
Abstract
Background:
Preoperative estimation of microvascular invasion is of great significance for the clinical decision making in hepatocellular carcinoma. Neutrophil-lymphocyte ratio (NLR) has been reported to be correlated with the poor prognosis of hepatocellular carcinoma. However, the conclusions are conflicting on whether high preoperative NLR level is associated with the presence of microvascular invasion.
Aim:
To evaluate the association between preoperative NLR level and the risk of microvascular invasion in hepatocellular carcinoma.
Methods:
Relevant studies were identified by searching PubMed and Embase through February 2019. Fixed or random models were applied to analyze the data based on the heterogeneity. Subgroup, sensitivity, and publication bias analyses were performed. Review Manager 5.3 and STATA software were used for the meta-analysis.
Results:
A total of 15 studies were eventually included in this meta-analysis. Pooled data based on retrospective cohort studies showed there are more hepatocellular carcinoma patients with vascular invasion (OR 1.74; 95% Cl 1.42, 2.12; P < 0.001) and microvascular invasion (OR 1.62 95% Cl 1.39, 1.89; P < 0.001) in the high NLR group than in the low NLR group. Of case-control studies, a higher preoperative NLR level was found in the microvascular invasion positive group than in the microvascular invasion negative group (OR 0.62; 95% Cl 0.35, 0.90; P < 0.001). The subgroup, sensitivity, and publication bias analyses did not change the results.
Conclusion:
A higher preoperative NLR level is positively correlated with the risk of microvascular invasion in hepatocellular carcinoma.
Keywords
Introduction
Hepatocellular carcinoma (HCC) accounts for 90% of primary liver cancer, 1 which is the sixth most common cancer and the fourth leading cause of cancer-related mortality worldwide. 2 Surgical resection is regarded as the most effective therapy for HCC patients. 3 However, a high postoperative tumor recurrence rate occurs after curative surgical resection, partly due to the presence of microvascular invasion (MVI).4,5 MVI is the independent risk factor of poor prognosis in HCC patients, which can reflect the capacity of the invasiveness and metastasis of HCC. 6 Furthermore, MVI can guide on whether to perform liver transplantation beyond Milan Criteria, anatomical liver resection, widening of the surgical margin, and neoadjuvant chemotherapy.7-10 Therefore, it is of great significance to predict the risk of MVI in HCC before surgery.
HCC is an inflammation-driven cancer in which chronic inflammation matters. 1 Neutrophil-lymphocyte ratio (NLR), an inflammatory indicator, has been reported to be correlated with the poor prognosis of HCC.11-13 However, to our knowledge, there are conflicting results on whether NLR is associated with the presence of MVI even though many studies have been reported on this topic. Thus, we performed a meta-analysis of case-control and cohort studies to evaluate the relationship between preoperative NLR level and the risk of MVI in HCC.
Materials and Methods
Search Strategy
The literature search was performed in PubMed and Embase through February 2019 using the search strategy (Table S1) by two authors. All eligible articles were retrieved, and their references of identified publications were searched for further potentially relevant articles.
Study selection
Studies included in the meta-analysis should fulfill the following inclusion criteria: (a) cohort or case-control design; (b) HCC patients; (c) data of preoperative NLR level in MVI negative and positive groups, or available data of the number of MVI-positive patients in high and low NLR groups. To avoid repeated reports from one author or institute, we only included the data from the recent studies with the largest numbers of patients. Studies were excluded if they did not meet the inclusion criteria.
Data retraction and quality assessment
All articles were retrieved and assessed independently by two authors. They extracted data including first authors, publication date, country of origin, study design, total cases, number of observed and expected cases, characteristics of the study population (including sex, age), and preoperative NLR level grouped by MVI or the number of MVI positive patients grouped by NLR level. Any disagreement was resolved by discussion.
The Newcastle–Ottawa Scale (NOS) was employed to assess the quality of included studies. 14 There are eight items in three aspects: selection, comparability and outcome (cohort), or exposure (case-control). The full score was 10 stars. Four to six stars was regarded as a moderate-quality study, and seven to nine stars as a high-quality study.
Statistical analysis
All the statistical analyses were carried out by Review Manager Version 5.3 (RevMan 5.3) software and STATA (Version 12.0; STATA Corporation, College Station, TX, USA) software. Statistical heterogeneity was assessed with I2 and P-value. 15 A fixed effects model was adopted if there was no evidence of significant heterogeneity (I2 ⩽ 50% and P ⩾ 0.1); otherwise, the random-effects model was used. Weighted mean difference (WMD) with 95% confidence intervals (95% CI) was calculated for continuous variables. Odds ratio (OR) with a 95% CI were used for discontinuous variables. Subgroup analyses of the association of NLR with the presence of MVI were performed based on different countries. To assess the stability of results, a sensitivity analysis was performed by omitting one study each time through influence analysis. Publication bias was evaluated with funnel plots and Egger’s test. For all the analyses, P ⩽ 0.05 was considered as significant.
