
Abstract
Introduction:
Serum carcinoembryonic (CEA) antigen is used as a diagnostic screening tool during follow-up in colorectal cancer patients. However, it remains unclear whether preoperative serum CEA is a reliable marker in the follow-up to predict recurrence. The aim of the study is to determine the value of elevated pre- and postoperative serum carcinoembryonic antigen levels (CEA > 5 µg/L) as an independent prognostic factor for locoregional and distant recurrence in patients who underwent curative surgery for colorectal cancer.
Methods:
This single center retrospective observational cohort study includes patients who underwent curative surgery for colorectal cancer between 2005 and 2015 and had pre- and postoperative serum CEA measurements. Five-year disease-free survival and multivariate Cox regression analyses were performed to adjust for confounding factors.
Results:
Preoperative serum CEA level was measured in 2093 patients with colorectal cancer. No significant association was found between an elevated preoperative serum CEA and locoregional recurrence (adjusted hazard ratio (HR) 1.29 (95% confidence interval (CI) 0.91, 1.84; P=0.26)). However, a significant association was found between an elevated preoperative serum CEA and systemic recurrence (adjusted HR 1.58 (95% CI 1.25, 2.00; P<0.01)]. The five-year disease-free survival was lower in patients with elevated preoperative serum CEA levels (P<0.01). Postoperative serum CEA level was the most sensitive for hepatic metastases during follow-up (73.3%).
Conclusions:
The preoperative serum CEA level is an independent prognostic factor for systemic metastasis after curative surgery for colorectal cancer in patients with stage I–III disease. The level is the most sensitive for hepatic metastasis compared to metastasis to other anatomic sites.
Introduction
Serum carcinoembryonic (CEA) is a set of glycoproteins involved in cell adhesion. 1 CEA levels can be elevated not only in patients with malignancies, such as colorectal cancer (CRC), but also in patients with breast, lung, and pancreatic cancer. Increased levels of CEA are also detected in patients with chronic renal failure, colitis, diverticulitis, and pneumonia, and in smokers.2,3 In most patients who are diagnosed with CRC, CEA blood levels are elevated and tend to decrease after successfully curative surgery and/or adjuvant treatment. Elevated preoperative serum CEA levels have been found to be associated with poor oncologic prognosis in patients with CRC.4-11 An early study on CEA showed an association between tumor stage and elevated CEA. On the other hand, there is an inverse relationship between CEA levels and tumor grade: well-differentiated tumors tend to produce more CEA than poorly differentiated tumours. 12 CEA has no value in screening for bowel cancer as the positive predictive value is too low. 13 However, measuring CEA during postoperative follow-up is common because CEA levels may rise with cancer recurrence, which is important for early detection, treatment at a curable stage, and therefor to improve survival.14,15 In the Netherlands, the follow-up program for CRC consists of a physical examination, imaging with an abdominal ultrasound and chest x-ray and serum testing for the tumor marker CEA. 16 International guidelines recommend measuring CEA in intervals of 3 to 6 months after surgical treatment for CRC.17-21 When CEA levels are elevated, further investigation is indicated typically with a computed tomography (CT) scan of the chest, abdomen and/or pelvis, or a positron emission tomography (PET)-CT scan. Some authors suggest that CEA levels appear to be the most sensitive for identifying hepatic and retroperitoneal located metastases and the least sensitive for local recurrence and peritoneal or pulmonary metastases.22-24 Therefore, during the follow-up period, CEA is used as a diagnostic screening tool; when the CEA blood level is elevated, the physician is alerted to initiate further investigation through imaging.17,25 Given the inconsistencies of CEA levels between tumor stage and tumor grade, it remains unclear if preoperative serum CEA levels provide accurate information regarding locoregional and distant recurrence during follow-up. The main aim of this study was to evaluate the role of preoperative CEA levels as an independent predictor for locoregional and systemic recurrence in patients who previously underwent curative surgery for CRC. The secondary aim was to determine the role of postoperative serum CEA level measurement during follow-up in patients who had undergone curative surgery for CRC.
