
Abstract
Introduction
Tuberculosis (TB) caused by many strains of Mycobacterium, especially Mycobacterium tuberculosis, is an airborne disease and the infection risk depends on the concentration of TB bacilli during respiration and the time of exposure.1,2,3 The main risk factors and gaps associated with the progress of the disease are the delay in the treatment due to the inadequate knowledge of the disease, transmission of disease, lack of health care facilities, particularly in rural areas, unhygienic lifestyle and inaccessibility of health care units. 4 The mortality due to TB depends on certain risk factors and its co-morbidities with other infectious and metabolic diseases such as diabetes mellitus, human immunodeficiency virus (HIV), hepatitis, cancer, cardiac diseases and other bacterial infections. 5
An association between diabetes mellitus (DM) and TB disease development have been elucidated due to the compromised immunity as a result of high serum glucose level. Al-Rifai et al., (2017) 6 reported in a meta-analysis of published articles that DM was associated with 2.00-fold (95% CI 1.78–2.24) increased risk of TB (I 2 = 90.5%) in all studies irrespective of the study design. According to International Diabetes Federation, 415 million people are infected with diabetes mellitus and this figure will reach up to 642 million by the year 2040 and more than half of the diabetes population are living undiagnosed. It has been estimated that 1/3rd of the people with diabetes belong to low and middle-income countries. Furthermore, it has also been reported in last meeting of International Diabetes Federation 7 that in Pakistan, more than 19 million adults are expected to live with diabetes and among them about 8.5 million are living undiagnosed and, are more prone to develop risks that may lead to life-threatening complications. 7 Apart from diabetes mellitus, another comorbidity which can alter the immune function is HIV. HIV is one among the most pressing health challenge all over the world affecting millions of people globally. The co-occurrence of TB and HIV infection poses an important global health challenge particularly in low- and middle-income countries. The TB co-infection with HIV is critical and the viral heterogeneity and its burden increases during the course of TB disease. Both HIV co-infection and drug resistant TB are the threat to global TB control. The co-infection of HIV in TB patients is more susceptible to hepatotoxicity. 8 Pakistan has been ranked with the second largest number of hepatitis C virus (HCV) infections globally. HCV co-infection with human immunodeficiency virus (HIV) in TB patients is an additional risk factor causing drug induced hepatitis during TB drug therapy. 9 It has been reported that about 60% of TB patients have cardiovascular disease such as myocarditis, pericarditis and atherosclerosis. 10
Biochemical alterations in pulmonary TB and comorbid patients are common and may be valuable aids in diagnosis. In present study, we investigated the variations in different biochemical parameters in TB patients coinfected with diabetes, HCV, HIV and Myocardial infarction (MI).
This research can contribute to the development of targeted interventions and personalized medicine approaches for individuals with comorbidities, ultimately leading to better health outcomes for these patients. Additionally, identifying patterns and trends in biochemical parameters can aid in early detection and diagnosis of comorbidities, allowing for timely intervention and treatment. Overall, this study aims to fill a gap in the current knowledge by investigating the variations in biochemical parameters in individuals with a single disease and those with comorbidities. By understanding these variations, healthcare providers can improve disease management, prevention, and overall healthcare for individuals with complex health conditions.
Materials and methods
Ethical/ study approval
The study was approved by the Graduate Studies and Research Board (GSRB) of the University of Agriculture Faisalabad, Pakistan, and written consent was obtained from all study participants.
Target population
The purpose of this study was to investigate the relationship between tuberculosis (TB) and infectious and metabolic disorders in the local population. A total of 366 subjects were recruited for this study based on the defined inclusion criteria from various TB hospitals of Central Punjab including Faisalabad, Lahore and Gojra during 2013. A group of healthy individuals were selected as a control group. TB patients with clinical symptoms and confirmed TB disease, as well as with suspected positive chest X-ray, were randomly selected from hospitals and surrounding areas. Patients with known cases of HCV, HIV, diabetes, and myocardial infarction (MI) were also included as positive control groups. Informed consent was obtained from all participants before inclusion in the study.
