
Abstract
Morphea is a rare fibrosing disorder of the skin and underlying tissues. To date, the size of morphea has not been adequately discussed. Here, we report two cases of small-sized superficial circumscribed morphea. Both cases clinically revealed single circumscribed, round to oval area of shiny sclerotic plaque at distal extremities. There are several options for the treatment of superficial circumscribed morphea, such as topical corticosteroid and phototherapy. The early recognition of small-sized morphea enables appropriate diagnosis and follow-up, leading to improve disease prognosis.
Introduction
Morphea, or localized scleroderma, is a rare fibrosing disorder of the skin and underlying tissues. 1 The disease is characterized by extra deposition of collagen leading to thickening of the skin. The early lesions of morphea clinically present as erythematous patches and plaques, while fully developed lesions are asymmetric sclerotic plaques. 2 Although morphea lesions are generally reported to be relatively large (>5 cm), 3 the clinical features of small-sized lesions (<5 cm) have been poorly discussed. In this study, we report two cases of small-sized superficial circumscribed morphea which probably represent the early lesion of the disease, and discuss the importance of early recognition of morphea.
Case Presentation
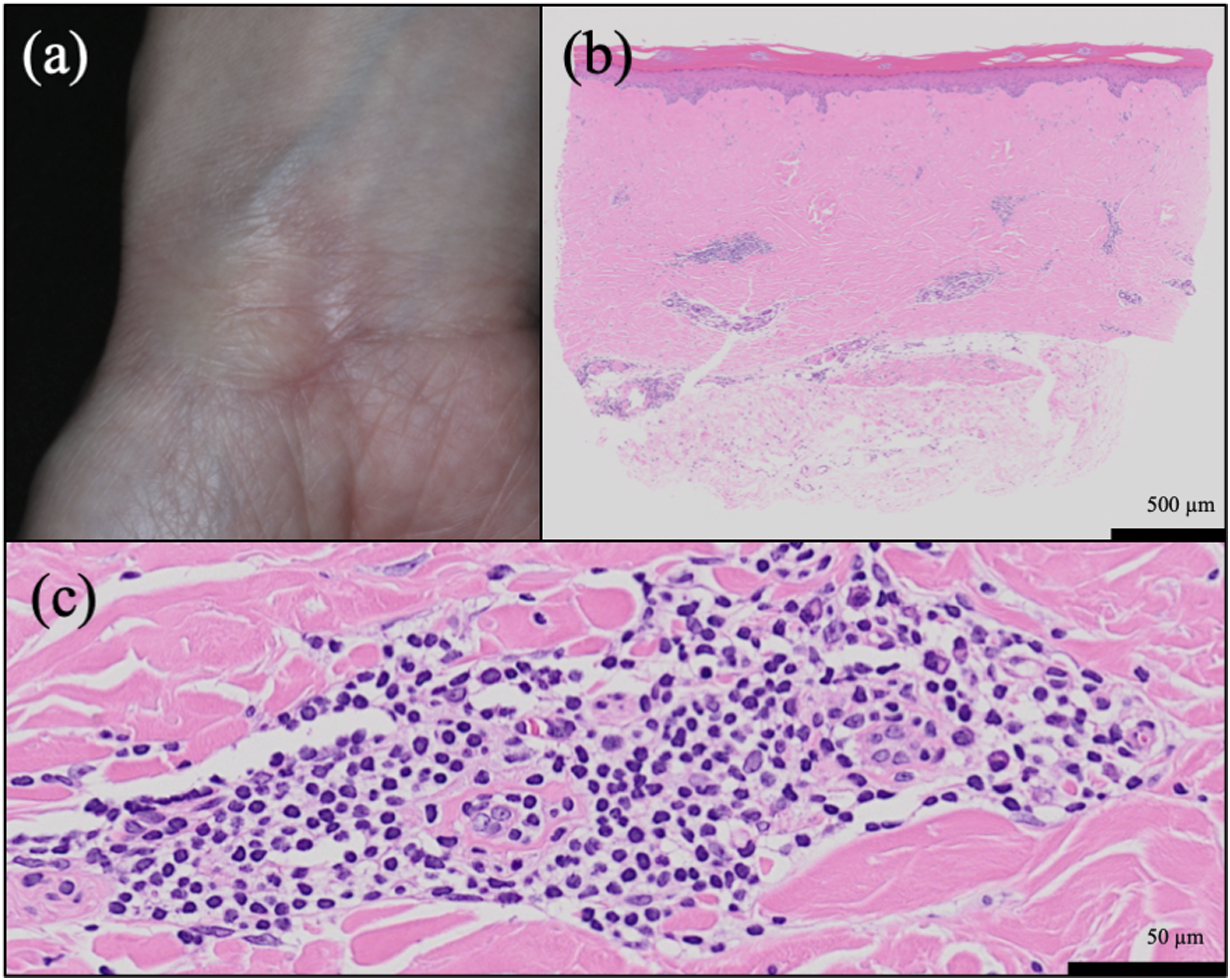
Patient one is a 41-year-old previously healthy woman presenting with a 1-year history of a white plaque on her left ring finger, which developed without any particular inducement. Patient two is a 40-year-old healthy woman presenting with a 2-months history of a white plaque on her right wrist. Patient two had a history of trauma to the same area 2 years ago. Physical examination revealed a circumscribed, oval or round area of shiny sclerotic skin that was 22 × 10 mm in size in patient 1 (Figure 1(a)) and 32 × 36 mm in size in patient 2 (Figure 2(a)). In patient 2, the sclerotic plaque was accompanied by an erythematous border (Figure 2(a)). Neither patient complained of symptoms, and there was no laboratory abnormality suggestive of systemic sclerosis. Histopathology revealed thickened and homogenized collagen bundles at the papillary and reticular dermis, mixed inflammatory cell infiltration (both patients), atrophic appendages (patient 1), and packing of sweat glands (patient 2) (Figures 1(b), 1(c), 2(b) and 2(c)). Subcutaneous infiltration and sclerosis were not evident. On the basis of these findings, we made a diagnosis of superficial circumscribed morphea. Topical high potency corticosteroid was initiated to these patients, and the size of lesions decreased after 4 weeks. Thereafter, the size of these lesions remained unchanged without treatment. Patient 1. (a) Clinical presentation. A 22 × 10 mm, circumscribed, oval area of shiny-white sclerotic skin on the left ring finger. (b, c) Histopathological findings revealing thickened and homogenized collagen bundles at the papillary and reticular dermis, mild inflammatory infiltration, and atrophic appendages (hematoxylin–eosin [HE], (b): ×10 original magnification; (c): ×100 original magnification). Patient 2. (a) Clinical presentation. A 32 × 36 mm, circumscribed, round area of shiny sclerotic plaque accompanied by an erythematous border. (b, c) Histopathological findings revealing thickened and homogenized collagen bundles at the papillary and reticular dermis, packing of eccrine glands, and perivascular infiltration of lymphocytes and plasmacytes (HE, (b): ×10 original magnification; (c): ×200 original magnification).
Discussion