Results
Search results, study characteristic, and quality assessment
Our search strategy yielded 953 studies, and an additional study was included from the reference review (Figure 1). Of the 954 studies, 32 were considered to have potential value and the full text was scanned. Among the 32 studies, 17 were further excluded for the following reasons: data repeatability (n=3), no preoperative NLR level reported (n=3), and review or comments (n=11). Finally, we identified 15 studies, all published between 2008 and 2018, which met the inclusion criteria.16-30
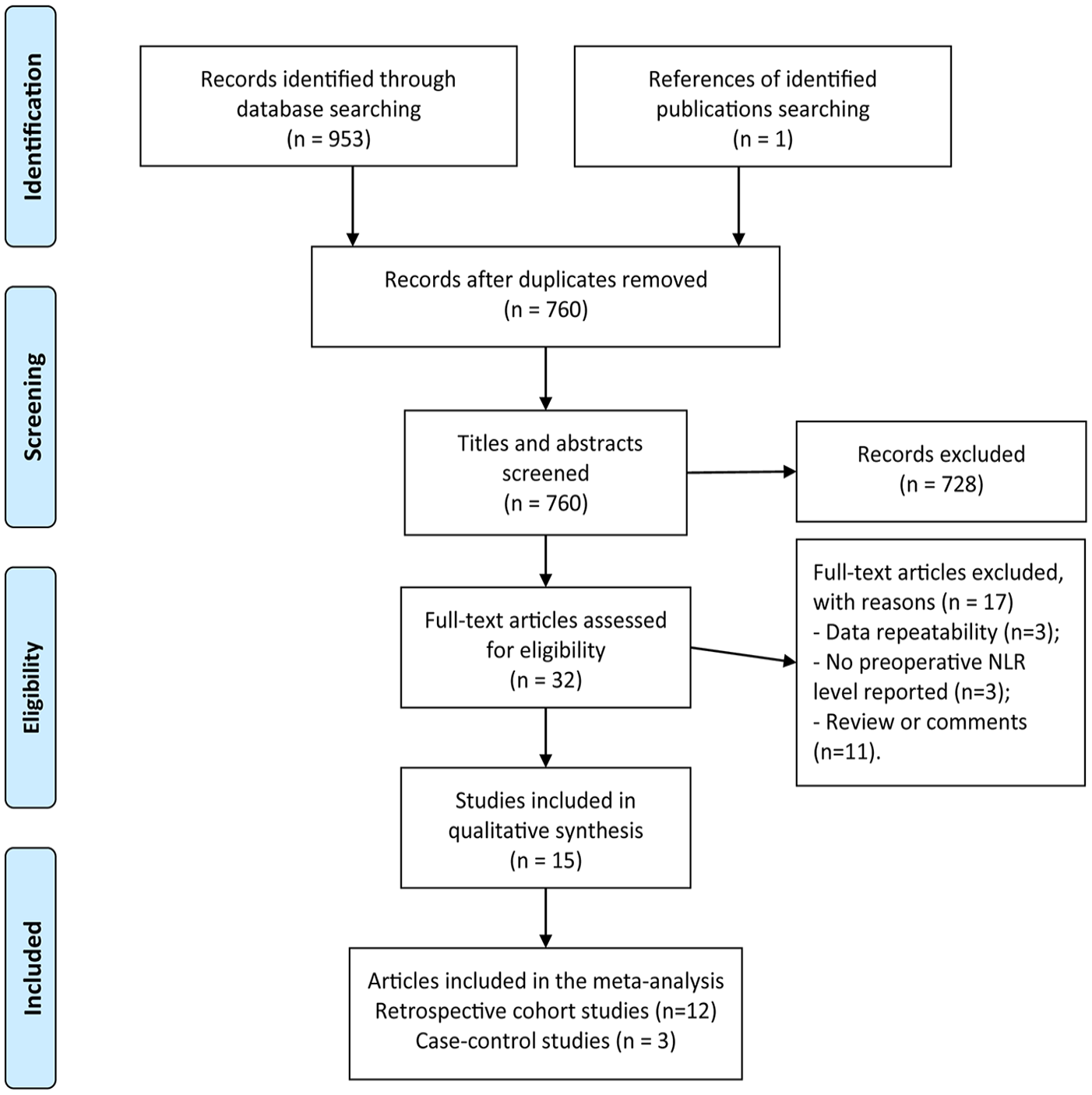
Literature search and filtering of studies.
