
Abstract
The aim of this study was to investigate the efficacy of treatment for complex anal fistula with cutting hybrid seton combined with tube drainage. A total of 66 consecutive patients with complex anorectal fistulae were divided into two groups: experimental group (group A with 36 patients) underwent cutting hybrid seton placement plus tube drainage and control group (group B with 30 patients) underwent same procedure without tube drainage. Comparison of clinical outcomes between two groups was conducted. The success rate, time for healing of the wound, postoperative pain, and recurrence rate were analyzed. No patient was lost to follow-up. Some major clinical outcomes presented significant differences. Experimental group was superior than the control group in the aspects of success rate, time for healing of the wound, postoperative pain score, and recurrence rate. We can conclude that cutting hybrid seton placement with tube drainage was an effective procedure and valid alternative for complex anorectal fistula with a favorable result on higher healing rate, less postoperative pain, and few impact on the function of sphincter.
Introduction
The management of complex fistulas remains a formidable challenge as no single technique is appropriate in every case. 1 The reported recurrence rate is up to 40%. 2 Traditional cutting seton placement surgery always comes with problems of damage of the perianal structure and a risk of sphincter muscle dysfunction postoperatively. Some serious morbidities such as incontinence, anorectal stricture, deformation, and recurrency are decreasing quality of life of patients after surgery. 3 An oldest and simple technique is to use a cutting seton. 4 To achieve the goal of reducing the complications associated with seton use and to improve certain weakness of this surgery, we modified the procedure with postoperative tube drainage and compared and evaluated the result with the observation group that did not receive tube drainage treatment.
Materials and methods
Ethical and informed consent
This research was approved by the Ethic Committee Approval Certification of Human Subject Research of the First Affiliated Hospital of Xinjiang Medical University. All participants and patients whose age ranging from 18 to 65 years old signed informed consent before this study. There were no child patients enrolled in this study. There were no commercial conflicts or other problems related to the participants. All anal examination was free to all the participants.
Patient selection
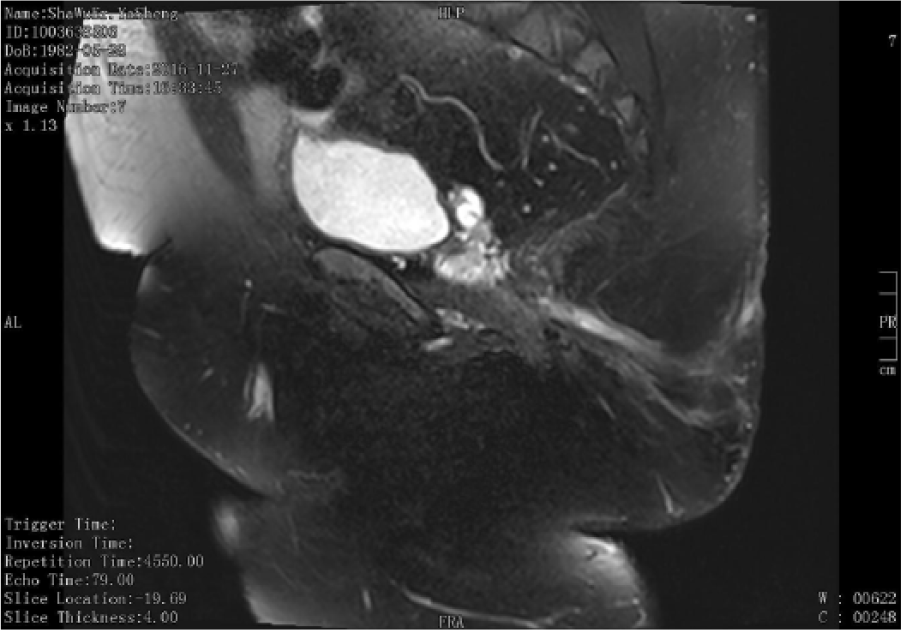
In all, 66 patients, 36 male and 30 female, mean age 36.5 years ranging from 18 to 65 years old, suffering duration 2–10 years who admitted to Anorectal Surgical Department of First Affiliated Hospital, Xinjiang Medical University from March 2013 to July 2016, were enrolled in this study. All patients were diagnosed with high complex suprasphincteric fistula according to the Association of Coloproctology of Great Britain and Ireland (CPGBI) Position Statement. 5 All the fistulas were suprasphincteric fistulas, and all fistulas meeting the inclusion criteria were preoperatively assessed by physical examination and confirmed with endoanal ultrasound, as common clinical practice in our hospital. The diagnosis of suprasphincteric fistula-in-ano was made by the medical history and physical rectal examination, fistulography, endoanal ultrasound, and magnetic resonance imaging (Figures 1–4). Additional imaging with nuclear magnetic resonance fistulography was obtained in selected cases. Patients were randomly divided into two groups: experimental group (group A) consisted of 36 patients, who underwent cutting hybrid seton placement plus tube drainage, and observation group (group B) contained 30 patients who underwent only traditional cutting hybrid seton placement.

