
Abstract
Four patients with localized plaque psoriasis had used various systemic drugs along with topical cream. However, their skin lesions recurred, and the disease was refractory. After 2 weeks of discontinuation of oral and external medication, they were given three consecutive irradiation treatments with intense pulsed light once every 2 weeks for a 6-week period. After treating for 6 weeks, the erythema colors of the patients were evidently darkened, the scales were evidently reduced, and the skin lesions were significantly thinner or even flattened. The treatment was satisfactory, without occurrence of severe adverse reactions.
Introduction
As a chronic, inflammatory, immune-mediated systemic disease induced by genetic and environmental factors, psoriasis has a prevalence of about 1–4% of the world’s population. 1 Lifelong treatment is often required, and topical therapy plays an important role as first-line therapy for patients with mild to moderate psoriasis, especially for those with localized psoriasis vulgaris.
Intense pulsed light (IPL) is a wide spectrum of light with a specific wavelength. It produce high-energy flashes of light of several milliseconds’ duration with a broad wavelength spectrum, ranging from visible light to the infrared spectrum. Intense pulsed light sources operate on the principle of selective photothermolysis, can be used in a wide variety of conditions (e.g., telangiectases, spider nevi; superficial pigmentary changes; and epilation). 2 IPL was also used to treat some inflammatory skin diseases such as acne, 3 rosette acne, 4 etc. Psoriasis is also a chronic inflammatory skin disease. However, there are few reports on the treatment of psoriasis with IPL.
Case series
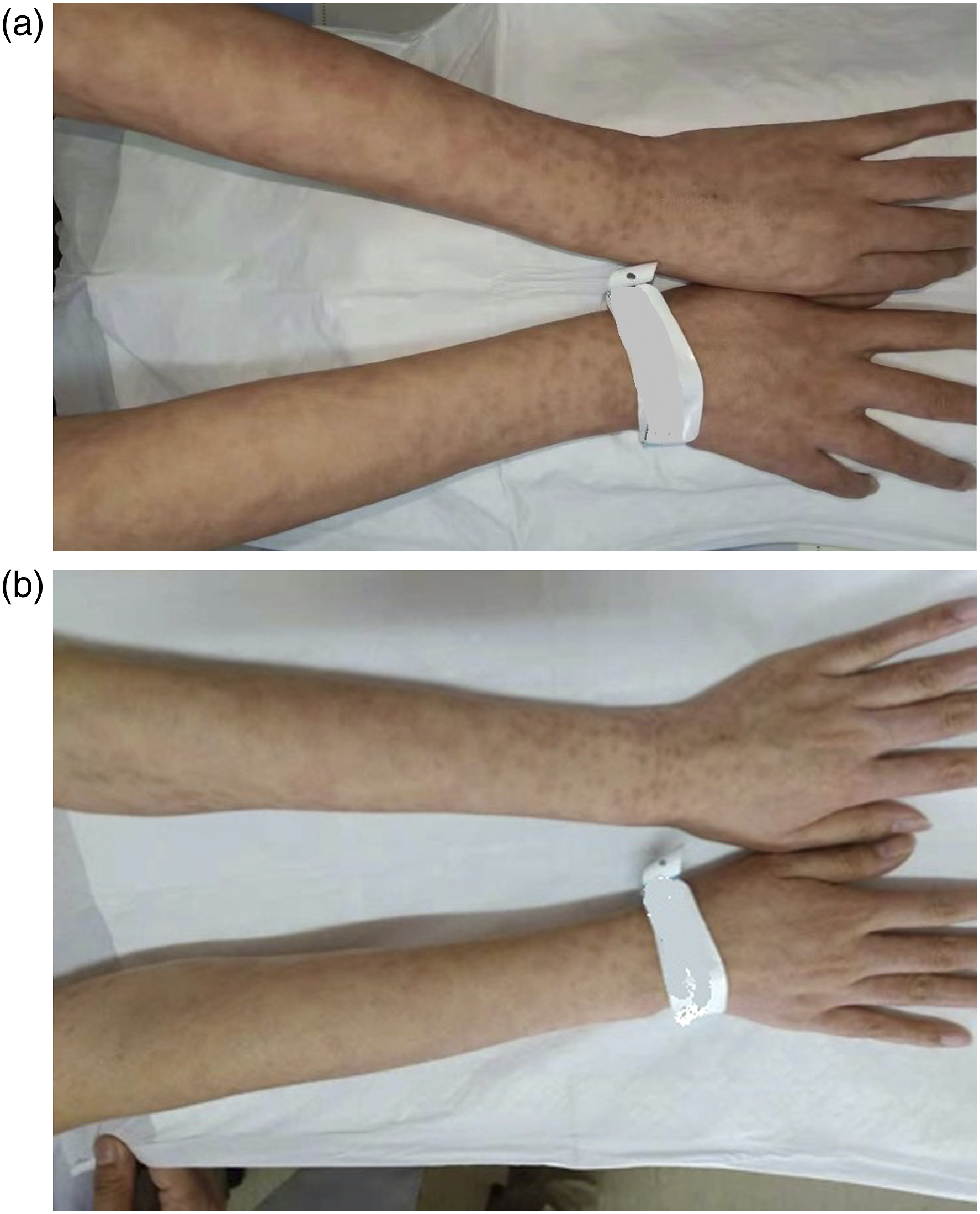
Four patients with localized plaque psoriasis, who were 28–60 years old with a disease course of 5–15 years, had used various systemic drugs including Acitretin, Xiaoyin (psoriasis-dissipating) Granules and Compound Glycyrrhizin Capsules, along with topical halometasone, mometasone furoate or calcipotriol cream. However, their skin lesions recurred, the disease was refractory and complete subsidence of partial localized skin lesions was hardly achievable. Case 1: A 28-years-old patient having skin lesions on bilateral lower legs, with a disease course of 5 years. The psoriasis area and severity index (PASI) score
5
was 8.4, and body surface area (BSA)
6
was 12%. (Figure 1(a)). Case 2: A 35-years-old patient having skin lesions on bilateral upper extremities, with a disease course of 8 years. The PASI score was 4, and BSA was 13%. (Figure 2(a)). Case 3: A 40-years-old patient having skin lesions on bilateral upper extremities, with a disease course of 10 years. The PASI score was 3.2, and BSA was 4%. (Figure 3(a)). Case 4: A 60-years-old patient having skin lesions on elbows and lower legs, with a disease course of 8 years. The PASI score was 8, and BSA was 7%. (Figure 4(a)). All the skin lesions conformed to the clinical features of psoriasis vulgaris, which were manifested as red infiltrative plaques with scaly surfaces. The scales could be easily scraped off, and membrane stripping and punctate hemorrhage were observable. (a) Pretreatment skin lesions on bilateral lower extremities (case 1). (b) Posttreatment skin lesions on bilateral lower extremities (case 1). (a) Pretreatment skin lesions on bilateral upper extremities (case 2). (b) Posttreatment skin lesions on bilateral upper extremities (case 2). (a) Pretreatment skin lesions on bilateral upper extremities (case 3). (b) Posttreatment skin lesions on bilateral upper extremities (case 3). (a) Pretreatment skin lesions on lower legs (case 4). (b) Posttreatment skin lesions on lower legs (case 4).


