
Abstract
This case report presents aortic dissection with aneurysm (ADA) related to Salmonella infection. An 84-year-old male patient was admitted to our hospital for fever and chest pain. Chest computed tomography (CT) showed ADA. The patient underwent aortic dissection and cavity isolation surgery; subsequently, the patient was found to be febrile. Blood culture detected the presence of Salmonella infection. We concluded that the case presented was mycotic aneurysm due to Salmonella infection.
Case report
An 84-year-old male patient with a history of Parkinson’s disease was admitted to our hospital for fever and chills for 48 h with a maximum temperature of 40°C. Physical examination revealed unremarkable results. Laboratory tests indicated the following: normal white blood cell count, 7040/mm3; increased neutrophil levels, 93.7%; C-reactive protein, 74.7 mg/L; and procalcitonin, 20.05 ng/mL. Blood culture indicated that no bacteria were present, and other laboratory tests showed normal results. Echocardiography as well as computed tomography (CT) of the chest and abdomen showed no clear evidence of focus of infection other than limited inflammation of the right upper lung (Figure 1(a)). The patient was treated with meropenem for broad coverage of pathogenic bacteria. After 4 days, the patient remained febrile with a temperature of up to 39.6°C and suffered from chest pain, particularly on the left side chest. A chest CT scan revealed pleural effusion on the left side (Figure 1(b)). Pleuritis was identified as the cause of fever and chest pain. Levofloxacin was given as an anti-infective; however, fever persisted and chest pain worsened. Notably, chest pain was not aggravated by coughing or breathing; thus, pleuritis was ruled out as cause of complaints. Contrast-enhanced chest CT scan was conducted, revealing an aortic dissection with aneurysm along the horizontal line from T10 to T11 (Figure 1(c)). On the basis of the clinical symptoms, aortic dissection with aneurysm (ADA) caused by infection was potentially present. The patient subsequently received aortic dissection cavity isolation (Figure 1(d)). Combined piperacillin sodium/tazobactam sodium was used to treat infection. After surgery, the chest pain was relieved, and the temperature fluctuated between 37°C and 39°C. Blood was extracted again from the patient, and blood culture was conducted, which indicated the presence of Salmonella infection. Thus, the patient diagnosis was conclusive: mycotic aortic aneurysm due to Salmonella infection. After treatment with meropenem for 20 days, the temperature of the patient returned to normal. Half a year later, the patient suffered a sudden attack of hemoptysis, leading to death.
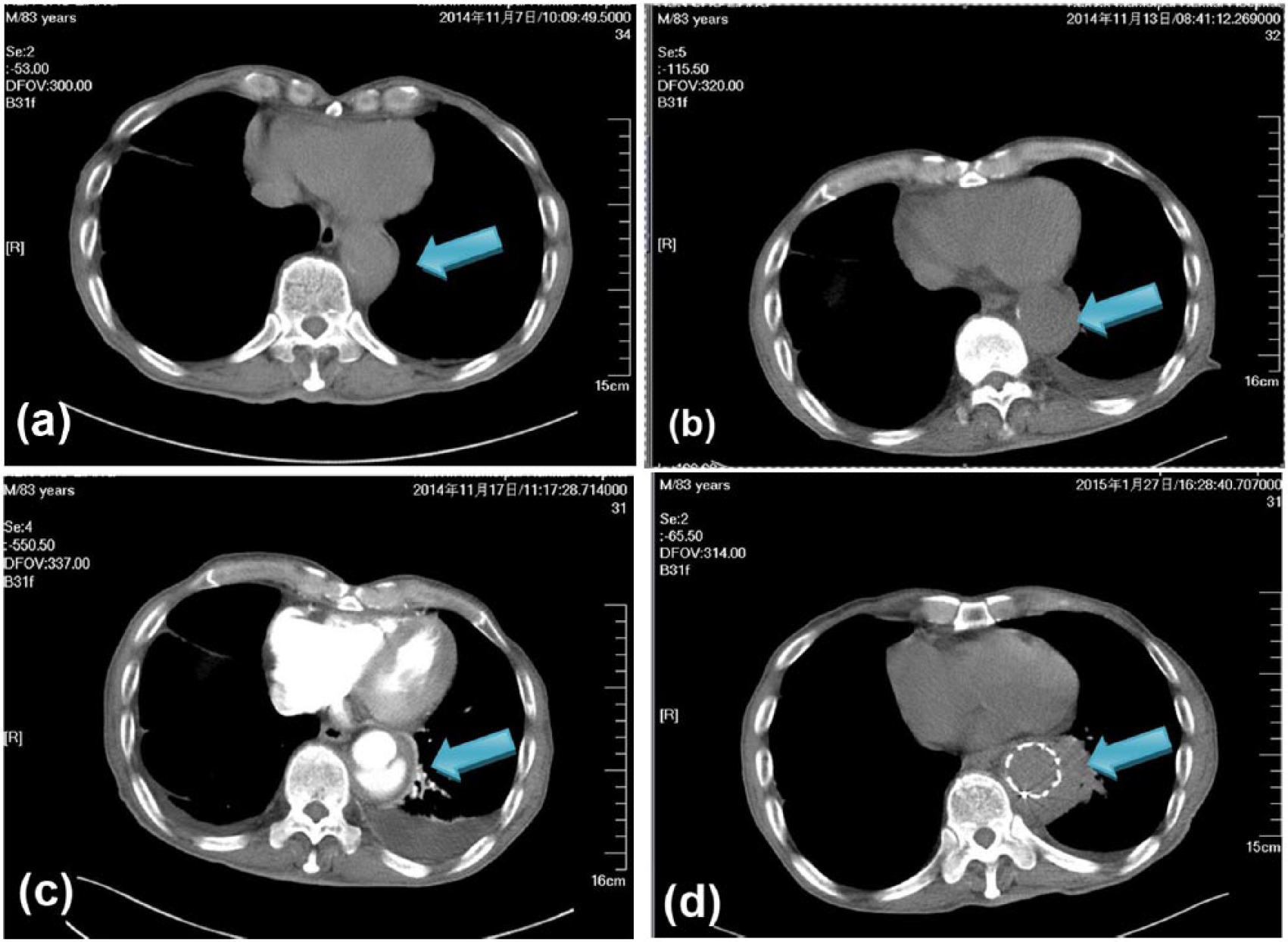
