
Abstract
Purpose:
Chondrosarcoma is a malignancy affecting cartilage and is chemo- and radio-resistant. Novel immune checkpoint inhibitors may play a role in treatment; however, expression of programmed cell death ligand 1/2 (PD-L1/PD-L2) in chondrosarcoma is unreported.
Methods:
Chondrosarcoma sections were collected and stained immunohistochemically for PD-L1, PD-L2, Ki-67, and TP53. Clinicopathological parameters were collected and analyzed statistically for associations and correlations. PD-L1/PD-L2 positivity was designated using 1% and 5% cutoffs, respectively.
Results:
A total of 59 chondrosarcoma samples excised between 1997 and 2017 were collected. There were 40 samples assessed as PD-L1-positive and 25 samples as PD-L2-positive. In univariate analysis, PD-L1 positivity was significantly associated with younger age (P = .001), larger tumor (P = .025), advanced tumor grade (P < .001), and recurrence (P < .001). PD-L1 positivity was not associated with gender, location, serum level of lactate dehydrogenase, or serum level of alkaline phosphatase. PD-L2 positivity was solely significantly associated with younger age (P = .015). The associations were however insignificant in multivariate analysis. PD-L1 expression was significantly correlated with Ki-67 (P < .001) and TP53 (P = .02) expressions. PD-L2 expression was not correlated with either Ki-67 or TP53 expression. When grouped as combined expression (both negative vs. either positive), PD-L1/PD-L2 expression was associated with earlier recurrence (P < .001), and was negatively correlated with expression of Ki-67 (P < .001) but not with the expression of TP53.
Conclusion:
PD-L1/PD-L2 is positively expressed in chondrosarcoma and is associated with advanced clinical phenotype. PD-L1/PD-L2 expression is also associated with Ki-67 expression. Our results support the application of immune checkpoint blockade in chondrosarcoma.
Introduction
Chondrosarcoma (CHS) is a rare malignant tumor that produces cartilage matrix. The estimated overall incidence of CHS is 1 in 200,000 per year, and it is the third most frequent malignant bone tumor following multiple myeloma and osteosarcoma. 1 Low-grade, well-differentiated CHSs generally behave as slow-growing tumors, and patients with these tumors have a more favorable clinical course than those with high-grade CHSs. 2
As CHSs are resistant to radiotherapy and chemotherapy, the treatment of choice is radical surgery. 3 In some cases, it is impossible to perform surgical resection with sufficient margins because of the location of the tumor adjacent to neural, vascular, or visceral structures. The cause is of CHS remains unknown. Patients may have a history of enchondroma or osteochondroma. 4 A small minority of secondary CHSs occur in patients with Maffucci syndrome and Ollier disease. 5 Novel treatments are in urgent need and a newly emerged immune checkpoint inhibitor is promising.
The PD-1/PD-L1 pathway in cancer is implicated in tumors escaping immune destruction and is a promising therapeutic target. 6 The development of anti-PD-1 and anti-PD-L1 agents marks a new era of immunotherapy for cancer. 7 While early immunotherapies focused on accelerating T-cell activity, current immune-checkpoint inhibitors take the brakes off the anti-tumor immune responses. Successful clinical trials with PD-1 monoclonal antibodies and other immune-checkpoint inhibitors have opened new avenues in cancer immunology. 8 Monoclonal antibodies that target either PD-1 or PD-L1 can block this binding and boost the immune response against cancer cells. These drugs (pembrolizumab, nivolumab, atezolizumab, avelumab, and durvalumab) have shown a great deal of promise in treating certain cancers. However, PD-L1/PD-L2 expressions and their clinical relevance in CHS is not well understood.
So far, there is a dearth of study that focuses on immune checkpoint profiles in CHS. Therefore, in the current study, we investigated the expressions of PD-L1 and PD-L2–two of the most important biomarkers for PD-1/PD-L1 blockade therapy in CHS–and discussed their associations with various clinicopathological parameters. Our study may hold promise to promoting novel immunotherapy for the disease.
Materials and methods
General information
CHS samples that were surgically removed between January 1997 and January 2017 at Wuxi Second People’s Hospital and Shanghai Ninth People’s Hospital were collected in the current study. None of the patients had received a blood transfusion, radiotherapy, or chemotherapy before surgery. Recurrence was defined as regional bulking or distant mass in organs like lung, with radiological diagnosis in unresectable cases or pathological confirmation in resectable cases. Grading was based on hematoxylin eosin staining, assessing nuclear size, hyperchromasia, cellularity, and mitoses. 9 Nuclear size was evaluated by assessing the tumor cells for whether those cells were small and dark staining, moderate sized with visible intranuclear detail, or large and pleomorphic. The background was considered chondroid if definite lacunae were observed and myxoid if the cells were separated by basophilic intercellular substance without definite lacunae. This study was approved by the Research Ethics Committee of Wuxi Second People’s Hospital and Shanghai Ninth People’s Hospital, PR China. Written informed consent was obtained from each patient.