Materials and methods
This is a single center retrospective observational cohort study of patients with CRC. Data of patients who underwent curative surgery between January 2005 and December 2015 were retrospectively reviewed. Data of CRC patients between 2005 and 2010 were assembled by the surgical team. Data of patients who underwent surgery in the Amphia Hospital for CRC between 2011 and 2015 were retrieved from the National Cancer Registration Centre (Integraal Kanker Centrum Nederland, IKNL). Demographic data and data regarding surgery (type of resection and location) were obtained from medical charts. Preoperative serum CEA levels and CEA levels at the time of diagnosis of cancer recurrence were retrieved. Before July 2015, all CEA samples were analyzed with the Siemens Immulite® 2000 CEA assay (Siemens Healthcare Diagnostics Ltd, Llanberis, Wales). After July 2015, all CEA samples were analyzed with the Roche Diagnostics CEA Elecsys® cobas e601 (Roche Diagnostics Ltd, Rotkreuz, Switzerland). Method comparison showed that the two methods agree, with nonsignificant bias between them (data not shown). Serum CEA levels between 0 and 5 µg/L were considered as normal. Pathology results were retrieved to obtain tumor grade and whether a radical resection of the tumor was achieved (R0 resection). Pathological classification was based on the fifth edition of the tumor-node-metastasis (TNM) classification. 26 All patients with recurrent disease were confirmed with histological examination whenever possible, or otherwise by diagnostic imaging or with surgery. Locoregional recurrence was defined as tumor growth inside (luminal) or outside the colonic/rectal wall, which can extend through the wall to cause perforation and/or invasion of adjacent organs or structures. 27 Recurrences in other anatomic sites were defined as systemic recurrence or distant metastases. Patients were followed up every 3 to 6 months for 5 years by the surgeon. Each follow-up visit included a physical examination, a CEA blood level, an ultrasound of the abdomen, and a chest x-ray. A chest CT, abdominopelvic CT, or PET-CT scan was performed when there was high suspicion of recurrence of disease on routine studies. Colonoscopy surveillance was performed approximately 1 year after curative resection and 3 years after the first postoperative colonoscopy. In case of incomplete preoperative visualization of the colon, a completing colonoscopy was performed within 3 months postoperatively. Date of death was confirmed in the Dutch Municipal Personal Records Database (Gemeentelijkebasisadministratie persoonsgegevens, GBA with their software program CompeT&TEindhoven) using the patient’s social security number.
Inclusion and exclusion criteria
Patients were included if they underwent colorectal surgery for a malignancy between 2005 and 2015. Patients were excluded if they had an oncologic resection of an appendix carcinoma or pseudomyxoma peritonei (PMP). Patients were also excluded when they had surgery for palliative purposes (palliative resection or debulking, palliative bypass, and palliative colostomies/ileostomies because of obstructing symptoms). Patients with no preoperative serum CEA measurements were also excluded.
Ethical approval
Ethical approval was obtained from the National Institutional Review Board Medical Research Ethics Committees United (MEC-U). Official approval of this study by the MEC-U was not required because the Medical Research Involving Human Subject Act under the wet medisch-wetenschappelijk onderzoek (WMO) does not apply to this study (reference number W17.073). The Institutional Review Board of Amphia Hospital (AMOA) confirmed that no formal written waiver for an ethics approval was required.
Statistics
The Kolmogorov–Smirnov test was used to determine if the data were normally distributed. Data were depicted as the mean and SD for normally distributed data, and median and interquartile range (IQR) for non-normal distributions. The χ2 test was used to compare categorical variables. Five-year disease-free survival analysis was performed with Kaplan–Meier curves for elevated and non-elevated preoperative serum CEA levels. The log-rank test was used to test statistical outcomes between these two groups. Cox proportional hazard models were used to estimate independent effect of covariates on locoregional and distant recurrence as measured by adjusted hazard ratio (HR) with a 95% confidence interval (CI). Variables that were statistically significant in the univariate Cox regression and/or had clinical relevance were included in the multivariate analysis. A two-sided P-value of less than 0.05 was used to indicate statistical significance. All data analyses were performed with IBM SPSS Statistics Program, version 24.
Results
Between 2005 and 2015, 2704 patients underwent oncologic colorectal surgery. Of this patient group, 284 patients were excluded. A total of 2420 patients underwent curative resection for CRC and 327 patients were excluded because of the absence of preoperative serum CEA measurements. The remaining 2093 patients were eligible for analysis (Figure 1). The median age was 69 years (IQR 62–76) and 1209 of them were male (57.8%, Table 1). Median follow-up duration was 43 months (IQR 24–76).