Inclusion and exclusion criteria
The patients having clinical symptoms of TB showing positive chest radiograph, positive ZN (Ziehl Neelsen) staining and TB patients co-infected with other metabolic and infectious diseases like diabetes, HCV, HIV and Myocardial infarction were included in the study. The known patients of each disease, including diabetes (62), hepatitis C (46), HIV (11) and MI (9) were included in the study as positive control. The positive control patients and the healthy control were randomly selected from hospitals and the surrounding areas where TB patients were included in the study. Suspected TB patients with negative ZN Staining on sputum smear microscopy were excluded from the study.
Sample collection
Blood and sputum samples were collected from TB hospitals in Faisalabad, DHQ hospital Faisalabad, Gulab Devi Chest Hospital (Lahore), DHQ hospital Gojra, and the district prison Faisalabad. ZN staining and polymerase chain reaction (PCR) analysis were conducted at the Molecular Pathology Laboratory in the Department of Pathology at the University of Agriculture Faisalabad, Pakistan. The collected blood samples were processed in the Bio-medical research laboratory, Department of Biochemistry at the University of Agriculture Faisalabad.
ZN staining and direct PCR
ZN Staining was performed for the detection of acid fast bacilli (AFB) in sputum samples and stained smears were observed under the microscope following the method described by Cheesbrough (2006). 11 AFB smear positive sputum samples were analysed by Direct PCR. Sputum samples were decontaminated using NaOH by the modified Petroff method while, bacterial DNA extraction was carried out by phenol chloroform method. The 16S ribosomal RNA (rRNA) oligonucleotide primer and MPB70 primer were used for the identification of Mycobacterium genus and MTB complex, respectively. Amplified DNA samples were run on 1% agarose gel electrophoresis, and bands were visualized under ultraviolet light transilluminator (BioRad; Gel Doc EZ Imager).
Determination of Serum Proteins, Immunoglobulins and minerals
Serum total protein was measured through biuret method, while serum albumin was measured through the Bromocresol purple method following the standard protocols. 12 The globulin concentration was calculated by subtracting serum albumin from total protein. The A/G ratio was calculated by dividing albumin with globulin. Serum IgG and IgM were determined by using Solid phase capture sandwich ELISA assay using a microwell format ELISA kit (Human Diagnostic worldwide) described by Pastorelli et al. (2012). 13 Serum minerals including Sodium (Na) and Potassium (K) analysis was done on fully automated electrolyte analyzer 9180 working on the principle of ion selective electrode while Calcium (Ca) and Phosphorus were determined using Hitachi-902 fully automated chemistry analyzer by Roche diagnostics. 14
Determination of blood glucose, creatinine and urea
Blood glucose was measured by enzymatic oxidation in the presence of an enzyme called glucose oxidase and peroxidase (GOD-POD) end point assay method. 1 15 Blood urea was measured by enzymatic urease method 16 while, serum creatinine was determined through alkaline method. 17
Determination of liver enzymes, lipid profile and cardiac enzymes
Serum bilirubin was estimated following diazotized sulphanilic acid method. 18 Alanine aminotransferase (ALT) also called serum glutamic pyruvic transaminase (SGPT) and aspartate aminotransferase (AST) also called serum glutamic oxaloacetic transaminase (SGOT) activities were measured using a colorimetric method as explained by Burtis et al.). 12 Alkaline phosphatase (ALP) was determined following the method described by Khan et al. 19 Serum total Cholesterol, HDL, LDL and Triglyceride were measured using Hitachi-902 fully automated Chemistry analyzer by Roche diagnostics as described by Mahmood et al. (2013). 14 CK-MB was determined by creatine kinase (CK) activity in the presence of an antibody to CK-M monomer. The sample is incubated in the CK-MB reagent which includes the anti-CK-M antibody. This antibody completely inhibits the activity of CK-MM and half of the activity of CK-MB while not affecting the B subunit activity of CK-MB and CK-BB. The CK-MB activity was obtained by multiplying the CK-B activity by two. 20 Creatine phosphokinase (CPK) was determined by standard colorimetric method based on enzymatic dephosphorylation of creatine kinase to creatine described by Burtis et al. 12 Lactate dehydrogenase (LDH) was determined based on the principal of catalytic activity of the reversible oxidation of L-lactate to pyruvate with the concurrent reduction of nicotinamide adenine dinucleotide (NAD+) to reduced nicotinamide adenine dinucleotide (NADH). 21
Statistical analysis
Serum biochemical parameters were analysed using analysis of variance (ANOVA) technique and means were compared with Duncan multiple range test (DMRT) using Minitab 17 for Windows developed at the Pennsylvania State University, USA. Winpepi software was used to compare the independent groups and to calculate Odds ratio.