Of the 15 studies, 12 were retrospective cohort studies16-22, 24-27, 29 and three were case-control studies23,28,30 (Table S2). Among the 12 cohort studies, nine were from China, one from England, one from Korea and one from Thailand. Among the three case control studies, two were from China and one from the United States. The sample size varied from 96 to 1135. Three studies did not describe the proportion of sex and age in high and low NLR groups.
The quality scores of each study are summarized in Table S3. Eleven studies were deemed of high quality (seven or more stars) and only four studies with six stars were deemed moderate. The median score was seven for case-control studies and cohort studies.
Preoperative NLR level and MVI risk
Twelve studies including 5116 patients reported the relationship between preoperative NLR level and vascular invasion.16-22,24-27,29 Considering the moderate heterogeneity (I2 = 43%, P = 0.05), we used a random model. The pooled data showed that more HCC patients were complicated by vascular invasion in the high NLR group than in the low NLR group (OR 1.74; 95% Cl 1.42, 2.12; P < 0.001) (Figure 2(a)). Of the 12 studies, only 7 clearly reported the association between the preoperative NLR level and MVI.17,19,20,22,25-27 The analysis of these seven studies arrived at a consistent conclusion (OR 1.62; 95% Cl 1.39, 1.89; P < 0.001) with a less heterogeneity (I2 = 38%; P = 0.14) (Figure 2(b)). Among the seven studies, five were from China, one from Thailand, and one from Korea. Subgroup analysis did not change the conclusion in China (OR 1.62; 95% Cl 1.24, 2.13; P < 0.001) (Figure 2(c)).

Forest plot based on retrospective cohort studies. (a) Pooled data of preoperative NLR level and risk of vascular invasion. (b) Pooled data of preoperative neutrophil-lymphocyte ratio (NLR) level and risk of microvascular invasion (MVI). (c) Pooled data of preoperative NLR level and risk of MVI in China.
