
Abstract
Investigating cytokine levels in ICU patients reveals their potential in predicting the occurrence of Persistent Inflammatory Response-Immunosuppression-Catabolic Syndrome (PICS). Our study encompassed clinical data from ICU patients admitted between December 2020 and January 2022. The cohort was divided based on the incidence of PICS, and a comparative analysis was conducted on their clinical data. Using logistic regression, we identified independent factors influencing PICS. Among 132 patients meeting our inclusion criteria, 39 (31.70%) developed PICS. Significant differences were observed between the PICS and non-PICS groups in terms of average age, APACHE II scores, hospital stay duration, mortality, and infection rates. Notably, laboratory parameters indicated lower pre-albumin and IL-4 levels, alongside higher IL-6, IL-10, IL-17, and IFN-y levels in the PICS group. Multivariate analysis pinpointed pre-albumin, IL-4, IL-6, and IL-10 as independent risk factors for PICS in ICU settings. Our findings underscore the importance of IL-4, IL-6, and IL-10 as key cytokines in the early detection and management of PICS, offering significant insights for clinical practice.
Introduction
Adequate nutrition and including natural compounds with antioxidant and anti-inflammatory properties, such as flavonoids and polyphenols, are fundamental in promoting human health and preventing diseases.1,2 However, despite the best nutritional and medical care, not all critically ill patients witness a favorable outcome after intensive care. Some patients may develop a state of persistent low-level inflammation, severe immunosuppression, catabolic abnormalities, and organ damage, known as Persistent Inflammation, Immunosuppression, and Catabolism Syndrome (PICS).3–5 A study in two level 1 trauma centers in the United States suggested that 19% of severe trauma patients had PICS, suggesting that PICS is a common clinical complication. 6 PICS patients often have prolonged conditions, long-term retention in ICU, need long-term close medical support, consume enormous medical resources, and have a high mortality rate and poor prognosis.7,8 A recent study explored the impact of PICS on the long-term prognosis of trauma patients, emphasizing the importance of early identification of trauma patients at risk of PICS-related complications in the ICU. Therefore, early screening of such high-risk patients and pre-intervention are the key to treatment. 9
Persistent Inflammation, Immunosuppression, and Catabolism Syndrome is mainly driven by a dysregulated immune response that leads to tissue damage and organ failure. 8 Cytokines are small proteins that mediate the communication between immune cells and regulate the inflammatory response. They include pro-inflammatory factors (IL-6, IL-17, TNF-α, IFN-γ) that promote inflammation and anti-inflammatory factors (IL-4, IL-10) that inhibit inflammation. Alongside cytokines, high-sensitivity C-reactive protein (HS-CRP) is a marker traditionally linked with systemic inflammation. 10 The balance between pro- and anti-inflammatory cytokines is crucial for maintaining homeostasis and resolving inflammation. However, this balance is disrupted in PICS patients, leading to chronic inflammation and immunosuppression. 11 Therefore, measuring the levels of cytokines in the early stage of critical illness may provide valuable information about the risk of developing PICS.
This study attempts to retrospectively collect the relevant information on critically ill patients in ICU. We aim to understand the potential role of cytokines in the early identification of PICS in critically ill patients.
Materials and methods
Study design, setting, and ethics approval
This study was conducted in the ICU ward of a tertiary grade A hospital in eastern China. It was part of a single-center retrospective study that adhered to the principles of the Declaration of Helsinki. All patients provided written informed consent for the study. The Dongyang People's Hospital Ethics Committee approved the study design and possible ethical issues (Approval number: 2021-YX-072).
Participants
Patients admitted to the ICU between December 2020 and January 2022 were enrolled in the study. The primary objective of this study was to evaluate the value of early measurement of cytokine levels in predicting the occurrence of PICS in ICU patients. Participants aged 18 years and older were included in the study. The exclusion criteria were: (1) age <18 years; (2) patients with a severe history of malignant tumor, autoimmune disease, or immunosuppression upon ICU admission; (3) length of hospital stay less than 14 days, including patients who died within this period; and (4) incomplete clinical data for main variables such as age, gender, and diagnosis.