Results
The Frequency Percentage and 95% Confidence Interval of Pcr Results, and Gender Distribution.

CI: confidence interval; PCR: polymerase chain reaction.

PCR Product of Mycobacterium Tuberculosis Complex. From Right to Left: Lane 1, DNA Ladder; Lane 2; Negative Control, Lane 3 – 7; Positive PCR Product.
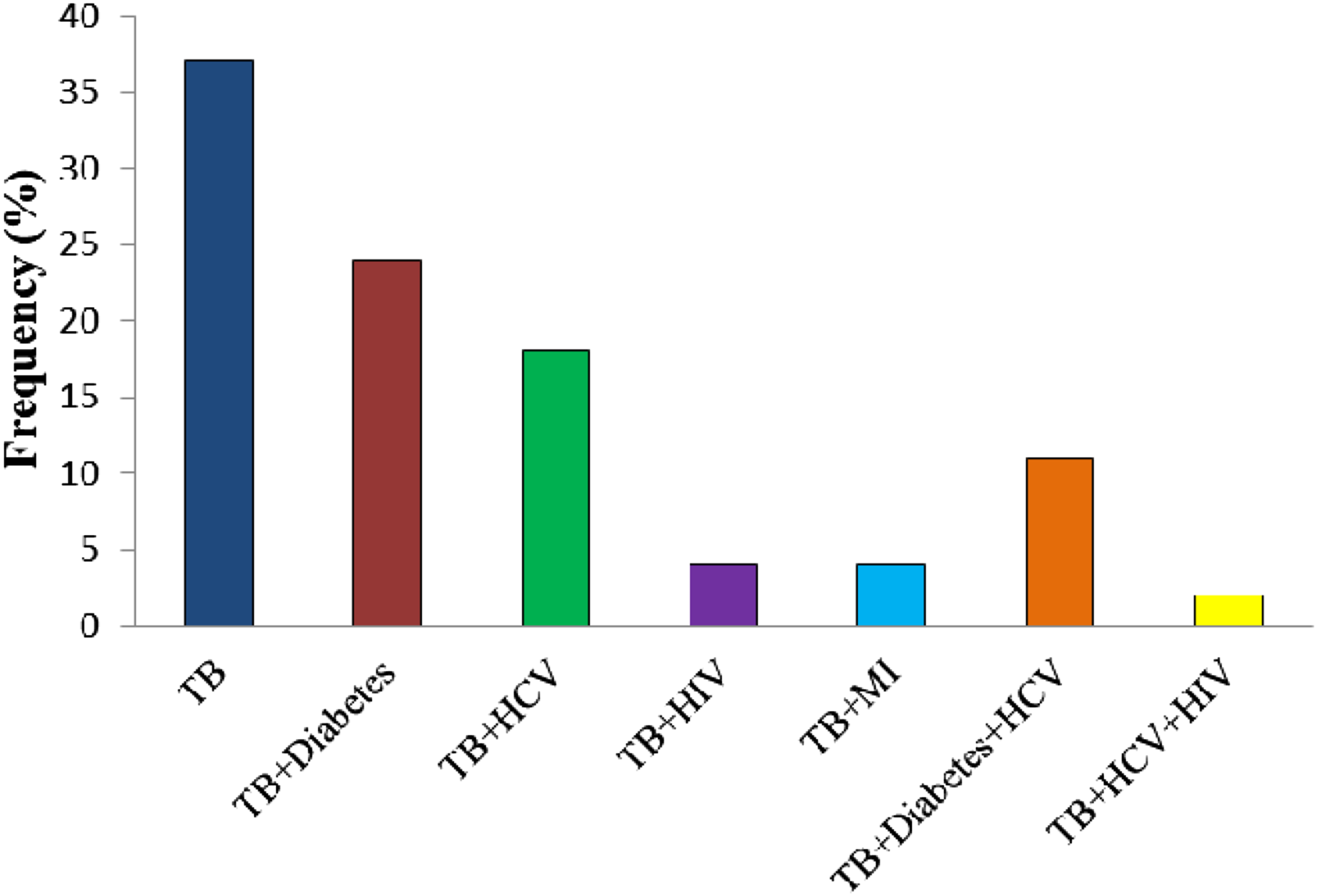
The Frequency Percentage of Tuberculosis and its Comorbidities.
