
Abstract
Objective
To explore the feasibility of ultrasound measurement of the transverse diameter of the cervical trachea at its narrowest point in patients undergoing severe scoliosis orthopedic surgery.
Methods
A total of 110 patients, aged 18-65, who scheduled for elective orthopedic surgery for severe scoliosis were included. Prior to surgery, all patients underwent two types of tracheal inner diameter measurements: (1) CT measurement of the anteroposterior diameter (Dmin,AP) and transverse diameter (Dmin,T) of the cervical trachea at its narrowest point; and (2) ultrasound measurement of Dmin,T. Based on the measurement results, the patients were randomly divided into two groups, the CT group (n = 55) and the ultrasound group (n = 55). We compared the Dmin,AP and Dmin,T measured by CT for all patients. Then, we compared CT and ultrasound measurements of Dmin,T. Furthermore, we conducted an analysis to determine the correlation and consistency between the two methods. Additionally, we examined the success rate of first-attempt tracheal intubation and the occurrence rate of tracheal tube being too wide or too narrow between the two groups, and assessed the occurrence of postoperative 24-h pharyngeal pain and hoarseness.
Results
When comparing the Dmin,AP and Dmin,T measured by CT in all patients, a statistically significant difference was observed (p < .001). When comparing the measurements of Dmin,T between CT and ultrasound in all patients, no statistically significant differences were found (p > .05). The correlation coefficient (r) between CT and ultrasound measurements of Dmin,T was 0.849 (p < .001). The mean difference in Dmin,T was 0.19 mm, and the limits of agreement (LoA) were −2.24 mm to 2.62 mm.
Conclusions
Ultrasound measurement of Dmin,T in severe scoliosis patients is feasible and provides valuable guidance for the selection of endotracheal tube sizes. It serves as a non-invasive and bedside auxiliary examination method for perioperative airway assessment.
Introduction
Scoliosis is a heterogeneous condition characterized by changes in the shape and position of the spine, thorax, and trunk. It is most commonly observed in children and adolescents, with an incidence rate ranging from 0.47% to 5.2%. 1 According to the criteria by the Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT), 2 patients with a Cobb angle greater than 10° and axial rotation are clinically diagnosed with scoliosis, while severe scoliosis is defined as a Cobb angle exceeding 40°. 3 Patients with scoliosis exceeding 80° may experience symptoms and develop dyspnea, potentially leading to cardiopulmonary functional impairment and failure. To improve the physical condition of patients, surgical treatment is the primary approach for severe scoliosis. Research has indicated that severe thoracic scoliosis can lead to main airway torsion and compression of the bronchi, 4 which significantly increases the risks associated with anesthesia, particularly in terms of airway management and the selection of an appropriate endotracheal tube.
Selection of the optimal endotracheal tube size is critical in anesthesia, A larger-than-optimal-sized endotracheal tube can damage the airway,a small-sized endotracheal tube increases the risk of aspiration and insufficient ventilation. The type of endotracheal tube is closely related to the diameter of the trachea. At present, MRI or CT is often used to measure the diameter of the trachea, which has limitations such as radiation and inconvenient operation。Ultrasound, as an essential tool for airway management, allows for the objective measurement of airway parameters to identify relevant upper airway anatomies. Furthermore, it can provide real-time dynamic images to guide airway interventions. Therefore, this study intends to employ ultrasound to measure the transverse diameter of the cervical trachea at its narrowest point and investigate its feasibility in guiding endotracheal tube selection. We aim to provide a reference for endotracheal tube selection in patients undergoing severe scoliosis orthopedic surgery.
Materials and methods
Basic data
This is a prospective, randomised, double-blinded study. This study received ethical approval from the Ethics Committee of The Second Affiliated Hospital of Chengdu Medical College/China National Nuclear Corporation 416 Hospital (Ethics Number: YJ-2022-001, Chinese Clinical Trial Registry, TRN: ChiCTR2200065452). Patients scheduled for elective severe scoliosis orthopedic surgery at The 2nd Affiliated Hospital of Chengdu Medical College/Nuclear Industry 416 Hospital between November 2022 and August 2023 were randomly selected for this study,Halo-pelvic traction was completed preoperatively for all patients (Figure 1). All patients willingly participated in the research and provided written informed consent before surgery. Patients scheduled for severe scoliosis orthopedic surgery. (Figure Source: Dr Liang Yijian’s Scoliosis Orthopedic Surgery Workshop, The Second Affiliated Hospital of Chengdu Medical College/China National Nuclear Corporation 416 Hospital)
Inclusion criteria included: patients with ASA (American Society of Anesthesiologists) 5 physical status classification II-III, aged 18 to 65 years, and scheduled for elective scoliosis orthopedic surgery, The Cobb Angle of the whole spine was greater than 40°.