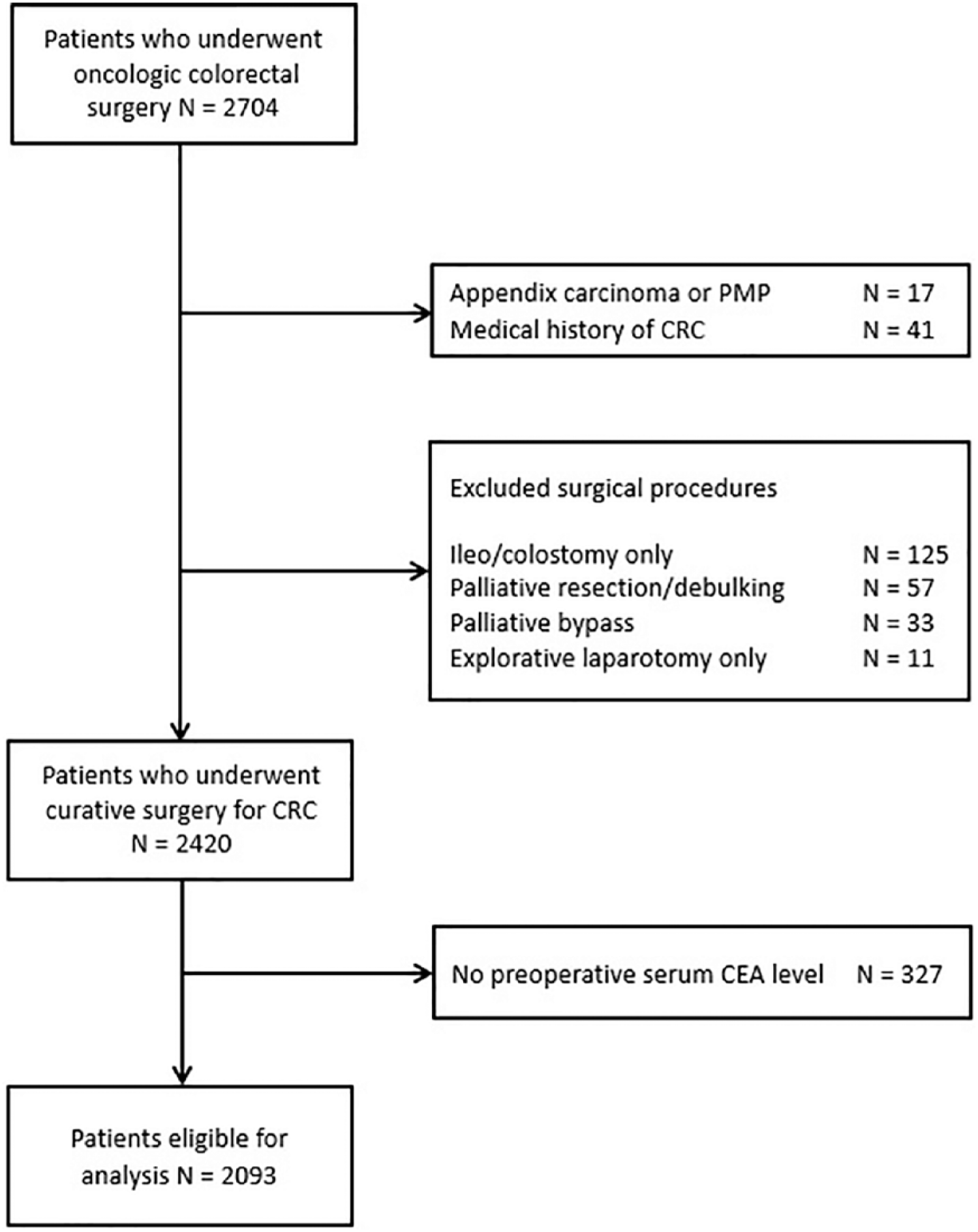
Flowchart of included patients who underwent curative surgery for CRC and had preoperative serum CEA level measurements.
Clinicopathologic characteristics of patients with normal (⩽ 5 µg/L) and elevated (> 5 µg/L) preoperative serum CEA concentrations.
