
Abstract
Background:
We report a case of prostatic carcinosarcoma, a rare variant of prostatic cancer, which is composed of a mixture of epithelial and mesenchymal components with a generally poor outcome.
Aims and methods:
We aim to identify molecular alterations, in particular copy number variations of AR and c-MYC genes, methylation and expression of glutathione S-transferase P1 (GSTP1), programmed death-ligand 1 (PD-L1), AR, and phosphorylated AR expression.
Results:
We found a distinct molecular pattern between adenocarcinoma and carcinosarcoma, which was characterized by high AR copy number variation gain; positive expression of PD-L1, AR, and phosphorylated AR; low espression of GSTP1 in epithelial component. The sarcomatoid component had a lower gain of the AR gene, and no expression of PD-L1, AR, phosphorylated AR, or GSTP1. Both components had a gain of c-MYC copy number variation.
Conclusions:
Our findings suggest that carcinosarcoma has specific molecular characteristics that could be indicative for early diagnosis and treatment selection.
Introduction
Carcinosarcoma is a rare type of prostate cancer, which is composed of a mixture of a high grade epithelial component (carcinomatous) and malignant mesenchymal or mesenchymal-like component (sarcomatous). 1 This cancer type often produces bladder obstruction with consequent urinary tract symptoms. 2 Carcinosarcoma has a very poor prognosis and about one-quarter of patients show metastasis at the time of diagnosis.3,4 Prostate-specific antigen (PSA) is often lower than expected considering tumor volume, 2 which complicates both the diagnosis and the monitoring of disease progression. Rodrigues et al. 5 have shown that three sarcomatoid carcinoma cases shared a TMPRSS2-ERG gene fusion with their paired adenocarcinomas, thus hypothesizing that carcinosarcoma originates from the epithelial type.
To the best of our knowledge, this is the first published study reporting genomic analyses on the principal of prostate-cancer-related biomarkers conducted on prostatic carcinosarcoma tissues. Beginning with literature data regarding prostatic adenocarcinoma, we selected the following important biomarkers for investigation in a sarcomatoid case: androgen receptor (AR) copy number and expression, 6 c-MYC copy number, 7 glutathione S-transferase P1 (GSTP1) methylation and expression 8 and programmed death-ligand 1 (PD-L1) expression. 9
Paraffin-embedded tissues from epithelial and sarcomatoid components of primary tumors and lymph nodal metastasis were analyzed for the above-mentioned markers.
Case description
A 79-year-old man who had been suffering from dysuria, macrohematuria and arterial hypertension for several months was seen at the Department of Urology of Morgagni-Pierantoni Hospital in Forlì. His PSA level was 8.89 µg/L. Ultrasound evaluation revealed a voluminous expanded mass extending into the bladder lumen; prostatic biopsies highlighted adenocarcinoma (Gleason score 4+5). The patient underwent cystectomy and prostatectomy. Histological examination revealed a malignant prostatic neoplasia with two main components: carcinomatous (acinar adenocarcinoma with different areas; Gleason score 4+5) and sarcomatous (leiomyosarcoma and osteosarcoma) (Figure 1). The tumor had spread to the periprostatic soft tissues, iliac lymph nodes, and presacral lymph nodes (pT4 N1 Mx). A thoracic and abdominal computed tomography scan with contrast medium was performed after surgical tumor removal; it showed a small pulmonary nodule (about 7 mm), a wide muscle-infiltrating, lytic iliac bone lesion, para-aortic adenopathies, and peritoneal carcinosis. The patient was treated with a combination of androgen deprivation therapy with leuprolide 22.5 every 3 months, and antiandrogen therapy with bicalutamide 50 mg/day orally for 6 months when radiological evaluation showed progressive disease. He was then treated with docetaxel for two cycles. Treatment was stopped because of rapid clinical progression, and palliative care was initiated. The patient died 3 months later.
