
Abstract
This study set out to investigate the number and the activation of peripheral blood basophils, and the correlation analysis between peripheral blood basophils and disease activity in patients with rheumatoid arthritis (RA). It was determined whether these indices could be used as a monitoring index of RA activation and thereby provide a new disease assessment method for RA. Using flow cytometry, the number and activation level of peripheral blood basophils were determined in RA patients compared with healthy donors. General clinical data were collected and laboratory indices of RA patients were analyzed. A correlation between the number and the activation of basophils was determined using the Disease Activity Score 28 (DAS28), anti-cyclic citrullinated peptide (CCP), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP).The absolute count and percentage of peripheral blood basophils in RA patients were significantly lower than that of controls (absolute count P = 0.033, percentage P = 0.047). However, the activation level of basophils was significantly higher than that in controls (P = 0.034). In addition, the activation level of basophils showed statistically significant differences in disease groups with different activities (P = 0.011, P = 0.037, and P = 0.002). With an increasing DAS28 score, the number of peripheral blood basophils was shown to decrease while activation level increased. The absolute count and activation level of basophils in RA patients and normal controls on receiver operator characteristic (ROC) curves were (area under the curve (AUC) = 0.676, P = 0.025; AUC = 0.694, P = 0.014), respectively, which were statistically significant in differentiating RA patients from controls. The activation level of basophils was positively correlated with CCP (P < 0.001, r = 0.831), was positively correlated with CRP (P = 0.001, r = 0.588). These data are correlated with disease activity assessment and can be used as an early monitoring index of RA activity. Therefore, these studies provide a new basis for evaluation of clinical disease activity in RA patients.
Introduction
Rheumatoid arthritis (RA), characterized by chronic and destructive joint lesions, is a systemic immune disease. Primary manifestations of the disease are symmetrical joint arthritis of both hands, wrists, and feet, along with additional complex clinical manifestations. 1 It is sometimes accompanied by fever, anemia, subcutaneous nodules, pulmonary fibrosis, lymph node enlargement, and other extra-articular manifestations. The RA is a progressive and aggressive disease. Without immediate treatment, the disease will gradually develop causing the invasion and destruction of bones and joints. Eventually, it will result in ankylosis, deformity, functional incapacitation, and varying degrees of disability. RA patients need to monitor the disease activity regularly after remission, so that intervention treatment can be carried out in the early stages of disease activity. Current RA disease activity monitoring indexes used to evaluate the disease activity of RA are still limited to rheumatoid factor (RF), cyclic citrullinated peptide (CCP), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), arthroncus, and tenderness number. These indicators have poor specificity and sensitivity and cannot reflect disease activity as early as possible. Therefore, doctors need simple and effective indicators with high specificity and sensitivity to monitor and judge the condition of RA in clinical treatment.
Normally, there are few basophils in the peripheral blood (<1%). An understanding of basophils function has been limited to mediation of the immunoglobulin E (IgE) hypersensitivity pathway. 2 With the application of special cell lines, monoclonal antibodies, and high purity cell sorting technology, the study of basophils has advanced in recent years. It has been found that basophils are not only involved in classic IgE-mediated hypersensitivity, but also are involved in immune regulation reactions by enhancing immune response memory and other aspects of adaptive immunity.3,4 For example, Denzel et al. 5 found that basophils can increase the production of antibodies. The activation of basophils and T cells can significantly increase the proliferation of B cells and the production of immunoglobulins. Increasing studies have shown that activated basophils can produce Th2 cytokines, such as interleukin-4 (IL-4) and interleukin-13 (IL-13), influencing the balance of Th1/Th2. 6 In addition, basophils may be involved in the pathogenesis of various autoimmune diseases, including RA and systemic lupus erythematosus, and thus, may be related to disease activity. However, studies on the role of basophils in RA are limited. Therefore, the studies presented here sought to detect the number and activation level of peripheral blood basophils in RA patients. This study was conducted to correlate peripheral blood basophils and disease activity in order to establish a new, simple, and effective method for RA monitoring.
Materials and methods
Research subjects
In this study, 27 untreated RA patients were selected who were hospitalized in Shengjing Hospital, Department of Rheumatology and Immunology, from September 2016 to February 2017. All selected patients conformed to the RA classification criteria recommended by American College of Rheumatology (ACR) 2009 and their personal medical histories were recorded in detail. When they were in hospital, the patients began to treat with disease-modifying anti-rheumatic drugs (DMARDS), such as methotrexate, leflunomide, sulfasalazine. Any patients, with other severe systemic diseases or other immune diseases, were excluded. The control group included 28 sex- and age-matched volunteers with no other basic diseases who were tested over the same time period.