Three studies including 1162 patients reported the preoperative NLR level in MVI positive and negative groups.23,28,30 We pooled the trials using a fixed effects model (P = 0.15; I 2 = 47%). There were higher preoperative NLR levels in the MVI-positive group than in the MVI-negative group (OR 0.62; 95% Cl 0.35, 0.90; P < 0.001) (Figure 3(a)). Of the three studies, two are from China and one is from the United States. A subgroup analysis also showed a higher preoperative NLR level in the MVI-positive group compared with the MVI-negative group (OR 0.85; 95% Cl 0.49, 1.21; P < 0.001) (Figure 3(b)).

Forest plot based on case-control studies. (a) Pooled data of preoperative NLR level and risk of MVI. (b) Pooled data of preoperative NLR level and risk of MVI in China.
Sensitivity analyses
Sensitivity analysis was performed to examine the stability and reliability by excluding one study each time. The results indicated that the pooled ORs and MDs were not significantly influenced by omitting any single study (Figure 4(a) to (c)).
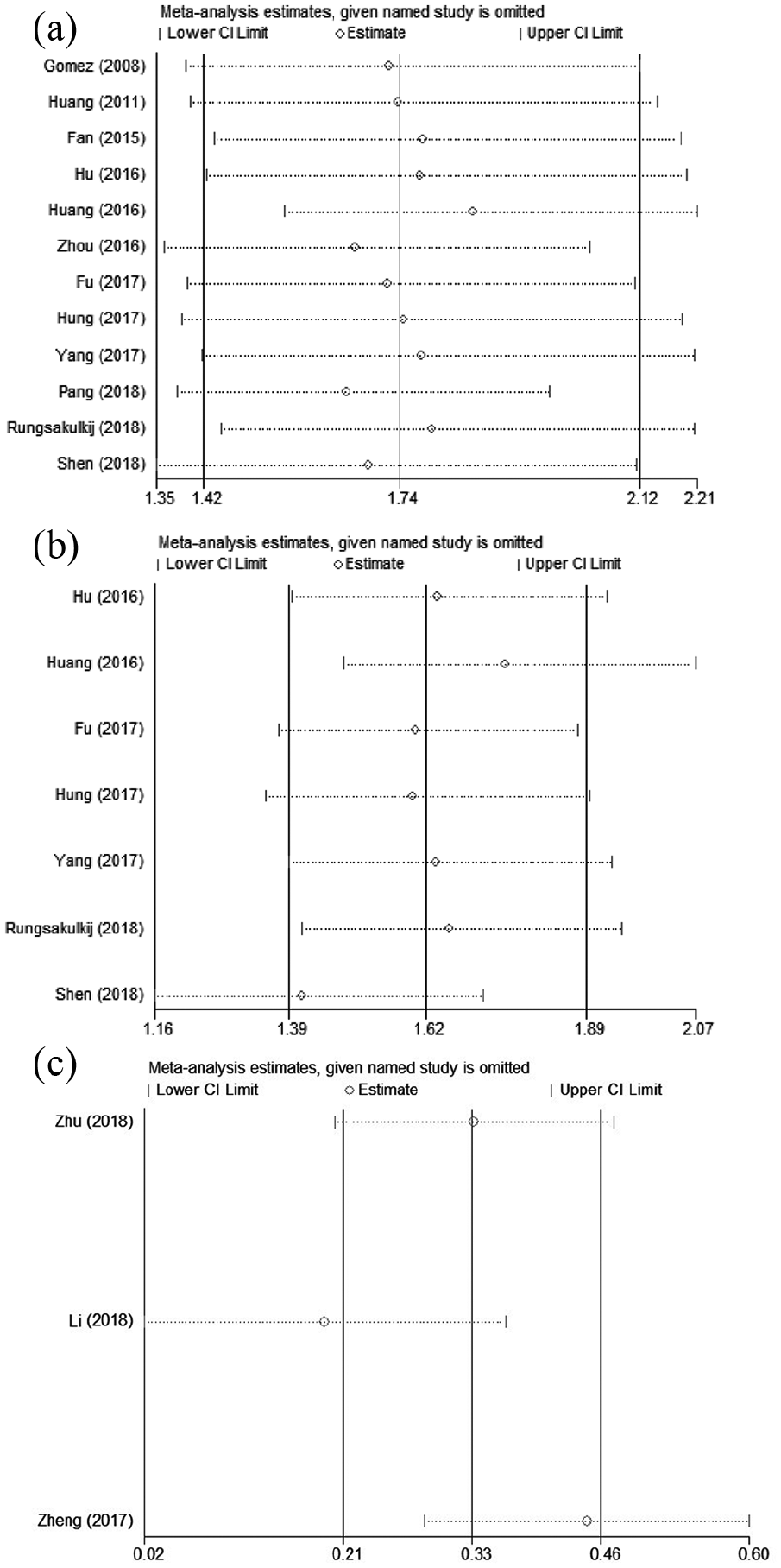
Sensitivity analysis. (a) Sensitivity analysis of preoperative NLR level and risk of vascular invasion based on retrospective cohort studies. (b) Sensitivity analysis of preoperative NLR level and risk of MVI based on retrospective cohort studies. (c) Sensitivity analysis of preoperative NLR level and risk of MVI based on case-control studies.
Publication bias
The funnel plot did not show any obvious asymmetry for the comparison between the preoperative NLR level and vascular invasion (Figure 5). Egger’s test also showed no evidence of publication bias (P = 0.847). Egger’s tests—but not funnel plots—are recommended to be used when the number of studies in a meta-analysis is fewer than 10. There was no publication bias on Egger’s test in the comparison between preoperative NLR level and MVI (P = 0.481). Besides, no publication bias was found in the comparison of preoperative NLR level between the MVI-positive and -negative groups (P = 0.854).
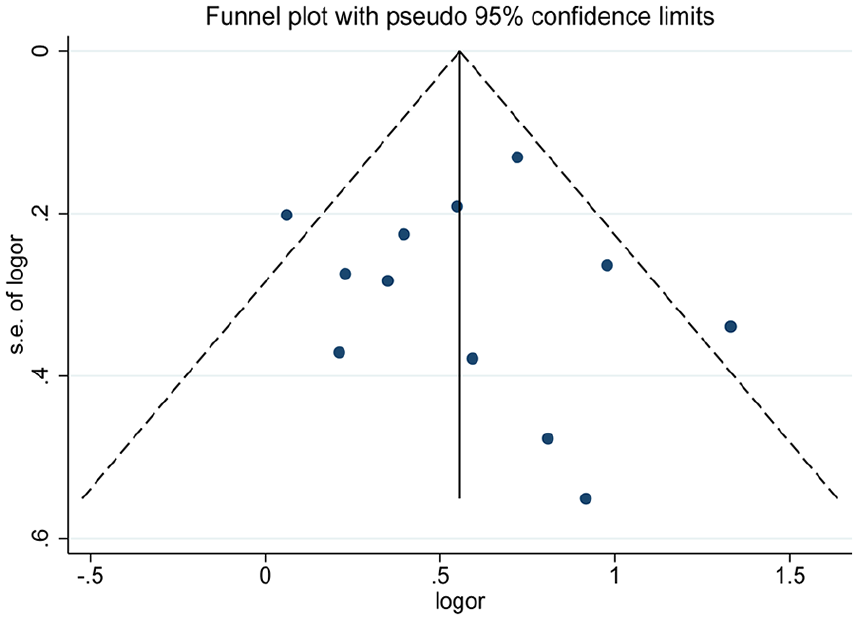
The funnel plot of preoperative NLR level and risk of vascular invasion based on retrospective cohort studies.