The 4 patients visited outpatient dermatologic clinic, where they were asked to discontinue relevant oral and topical drugs for 2 weeks. 2 weeks later, they were given three consecutive irradiation treatments with intense pulsed light (IPL; Energy to Healthcare Lumenis) once every 2 weeks for a 6-week period. The optical filter wavelength was 560/590 nm, and the spot size was 15 mm*35 mm. The triple-pulse OPT mode was adopted, the sub-pulse energy density was set at 18–20 J/cm2, the pulse width was 4.0–6.0 ms, the pulse delay was 20–40 ms, and the cooling method was contact cooling. Each patient was irradiated twice every time. During the treatment course, patients were instructed to avoid scratching or washing the skin lesions with hot water, and to apply white vaseline once daily.
PASI score before and after treatment.

TPSS before and after treatment.

Discussion
According to previous reports from foreign countries, the application of pulse dye laser (PDL) and IPL was somewhat efficacious in the treatment of nail psoriasis.8,9 Guarino F 8 applied PDL for treating nail psoriasis, finding that a 33% improvement was achieved at 12 weeks, as well as a 58% improvement at 24 weeks. Tawfik 9 AA found that the application of IPL with a 550–1200 nm filter was also efficacious in treating nail psoriasis. Twenty patients with toenail psoriasis received about eight treatments with IPL, and the results showed that the nail bed improved by 71.2%, while the nail stroma improved by 32.2%, with an overall the nail psoriasis severity index (NAPSI) of 82.4%. 9 Suggestively, IPL is a promising treatment for nail psoriasis. In this study, 4 patients with localized psoriasis vulgaris were treated with IPL for refractory skin lesions. Remarkable clinical efficacy was achieved, and the treatment process was safe and the patient tolerance good.
The specific psoriasis-treating mechanism of IPL is unclear, which may be attributed to the following reasons: (1) IPL can coagulate the dilated blood vessels in the dermal papillae based on the principle of selective photothermy, thereby exterting a therapeutic effect 10 ; (2) molecular mechanism of action: IPL has been found to down-regulate the tumor necrosis factor, a presumed therapeutic target of IPL. 11 Further researches are required to confirm these theoretical speculations, with a view to providing a basis for the clinical application of this technique.
Conclusion
Our treatment of these patients demonstrated that IPL was effective in the treatment of localized plaque psoriasis. IPL can be a potential therapeutic modality for localized plaque psoriasis and further clinical trials are still needed to confirm its efficacy.
Footnotes
Acknowledgements
We are very grateful to the patients who participated in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our study did not require an ethical board approval because this is a case series, not a research, so we didn’t apply for ethical approval.
Informed consent
Written informed consent was obtained from these patients for their anonymized information to be published in this article.