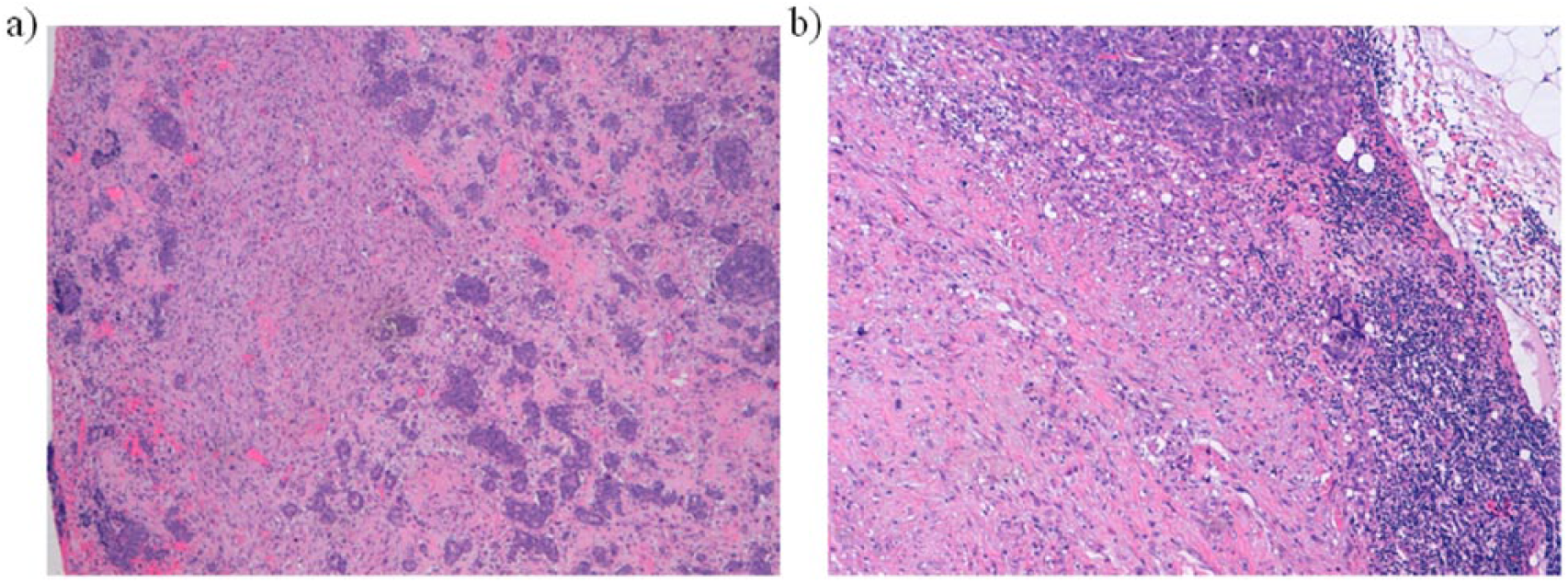
Hematoxylin and eosin staining of (a) adenocarcinoma and leiomyosarcoma; (b) lymph nodal metastasis with epithelial and leiosarcomatoid components.
Copy number variation analysis
After macrodissection of the different histological types, DNA was extracted using QIAamp DNA FFPE Tissue Kit (Qiagen, Milan, Italy), according to the manufacturer’s instructions. Copy number variation (CNV) analyses were performed by a duplex TaqMan real-time PCR assay (Applied Biosystems, Foster City, CA, USA) for the target genes (assays ID: AR=Hs04107225; c-MYC=Hs01764918) and the internal standard reference gene (RNaseP), using 10 ng of DNA. Three samples with benign prostatic diseases were used as internal calibrators. CNVs of AR and c-MYC genes were evaluated by the CopyCaller™ Software (Applied Biosystems). For c-MYC, values >2.5 were evaluated as amplification and <1.5 as deletion. For AR, we considered values >1.5 for amplification and <0.5 for deletion. Data were confirmed by Digital PCR QuantStudio® 3D System.