Immunohistochemistry
A standard immunohistochemistry (IHC) protocol was followed. 10 All samples were formalin-fixed and subsequently paraffin-embedded. Slices were cut at 4 μm and endogenous peroxidase was blocked by incubation with 3% hydrogen peroxide for 15 min. Heat-mediated antigen retrieval was performed by boiling the slides in 0.01M citrate buffer, pH 6.0, for 20 min in a microwave oven. The PD-L1 staining was performed using commercially available rabbit monoclonal antibody clone 28-8 (dilution 1:450; Abcam, Cambridge, UK). PD-L2 antibody was as follow: PD-L2 (Anti-PD-L2 antibody, ab214221, Abcam), at dilution of 1:450. TP53 antibody (Novocastra, Newcastle, UK) was diluted at 1:50 and Ki-67 antibody (Novocastra, Newcastle, UK) was diluted at 1:100. The immune complex was detected with a DAKO EnVision Detection System (DAKO). All slides were then counterstained with Mayer’s hematoxylin blue in 0.3% ammonia. Slides were subsequently dehydrated through graded alcohols to xylene and mounted in a mounting medium. For positive control, we used placenta for PD-L1 and PD-L2, colon carcinoma for TP53, and bladder cancer for Ki-67. For the negative control, we omitted the primary antibodies.
Assessment of PD-L1, PD-L2, Ki-67 and TP53 staining
The proportions of PD-L1-positive tumor cells and tumor-infiltrating lymphocytes were estimated as the number of stained cells divided by the total numbers, respectively. Each slide was reviewed by three independent pathologists and a final reading could only be valid when a consensus was reached. Positive PD-L1 staining is defined as complete and/or partial circumferential linear plasma membrane staining at any intensity that can be differentiated from background and diffuse cytoplasmic staining. For PD-L1, cases with fewer than 1% stained cells were considered negative (1% cutoff). 11 For PD-L2, cases with fewer than 5% stained cells were considered negative (5% cutoff). 12 For Ki-67, at least 1000 tumor cells (×400 magnification) from the most immunopositive regions of the noninvasive part of each neoplasm were visually counted, and a cutoff < 20% was designated as negative. However, for TP53, a cutoff of < 5% was designated as negative. 13
Statistics
The Stata version 12.0 for the Macintosh program was used for statistical analyses. All data were presented as binary in univariate analyses. The Fisher’s exact test was used to evaluate the association between clinicopathological parameters and IHC results. The Spearman’s test was used to evaluate correlation between expressions of factors. Age was labeled as continuous variable in multivariate analyses. The logistic regression model was used for adjustments for the association between clinicopathological parameters and IHC results, and the Cox proportional hazard model was used for the impact of clinically relevant parameters on recurrence-free survival, which was plotted using the Kaplan–Meier method and was compared using the Log-rank test. A P value of <.05 was considered statistically significant.
Results
This was a retrospective study. A total of 59 CHS samples excised between 1997 and 2017 were collected. The demographic data are summarized in Table 1. Recurrence was noted in 44 patients, among whom 23 underwent repeated surgical resection, 13 underwent radio- and/or chemotherapy, and 8 underwent individualized therapies including anti-angiogenic agents, integrative medical therapy, and complimentary therapy. The median follow-up time was 20.04 months (0.9 to 118 months).
Correlation of PD-L1/PD-L2 expression with clinicopathological features of chondrosarcoma in univariate analysis.