Exclusion criteria included: skin infections in the neck area; neck trauma; history of throat or bronchial surgery; thyroid enlargement or intratracheal tumors; recent symptoms such as sore throat or hoarseness; and mental disorders or other reasons leading to collaboration difficulty.
Exclusion criteria for analysis included: patients in whom tracheal intubation failed and surgery was temporarily suspended; patients transferred to the intensive care unit (ICU) after surgery (Reasons for admission to ICU includes: (a) Patients were unable to undergo early tracheal extubation; (b) Patients exhibited unstable vital signs postoperatively and need vasoactive drugs.), and patients who required re-intubation after extubation.
Randomization and blinding procedures
All enrolled patients underwent two methods of tracheal inner diameter measurement before surgery: (1) CT measurement of anteroposterior diameter (Dmin,AP) and transverse diameter (Dmin,T) of the cervical trachea at its narrowest point, and (2) ultrasound measurement of the transverse diameter (Dmin,T) of the cervical trachea at its narrowest point. Researcher 1 not involved in the following experiments recorded Dmin,AP and Dmin,T from CT and ultrasound for all patients. Using SPSS 25.0 software, patients were randomly divided into two groups, CT group and ultrasound group, at a 1:1 ratio. The results of CT (Dmin,AP and Dmin,T) and ultrasound measurements were sealed in envelopes and kept by Researcher 2 who was unaware of the group assignments. Only Researcher 2 could open the envelopes and choose the endotracheal tube size. Specifically, endotracheal tube size selection was based on CT measurement results in CT group and on ultrasound measurement results in ultrasound group. Researcher 3, unaware of the group assignments and endotracheal tube size selection, was responsible for the observation and recording of experiment-related data. The anesthesiologists, surgeons, patients, and researchers involved in the study were all blinded to the group assignments. In case of a life-threatening situation, the envelopes were opened for unblinding immediately to take necessary emergency actions.