(a) CT scan of the chest on the first day of hospitalization: no significant aneurysm is detected, (b) CT scan of the chest after 6 days: widened aorta is observed (contrast-enhanced CT is recommended), (c) Contrast-enhanced CT scan of the chest shows thickening of the wall of the descending aorta and a low-density crescent in the cavity of the descending aorta. A double-cavity image is observed in the lumen of the aorta, which appears wide on the T10 to T11 horizon, with a maximum diameter of 5.3 cm. The probable diagnosis is aortic dissection with aneurysm and (d) CT scan of the chest 10 days after aortic dissection cavity isolation and contrast-enhanced CT scan of the chest. A metal holder is inserted inside the aorta. A low-density annular region around the aorta does not contain contrast media. The illustration above conformed to the changes after surgery.
Discussion
ADA rarely occurs and usually has a poor diagnosis and prognosis because of its acute progression and high mortality rate exceeding 90% in 3 months without treatment. 1 Possible leading risk factors for ADA include the following: hypertension, genetics, atherosclerotic disease, inflammatory reaction, congenital anomaly, iatrogenic injury, trauma, and gravidity, among others. 2 Despite the rare occurrence of the disease, the pathogenetic factor of infection that leads to ADA is even more rarely observed worldwide. A study indicates that mycotic aneurysm rarely occurs comprising 0.9% of cases of ADA. The cause could be identified as either infection after aneurysm or infection of arterial wall induced by aneurysm. Risk factors include arterial injury, bacterial endocarditis, hypoimmunity, and old age. 3 Thus, to potentially improve prognosis and targeted treatment, clinical physicians who encounter patients with ADA, febrile or not, should consider infection as a factor when none of the aforementioned risk factors are present. According to recent studies, pathogen testing indicates that Salmonella is the leading cause of aneurysm, comprising 75% of the cases. 4 The patient in the case report was verified to have ADA by contrast-enhanced CT of the chest and detection of Salmonella infection by blood culture. The case presents mycotic aneurysm due to Salmonella infection. A common food-borne pathogen, Salmonella is also an intracellular bacterium and usually causes gastroenteritis in those infected. People with Salmonella infection would typically suffer from gastroenteritis. In children, as well as in elderly and immunocompromised patients, Salmonella would be phagocytosed by macrophages but not killed. For the elderly, macrophages carrying Salmonella are eventually located in the atheroma and lead to infection, followed by ADA. 5 In addition to Salmonella, Staphylococcus aureus and Streptococcus rank as the second and third leading pathogenic bacteria causing mycotic aneurysm, with 16% and 5% rates of occurrence, respectively. 4 S. aureus mainly causes infection through risk factors such as repeated injection and arterial vascular damage, whereas Streptococcus is usually related to bacterial endocarditis. The infected region was often confirmed by tissue pathology and germiculture after surgery but not before the procedure, which may be traced back to the fact that the focus of infection is usually located inside the atheroma, causing a negative blood culture; consequently, the occurrence of ADA is either reduced or underestimated. However, 25% of germicultures exhibit electronegativity. 4 The case discussed is Salmonella-positive only according to serology.