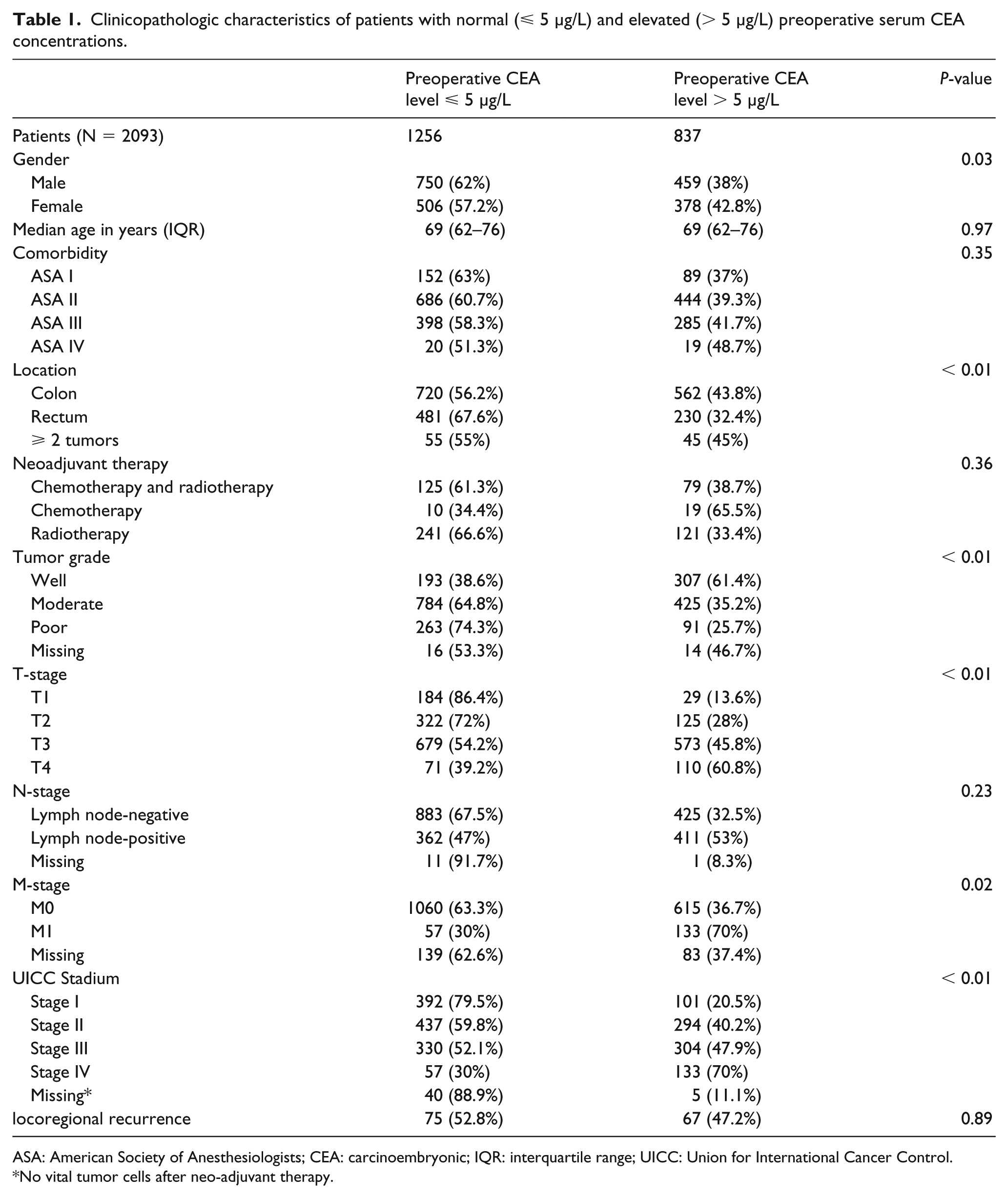
ASA: American Society of Anesthesiologists; CEA: carcinoembryonic; IQR: interquartile range; UICC: Union for International Cancer Control.
No vital tumor cells after neo-adjuvant therapy.
Preoperative serum CEA
Preoperative serum CEA was elevated in 837 patients (40%), which corresponds to the sensitivity of the tumor marker for detecting CRC. Of the 2093 patients, 190 (9.1%) had distant metastases at the time of diagnosis (M1) (Table 1). Of these patients with M1 disease at presentation, 133 patients had preoperative serum CEA levels greater than 5 µg/L, and 57 patients had CEA levels less than 5 µg/L. The median CEA level was 11 µg/L (IQR 4.1–38.5 µg/L) in this M1 group. Of the 1903 patients without metastases at the time of diagnosis (M0), 704 patients had CEA levels greater than 5 µg/L, and 1199 patients had CEA levels less than 5 µg/L. The median CEA level was 3.4 µg/L (IQR 1.9–7.9 µg/L) in the M0 group. The overall sensitivity and specificity of CEA in detecting metastasis at the time of diagnosing of CRC were 70% and 63%, respectively. In 25.7% of patients with a tumor with poorly differentiated cells, the CEA level was >5 µg/L; the CEA level was elevated in 35.2% of patients with moderate differentiation and in 61.4 % of patients with well-differentiated tumors (Table 1).