CT examination
The tracheal measurements were conducted by a radiologist with over 5 years of experience in radiology using Philips Brilliance iCT 128 and 256 Slice CT Scanner (Amsterdam, Holland). The CT scan was performed with a slice thickness of 1 mm. Patients were positioned in a supine position without a pillow to maintain normal breathing while undergoing the cervical CT scan. Using the built-in data processing software of the CT machine, measurements of Dmin,AP and Dmin,T were taken (Figure 2). CT measurement of Dmin,AP and Dmin,T.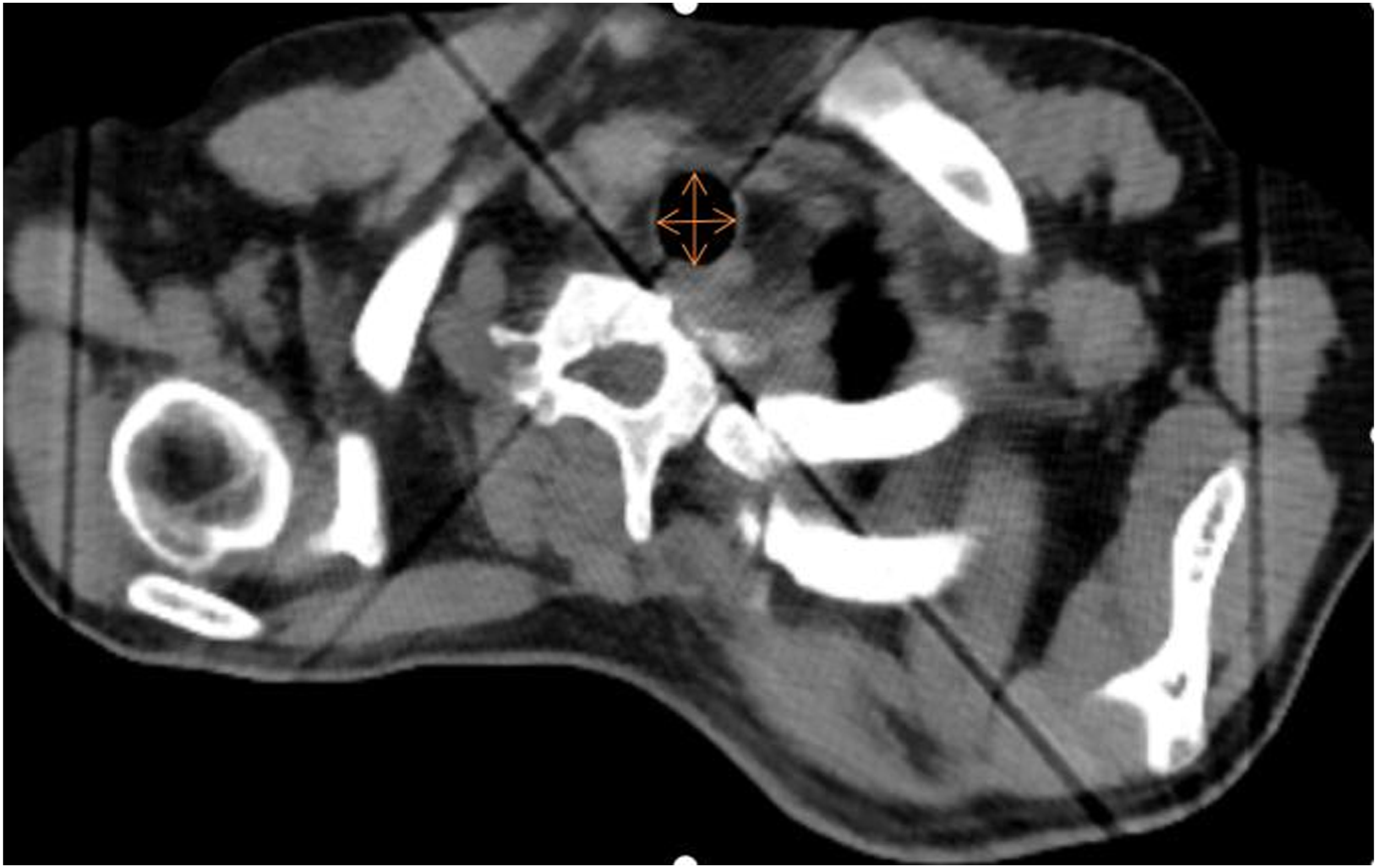
Ultrasound examination
The ultrasound examination was performed by an anesthesiologist who had received specialized training in ultrasound, using the Mindray M9 Color Ultrasound Machine (Shenzhen, China). A linear array probe was employed, at a frequency ranging from 5 to 10 MHz, and a depth of 2 to 4 cm. Patients were placed in the same position as during the CT examination. The ultrasound probe was oriented perpendicular to the midline of the neck, starting from the level of the vocal cords, moving downward in a parallel fashion. The positioning involved identifying the cricoid cartilage (represented by two high-echoic arc-shaped edges formed by the inner and outer tracheal membranes enclosing the low-echoic band). The ultrasound probe was gently moved downwards from the level of the cricoid cartilage until reaching the suprasternal notch. In each transverse section, the probe was maneuvered left and right until a complete view of the tracheal rings was obtained. Simultaneously, the ultrasound was used to observe the echo from cartilage of anterior tracheal wall, ensuring its integrity, regularity, and continuity. The measurement of Dmin,T was obtained by scanning both above and below the visibly narrowed portion (Figures 3 and 4). Ultrasound measurement of the airway. Ultrasound measurement of the airway transverse diameter.