Immunohistochemistry
We manually performed immunohistochemistry using a rabbit monoclonal antibody of GSTP1 (anti-GST3/GSTp, Abcam, Cambridge, UK) at a dilution of 1:500 for 60 min incubation and a monoclonal antibody of androgen receptor (p Ser213- p Ser210) (Novus Biological, Littleton, CO, USA) at a dilution of 1:50 for 60 min. For PD-L1 samples were automatically processed using Benchmark XT Ventana instrument using clone SP142 (Spring), at a dilution of 1:30 and 60 min incubation.
Methylation-Specific Polymerase Chain Reaction
Sodium bisulfite conversion using EZ DNA Methylation-GoldTM kit (Zymo Research Corporation, Irvine, CA, USA) was used starting from 150 ng of FFPE DNA and 100 ng of LNCaP (methylated control) and from the peripheral blood of a healthy volunteer (unmethylated control). Real-time polymerase chain reaction (PCR) was performed using SYBR-GREEN master mix (Biorad, Milan, Italy) and primers specific for bisulfite-converted DNA. GSTP1 methylation status was determined by melt curve analysis as previously described. 8
Results
CNV
AR and c-MYC genes were both amplified in the primary tumor. AR was highly amplified (CNV=8) in the epithelial component and duplicated in the sarcomatous component (CNV=2). c-MYC was duplicated in both components. The epithelial component of nodal metastasis showed an amplification of AR and c-MYC similar to that obtained in the primary tumor (CNVs were 7 and 3, respectively). In contrast, the sarcomatous component had no gene copy number variation for either AR or c-MYC (Table 1).
Gene copy number variations and marker expression.