According to the Rheumatoid Arthritis Disease Activity Score 28 (DAS28), all patients were divided into three groups with different disease activities. The criterion was as follows: DAS28 < 3.2 was the low disease activity group, 3.2 ⩽ DAS28 ⩽ 5.1 was the moderate disease activity group, and DAS28 > 5.1 was the high disease activity group.
Methods
EDTA anticoagulated peripheral blood (2 mL) was collected from the eligible RA patients and healthy volunteers. Laboratory general clinical data and the DAS28 scores of the RA patients were collected. Informed consent of the patients and volunteers was obtained before specimen collection. The number and activation level of peripheral blood basophils of RA patients and healthy volunteers were detected using flow cytometry (Figure 1). All samples were tested within 3 h. The CD203c allophycocyanin (APC) and CD123 fluorescein isothiocyanate (FITC) antibodies (eBioscience, USA) were added to 50 µL blood samples and mixed on an oscillator 1 min. 2 mL Erythrocyte lysate was added to the specimens after 15 min of reaction without light and then the specimen were left to react for 11 min after mixing. The samples were centrifuged for 4 min at 900 r/min. The clear supernatant was discarded. Then 1 mL phosphate buffer saline (PBS) was used to resuspend the pellet followed by centrifugation second time at 900 r/min for 4 min. The clear supernatant was again discarded. The pellet was resuspended in 310ulPBS and subject to flow cytometry by fluorescence activated cell sorting (FACSCalibur, # E97500357, software MultiSET V2.2). Results were represented as the number of CD123 FITC positive cells, and the percentage of CD123 FITC positive cells in leucocyte and CD203c Median.

The flow cytometry scatter plot of basophils.
Clinical data
Clinical data, including CCP, CRP, ESR, and other indicators were collected from the medical records.
Statistical analysis
Statistical analysis was carried out by IBM SPSS19.0 and GraphPadprism5.0. These products analyze whether the data between different groups are statistically significant through independent sample t test and one-way analysis of variance. The homogeneity test of variance and multiple comparisons were carried out by Levene and Bonferroni/Tamhane, respectively. The correlation between data and diagnostic significance of experimental indexes were analyzed by the Spearman correlation and receiver operator characteristic (ROC) curve, respectively. All statistics were described by mean and standard deviations such that statistical significant was determined when P < 0.05.
Results
Basic features of patients
There were 27 RA patients (22 females and 5 males) in this study with an average age of 57 ± 14 years .The average DAS28 score was 4.41 ± 1.19. There were 8 RA patients in the mild disease activity group (DAS: 2.88 ± 0.41), 10 RA patients in the moderate disease activity group (DAS: 4.48 ± 0.44), and 9 RA patients in the severe disease activity group (DAS: 5.68 ± 0.27). The average age of the 28 healthy volunteers was 40 ± 15 years. Other clinical data are shown in Table 1.
Characteristics and laboratory data of patients and healthy controls.

WBC: white blood cell; CD203: cluster of differentiation 203; DAS28: Disease Activity Score 28; CCP: cyclic citrullinated peptide; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; RA: rheumatoid arthritis.
Values are shown as mean ± SD. The data are from 28 healthy controls and 27 RA patients, who were divided into four groups with DAS28 scores.
Compared with the controls, the absolute count, and percentage of peripheral blood basophils of RA patients decreased and the activation level increased significantly
Experimental results showed that the number of the peripheral blood basophils of RA patients (absolute count: 17.30 ± 15.28/μL; percentage of basophils: 2.79 ± 1.98%) was significantly lower than those in the control group (absolute count: 28.14 ± 21.09/μL; percentage of basophil: 4.11 ± 2.73%) (P = 0.033; P = 0.047) (Figure 2(a) and (b)); the difference was shown to be statistically significant. The fluorescence intensity CD203 median of the peripheral blood basophils from RA patients (34.63 ± 11.28) was statistically higher than the fluorescence intensity CD203 median of controls (27.14 ± 14.06) (P = 0.034) (Figure 3(c)). The difference was shown to be statistically significant (Figure 2).

The relationship between the number of peripheral blood basophils and the activation of RA patients and controls: (a) absolute count of basophils from the two groups, (b) percentage of basophils in the peripheral blood from the two groups, and (c) activation level of basophils from the two groups.

Basophils CD203 median in different disease activity groups.