Anesthesia method
A total of 121 patients were initially included in this study. However, 11 cases were excluded before surgery, as 7 cases refused to participate, and 4 cases had a recent history of pharyngeal pain. Thus, 110 patients in total underwent CT and ultrasound measurements of the narrowest inner diameter of the cervical trachea and participated in randomization, with 55 patients in each group (Figure 5). All patients underwent fasting for 8 h and refrained from drinking for 6 h prior to surgery. Upon entering the operating room, routine monitoring of heart rate, pulse oxygen saturation, invasive arterial blood pressure, and central venous pressure was initiated. Additionally, patients were provided with warming blankets for temperature maintenance, and their body temperature was monitored. A conscious intubation for general anesthesia was performed under surface anesthesia by applying tetracaine mucilage to the throat. Cricothyroid membrane puncture was performed, and 2% lidocaine at a dose of 1 mg/kg was injected for endotracheal local anesthesia. Endotracheal intubation was conducted by the same anesthesiologist with over 5 years of experience using a fiberoptic bronchoscope. Intubation success was confirmed by monitoring the end-tidal carbon dioxide waveform. Anesthesia induction included midazolam at 0.04 mg/kg, sufentanil at 0.4 μg/kg, cisatracurium at 0.2 mg/kg, and propofol at 2 mg/kg. The endotracheal tube cuff was maintained at 25 cmH2O. Anesthesia maintenance included propofol at 5–8 mg/(kg·h), remifentanil at 0.1–0.2 μg/(kg·min), and intermittent administration of sufentanil as needed. Anesthesia depth was monitored using BIS (bispectral index)
6
and maintained between 40 and 60. Mechanical ventilation was provided with 50% oxygen concentration, and respiratory parameters included tidal volume (VT) of 6–8 ml/kg, a respiratory rate (RR) of 10–16 breaths/min, and end-tidal carbon dioxide pressure maintained between 35 and 45 mmHg. In case of hemodynamic instability, medications such as ephedrine, norepinephrine, or atropine were administered as required. In both groups, the infusion of propofol and remifentanil was stopped 10 min before the end of surgery, and additional sufentanil was administered for analgesia. The endotracheal tube was removed once the patients regained consciousness, demonstrated spontaneous breathing, and had stable vital signs after the surgery. Flowchart of patient enrollment of the study.
Endotracheal tube size selection and criteria for size assessment
Selection Criteria for Endotracheal Tube: Based on the ultrasound or CT measurements of Dmin, T, an endotracheal tube with an outer diameter that is 5 mm less than Dmin,T was selected as the tube size. 7
Criteria for Endotracheal Tube Being Too Wide:In the presence of resistance to passage of the tube into the trachea, or in the absence of an audible leak at airway pressure >25 cm H2O, the ETT was replaced with a tube of 0.5 mm less internal diameter. Tube Being Too Narrow:If a leak was audible at airway pressures <10 cm H2O, if a seal could not be achieved with a cuff pressure >25 cm H2O, or if a peak airway pressure <25 cm H2O was observed during ventilation, the tube was exchanged for one a size larger. 8
Evaluation indicators
The following clinical data were collected for both groups of patients: CT measurements of Dmin,AP and Dmin,T, ultrasound measurement of Dmin,T, endotracheal tube size, success or failure of first-attempt endotracheal intubation, presence of endotracheal tube being too wide or too narrow,the occurrence of postoperative 24-h pharyngeal pain visual analogue scale (VAS) 9 Score and hoarseness Incidence.
Statistical analysis
Sample Size Calculation: For this study, a significance level of α = 0.05 and a power of 1-β = 0.8 were set. Based on previous research results (r = 0.882), 10 sample size calculations were performed using Power Analysis and Sample Size (PASS) 15.0 software, resulting in a required sample size of 99 cases. Accounting for an expected dropout rate of 10%, a total of 110 cases were planned.
All data and statistical graphs were processed using SPSS 25.0 and MedCalc Statistical Software 22.009 (MedCalc Software Ltd, 2023, Ostend Belgium), both of which have been licensed. Normally distributed measurement data were expressed as mean ± standard deviation (
Results
General data comparison
Comparison of demographics and intraoperative conditions.

Comparison of CT Measurements of Dmin,AP and Dmin,T, Comparison of CT and Ultrasound Measurements of Dmin,T, and Analysis of Their Correlation and Consistency
Comparison of CT and ultrasound measurements of Dmin,T and Dmin,AP (n = 110,

When compared to CT measurements of Dmin,T, △p < .05.
The correlation coefficient (r) between ultrasound and CT measurements of Dmin,T was found to be 0.860 (p < .001), as shown in Figure 6. Correlation between ultrasound and CT measurements of Dmin,T (n = 110).
Bland-Altman Analysis for Consistency Between the Two Measurement Methods: The average difference in Dmin,T was 0.16 mm, with a LoA ranging from −2.24 mm to 2.55 mm, as depicted in Figure 7. Bland-Altman analysis of consistency between CT and ultrasound measurements of Dmin,T (n = 110).
The upper and lower horizontal dashed lines represent the upper and lower limits of the 95% consistency interval, while the middle solid horizontal line represents the mean difference value.
Comparison of first-attempt Endotracheal Intubation Success Rate and Incidence of Endotracheal Tube Being Too Wide or Too Narrow
Comparison of first-attempt endotracheal intubation success rate and incidence of endotracheal tube being too wide or too narrow [n (%)].

Comparison of postoperative 24-HourPharyngeal pain VAS score and hoarseness incidence
Comparison of postoperative 24-hour pharyngeal pain VAS score and hoarseness incidence.