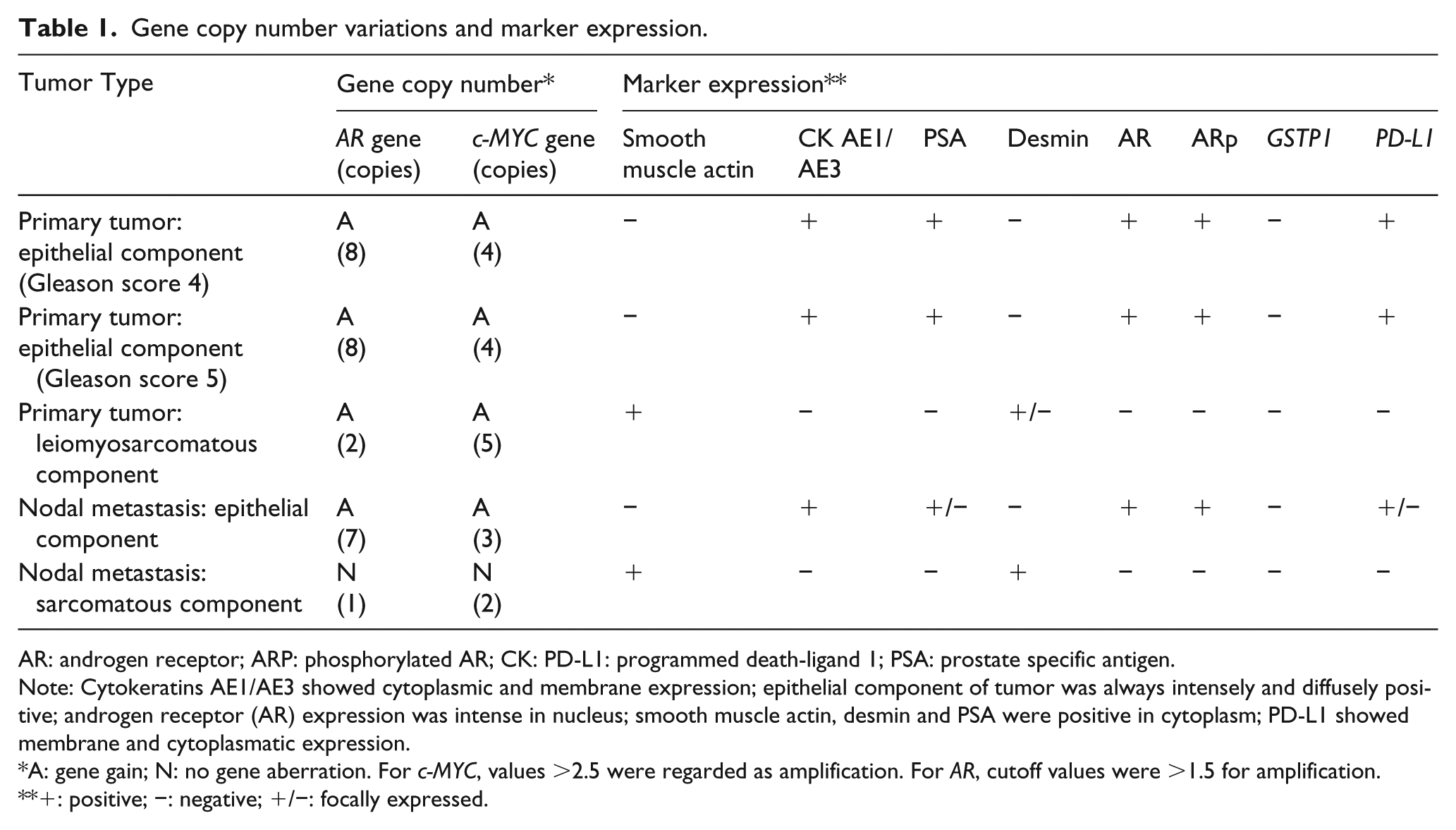
AR: androgen receptor; ARP: phosphorylated AR; CK: PD-L1: programmed death-ligand 1; PSA: prostate specific antigen.
Note: Cytokeratins AE1/AE3 showed cytoplasmic and membrane expression; epithelial component of tumor was always intensely and diffusely positive; androgen receptor (AR) expression was intense in nucleus; smooth muscle actin, desmin and PSA were positive in cytoplasm; PD-L1 showed membrane and cytoplasmatic expression.
A: gene gain; N: no gene aberration. For c-MYC, values >2.5 were regarded as amplification. For AR, cutoff values were >1.5 for amplification.
+: positive; −: negative; +/−: focally expressed.
Immunohistochemistry
Epithelial component of the primary tumor was cytokeratin AE1/AE3 positive, PSA positive, AR and AR phosphorylation positive, PD-L1 positive, actin smooth muscle negative, desmin negative and GSTP1 negative. The heterologous component of the tumor was represented by two different phenotypes that did not express AR, phosphorylated AR, GSTP1, PSA, or PD-L1. One was a more extensive leiomyosarcomatous component expressing widespread immunohistochemical positivity for smooth muscle actin and desmin, while the other was an osteosarcomatous component (recognizable by its bone matrix production) expressing no immunohistochemical marker. The lymph node metastasis showed the same different expression profiles in both epithelial and sarcomatous components (Table 1). Immunohistochemical results for GSTP1 expression, phosphorylated AR, and PD-L1 expression are reported in Figures 2 and 3.