Recurrence
Of the 2093 patients who underwent curative surgery for CRC, 142 (6.8%) developed locoregional recurrence during follow-up with a median time to recurrence of 11 months (IQR 6–18 months). There were 1903 patients with stage I–III disease, and 336 (19.1%) of them developed systemic recurrence during follow-up. The median time to systemic recurrence was 12 months (IQR 5–24 months). The median time between a CEA increase and the actual confirmation of cancer recurrence through histologic examination or diagnostic imaging or with surgery was 12 days (IQR 10–14). In the univariate analysis, an elevated preoperative serum CEA was associated with locoregional recurrence (hazard ratio (HR) 1.47 (95% confidence interval (CI) 1.06, 2.04; P=0.02)). However, in the multivariate analysis, no significant association between preoperative serum CEA and locoregional recurrence was found (adjusted HR 1.29 (95% CI 0.91, 1.84; P = 0.26)). Covariates with a significant association with locoregional recurrence were poorly differentiated tumors, T-stadium, tumor stage, and tumors that were not radically removed. In contrast to locoregional recurrence, there was a significant association between an elevated preoperative serum CEA level and systemic recurrence in patients with stage I–III disease. This finding was significant in the univariate analysis (HR 1.97 (95% CI 1.58, 2.45; P<0.01)) and confirmed in the multivariate analysis (adjusted HR 1.58 (95% CI 1.25, 2.00; P<0.01)). In addition, rectal tumors, T-stadium, nodal stage, surgical approach, tumor-stage, and tumors not radically removed were significantly associated with distant recurrence (Table 2). The 5-year disease-free survival was significantly lower in patients with an elevated preoperative serum CEA level than in those without (P<0.01, Figure 2).
Multivariate Cox regression analysis of locoregional and systemic recurrence in patients who underwent curative surgery for colorectal cancer.
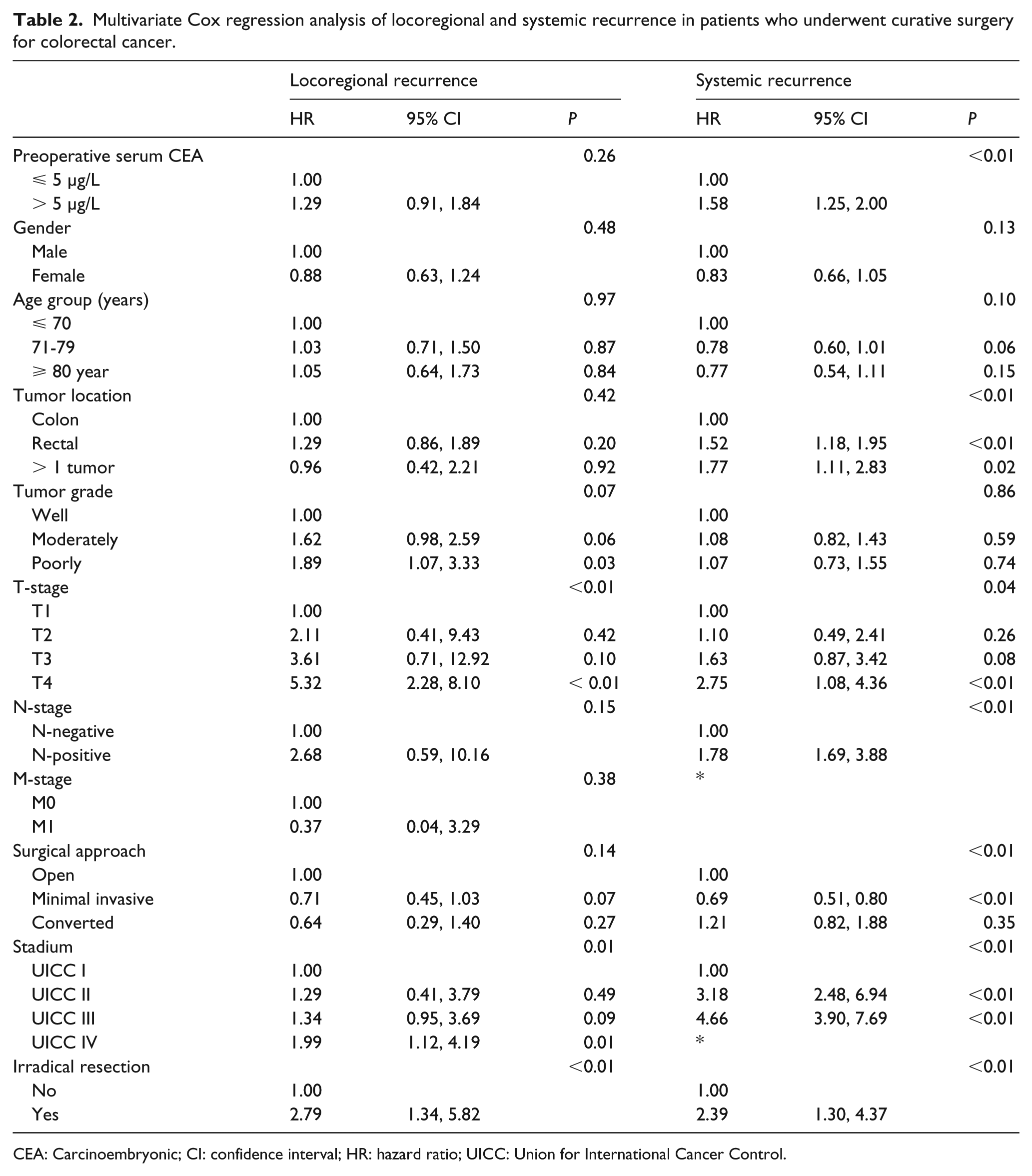
CEA: Carcinoembryonic; CI: confidence interval; HR: hazard ratio; UICC: Union for International Cancer Control.