Discussion
In this study, all patients underwent measurements of the tracheal inner diameter at its narrowest point by CT or ultrasound. Subsequently, the patients were divided into two groups based on the results obtained from CT and ultrasound measurements, respectively, for the selection of endotracheal tubes. The findings revealed that in all enrolled patients, the Dmin,T, as measured by CT, was significantly smaller than Dmin,AP. Moreover, there was good consistency between CT and ultrasound measurements of Dmin,T. Additionally, there were no significant differences observed between the two groups in terms of first-attempt endotracheal intubation success rate, incidence of endotracheal tubes being too wide or too narrow, and the occurrence of postoperative 24-h pharyngeal pain and hoarseness. Consequently, this study suggests that ultrasound evaluation of Dmin,T in patients undergoing the surgery for severe orthopedic scoliosis is a feasible approach. It can also assist in the selection of endotracheal tube size.
Patients with severe scoliosis not only have deformities in the spine but also in the chest wall and airway. These deformities often lead to reduced chest wall compliance, resulting in suboptimal lung function and narrowing and curvature of the airway. 12 Surgery is a crucial intervention for patients with severe scoliosis, as it can significantly improve their lung function, activities of daily living, and physical appearance. Prior to scoliosis orthopedic surgery, halo-pelvic traction is typically applied, which immobilizes the head and neck. However, some patients, especially those with ankylosing spondylitis, may experience stiffness in the temporomandibular joint, leading to difficulty in opening the mouth. In such cases, using a laryngoscope to expose the vocal cords and structures of the throat can be challenging, and it may be even impossible to insert the laryngoscope. This presents a significant challenge for anesthesiologists, particularly when it comes to establishing a secure airway. 3 For such patients, in order to prevent complications associated with intubation and to ensure a clear and safe airway, awake anesthesia with fibrobronchoscopy-guided endotracheal intubation is often preferred. To minimize discomfort during awake intubation, it is essential to maximize the success rate of first-attempt endotracheal intubation. Choosing the appropriate endotracheal tube size before intubation is of paramount importance. If the endotracheal tube is too wide, it can lead to difficulty in intubation and an increased risk of mucosal injury, increasing the likelihood of tube replacement. On the other hand, if the endotracheal tube is too narrow, it may increase the risk of ventilator-associated pneumonia. Furthermore, to prevent air leak, higher cuff pressures may be required, which can compromise blood flow to the tracheal mucosa, potentially leading to ischemia and necrosis of the tracheal mucosa.
The selection of an appropriate endotracheal tube size is closely related to the diameter of the patient’s trachea. Currently, there are several methods for measuring tracheal inner diameter, with the most common approaches involving non-invasive MRI, CT scans, or invasive bronchoscopy-guided measurements. 13 MRI is considered as the gold standard for non-invasive measurements, providing high-quality imaging of the pharyngeal region to accurately measure throat parameters. 14 However, the patients with severe scoliosis, as seen in this study, often undergo halo-pelvic traction, which is problematic for MRI scans due to the presence of the metallic head ring and pelvic ring. Calloway et al. 15 Have suggested that bronchoscopy measurements of tracheal inner diameter correlate well with CT measurements. However, bronchoscopy is an invasive procedure with relatively high requirements, making it less practical as a routine method for measuring tracheal diameters. With advancements in CT technology, chest CT scans have become a preferred and convenient means for measuring airways and observing the trachea’s dimensions. 16 CT scans are generally faster than MRI, do not require sedation or anesthesia, and are more cost-effective. In recent years, ultrasound has gained popularity as a safe, non-invasive, bedside tool for airway assessment and management. Studies have found that ultrasound can measure soft tissue thickness at the hyoid bone, thyroid cartilage, and vocal cord junction, which serve as good independent predictors of difficult airways. 17 Ultrasound can measure upper airway parameters and access the changes before and after anesthesia induction, airway collapsibility, 18 confirm endotracheal tube placement, measure tracheal inner diameter, evaluate post-extubation laryngeal edema, and locate the cricothyroid membrane.7,19 In a study conducted by Lakhal et al. 20 Involving 19 healthy adults, the ultrasound examination is proved to be a reliable tool for assessing the minimum diameter of the tracheal lumen.