Means ± Standard Deviation of Biochemical Markers of Different Study Groups.
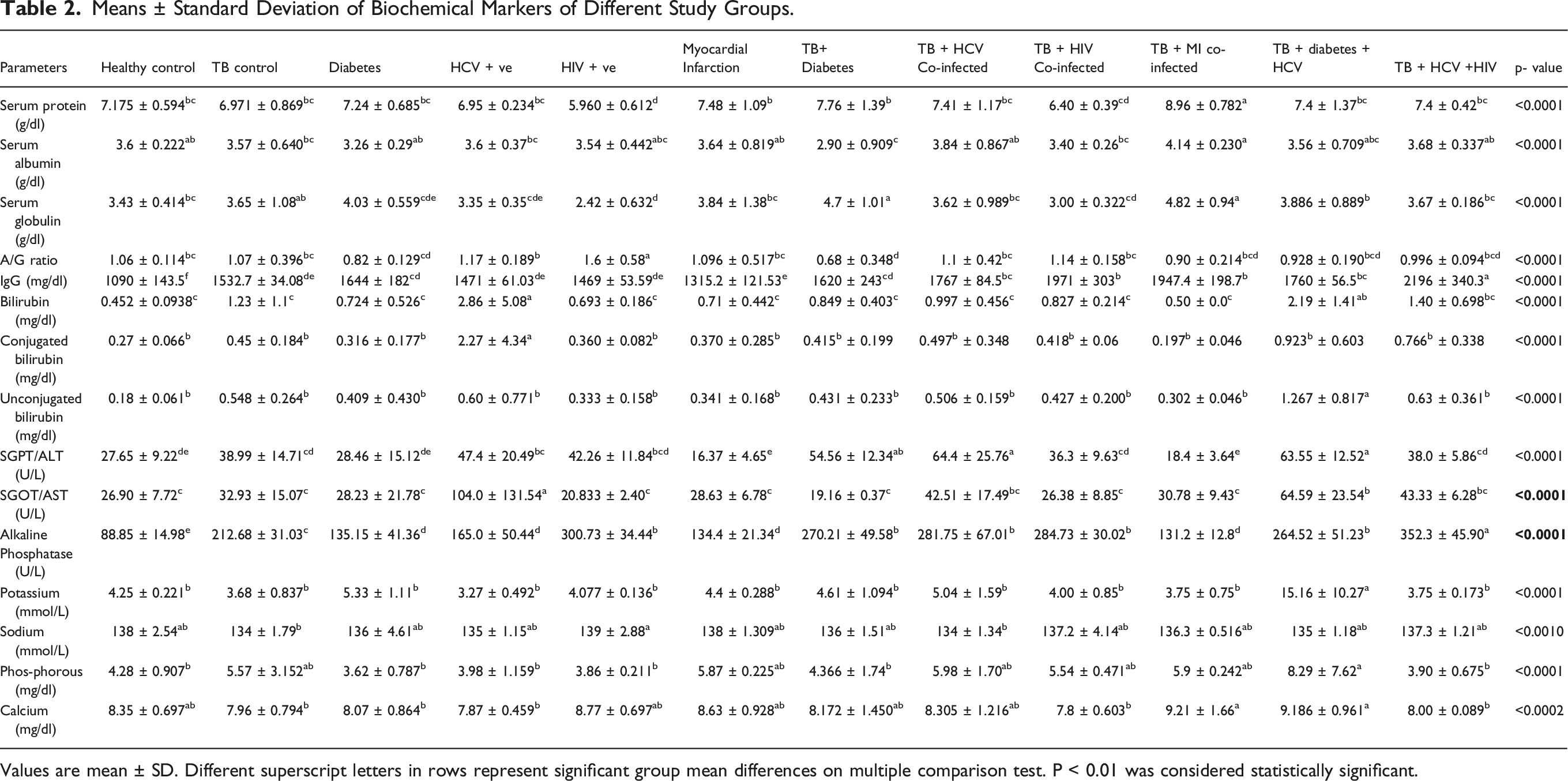
Values are mean ± SD. Different superscript letters in rows represent significant group mean differences on multiple comparison test. P < 0.01 was considered statistically significant.