Elevated activation intensity of peripheral blood basophils in patients with RA in the high disease activity group
Results showed that comparisons of peripheral blood basophils fluorescence intensity CD203 median of RA patients in different disease activity groups were statistically significant. Comparison of results was conducted between the mild disease activity group and the moderate disease activity group (P = 0.011), between the mild disease activity group and the severe disease activity group (P = 0.002), and between the moderate disease activity group and the severe disease activity group (P = 0.037). It is suggested that the degree of activation of peripheral blood basophils increases with the increase of disease activity score in patients with RA (Figure 3). The absolute count and the fluorescence intensity of peripheral blood basophils were significant in differentiating RA patients from controls
Correlation of the absolute count and the fluorescence intensity of basophils was analyzed in patients with RA from controls by the ROC curve. The area under the curve (AUC) of the absolute count of basophils was 0.676 (P = 0.025) (Figure 4(a)) and the AUC of basophil fluorescence intensity was 0.694 (P = 0.014) (Figure 4(b)). The differences were statistically significant (Figure 4).

ROC curve of the absolute count and the fluorescence intensity of basophils in RA patients and healthy controls: (a) AUC of the absolute count of basophils, (b) AUC of the basophil fluorescence intensity.
Correlation analysis between the activation level of peripheral blood basophils in RA patients and the laboratory indexes
Through the Spearman correlation analysis, it was found that the activation level of peripheral blood basophils in RA patients was positively correlated with CCP (r = 0.831, P < 0.001) (Figure 5(a)) and CRP (r = 0.588, P = 0.001) (Figure 5(b)); it was not correlated with ESR (r = 0.029, P = 0.885).
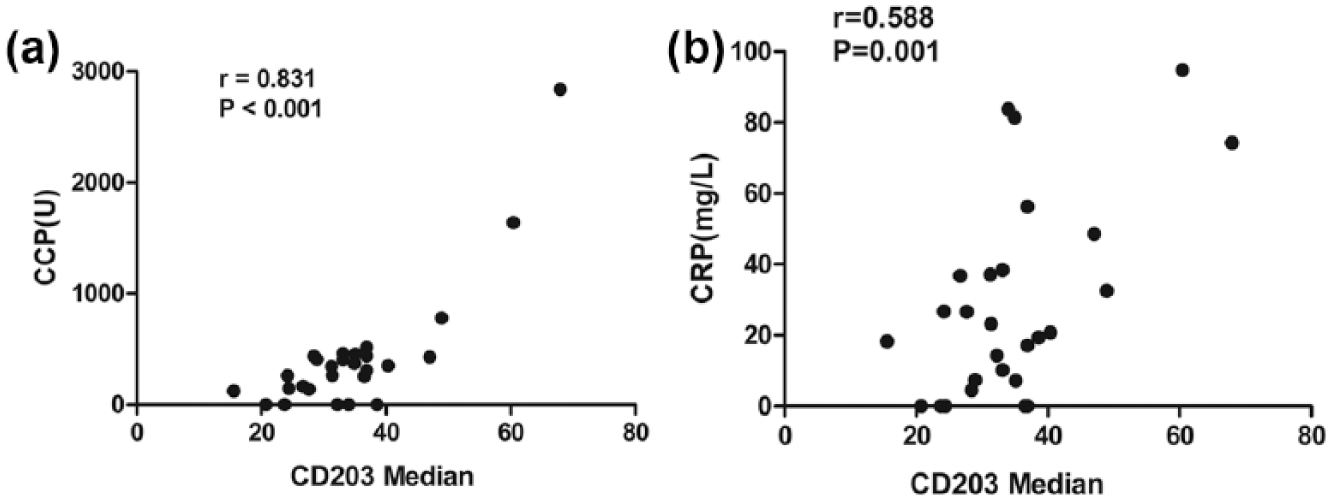
Correlation between the activation level of peripheral blood basophils in RA patients with CCP and CRP.