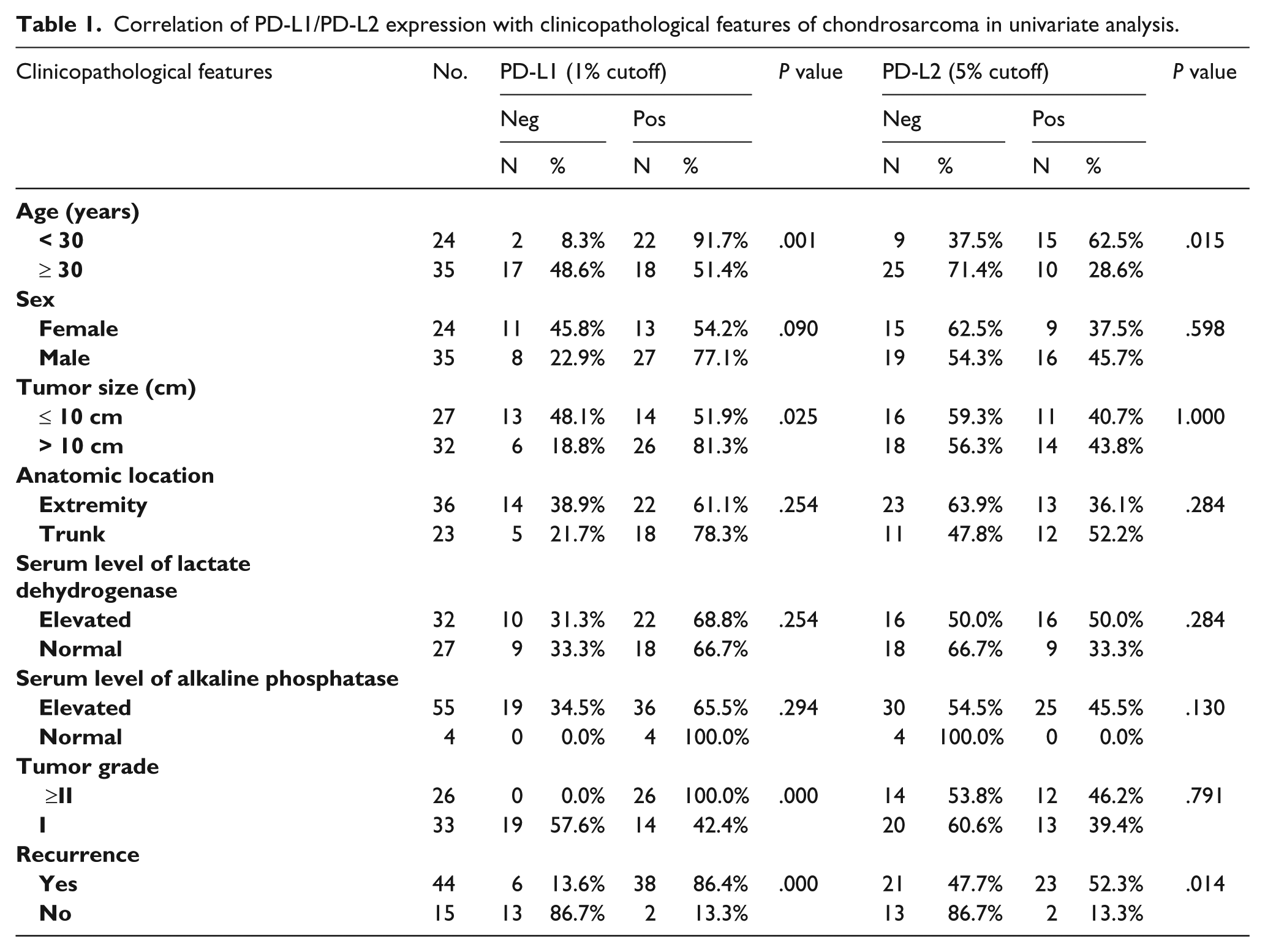
A total of 40 samples were assessed as PD-L1-positive, and 25 samples were PD-L2-positive, whereas 46 samples were positive for both PD-L1/PD-L2 (Figure 1). As shown in the univariate analysis in Table 1, PD-L1 positivity was significantly associated with younger age (< 30 years), larger tumor (>10 cm), advanced tumor grade, and recurrence. PD-L1 positivity was not associated with gender, location, serum level of lactate dehydrogenase (LDH), or serum level of alkaline phosphatase (ALP). PD-L2 positivity was significantly associated with younger age and recurrence. PD-L2 positivity was not associated with gender, tumor size, location, serum LDH or ALP level, or tumor grade. However, in the multivariate analysis, none of the clinical parameters were associated with the expression of either PD-L1 or PD-L2 (Table 2).