Discussion
MVI was reported to be associated with HCC invasiveness and metastasis. 6 For a long time, the significance of MVI has been underestimated, partly because MVI was regarded as a mild form of macrovascular invasion and the diagnosis of MVI only depends on the postoperative histopathological examination.3,31 With increasing understanding, MVI has become a hot topic in HCC. The ability of MVI not only helps to predict the poor prognosis but also helps with clinical decision making before surgery. For example, the absence of MVI is a precondition of up to seven criteria of liver transplantation. 8 Besides, patients with MVI benefit more from anatomical liver resection and wide surgical margin.7,10 Thus, discovering the predictive indictors for MVI is significant for the estimation of the presence of MVI preoperatively.
NLR has been recognized as an easily available marker of systematic inflammation response. 32 Elevated NLR has been reported to be associated with poor prognosis in many cancers.4,33-37 In the past decade, the role of preoperative NLR level in the development of MVI in HCC has been increasingly recognized. However, the conclusions have not been consistent. In this meta-analysis, by analyzing the 12 retrospective cohort studies, we concluded that there were more HCC patients with vascular invasion in the high NLR group than in the low NLR group. Considering that 7 out of the 12 studies reported the relationship between preoperative NLR level and MVI, we analyzed the 7 studies and yielded consistent results. Heterogeneity decreased but still existed (from I2 = 43% P = 0.05 to I2 = 38% P = 0.14). Subgroup analysis did not change the conclusion in China while there was still moderate heterogeneity (I2 = 52%; P = 0.08). Of the three case-control studies, the preoperative NLR level was higher in the MVI-positive group compared with the MVI-negative group. Subgroup analysis confirmed the conclusion in China with less heterogeneity (from I2 = 47%, P = 0.15 to I2 = 0%, P = 0.78). In short, by analyzing the cohort and case-control studies, we demonstrated that a high preoperative NLR level was significantly associated with an increased risk of MVI. Subgroup analysis yielded similar results in China.
The mechanism by which a high preoperative NLR level is associated with the presence of MVI has been not investigated. A possible explanation is that higher NLR is an objective reflection of inflammation. Some proinflammatory cytokines, such as TNF and IL-6, can activate the transcription factors NF-κB and STAT3, which have been reported to accelerate the development and progression of HCC.38,39 Also, chronic inflammation can affect the tumor micro-environment, which is one of the factors involved in vascular invasion. 40
Our study is the first meta-analysis to analyze the relationship between the preoperative NLR level and the risk of MVI. Through the analysis of subgroup, sensitivity, and publication bias, our conclusion appears stable and consistent. Undeniably, our study had several limitations. First, the cutoff of NLR is different in individual studies and our analysis cannot determine the best cutoff. Second, many other inflammatory indictors exist, such as platelet-lymphocyte ratio and lymphocyte-monocyte ratio in the clinic, while we just focused on the relationship between the preoperative NLR level and the risk of MVI. More studies analyzing all the inflammatory indicators are needed. Finally, the studies included in our meta-analysis were mainly from China. We could not demonstrate whether the conclusion was consistent in other countries.
In conclusion, this meta-analysis demonstrated that a higher preoperative NLR level was positively associated with the risk of MVI. However, considering that most of the studies were from China, the conclusion should be considered with caution for other countries. Further well-designed, large, prospective studies are needed to confirm this assessment and to establish the potential dose-response relationship between the preoperative NLR level and the MVI grade.
Supplemental Material
supplementary_materials – Supplemental material for Preoperative neutrophil-lymphocyte ratio predicts the risk of microvascular invasion in hepatocellular carcinoma: A meta-analysis
Supplemental material, supplementary_materials for Preoperative neutrophil-lymphocyte ratio predicts the risk of microvascular invasion in hepatocellular carcinoma: A meta-analysis by Furong Zeng, Bin Chen, Jiling Zeng, Zhiming Wang, Liang Xiao and Guangtong Deng in The International Journal of Biological Markers
Footnotes
Author contributions
Furong Zeng and Bin Chen contributed equally to this work.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.