Means ± Standard Deviation of Serum Glucose, Creatinine, Urea, of Different Study Groups.

Values are mean ± SD. Different superscript letters in rows represent significant group mean differences on multiple comparison test. P < 0.01 was considered statistically significant.
The results of liver enzymes showed significant differences in different study groups. The total Bilirubin levels were significantly increased in HCV positive individuals and TB patients co-infected with diabetes and HCV. Conjugated Bilirubin level was only increased in HCV patients. Unconjugated Bilirubin levels were increased in individuals with diabetes. SGPT/ALT levels were significantly increased in HCV positive individuals, as well as in co-infected patients as TB + diabetes, TB + HCV, and TB + diabetes + HCV. SGOT/AST levels were significantly increased in HCV positive individuals and in those with TB + diabetes + HCV co-infected patients. Alkaline phosphatase levels were increased in all groups of patients when compared to the positive and negative control groups. The results of serum proteins, bilirubin and liver enzymes are given in Table 2.
Means ± Standard Deviation of Lipid Profile and Cardiac Markers of Different Study Groups.

Values are mean ± SD. Different superscript letters in rows represent significant group mean differences on multiple comparison test. P < 0.01 was considered statistically significant.
Discussion
In spite of the advancement of health care facilities, population is still facing many health challenges because of the co-infection with two or more diseases. There are substantial evidences to support the fact that concomitant infections increase the risk of certain chronic diseases. The association of TB with other diseases like diabetes, hepatitis, atherosclerosis and acquired immunodeficiency syndrome, etc. is well known from early 20th century. The current study emphasized on the variation of different biochemical parameters in single disease and co-infection with metabolic and infectious diseases.
Variations in the levels of different plasma proteins and immunoglobulins are a result of various diseases and can be used for diagnostic purposes. Additionally, the activities of specific enzymes found in plasma are also useful for diagnosis of several pathological conditions. Albumin, which constitutes around 60% of the total plasma protein, is the main plasma protein. The liver produces approximately 12 g of albumin per day, accounting for about 25% of the total protein synthesis in the liver. Genesan et al. 22 reported low levels of albumin in TB patients. Awodele et al. (2012) 2 23 in their study found that TB patients co-infected with HIV have significantly higher levels of plasma proteins. On the other hand, Shah et al. (2009) 24 found lower levels of total protein and albumin, but higher levels of serum globulins in HIV co-infected TB patients. The results of our study also showed a highly significant increase in total protein levels and albumin in TB co-infected MI patients, and a significantly lower concentration of total protein and globulin was observed in HIV positive patients. Moreover, serum globulin was found significantly increased in TB co-infected diabetes and TB co-infected MI patients, while serum albumin level was decreased in TB patients co-infected with diabetes. Consequently, the serum albumin/globulin (A/G) ratio also significantly increased in HIV positive patients, while decreased in the TB patients co-infected with diabetes. Matsegora et al. 25 and Sharma et al. 26 also reported an increased IgG levels in TB patients. Rohini et al. (2012) 27 reported a significant increase in IgM levels in TB patients. Hjelmar et al. 28 reported a significant change in IgG levels in patients who tested positive for TB. These results are in agreement with our studies as IgG was significantly increased in all study groups, with higher levels observed in TB patients co-infected with HCV as well as HIV. Additionally, IgM also showed a significant increase in all studied groups. The lower levels of minerals disrupt the immune system, which activates various infectious agents. Further understanding of the function of each mineral may help us establish stronger immunity, thus preventing the body from such infections. Calcium is not only an essential mineral for bones, but it also plays an important role in eliminating the invading viruses from cells. Calcium ions also defend against the common cold. 29 Rahman et al. 30 reported no significant difference in serum urea, potassium, sodium, and calcium levels in TB patients. The results of the present study showed no significant variation in serum calcium levels among different study groups. Okogun et al. (2010) 31 also reported a significant increase in serum calcium and inorganic phosphate in TB patients. Our study results are in line with these studies as we also observed a significant increase in potassium and phosphorus levels in the group of TB patients co-infected with diabetes + HCV. Measuring enzyme activities in body fluids can be helpful in diagnosing and investigating diseases. Enzymes are not produced in serum but are derived from metabolized tissues and blood cells. 