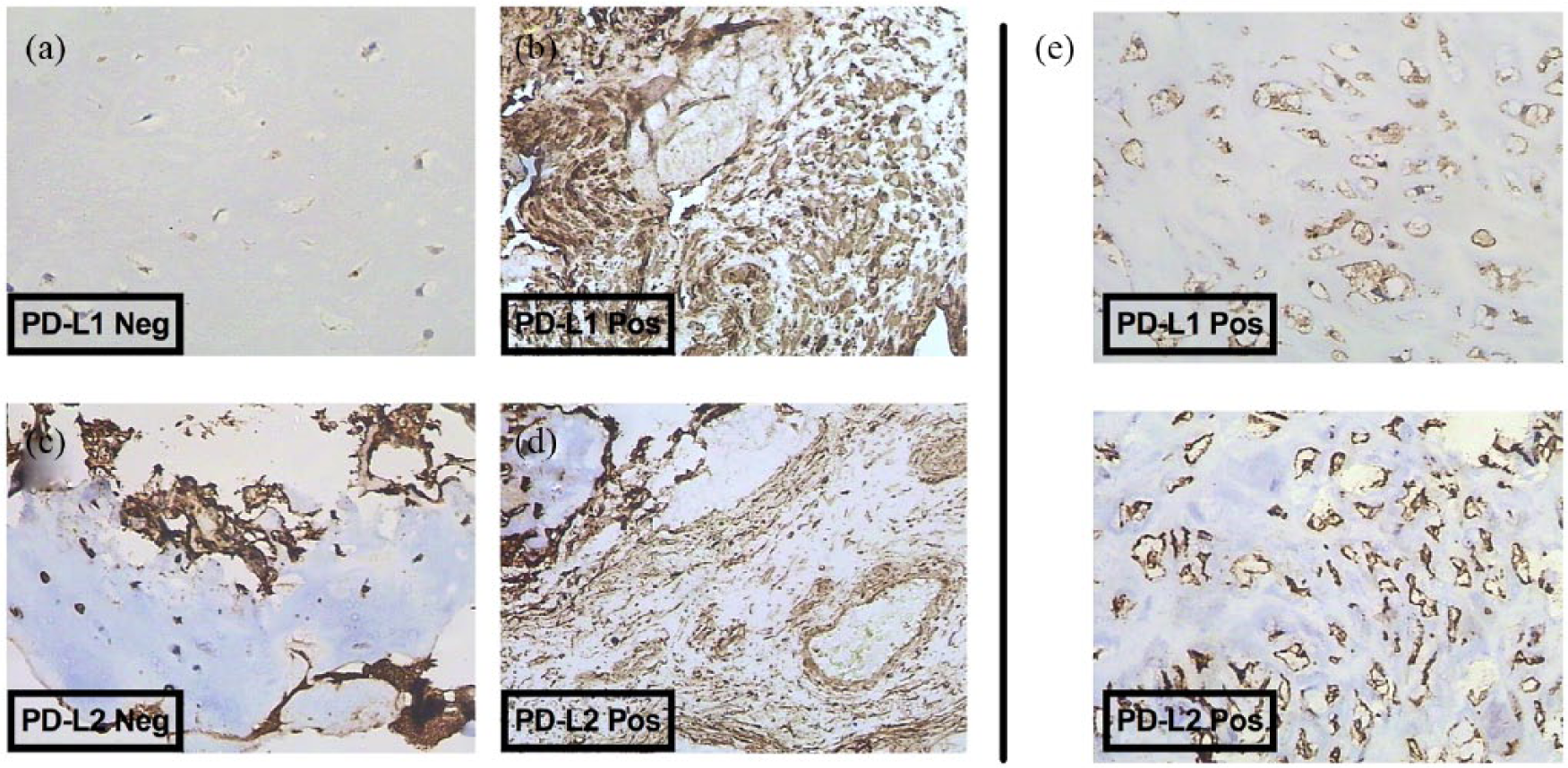
Immunohistochemical staining of PD-L1 and PD-L2 in CHS, showing (a) negative staining for PD-L1; (b) positive staining (1% cutoff) for PD-L1; (c) negative staining for PD-L2; (d) positive staining for PD-L2 (5% cutoff) for PD-L1; and (e) sample that is positive for both PD-L1 and PD-L2. (All were captured at magnification of ×200.)
Correlation of PD-L1/PD-L2 expression with clinicopathological features of chondrosarcoma in a multivariate analysis.