The four possible routes leading to infection of mycotic aortic aneurysm include the following: (1) detachment of bacterial emboli secondary to bacterial endocarditis, (2) endarterium infected by pathogenic microorganisms, (3) bacterial infection secondary to already existing ADA, and (4) arterial wall damage during surgery, along with the presence of pathogenic microorganisms. The second and third routes are regarded as the most common reasons. Mycotic aortic aneurysm exhibits an extremely low morbidity. Therefore, the lack of large-scale clinical studies (most of the clinical articles are case reports) is inevitable given that the majority of the studies are animal experiments. Mycotic aortic aneurysm comprises 0.7%–2.3% of all aortic aneurysms, mostly affecting men; the male:female ratio is 2–4:1. Age of onset is from newborn to elderly, with the latter being the more affected group. Unlike atheromatous ADA (AADA), mycotic aortic aneurysm has no predilection site in the aortic segment, and no significant differences were observed in the incidence of all segments. Regardless, owing to tissue damage and rapid disease progression, mycotic aortic aneurysm has a considerably greater chance of rupture, compared with AADA. Meanwhile, the average diameter of rupture is considerably smaller in mycotic aortic aneurysm than in AADA. Generally, surgery is safe or no surgery is needed when the diameter of ADA is smaller than 5.5 cm; when the diameter reaches 3 cm, the rupture rate of aortic aneurysm becomes extremely high. Most studies indicate that the rupture rate ranges from 42.9% to 89.5%.6,7
The principles involved in the treatment of mycotic aortic aneurysm include bleeding control, infection elimination, and rebuilding of blood supply, together with sensitive anti-infective drugs and adequate duration of treatment. Salmonella and S. aureus are regarded as the most common bacterial pathogens associated with mycotic aortic aneurysm. Salmonella coverage remains difficult because it is an intracellular bacterium. Although ceftriaxone cannot cover S. aureus, it can cover Salmonella; thus, ceftriaxone is the preferred drug of choice. Once S. aureus develops in blood germiculture, vancomycin, teicoplanin, or daptomycin may be combined, with daptomycin as the preferred treatment. Regarding the duration of treatment, no consensus has thus far been reached and could vary from 6 to 8 weeks to a lifetime. Mycotic aortic aneurysm has a rather poor overall prognosis, with a considerably higher surgical risk than AADA. The mortality rate during the perioperative period is approximately 30%. Finally, thorough removal using any of the blood supply rebuilding methods is difficult to accomplish because of the deep location of the focus of infection; in addition, the rate of re-infection reaches 10%–30%, which is considerably higher than that in AADA. Overall, the 5-year survival rate is less than 50% according to various clinical observations. 8
Mycotic aortic aneurysm due to Salmonella occurs extremely rarely in China mainland. The reason is that the focus of the infection rarely occurs in the thoracic aorta and instead occurs in the abdominal aorta. However, AADA occurs mostly in this location. Therefore, the infective factor, along with the anti-infective treatment, is usually disregarded and cannot sufficiently counter Salmonella or S. aureus. In this case, the pre-surgical anti-infective treatment given prior to the removal of focus might have been insufficient, thereby stimulating the vascular wall and causing a new ADA, resulting in repeated occurrences of fever and massive hemoptysis, leading to death. In conclusion, giving importance to ADA treatment, in addition to surgical treatment, is highly recommended to doctors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.