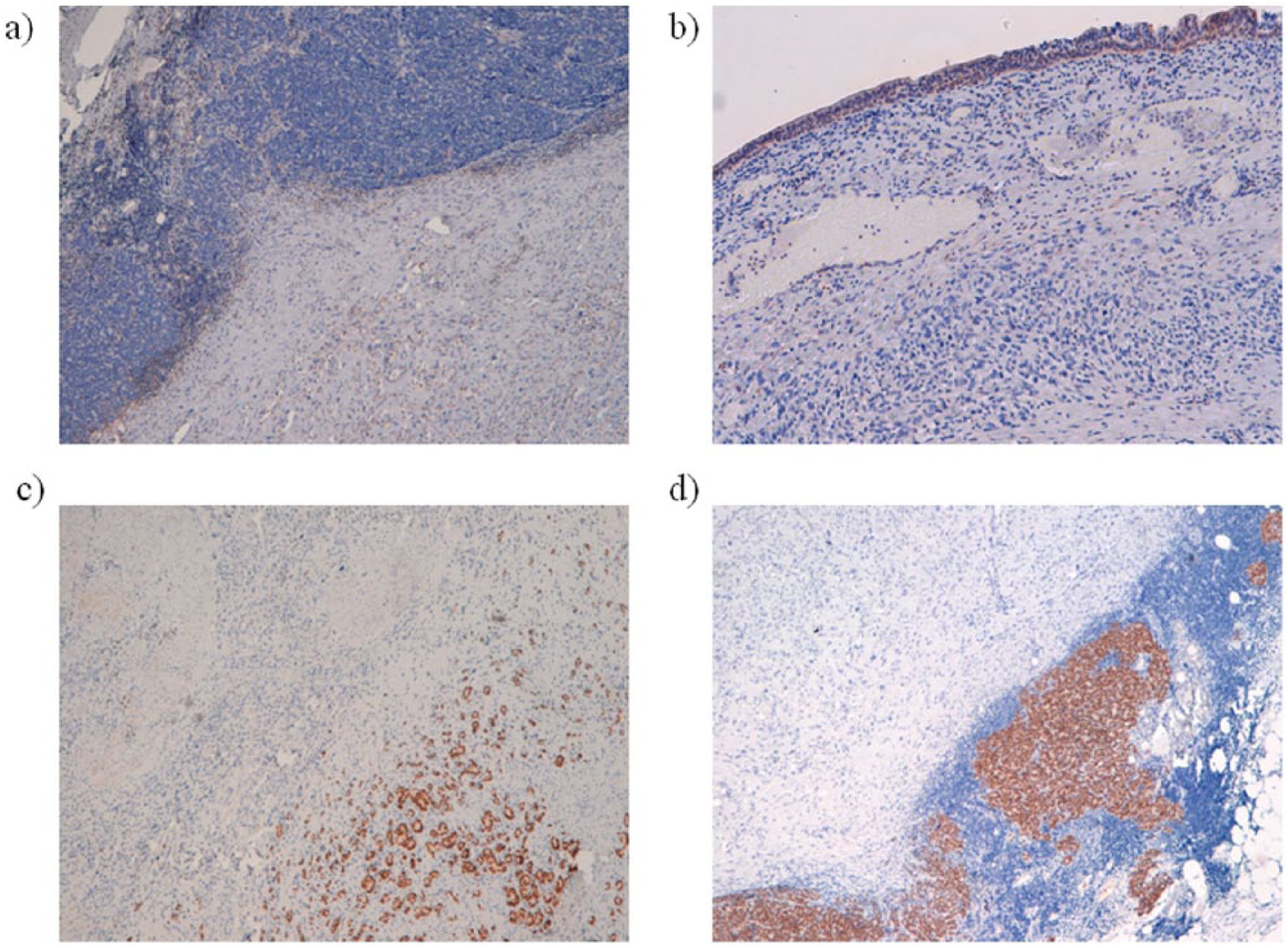
Immunohistochemical results for GSTP1 expression and phosphorylated AR (ARp). (a) Adenocarcinoma and leiomyosarcoma negative for GSTP1 staining. (b) Adenocarcinoma negative for GSTP1, healthy urothelial cells positive for GSTP1 staining. (c) Adenocarcinoma positive for ARp, leiomyosarcoma negative for Arp. (d) Lymph nodal metastasis: epithelial component positive for ARp, leiosarcomatoid component negative for ARp.