Morphea is a rare fibrosing disorder of the skin and underlying tissues characterized by thickening of the skin resulting from inflammation and the deposition of collagen-rich extracellular matrix.1,4 Based on the clinical phenotype, morphea is classified into several subtypes, of which circumscribed morphea is the most common variant in adults. 5 Superficial circumscribed morphea is described as single or multiple and oval or round circumscribed areas of sclerosis limited to the dermis, often accompanied by altered pigmentation.6,7 In early active morphea, a violaceous or erythematous border, called the characteristic ‘lilac ring,’ is also observed. 6 Histopathological findings revealed perivascular infiltration composed of lymphocytes and plasma cells in early active morphea, and sclerotic skin demonstrating thickened and homogenized collagen bundles at the papillary and reticular dermis. The abundant collagen bundles enclose eccrine glands, and a few dermal vessels with fibrotic walls and narrow luminae may be observed as the sclerosis progresses.4,6 Early active morphea with indistinct sclerosis sometimes clinically and histopathologically simulates other inflammatory dermatoses such as mycosis fungoides. 8 In the present study, patient two presented 2 months after disease onset, and she was diagnosed with early active morphea based on the clinical manifestation of a ‘lilac ring’ and histopathological lymphocytic perivascular infiltration. Conversely, patient one visited our site 1 year after presentation, and the histopathological findings mainly included thickened and homogenized collagen bundles at the dermis and atrophic appendages.
It is noteworthy that the size of the morphea was fairly small in both cases. To date, only one report reviewed the size of morphea, which suggested that approximately 80% of the lesions were relatively large (>5 cm).
3
Furthermore, 90% cases of small-sized morphea showed multiple and disseminated lesions, and only 10% showed a single lesion. Small-sized morphea as described in the present case, particularly in patient 1, has not been reported previously. The underlying etiology of morphea remains unclear. The development of morphea is believed to be associated with environmental factors (e.g. trauma, radiation, medications, infections) and autoimmunity.1,9 In patient 2, the onset of morphea was possibly triggered by trauma 2 years previously, although she had no autoimmune predisposition. However, in patient 1, morphea appeared without any particular inducement. In the majority of cases, the skin softens in months to years, and the disease is self-limiting within three to 5 years. However, in some cases, morphea remains progressive and grows in size for multiple years, or flares of disease occur frequently.
6
The early recognition of small-sized morphea enables appropriate diagnosis and follow-up. Currently, no consensus regarding the optimal treatment for morphea has been reached. There are several options for topical therapy, such as topical corticosteroid and phototherapy, often used particularly in the most superficial and limited forms of morphea, such as superficial circumscribed morphea. Topical corticosteroids, especially high potency corticosteroids, have traditionally been recommended on morphea, particularly during the early, most inflammatory stages. Phototherapy is particularly effective in the fibrotic phase of morphea, although it is not very useful in patients with aggressive forms of the disease characterized by involvement of the subcutaneous tissue and muscle.
10
The early diagnosis of morphea may lead to control the disease with less invasive treatment before the progression in long-term growth disturbance, contractures, deformity and muscle atrophy that require systemic treatment.
Conclusions
In summary, we present two cases of small-sized superficial circumscribed morphea. Morphea should arise as a differential diagnosis of small-sized sclerotic lesions, in order to achieve an early diagnosis and less invasive treatment. The early recognition of small-sized morphea enables appropriate diagnosis and follow-up, leading to improve disease prognosis.
Footnotes
Acknowledgements
We wish to acknowledge our patients as well as all members of our laboratory for their helpful advice.
Authors contributions
HH wrote the manuscript, NT revised the manuscript, HH did the data analysis, and HH did the data collection. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from *the Kyushu University Institutional Ethics Committee (30-363; 27 November 2018)*.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images as per our standard institutional rules.