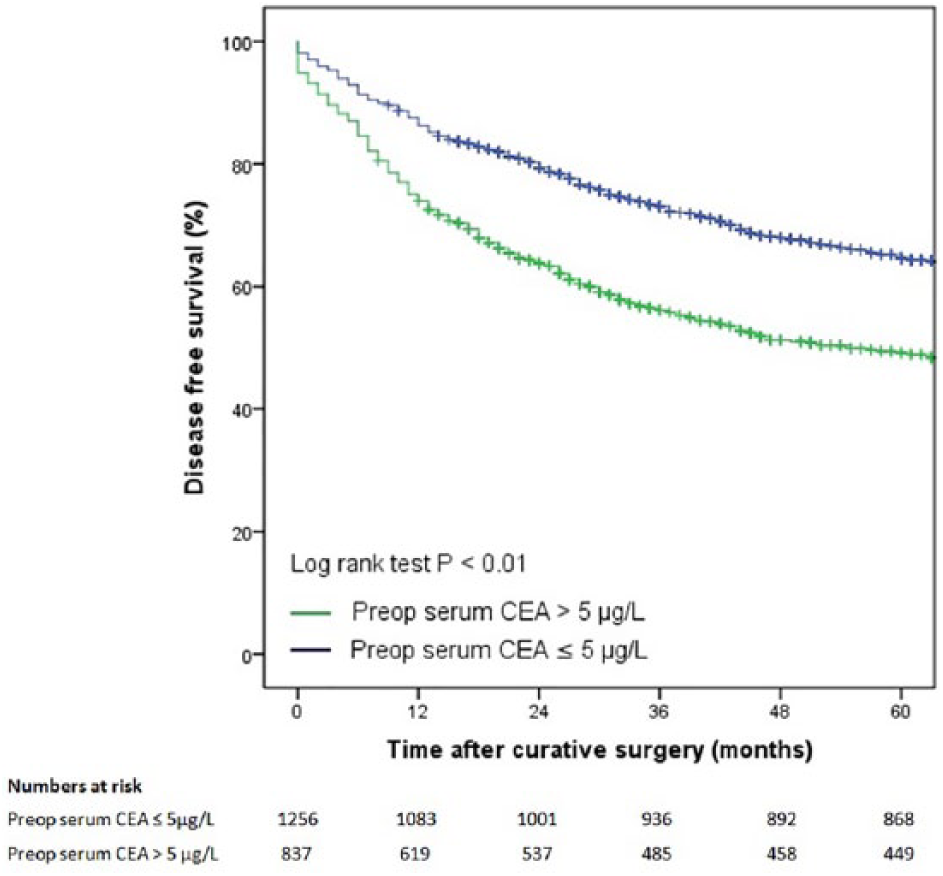
Five-year disease-free survival of patients with and without elevated preoperative serum CEA levels.
CEA during follow-up
Follow-up CEA was elevated in 95 of 142 patients with locoregional recurrence (66.9%).
The median CEA level of patients with locoregional recurrence was 9.1 µg/L (IQR 4.9–13.3 µg/L). Follow-up serum CEA levels were measured in 332 of the 336 patients with stage I–III disease who developed systemic metastasis. Follow-up CEA was elevated in 121 of 165 patients with hepatic metastasis. The sensitivity of CEA levels in detecting hepatic metastasis was 73.3%. The median serum CEA level was the highest for hepatic metastasis and the lowest for pulmonary metastasis (Table 3.)
Follow-up serum CEA measurements in patients with stage I–III disease who developed locoregional or systemic recurrence.