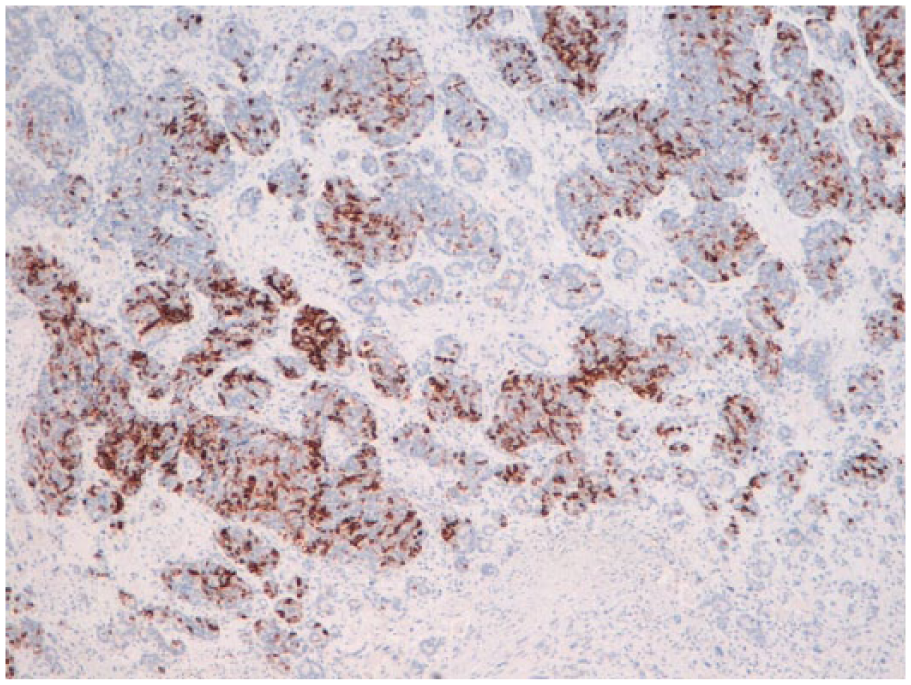
Immunohistochemical results for PD-L1 expression. PDL-1 is highly expressed in adenocarcinoma component.
GSTP1 methylation
GSTP1 was found methylated in both epithelial and sarcomatous components of primary tumor. Lymph nodal metastasis provided an insufficient yield of DNA to perform methylation-specific PCR analysis.
Conclusions
We demonstrated that the two components of carcinosarcoma (epithelial and mesenchymal-like) have different molecular alterations, which was also confirmed in lymph nodal metastases. In line with previously published papers 5 we showed the absence of AR and its phosphorylated isoform expression in the two sarcomatous components (primitive and lymph nodal metastasis). Despite their different phenotypes, the two components seem to share some molecular alterations leading to a unique cellular clone. Both adenocarcinoma and sarcoma have c-MYC gene gain and methylation, and consequent protein hypoexpression of the GSTP1 gene.
Our findings indicate that the methylation of GSTP1 could be a good diagnostic marker for sarcoma as a substitute for PSA, which is often negative in this type of tumor. Our results regarding AR and PSA expression suggest that androgen deprivation therapy could represent a failure. This indicates that, as the two components have many different molecular alterations, the main goal is to find a drug combination that can be effective against both component types.
AR gain is usually involved in the castration-resistant phase, and new drugs, such as enzalutamide or abiraterone, are demonstrated to effectively increase overall survival of patients with castration-resistant prostate cancer. 10 Considering that AR gain was detected in both epithelial and sarcomatous components, we hypothesize that this patient was unlikely to receive any benefit from either enzalutamide or abiraterone, as previous studies suggested. 6 We also observed PD-L1 expression only in the epithelial component, but not in the sarcomatous component. However, given that some cancer patients benefit from anti PD-L1 drugs even in the absence of PD-L1 expression in the primary tumor, carcinosarcoma patients could potentially receive this therapy.
This study reports a single case and our observations are hypothesis generating. Further studies on molecular characterization are needed to better understand this type of tumor and to find new potential targets for therapy.
Footnotes
Acknowledgements
The authors thank Laura Lotito for editorial assistance.
Author contributions
Samanta Salvi and Valentina Casadio contributed equally to this work.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.