32 The results of liver enzymes showed variation among the different groups studied specially those groups infected with HCV. Total bilirubin levels were significantly increased in all HCV positive group and co-infected groups, while conjugated bilirubin levels were only increased in HCV patients. However, unconjugated bilirubin levels were increased in patients with diabetes. ALT activities were significantly increased in the HCV positive group, TB + diabetes group, TB + HCV group, and TB + diabetes + HCV group. Alkaline phosphatase levels were increased in all groups of patients compared to positive and negative controls. Our results are in agreement with Obienu and Nwokediuko (2011) 3 33 who reported significantly higher levels of serum total bilirubin and ALP in TB patients co-infected with HCV. Serum urea and creatinine are baseline tests used to determine and predict diabetes, along with serum glucose. The present study showed a significant increase in serum glucose, serum creatinine and serum urea in patients with diabetes, MI, and diabetes co-infected groups. Viswanathan et al. (2012) 34 also reported similar levels of urea and creatinine in patients with tuberculosis and diabetes. Stec et al. 35 reported that the development of infection is associated with low cholesterol levels in TB patients. They further reported that lower levels of cholesterol, HDL, and LDL occur in the early stages of the illness. Similarly, Metwally and Raheem (2012) 36 reported lower levels of serum cholesterol and triglycerides in patients with TB, while Rao (2009) 37 reported lower levels of serum cholesterol, HDL, and LDL in smear-positive TB patients. Akpovi et al. (2013) 38 also reported significantly lower levels of total cholesterol, HDL, and LDL in patients with TB. They concluded that lower levels of LDL and HDL correlated well with the extent of smear positivity. Our results also showed similarity with these studies as decrease in serum cholesterol, HDL and LDL was observed in TB patients, while an increase in MI and TB + MI patients. Creatine Kinase (CK-MB) is the enzyme being used as the definitive serum marker for the diagnosis or exclusion of acute myocardial infarction (AMI), a heart disease.39,40 The cardiac markers CK-MB, CPK, and LDH revealed a significant increase in patients with MI and TB co-infected MI patients.
Biochemical changes in patients with TB and co-infections can provide valuable information for healthcare providers to understand the complications that arise from these comorbidities. The impact of TB on comorbidities, which was studied in this investigation, does affect serum biochemical parameters. However, it is important to note that these parameters can vary depending on the severity of infection and other socio-demographic factors. Nevertheless, certain biochemical abnormalities are quite common in TB patients and clinicians must maintain a high index of suspicion for diagnosis of TB and co-infections in patients with these abnormalities. The present study has certain limitations as this study investigated only selected biochemical parameters of TB and co-infected patients from few hospitals. Calculating the sample size for the study and the generalizability are also the limitations of this study.
Conclusion
The study concluded that despite the advancements in healthcare facilities such as advanced testing for the diagnosis of TB, the population still faces numerous health challenges due to the coexistence of multiple diseases like TB co-infection with certain metabolic and infectious diseases including diabetes, HCV, HIV and MI. Understanding the variations in biochemical parameters in individuals with a single disease and those with co-infections is crucial for improving the public health and providing better healthcare for individuals with complex health conditions.
Footnotes
Acknowledgment
The authors highly acknowledged the Higher Education Commission (HEC), Islamabad, Pakistan and the Department of Biochemistry, University of Agriculture, Faisalabad, Pakistan for providing the facility to complete this research work.
Ethical considerations
The study was approved by the Graduate Studies and Research Board (GSRB) of the University of Agriculture Faisalabad, Pakistan.
Consent to participate
Written consent was obtained from all participants in the study.
Authors contribution
Irum Javid: Study design, Conceptualization, Methodology, Analysis, Writing – original draft.
Muhammad Riaz: Methology, Analysis, Visualization, Validation, Writing – review & editing.
Fatima Yousaf: Investigation, Analysis, Visualization, Writing – review & editing.
Shamim Khan: Writing – review & editing, Analysis, Validation.
Salma Shahid: Writing – review & editing, Investigation, Visualization.
Farrukh Bashir: Writing – review & editing, Investigation, Validation.
Ghulam Rasool: Writing – review & editing, Analysis, Visualization.
Funding
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) received no financial support for the research, authorship, and/or publication of this article.