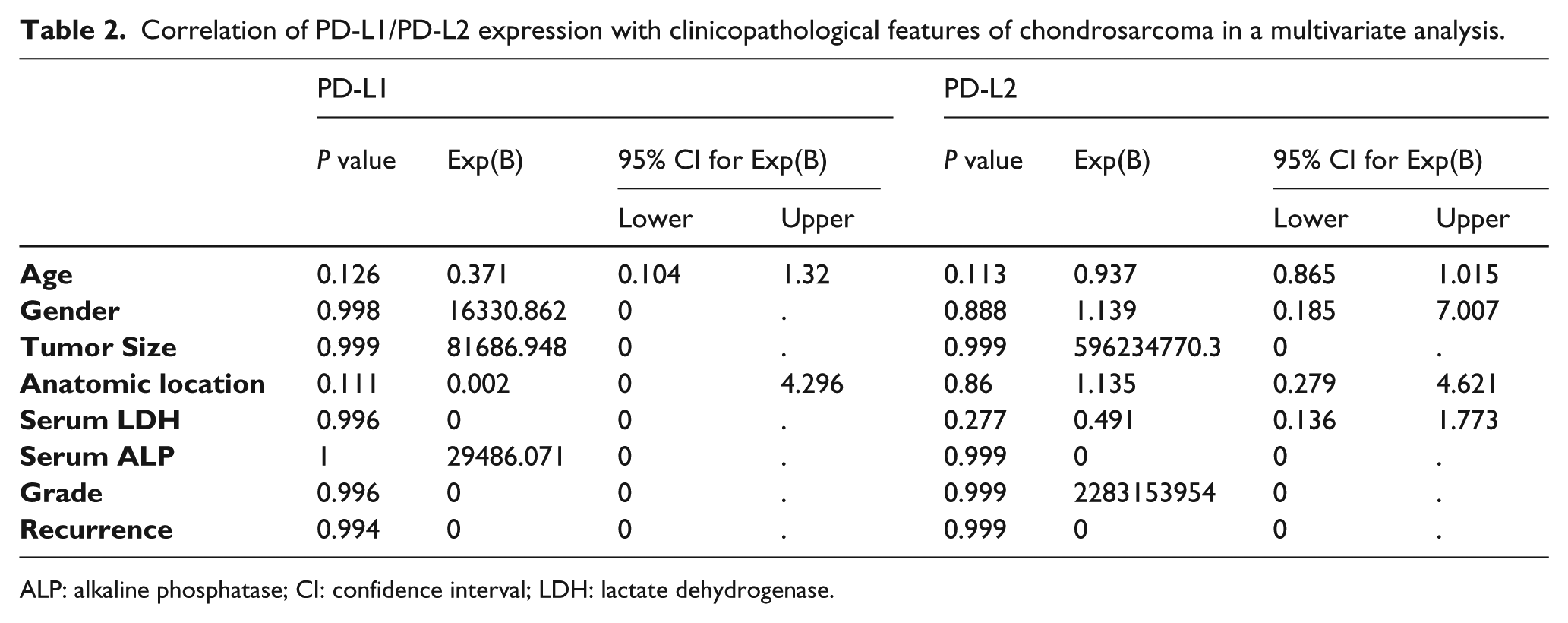
ALP: alkaline phosphatase; CI: confidence interval; LDH: lactate dehydrogenase.
When recurrence-free survival was analyzed, we found that expressions of Ki-67, PD-L1 and both PD-L1/PD-L2 were significantly associated with shorter recurrence-free survival (Figure 2). The expression of TP53 or PD-L2 was not associated with recurrence-free survival. However, in the multivariate analysis, only age and sex remained significantly associated with recurrence-free survival (Table 3).