All patients received standard treatment after admission, and the observation point was 14 days after admission to ICU. We assessed the presence of PICS by measuring clinical data on day 14; the specific diagnostic criteria are as follows 12 : (1) The patient’s body due to the ongoing inflammatory response. C-reactive protein (CRP) > 50 μg dL−1 (2) The patient was in a state of immunosuppression. Total peripheral blood lymphocyte count <0.80 × 109 L−1, (3) The patient was in a state of abnormal catabolism. Plasma albumin <3 g DL−1, pre-albumin <10 mg DL−1. In this study, patients who met the above diagnostic criteria were included in the PICS Group, and the rest in the non-PICS group.
Data collection
General clinical data and demographic characteristics of Critically ill patients admitted to the ICU were collected and recorded using our hospital’s Le Jiu data platform. The data encompasses various parameters: gender, age, BMI, and history of underlying diseases such as hypertension and diabetes. Additionally, nutritional scores were evaluated using the NRS2002 13 and the NUTRIC 14 scores at the time of ICU admission. Other details documented include the diagnosis leading to ICU admission, whether surgery was conducted, and the duration of the ICU stay. Laboratory indicators were collected on Day 1 and 14 of ICU admission. The indicators include blood routine (measured by Beckman-coulter LH 750 automated blood cell analyzer), coagulation function (measured by Sysmex CA-1500 coagulation analyzer), liver function and renal function, along with high-sensitivity C-reactive protein and procalcitonin (measured by Beckman Coulter AU5800 automatic biochemical analyzer). The APACHE II score on the first day of ICU admission was calculated based on the collected information and indicators. 15
For detecting cytokine levels (including IL-4, IL-6, IL-10, IL-17, TNF-α, and IFN-γ), all cases were measured by collecting venous blood in the morning on the 1st day of ICU admission, and serum was separated by centrifugation at 3000 r/min for 10 min, and stored at −80°C for detection. The cytokine levels were measured using enzyme-linked immunosorbent assay (ELISA) methods. The ELISA kits for these measurements were procured from J & L Biological, China. The specific batch numbers for the kits are as follows: IL-4 (JL19287), IL-6 (JL14113), IL-10 (JL19246), IL-17 (JL19255), TNF-α(JL10208), and IFN-γ(JL12191). For outlier data, we use the box diagram's interquartile distance (IQR) to detect outliers, and IQR is the difference between the upper and lower quartiles. We adopted 1.5 times IQR as the standard. We stipulated that points exceeding (upper quartile +1.5 times IQR distance or lower quartile −1.5 times IQR distance) were outliers, and the outliers screened out were treated as missing values.
Statistical analysis methods
This paper’s statistical data analysis was performed by applying SPSS 25.0 software. The measurement data were expressed as mean ± SD or median (upper and lower quartiles), and the two independent samples, the t test or Mann-Whitney U test, were used for comparative analysis. Counting data were expressed as adoption rates and percentages, and differences between groups were compared using Chi-square tests or Fisher’s exact tests. A multivariate logistic model was used to analyze and screen the independent influencing factors of PICS. Taking p < .05 was considered statistically significant.
For the outlier value, we use the box diagram’s interquartile distance (IQR) to detect outliers, and IQR is the D-value between the first and third quantile of the variable. One and a half times the IQR was considered the standard. We stipulated that values exceeding (upper quartile add one and a half times IQR distance or lower quartile minus 1.5 times IQR distance) were outliers, and the outliers screened out were treated as missing values.
For missing value data, we treat missing values according to the percentage of missing values if the incidence of missing values. If the incidence of missing values was less than 2%, we used the mean or median of the variable for continuous quantitative data and the mode attribute of the variable (i.e., the value with the highest frequency) for qualitative data to impute the missing values. If the missing ratio is greater than 2% and less than 15%, we excluded patients who had more than 15% of their data missing or incomplete, and we used multiple interpolation methods 16 to impute the missing values for the remaining patients who had less than 15% of their data missing or incomplete. Multiple interpolation methods estimate the missing values based on the available data and some assumptions, such as the distribution and correlation of the variables. All variables had a missing percentage of less than 15%.