MRI findings of complex fistula-in-ano.

MRI findings of complex fistula-in-ano.
MRI findings of complex fistula-in-ano.

MRI findings of complex fistula-in-ano.
Surgical technique
Group A
All patients underwent preoperative regular test, endoscopy, anorectal ultrasound, and mechanical bowel preparation before surgery. Patients were placed in lateral or lithotomy position under spinal anesthesia. After primary opening was located with fistula probe, all fistula tracts were irrigated with a hydrogen peroxide solution. A flexible metal fistula probe was gently passed through the fistula tract from the secondary opening and pulled out through the primary opening. After the fistula tract was identified, mucosa of internal opening and skin overlying the fistulous tract were incised, the portion of the tract outside was put lay-open and curetted, to clear any potential lateral secondary tracts and to make sure postoperative drainage. The latex circular hybrid seton which is cut from the end of a surgical glove was tied to the tip of the metal probe and inserted through the main tract in a double-strand fashion, or it was pulled into position using a silk suture. Then, the hybrid seton was tied over itself or with a silk suture on the sphincter tightly. After eliminating the sepsis and necrotic tissue of suprasphincteric fistula tract which passed upward in the intersphincteric plane, a silicone tube is put at the top of the cavity and fixed with the skin. The incision should be managed carefully to make sure not being closed at early postoperative days. Postoperatively, gentle cleaning of the anal region with warm water and metronidazole after each bowel movement was advised, combined with traditional Chinese medicine treatment regularly. The patients were informed about the possible serous discharge that would continue until the hybrid seton dropped, and the wound healed.
Group B
All patients underwent a similar surgical procedure as described for group A, but the difference in group B is that they only received the treatment of eliminating the sepsis and necrotic tissue of suprasphincteric fistula tract without tube drainage.
Assessment of success
The efficacy of surgery is evaluated according to Guidelines for Fistula-in-Ano: 6 Healed, completely disappearance of clinical symptoms and signs, and completely healing of wound; Excellence, disappearance of most of the clinical symptoms and signs, and healing of the wound; Effective: disappearance of part of the clinical symptoms and signs, without completely healing of the wound; Ineffective: Persistent symptoms and signs, without healing of the wound. Overall healing rate (%) = (No. of the Healed + Excellence + Effective patients)/ total no. of patients ×100%. Other aspects to compare are time for healing of the wound, postoperative pain score, and anal sphincter function score. Postoperative pain was evaluated with a visual analog score (VAS) on the first and seventh postoperative days.
Postoperative anal incontinence
Postoperative anal incontinence scores of each group were assessed with the Cleveland Clinic Incontinence Score (CCIS) system at postoperatively at 6 months. Continence was assessed by the patient’s ability to hold solid stool, liquid stool, and flatus and by the assessment of anal sphincter tone during rectal examination. No anal manometry was performed because of diversity of anorectal pressure in different period of management or different patients with different nations.
Follow-up
The primary endpoint of this study was success or failure of treatment. Success was defined as closure of both internal and external openings, absence of purulent drainage, and absence of abscess formation. First-line assessment was performed using the entire series of patients. Considering that most recurrences occurred within 6 months of the procedure, a secondary evaluation was performed on the series of patients healed at the 6-month time point to explore the pattern of outcomes achieved after healing at 6 months had been confirmed. Postoperatively, patients were assessed for complications by follow-up visit to the clinic at 1 and 6 weeks, 6 months post-surgery. No patients were lost to follow-up in this study.
Statistical analysis
The Excel data statistical analysis was performed using SPSS software version 19.0. The intention-to-treat principle was applied in this study. Data outside the normal range data are expressed as medians and full ranges. The values of the numerical data are expressed as median and ranges. Student’s t-test was used to compare the treatment results, and the chi-square (χ2) test was used for the comparison of proportions. Each intervention option was assessed by Fisher’s exact test. Healing time and postoperative pain were calculated by Wilcoxon’s test or log-rank test. P < 0.05 was considered statistically significant.
Results
Comparison of baseline data
All patients had no particular complications related to surgery. There were no statistical differences between the participants in the two groups with regard to age and gender, or the persistent symptoms. The general characteristics of the two groups showed no significant differences (P > 0.05; Table 1).
The general characteristics of the two groups.