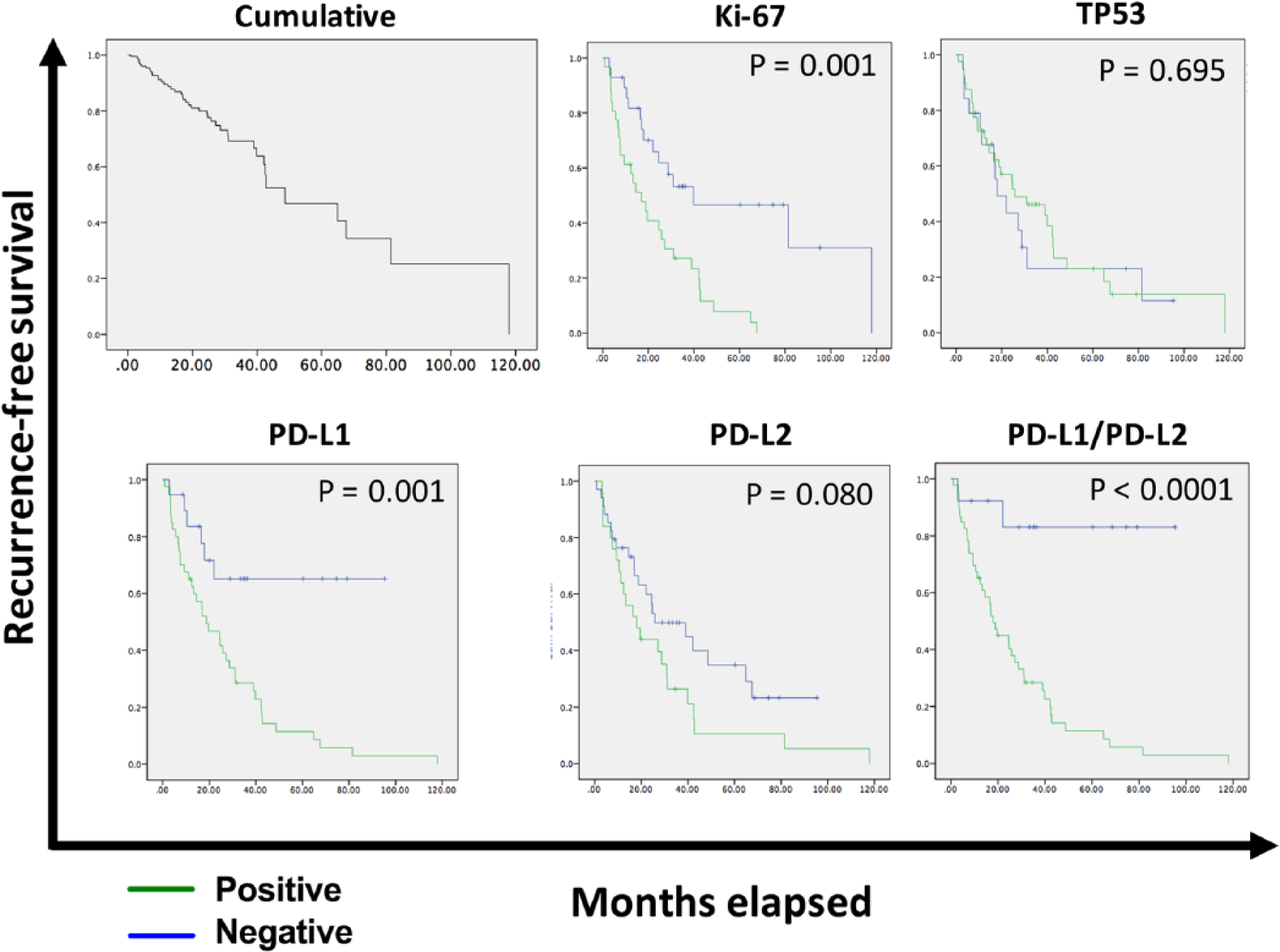
Kaplan–Meier plots of cumulative and grouped recurrence-free survival according to immunohistochemical staining positivity of different pathological factors.
Cox proportional hazard ratio model for the impact of clinicopathological factors on recurrence-free survival.
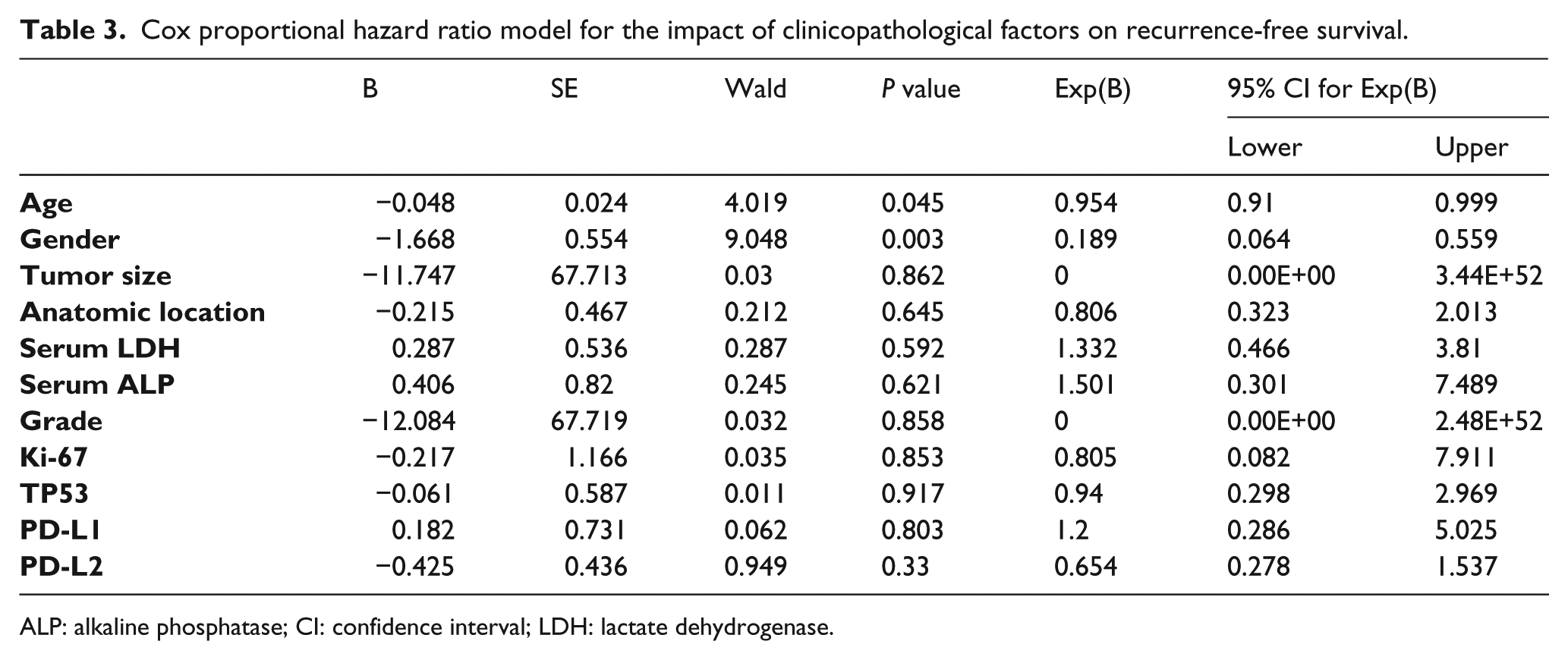
ALP: alkaline phosphatase; CI: confidence interval; LDH: lactate dehydrogenase.