Discussion
RA is a common chronic autoimmune disease characterized by the infiltration of inflammatory cells in the joint synovium. In addition, the pathogenesis of RA was not clear yet. It may be related to heredity, immune disturbance, infection, endocrine, and environmental factors. Recent a study found that the imbalance of Th1/Th2 response may play an important role in the development of RA. 7 Moreover, a study also found that Th2 response is the main element in peripheral blood in the early stage of RA, while Th1 response is the main element in the later stage. 8 Early diagnosis and early treatment can control the disease in time. To find the appropriate indices of early monitoring of RA disease activity, the study presented here sought to detect the number of peripheral blood basophils by examining the expression of CD203c, an activation marker of basophils, in RA patients and controls. Flow cytometry was the method used for detection of CD203c basophils. These studies showed that the absolute number and percentage of peripheral blood basophils in RA patients were significantly lower than those in controls. Kroeger et al. 9 showed that the number of peripheral blood basophils in RA patients decreased. This was attributed to basophil functions that include secretion of cytokines and inflammatory factors, participation in pathogenic autoimmune diseases, and migration from peripheral blood to draining lymph nodes, and expression of major histocompatibility complex II (MHC II) molecules. Additionally, basophils express co-stimulatory molecules and function in antigen presentation to initial T lymphocytes. Activation is the committed step for basophils to achieve these biological functions. 10 The research of the activation mechanism also evolved from classical IgE mediated to multiple pathways. Human basophils can produce a series of toll-like receptors (TLR), including TLR2, TLR4, TLR9, and TLR10. 11 TLR initiates the activating signal transduction pathway to induce the production of cytokines and effector factors by identifying and combining with the pathogen-associated molecular patterns. 12 The abnormal activation of TLRs signal will lead to infections, allergic diseases, and autoimmune diseases. As the effector cell of the emergence and development of RA, basophils can be highly activated by TLR and further aggravate the progress of the disease. Bieneman et al. 13 showed that ligands of the TLR2 peptidoglycan can stimulate basophils to secrete Th2 cytokines in vitro, enhancing the release of cytokines in the IgE pathway. In addition, these ligands activate the nuclear factor-kB (NF-kB) intracellular signal transduction pathway, and thus aggravate RA. The results presented here showed the fluorescence intensity of peripheral blood basophils with RA patients was higher than those in controls (P = 0.034). Meanwhile, our study also showed that the compression of peripheral blood basophils fluorescence intensity CD203 median of RA patients in different disease activity groups were statistically significant (P = 0.011, P = 0.037, P = 0.002). In addition, it was confirmed that with an increase in the DAS28 score, the activation level of basophils increased. Thus, it was shown that the absolute count and the fluorescence intensity of peripheral blood basophils were significant in differentiating RA patients from controls, the absolute count AUC was 0.676 (P = 0.025), and the activation level AUC was 0.694 (P = 0.014). These results indicate that basophils are involved in the pathogenesis of RA. From this study, it was also determined that the activation level and number of basophils can be used as an index to monitor the disease activity of RA, in a manner even more sensitive than the DAS28 score.
The correlation between the fluorescence intensity of basophils and the common laboratory indexes (CCP, CRP, and ESR) was analyzed in the research. Our research has also shown that the activation level of basophils is positively correlated with CCP (r = 0.831, P < 0.001). CCP is considered to be highly specific to RA. The higher the CCP value, the worse the RA prognosis, and the greater the degeneration of the joint. 14 It was found from a murine joint model of RA that increasing CCP indicates increased joint damage. Conversely, the reduction of CCP can alleviate the progression of joint injuries. 15 Basophils can be activated by IgE-dependent or IgE-independent pathway. In addition, IgE antinuclear antibodies exist in the serum of RA patients in the form of immune complexes, which can activate basophils.16,17 Besides, a study reported that IgE immune complexes were present in RA patients especially the patients with severe arthritis and nodular vasculitis. 18 In addition, the etiology of CCP positive RA is significantly different from that of CCP negative RA. Huizinga et al. 19 and Verpoort et al. 20 found that the human leukocyte antigen (HLA) genotype expression was different in the two types of RA patients. And a study had shown that CCP positive and CCP negative RA patients were different in clinical manifestations and treatment strategies. 21 It has been reported that immune complexes formed by citrullinated proteins and type IgE against citrulline synthesis protein antibodies (ACPA) can activate basophils in RA patients by cross-linking with the FcεRI receptor. The immune complex induces macrophages to release tumor necrosis factor-α (TNF-α) inflammatory factors by cross-linking with FcγRIIa to aggravate RA. 22 However, there was no significant correlation between the fluorescence intensity of basophils and ESR (P = 0.885, r = 0.029). ESR is easily influenced by some factors, such as infection, anemia. Compared to ESR, basophils can reflect a more authentic and reliable disease activity as early as possible.
In conclusion, the studies presented here showed that the number and activation level of peripheral blood basophils are an appropriate indicator of early monitoring of RA disease activity. This method can be used in both clinical early diagnosis and long-term monitoring providing be a new, simple, and effective way of monitoring RA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by a grant from the Project of Shenyang City Science Foundation (no. F14-158-9-44).