IEN, intraepithelial neoplasia.
Comparison of gastrin level in serum and Ki-67 expression in tumor tissue among Hp+CagA+, Hp+CagA− and Hp− patients
In order to explore the potential role of Hp in CRA pathology, we further investigated the gastrin level in serum and Ki-67 expression in tumor tissue in Hp+CagA+ patients (n=510), Hp+CagA− (n=113) patients, and Hp− patients (n=337). The results showed that serum gastrin expression was elevated in Hp+CagA+ patients (P < 0.001) and Hp+CagA− patients (P < 0.001) compared to Hp− patients, and was also increased in Hp+CagA+ patients compared to Hp+CagA− patients (P < 0.001) (Figure 2(a)). For ki-67 expression in tumor tissue, it was increased in Hp+CagA+ patients and Hp+CagA− patients compared to Hp− patients, and was also elevated in Hp+CagA+ patients compared to Hp+CagA− patients (Figure 2(b)).
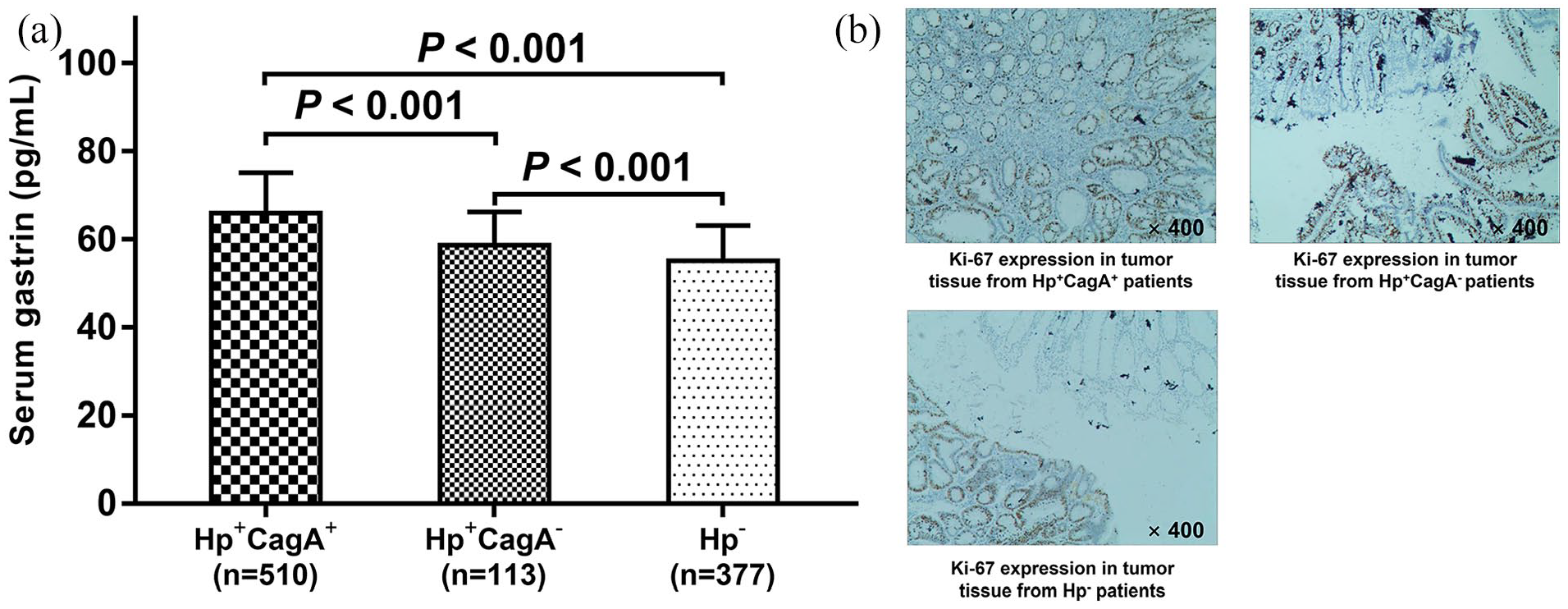
Gastrin level in serum and Ki-67 level in tumor tissue in Hp+CagA+ patients, Hp+CagA−, and Hp− patients. Comparison of serum gastrin level among Hp+CagA+ patients, Hp+CagA− patients, and Hp− patients (a). Ki-67 level in tumor tissue in Hp+CagA+ patients, Hp+CagA− patients, and Hp− patients (b). Comparison among three groups was determined by one-way ANOVA followed by multiple comparisons with Bonferroni correction. P < 0.05 was considered significant.