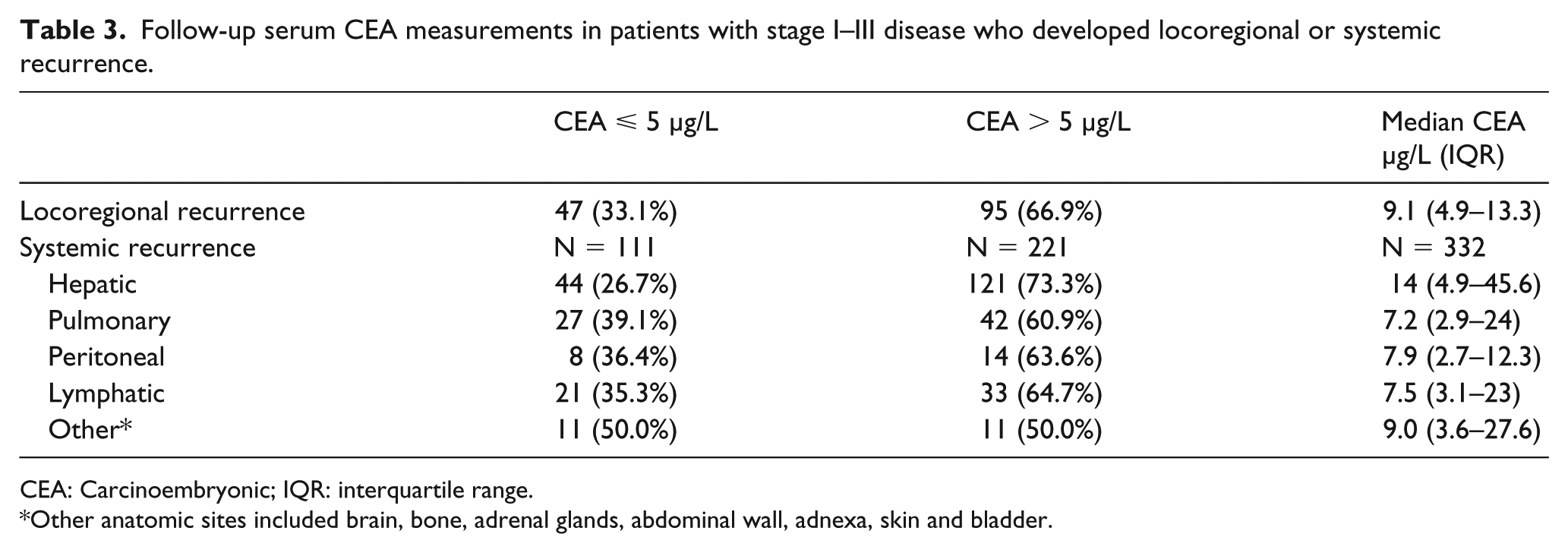
CEA: Carcinoembryonic; IQR: interquartile range.
Other anatomic sites included brain, bone, adrenal glands, abdominal wall, adnexa, skin and bladder.
Of the 1903 patients with stage I–III disease, postoperative serum CEA levels were measured in 1727 (90.8%) patients. An elevated CEA was found in 351 patients, but only 221 of them had distant metastasis confirmed with histological examination or by diagnostic imaging. The false positive rate for postoperative CEA measurements was 37.0% and the true positive rate was 63.0%. On the other hand, a normal CEA was found in 1376 patients during follow-up. In 111 of them, distant metastasis was found through imaging or with histological examination. The false negative rate for postoperative CEA measurement was 8.1% and the true negative rate was 91.9%.
Discussion
This single center retrospective observational study shows that the preoperative serum CEA level is not an independent prognostic factor for predicting locoregional recurrence. However, even after adjusting for confounding variables in the multivariate analysis, an elevated preoperative serum CEA level is a prognostic factor for systemic recurrence in patients who previously had curative surgery for CRC. Our findings confirm the results of previous studies, which also found that an elevated preoperative serum CEA level is a prognostic marker for poor oncological outcome.4,24,28-36 The sample size of these studies varied between 124 and 2230 patients, with only three studies with more than 1000 patients. Moreover, the definition of an elevated CEA ranged from 2.5 and 10 µg/L, leading to heterogeneity among these studies. The major inconsistency in the definition of an elevated CEA generates a broad range of values for the sensitivity and specificity of CEA as a preoperative diagnostic tool. In this study, a preoperative elevated CEA measurement of > 5 µg/L has a sensitivity of 40% for detecting CRC. Lowering this threshold would cause a higher rate of false positives. On the other hand, increasing the threshold would cause a higher rate of false negatives. Patients with an elevated preoperative serum CEA level have a decreased 5-year disease-free survival compared to patients with a normal preoperative serum CEA level. Takagawa et al. 36 also evaluated the prognostic value of preoperative serum CEA levels in 638 patients with CRC. They found a significant difference in disease-free survival with a threshold value of 10 µg/L. However, a significant difference was only observed in patients with stage II and stage III disease, whereas stage I only included six patients. 36 Our findings are similar for patients with stage I–III disease with a CEA threshold of 5 µg/L, which is used as a cut-off point in the Netherlands. 16 Park et al. 37 found similar results in a larger retrospective cohort of 212 patients with stage I CRC out of a total of 1236 CRC patients, although only 14 of 212 patients with stage I disease had elevated preoperative serum CEA levels. The only limitation of this study from South Korea is that they did not evaluate the value of postoperative serum CEA measurements for detecting recurrent disease. 35 Our database contained follow-up data regarding postoperative CEA levels in patients with systemic recurrence, which provides more comprehensive insight into the value of obtaining follow-up serum CEA measurements. Disease-free survival is also significantly lower in patients with stage II and stage III disease. 35 Patients with stage II or stage III disease and elevated preoperative serum CEA levels may have occult systemic disease at the time of curative surgery. Lloyd et al. 38 proved that 32.8% of patients with stage I and II disease test positive for disseminated tumor cells after surgery. Therefore, even after curative resection, residual malignant cells can remain in situ. 38 Several authors have attempted to determine the correlation between histological characteristics and vascular or perineural invasion.35,36 However, no convincingly significant differences have been found in these retrospective Asian studies. This study found a significant association between preoperative serum CEA level and tumor grade, which is consistent with previous reports. 12 In this study, an elevated preoperative serum CEA level was associated with systemic recurrence in patients with stage I–III disease. In the Netherlands, serum CEA monitoring is conducted every 3 to 6 months in the first 3 years and every 6 months thereafter until 5 years after the initial surgical treatment. 