Results
Initially, 132 patients admitted to the ICU in this study were included in our study, in which 9 patients died within 14 days of admission to the ICU. A total of 123 patients met the inclusion criteria for inclusion in this study (see Figure 1). After 14 days of hospitalization, a total of 39 patients met the diagnosis of PICS, and 84 patients did not meet the diagnosis of PICS. The incidence of PICS was 31.70%. The diagram showing the patient screening process.
Comparison of general clinical data between the two groups on the first day of hospitalization.
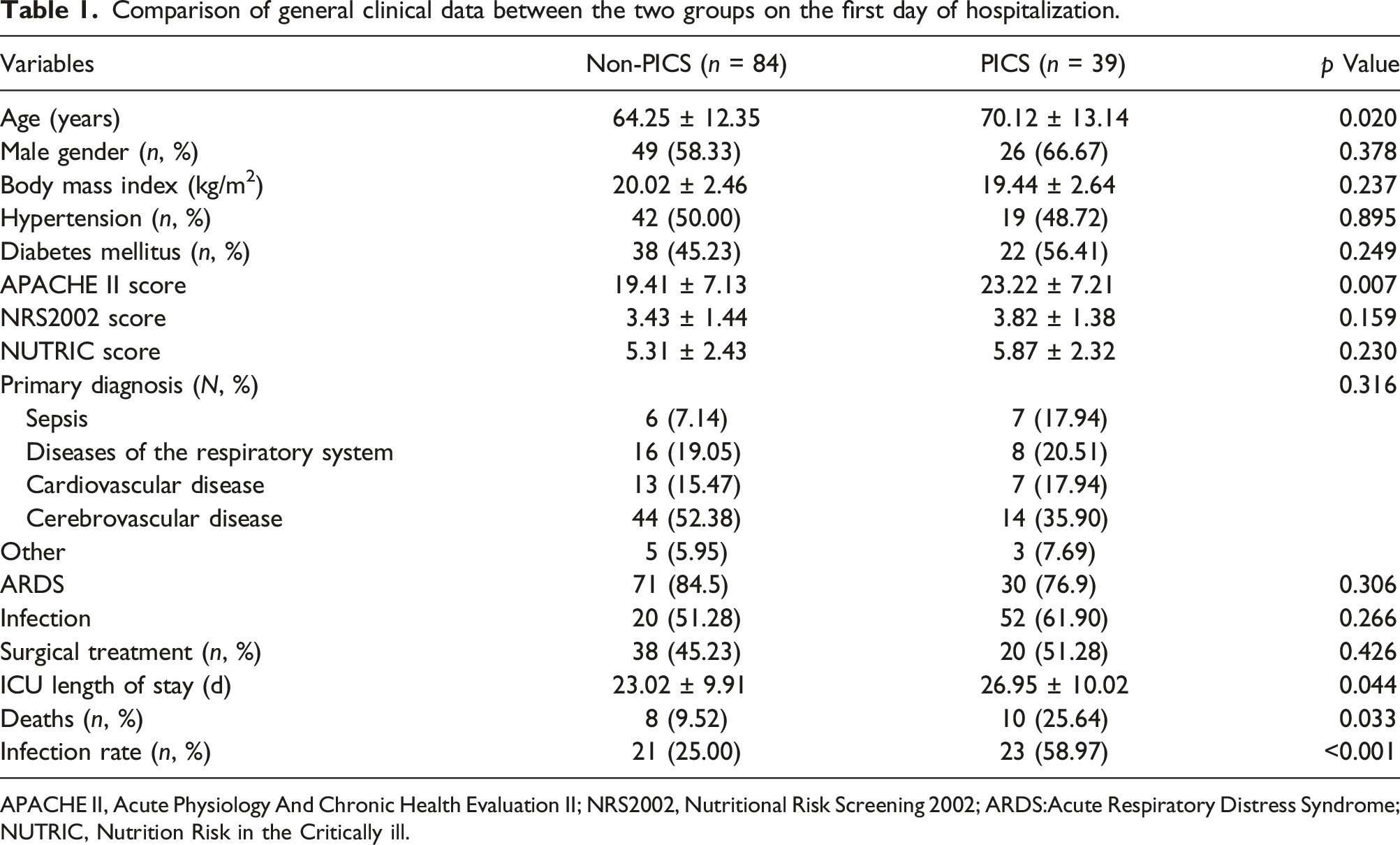
APACHE II, Acute Physiology And Chronic Health Evaluation II; NRS2002, Nutritional Risk Screening 2002; ARDS:Acute Respiratory Distress Syndrome; NUTRIC, Nutrition Risk in the Critically ill.