CT is considered as the gold standard for imaging the airway and is the preferred radiological examination for assessing the larynx and hypopharynx. 21 In our study, we observed that in patients with severe scoliosis, the CT measurements of Dmin,AP were larger than Dmin,T (16.19 ± 2.77 vs 14.40 ± 2.20, p = .000). This finding aligns with the results of a study by Karmakar et al. 22 confirming that Dmin,T can serve as a reference for the narrowest tracheal dimension. However, it is worth noting that air within the airway can be a significant impediment during imaging as it attenuates ultrasound transmission, resulting in artifacts and making it challenging to measure the anteroposterior diameter. Therefore, in this study, we solely measured the Dmin,T using ultrasound. The visualization of anatomical structures during ultrasound assessment of the airway closely correlates with the anatomical structures observed in CT images. 23 Previous research has demonstrated good consistency between CT and ultrasound measurements of the cricoid cartilage diameter. 24 Our study also revealed a high degree of correlation between ultrasound and CT measurements of Dmin,T (r = 0.849, p = .000, LoA −2.24 mm to 2.62 mm). This indicates that the ultrasound measurement of Dmin,T is a feasible alternative.
The selection of endotracheal tube sizes for intubation is a critical consideration in clinical practice. While conventional guidelines often recommend using standard tube sizes such as 7.5 mm for adult males and 7.0 mm for adult females, this approach may not be suitable for patients with severe scoliosis or airway anomalies. Since patients with severe scoliosis also often suffer from associated airway anomalies, including narrowing and twisting, due to developmental anomalies, estimating the size of the tracheal tube based on conventional formulas or age, height, and weight is not feasible in such patients. Therefore, the use of tools to measure tracheal diameter for precise endotracheal tube selection is essential. Previous research has demonstrated that CT measurements of tracheal diameter can guide the selection of endotracheal tube sizes. 25 Furthermore, the ultrasound has been proven to be valuable for measuring tracheal diameter not only in healthy adults but also in pediatric patients, aiding in the selection of appropriate endotracheal tube sizes and determining insertion depth. 7 In our study, we utilized ultrasound and CT measurements to guide the selection of endotracheal tube sizes, and the results indicated that there were no significant differences in the first-attempt endotracheal intubation success rate (92.2% vs 88%, p = .484) between the two groups. Additionally, the rates of endotracheal tube being too wide (7.8%) and too narrow (3.9%), and the occurrence of postoperative 24-h hoarseness (9.8%) in the ultrasound group reaffirmed the efficacy of using ultrasound to measure airway diameter and guide endotracheal tube size selection.
CT is recognized for its high accuracy in measuring anterior soft tissue thickness in the neck. However, it has limitations, including radiation exposure and cost, which may hinder its use in the operating room. Moreover, CT measurements may introduce some degree of error, especially when patients need to breathe deeply during the scan. In contrast, ultrasound imaging offers several advantages, including portability, safety, affordability, rapid imaging, real-time visualization, and the absence of radiation exposure. Notably, ultrasound measurements can be performed at the bedside on awake patients, with precision nearly matching that of the above imaging technique. 17
There are some limitations to our study. First, we focused on a specific population of patients with severe scoliosis, which constitutes a relatively small sample size, potentially limiting the generalizability of our findings. Second, our ultrasound assessment of the airway primarily measured the tracheal diameter, which has its own limitations. Future research could expand the scope of airway evaluation to enhance accuracy and comprehensiveness.
Conclusions
In summary, our study found that Dmin,T measured by ultrasound and Dmin,T measured by CT were in good consistency, with no significant differences in success rate of first-attempt tracheal intubation, tracheal tube size, postoperative pharyngeal pain and hoarseness between the two methods. Therefore, ultrasound-guided tracheal tube selection is feasible to some extent and may serve as a convenient, non-invasive and auxiliary bedside examination method for perioperative airway assessment. However, it is essential to note that the sample size of patients with severe scoliosis used in this study is small. Further studies with a larger sample size are warranted.
Footnotes
Acknowledgments
We are thankful to all the patients and/or their guardians who showed consent and participated in the study. We are also thankful to Dr Liang Yijian’s Scoliosis Orthopedic Surgery Workshop.
Authors’ contributions
Conceived and designed the experiments: Ying Tian and Mingshuai Yu. Performed the experiments: Ying Tian, Zuqi Chen, Tianke Xiao and Ke Zhang. Analyzed the data: Ying Tian, Tianke Xiao, Ke Zhang. Designed this study and modified the manuscript: Mingshuai Yu. Wrote the paper: Ying Tian. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chengdu Medical Research Project (2022467).
Ethical statement
Trial registration
Registration of China Clinical Trial Center:ChiCTR2200065452*