16 In some patients, it remains unclear how to interpret an elevated follow-up serum CEA level and its accuracy in detecting metastatic disease. It is also unclear whether postoperative CEA levels should be monitored in patients with recurrence who had normal preoperative serum CEA levels. In this cohort, 332 patients with stage I–III disease were diagnosed with distant metastases. In 221 of them, serum CEA was elevated during follow-up (66.5%), which appears to be an accurate indicator for further imaging. However, only 221 of the 351 patients with elevated follow-up serum CEA levels actually had distant metastases. Therefore 130 (37%) patients had false positive elevated serum CEA levels, causing unnecessary additional imaging, radiation exposure, and longer waiting lists. Along with serum CEA, information from the patient’s medical history and physical examination are needed to decide whether or not to perform additional imaging. A recently published randomized controlled trial (RCT) evaluated the role of CEA in predicting recurrence and outcomes of surgical treatment with curative intent. The Follow-up after Colorectal Surgery (FACS) trial concluded that CEA testing should not be used as a single triage test. 39 The correlation between follow-up elevated serum CEA levels and recurrence to distant sites has been reported, and is the greatest for hepatic metastases compared to metastases at other organs or structures.24,40 The results of the current study strengthen this finding. We found that 73.3% of patients with liver metastasis had elevated follow-up serum CEA levels. The serum level was not as sensitive for detecting distant metastases in other sites. Pulmonary metastasis and peritoneal metastasis had the lowest sensitivity rate of 60.9% and 63.6%, respectively, which is in line with previous studies.22-24 These findings indicate that postoperative serum CEA levels are more effective in predicting hepatic metastasis than for other types of metastases. There are also studies that suggest the benefit of an intensive follow-up schedule with more frequent CEA monitoring to improve survival in patients with hepatic metastasis.41-43
There are several limitations of the present study. First is the retrospective design, although we attempted to reduce this bias with a multivariate Cox regression analysis. Unfortunately, there were 327 (13.5%) patients with missing preoperative serum CEA measurements. This relatively large number of missing data points negatively influences the power of this study. One reason for the high number of missing preoperative serum CEA measurements is that a preoperative CEA measurement is not considered standard of care in the Dutch guidelines because of its low diagnostic value. The Dutch guidelines only recommend serum CEA monitoring in patients who enter a follow-up program to detect metastatic disease after curative surgery for CRC. 16 However, serum CEA is a minimally invasive diagnostic tool that provides information of a patient’s normal range of CEA while having active CRC, which is especially valuable during follow-up to monitor for CRC recurrence. A second limitation of the study concerns patients who presented with obstructive CRC and underwent emergency surgery. In these patients, the diagnosis of CRC is unclear until it is histologically confirmed; therefore, a preoperative serum CEA level is not typically measured in this specific patient group. In the near future, it is possible that physicians will have a more complete panel of clinical biomarkers in addition to CEA to obtain more information regarding prognosis and to guide treatment. Recently, advancements from molecular studies have provided the opportunity to test novel tumor markers. 44 Additional methods for authentication of new tumor biomarkers and multicenter RCTs are necessary.
In conclusion, in this large study cohort, we show that the preoperative serum CEA level is an independent prognostic factor for systemic recurrence but not for locoregional recurrence after curative surgery for CRC. Patients with hepatic metastasis are more likely to have elevated postoperative serum CEA levels than patients with metastasis involving other anatomic sites.
Footnotes
Acknowledgements
The authors would like to thank Dr. Marc Thelen (clinical chemist) and Dr. Judith M.A. Emmen (clinical chemist) for extracting pre- and postoperative serum CEA data from the database, and for providing technical information regarding both CEA assay methods of the Clinical Chemistry and Haematology Department (Amphia Hospital Breda, the Netherlands).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.