Comparison of laboratory indexes between the two groups on the first day of hospitalization.
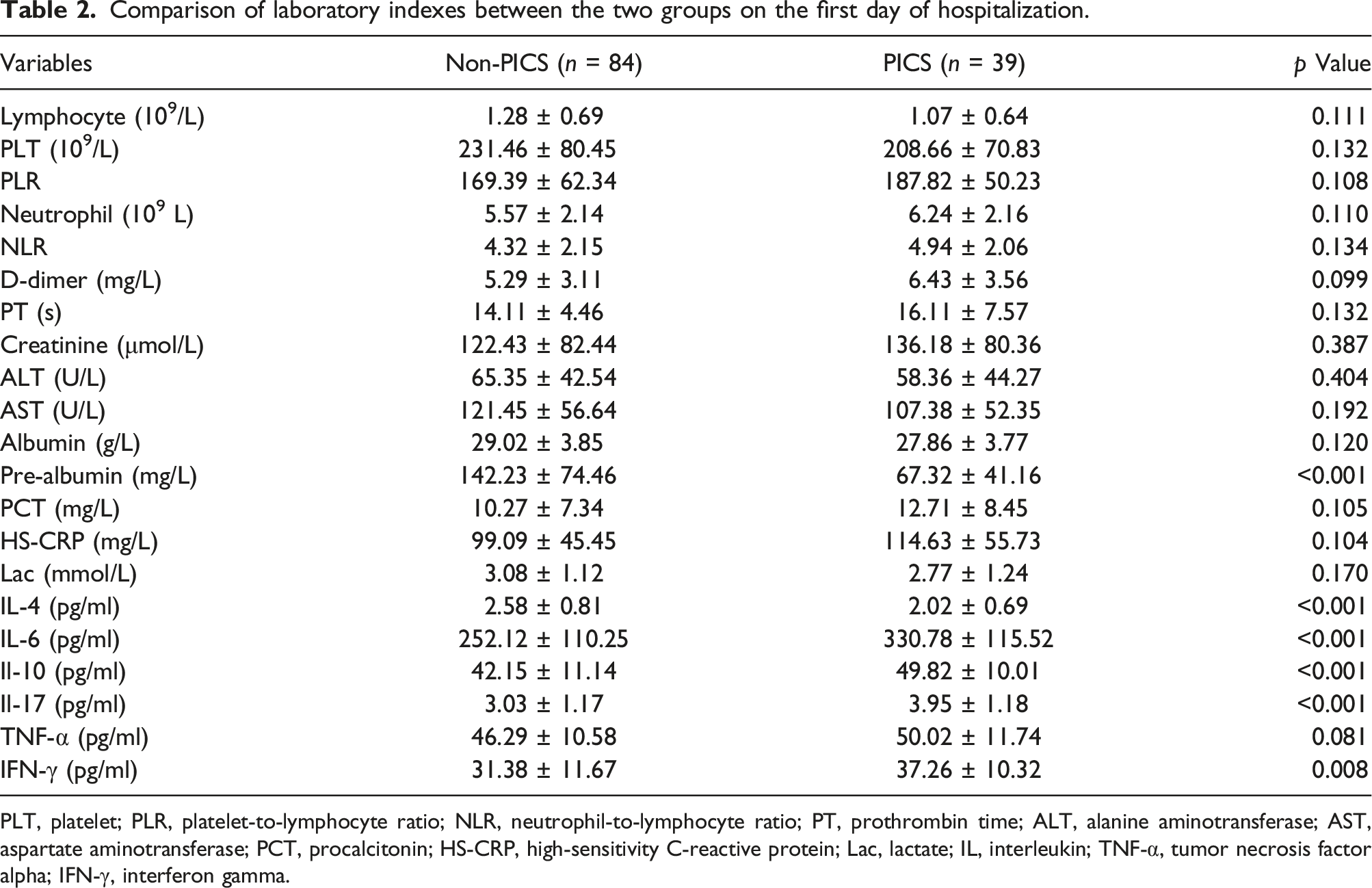
PLT, platelet; PLR, platelet-to-lymphocyte ratio; NLR, neutrophil-to-lymphocyte ratio; PT, prothrombin time; ALT, alanine aminotransferase; AST, aspartate aminotransferase; PCT, procalcitonin; HS-CRP, high-sensitivity C-reactive protein; Lac, lactate; IL, interleukin; TNF-α, tumor necrosis factor alpha; IFN-γ, interferon gamma.