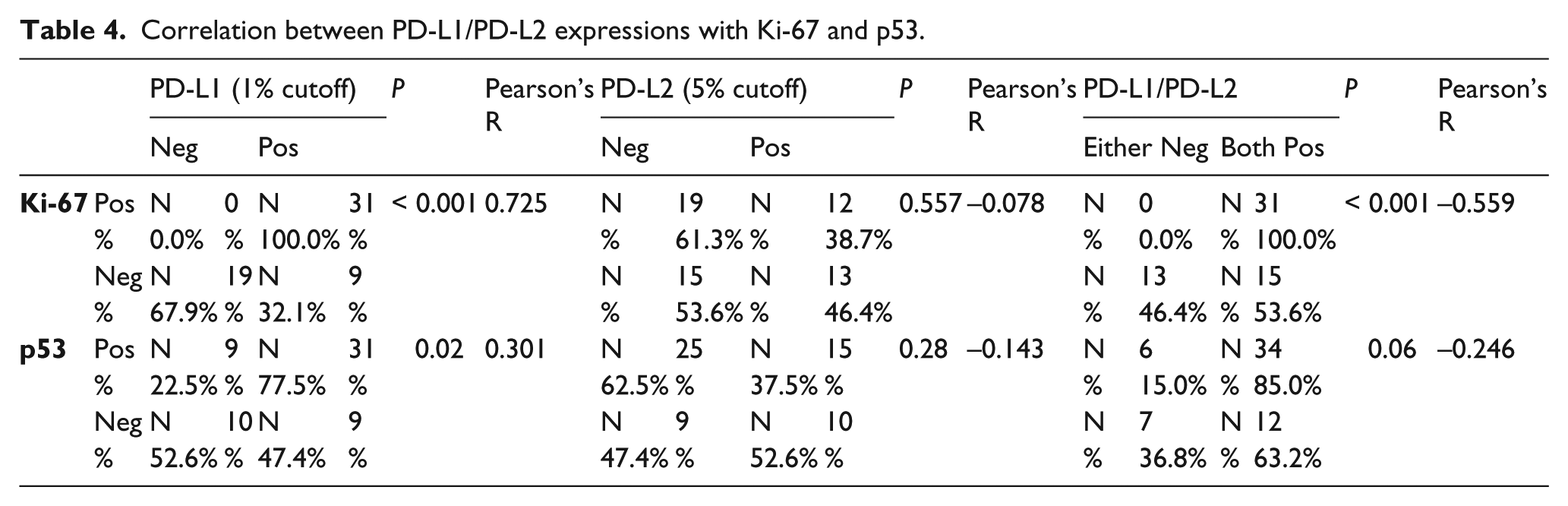
PD-L1 expression was positively correlated with Ki-67 and TP53 expressions. PD-L2 expression was not correlated with either Ki-67 or p53 expression. However, when grouped as a combined expression (both negative vs. either positive), PD-L1/PD-L2 expression was negatively correlated with the expression of Ki-67 (Table 4) but not with p53.
Correlation between PD-L1/PD-L2 expressions with Ki-67 and p53.