Discussion
Hp has been demonstrated to promote the development of gastric cancer16,17,18 Recently, it was reported that Hp correlated with increased cancer risk in the digestive system (such as pancreatic cancer and hepatocellular carcinoma).10,11 The opinions in previous studies are still conflicting regarding Hp with CRA risk.12,13,19 According to previous studies, Hp infection increases the CRA incidence12,19; however, there is also a study reporting that Hp infection is not associated with CRA risk. 13 Thus, whether Hp is associated with CRA risk still remains unclear. Therefore, a large-sample-size study is needed to clarify the association of Hp infection with CRA risk and CRA patients’ clinical features. In the present study, 1000 CRA patients and 1500 matched controls were enrolled to compare their Hp+ rates, which revealed that the Hp+ rate in CRA patients was higher than that in controls, suggesting that Hp infection was correlated with increased CRA risk. Also, Hp+ was an independent predicting factor for higher CRA risk. There are several possible reasons for the result: (a) Hp infection might weaken normal functions of gastric mucosa so that the weaken gastric mucosa was unable to destroy many toxic substances and pathogens (derived from food); these toxic substances and pathogens went into the colon and rectum, and then caused injury to both, subsequently increasing the CRA risk. (b) Hp infection might also directly secrete toxic proteins (such as CagA) and then upregulate a few CRA-related proteins (such as gastrin), which subsequently elevate the CRA risk.20,21 In this study, we also discovered that Hp+ was positively correlated with tumor size and high-grade IEN, suggesting that Hp infection was associated with worse disease conditions in CRA patients. The possible explanations might be as follows: (a) Hp impaired CRA patients’ stomach capacities, which caused larger burdens to the colon and rectum, leading to an aggravation of their disease condition. (b) Hp upregulated several cancer-related proteins (including gastrin), and subsequently stimulated tumor cell proliferation while reducing apoptosis, which contributed to worse disease conditions in CRA patients.20,21
Gastrin is a pivotal hormone that maintains the normal functions of the stomach, which has been found to be upregulated by Hp in gastric cancer cells.22,23 There are recent reports illuminating that an elevated gastrin level promotes CRA tumorigenesis, which could also be seen in our multivariate logistic regression model analysis.24,25 Considering that Hp stimulates gastrin expression, and that both Hp and gastrin exert the carcinogenic effect of CRA, we therefore hypothesized that Hp might stimulate gastrin expression and then promote tumor progression in CRA patients. However, because the relevant information is still limited, we compared the serum gastrin expression and inter-tumor ki-67 (a well-known biomarker for cancer cell proliferation) expression between Hp+CagA+/Hp+CagA− patients and Hp− patients, and the results disclosed that both of them were increased in Hp+CagA+ patients and Hp+CagA− patients compared to Hp− patients, suggesting that Hp might promote CRA progression by advocating gastrin expression, which might be caused by Hp-induced atrophy changes of the gastric body mucosa, leading to increased levels of serum gastrin by negative feedback on antral G cells, and subsequently stimulated tumor cell proliferation of CRA, which caused an elevated ki-67 expression.22,26
CagA, a soluble protein that presents in highly virulent strains of Hp, is an important virulence factor for Hp-generated pathogenicity.9,20 Accumulating evidence reveals that CagA+ Hp strains strikingly promote the gastrin expression and then elevate the risk of gastric cancer.20,27-29 For the purpose of analyzing the effect of CagA on Hp-induced gastrin expression and CRA progression, we subsequently compared the serum gastrin expression and inter-tumor ki-67 expression between Hp+CagA+ patients and Hp+CagA− patients, which elucidated that both of them were elevated in Hp+CagA+ patients compared with Hp+CagA− patients, indicating that CagA enhanced the carcinogenic effect of Hp in CRA patients. There are several possible reasons for the result: (a) CagA was able to strengthen the virulence of Hp, thereby enhancing the gastrin upregulation as well as the ki-67 upregulation effect of Hp indirectly;30,31 and (b) CagA might also directly promote gastrin expression, thereby increasing ki-67 expression. 23 Briefly, this large-sample-size study not only illuminated the positive correlation of Hp infection with higher CRA risk and worse disease conditions, but also disclosed the associations of Hp+CagA+ with gastrin and ki-67 expressions in CRA patients.
There are a few limitations in this study. First, it was a single-center study where most of the participants were recruited from Middle China, which might bring in selection bias. Second, Hp infection is the most common cause of chronic gastritis, and Hp-related chronic gastritis as a risk factor for colorectal neoplasm. In order to ensure the relatively high positive percentage of Hp infection (to increase statistical power and decrease the requirement of sample size), all CRA patients and controls enrolled in this study were complicated with Hp infection. However, this might be a potential source of bias. Third, the detailed molecular mechanisms of Hp+CagA+ in promoting CRA progression also required additional exploration.
In conclusion, this large-sample-size clinical study revealed a positive correlation of Hp infection with higher CRA risk and worse CRA patients’ disease conditions, and discloses a positive association of Hp+CagA+ with gastrin and ki-67 expressions in CRA patients.
Supplemental Material
Supplement_files – Supplemental material for Cytotoxin-associated gene A increases carcinogenicity of helicobacter pylori in colorectal adenoma
Supplemental material, Supplement_files for Cytotoxin-associated gene A increases carcinogenicity of helicobacter pylori in colorectal adenoma by Heng Zhang, Yusheng Liao, Hongfeng Zhang, Jie Wu, Dan Zheng and Zhitao Chen in The International Journal of Biological Markers
Footnotes
Author contributions
Heng Zhang and Yusheng Liao contributed equally to this work.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This study was supported by Natural Science Foundation of China (81400578), The Ministry of Education Doctoral Fund (20130142120096), and the Wuhan City Health Bureau project (WX13A07).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.