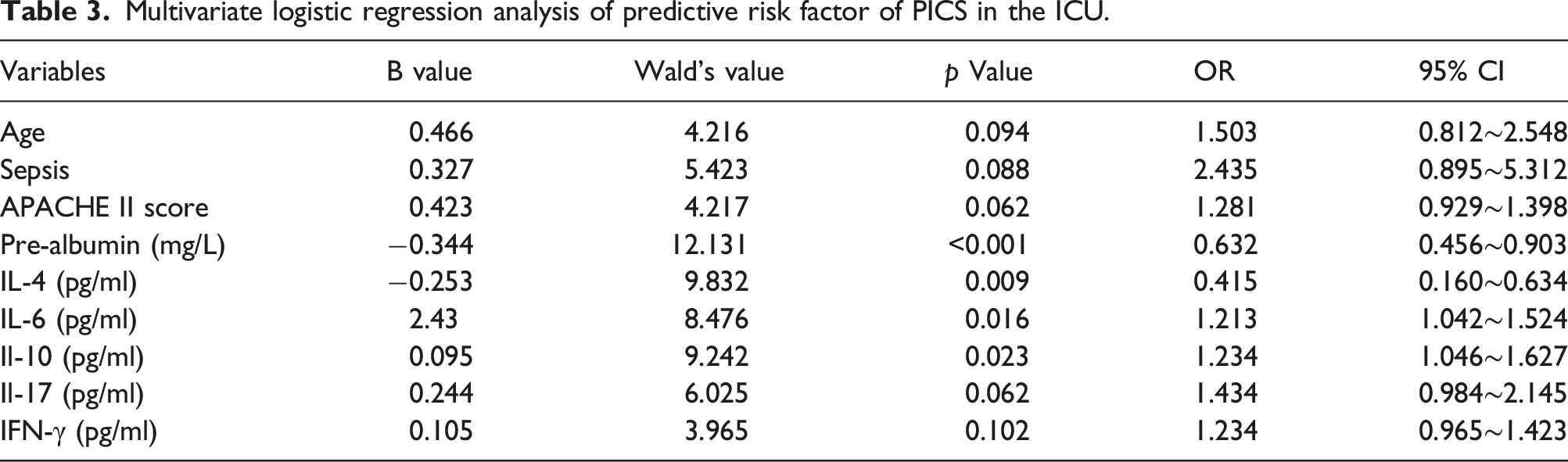
Multivariate logistic regression analysis of predictive risk factor of PICS in the ICU.
Discussion
Persistent Inflammation, Immunosuppression, and Catabolism Syndrome often arises as a complication of severe trauma or sepsis in ICU patients. It begins with an innate immune response to infection or trauma, characterized by the release of inflammatory mediators and an acute inflammatory response. Progression of the disease is marked by T lymphocyte depletion, apoptosis, and subsequent immunosuppression. This state can lead to nutrient synthesis decline, increased metabolic consumption, and malnutrition, exacerbating patient outcomes by impairing wound healing and increasing infection risk. In advanced stages, this can escalate to malignancy or mortality. 17
In our study, the incidence of PICS during ICU hospitalization was 31.70%, lower than the 43.1% reported by Hu 18 and about 60% reported by Nakamura. 19 This difference may be attributed to the study population’s inclusion and diagnostic criteria. Hu’s cohort included patients with a minimum 10-days hospital stay and conditions like intestinal fistula and acute ileus, which may increase the risk for PICS. Meanwhile, our study used a 14-days benchmark. Moreover, diagnostic criteria for PICS remain inconsistent across studies, with Nakamura redefining the CRP threshold at 3.0 mg/dl, diverging from our adherence to the 2012 standards. 12 Differences in healthcare environments and treatment protocols between studies could also significantly influence the observed variations in PICS incidence.