Discussion
In the current study, we have shown that positive PD-L1/PD-L2 expression was present in more than half of the CHS cases. This finding, together with other reports, addresses the importance of and the potential for further extrapolating of immune checkpoint inhibitors in CHS.14-16 Zhu et al. 17 reported that in a meta-analysis that correlation between PD-L1 expression with overall survival in bone sarcoma (osteosarcoma and CHS) patients was statistically significant. They concluded that high PD-L1 expression was likely to be a negative factor for patients with sarcomas, and that it predicted worse survival outcomes. Kösemehmetoğlu et al. 18 investigated PD-L1 expression in malignant mesenchymal tumors and found that PD-L1 expression was present in a subset of sarcomas, both at the protein and mRNA level. High-grade pleomorphic sarcomas tend to show PD-L1 expression more frequently. They suggest that clinical trials are necessary to further assess the effect of anti-PD-L1 drugs on sarcomas showing PD-L1 expression. Torabi et al. 19 studied PD-1 and PD-L1 expressions in bone and soft tissue sarcomas (STSs) and found that osteosarcomas, CHSs, and all variants of liposarcomas and rhabdomyosarcomas overexpressed cytoplasmic PD-1, while PD-L1 was negative. We suggest that the different results could result from different antibodies used across the studies. Kim et al. 20 reported prognostic implications of PD-L1 expression in patients with STS and confirmed PD-L1 expression in various STSs of a young population and demonstrated its independent negative prognostic role, thereby suggesting the PD-1/PD-L1 axis is a potential therapeutic target for the treatment of young STS patients.
All abovementioned studies, together with our findings, provide strong evidence that CHS patients may benefit from a PD-1/PD-L1 blockade, which is now used in a variety of cancers with satisfactory effect. Sharma et al. 21 studied nivolumab in metastatic urothelial carcinoma after platinum therapy in CheckMate 275, a multicenter, single-arm, phase 2 trial and found that nivolumab monotherapy provided meaningful clinical benefit, irrespective of PD-L1 expression, and was associated with an acceptable safety profile in previously treated patients with metastatic or surgically unresectable urothelial carcinoma. Goldberg et al. 22 reported the early analysis of pembrolizumab for patients with melanoma or non-small-cell lung cancer and untreated brain metastases in a non-randomized, open-label, phase 2 trial, and found that pembrolizumab showed activity in brain metastases in patients with melanoma or lung cancer with an acceptable safety profile, which suggested that there might be a role for systemic immunotherapy in patients with untreated or progressive brain metastases. Kaufman et al. 23 studied avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma in a multicenter, single-group, open-label, phase 2 trial and found that avelumab was associated with durable responses and was well tolerated; therefore, avelumab represented a new therapeutic option for advanced Merkel cell carcinoma. Seiwert et al. 24 reported safety and clinical activity of pembrolizumab for the treatment of recurrent or metastatic squamous cell carcinoma of the head and neck in an open-label, multicenter, phase 1b trial, and found that pembrolizumab was well-tolerated and demonstrated clinically meaningful antitumour activity in recurrent or metastatic squamous cell carcinoma of the head and neck. Weber et al. 25 studied nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment in a randomized, controlled, open-label, phase 3 trial, and found that nivolumab led to a greater proportion of patients achieving an objective response and fewer toxic effects than with alternative available chemotherapy regimens for patients with advanced melanoma that has progressed after ipilimumab or ipilimumab and a BRAF inhibitor. Antonia et al. 26 reported safety and antitumour activity of durvalumab plus tremelimumab in non-small cell lung cancer in a multicenter, open-label, phase 1b trial, and found that in patients with recurrent or metastatic PD-L1-positive gastric cancer pembrolizumab had a manageable toxicity profile and promising antitumour activity.
Apart from the findings that hold promise, our study had limitations and raised intriguing questions. First, the detection of TP53 mutation using IHC could be inaccurate as both complete lack of expression and overexpression could suggest the presence of TP53 mutations. Oncogenic TP53 alteration is predominantly characterized with overexpression of its mutant form. Several reports comparing the accuracy of IHC as a surrogate for TP53 mutation with sequencing tech also supported IHC as a routine proxy in the oncology setting.27,28 Whether association between PD-L1 and TP53 could be extrapolated warrants further study. Second, we have for the first time addressed PD-L2 expression in CHS and have found that PD-L2-expressing CHS is phenotypically distinct from the PD-L1 counterparts. PD-L2-positive CHS cases are less aggressive in terms of recurrence and proliferation index. Intriguingly, combined PD-L1/PD-L2 positivity revealed reversed correlation with Ki-67 expression compared with PD-L1. Further insightful studies are warranted to elaborate the biological difference between PD-L1 and PD-L2 in CHS.
To sum up, PD-L1/PD-L2 is expressed in CHS and plays a role in the clinical course of the disease. The modest positivity of both indicators warrants further studies applying immune check point inhibition in CHS.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the grants from Wuxi-municipal level key discipline project (ZDXK006).