Our study observed a higher average age in the PICS group compared to the non-PICS group, suggesting that the former’s increased susceptibility may be linked to age-related immune decline and chronic inflammation. 20 Older adults’ multiple comorbidities and nutritional issues also contribute to this heightened risk. 21 Therefore, vigilant immune and metabolic monitoring, along with timely intervention, is particularly critical for elderly patients with severe diseases.
The APACHE II score, a well-established metric for assessing illness severity, emerged as an independent risk factor for PICS, corroborating the score’s predictive validity as reported in other critical conditions, including sepsis and COVID-19 pneumonia.22–26 Regarding the severity of their conditions, our data revealed that the PICS group possessed significantly higher APACHE II scores than the non-PICS group, indicating that they had more severe disease and organ dysfunction at admission. This group also experienced significantly greater mortality (25.64% vs 9.52%, p < .05) and hospital infection rates (58.97% vs 25.00%, p < .001) after 14 days compared to their non-PICS counterparts.
The presence of catabolic imbalance is a defining feature of PICS, with serum pre-albumin levels serving as a key indicator. Pre-albumin plays a dual role in metabolism and immune defense, which is particularly crucial during infections to eliminate toxic metabolites. 27 Despite robust nutritional support, severe cases, often exacerbated by sepsis, can result in marked malnutrition. Our data revealed significantly lower pre-albumin levels in PICS patients, establishing it as an independent risk factor and underscoring the urgency of addressing nutritional deficits to prevent PICS.
Persistent Inflammation, Immunosuppression, and Catabolism Syndrome’s pathology involves persistent inflammation and immunosuppression, leading to protracted tissue damage. A notable strength of our study is assessing several cytokines not previously extensively studied in PICS. In this study, the levels of IL-4, IL-6, IL-10, IL-17, and IFN-γ were statistically different between the two groups. Multivariate logistic regression analysis showed the levels of IL-4, IL-6, IL-10 were independent influencing factors for PICS in ICU patients. Delving deeper into the role of specific cytokines, IL-6 stands out in numerous inflammatory events, and its transient spike can also spur the release of counter-cytokines such as IL-10. The simultaneous increase in both pro-inflammatory (specifically IL-6) and anti-inflammatory markers (like IL-10) in the PICS group can be likened to the phenomenon of a “cytokine storm”. Broadly, this “storm” represents a hyperactive immune response characterized by the excessive release of interleukins, interferons, tumor necrosis factors, chemokines, and other mediators.28,29 Consistent with Mankowski’s findings, IL-10 in our study mirrored disease severity, particularly in the elderly with chronic conditions. 30 Reduced IL-4 implicates immunosuppression, while increased IFN-γ and IL-17 levels reflect their roles in inflammation and immune activation.31–33 These insights into cytokine dynamics in PICS patients underline the need for further research to fully elucidate their roles.
Acknowledging the limitations of our retrospective study design and the single-center, modest sample size, we recognize that these factors may impact the generalizability of our findings. One notable limitation was the incomplete collection of serum cytokine data on the 14th day of ICU admission, which may have provided additional insights into the progression of PICS. This gap underscores the need for more systematic data collection protocols in future research. Future studies could benefit from a prospective or cohort methodology and a larger, multi-center sample to validate and extend our results. Moreover, monitoring older patients with serious illnesses for immune and metabolic changes remains paramount for early intervention, a notion that is central to the management of PICS.
Conclusions
Our study found that the combination of cytokines, including IL-4, IL-6 and other indicators, is associated with the occurrence of PICS in ICU patients. This has implications for improving early diagnosis and intervention strategies for PICS in ICU patients.
Footnotes
Author contributions
This study was designed and conducted by YH, YW, and SG. YH and YW collected and analyzed the data. SG performed the ELISA assays. YH wrote the manuscript. WZ supervised the study and revised the manuscript. All authors read and approved the final version of the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jinhua Science and Technology Bureau Project (2022-3-014).
Data availability statement
All data included in this study are available on request from relevant authors.