Comparison of healing rate of the two groups
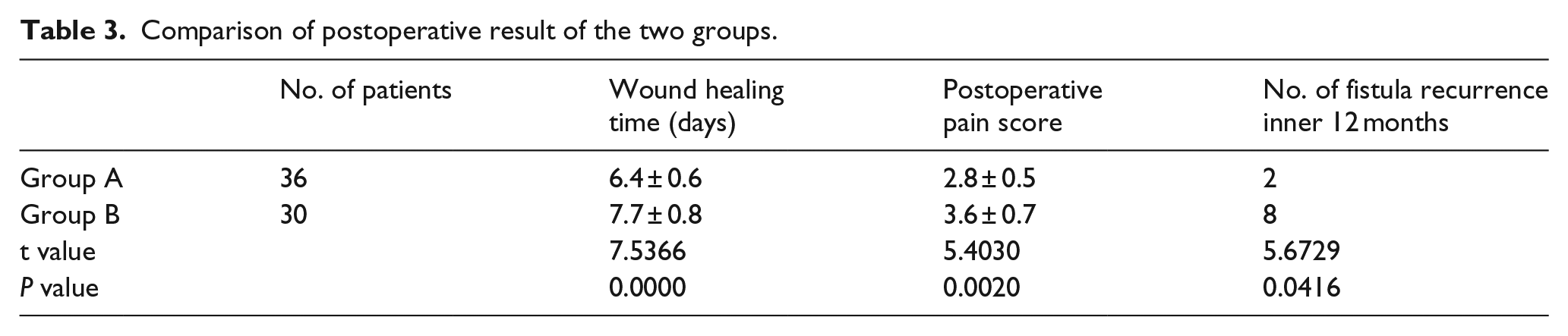
According to our preliminary results, the efficiency of hybrid seton placement with tube drainage was better than without tube drainage. Experimental group was superior than the control group in the aspects of success rate, time for healing of the wound, postoperative pain score, and recurrence rate (P < 0.05; Tables 2 and 3). However, anal continence score results of two groups were not statistically significant. In our final step, we did not find incontinence of liquid stool and flatus in the two groups.
Comparison of healing rate of the two groups.

Comparison of postoperative result of the two groups.
Discussion
Fistula-in-ano is an old and common disorder in general surgery. A simple laying-open procedure is effective for simple or low fistula. However, it also presents as a surgical hazard because of the high recurrence rate and risk of incontinence that may occur, especially in patients with a complex or higher, multiple-tract fistula. Surgery was considered a radical treatment of the disease. Although a broad spectrum of modalities has now been applied to clinical practice, it still needs to be standardized. The ideal modality of complex anorectal fistula treatment usually has the merit of low recurrence rate, minimal incontinence, and improvement of patients’ quality of life. High complex fistula could be suffered at any age. However, it is considered to happen more frequently in male gender. 7 Recent evidences showed that there are no statistical significance in circulating sex hormone levels between patients with fistula-in-ano compared with matched controls. 8 Fistulotomy is now considered an improper option when the fistula tract incorporates a significant amount of the internal and external anal sphincter, as in many cases of high, complex, trans-sphincter fistulae. Regarding complex trans-sphincteric or suprasphincteric anal fistula, the internal opening begins above the anal sphincter, meaning that fistula tract passed through the external sphincter at a varying level or passed upward in the intersphincteric plane before looping over the puborectalis muscle to penetrate the levator ani muscle. 9 Surgery is the mainstay of therapeutic method, but it usually results in large wounds which can take months to heal and, moreover, has a risk of fecal incontinence because of the damage of the anus. To date, none of the single procedures can be considered a perfect standard, and for this reason, a variety of novel surgical methods have been introduced that aim to improve efficacy. Therapeutic methods for anal fistula range from fistulectomy, fistulotomy, draining and cutting setons, rectal mucosal or advancement flaps, 10 anal fistula plug, 11 ligation of the intersphincteric fistula tract (LIFT), 12 or fibrin glue. The intervention for complex fistulas should balance the outcomes of cure and continence.
This study used a simple tube drainage after cutting hybrid seton placement (Figures 5–7), aiming to completely eliminate deep focal lesion and sufficient drainage, to decrease postoperative morbidity and recurrence. Compared to hybrid seton placement without tube drainage (Figure 8), our new technique could have better result after 6-month follow-up. In our study, the overall success rates were 100% and 82.22%, respectively, for group A and B and showed statistical significant differences (P < 0.05). Wound healing period and postoperative pain score also demonstrated an improvement after when applied tube drainage method, presented statistical significance (P < 0.05). On the other hand, anal sphincter function did not show significant difference in the two groups. Tube drainage of our procedure after seton placement could overcome high recurrent rate after surgery.

Hybrid seton with tube drainage (case 1).

Hybrid seton with tube drainage (case 2).

Hybrid seton with tube drainage (25th day post-surgery).

Hybrid seton without tube drainage.
Besides healing, continence is the next goal to be achieved. Related literatures report a 0%–5% rates of incontinence when hybrid seton treatment is applied.13,14 Another consequence aspect is recurrence rate. It is reported that using a variety of hybrid seton materials and varying methods, recurrence or persistence rates are 0%–18%. No major anal incontinence and recurrence has been reported by our patients during follow-up period. Tube drainage technique was reported previously, 15 and the fistula was cured in 18 (75%) of the 24 patients in whom the tube remained in place. Compared with that report, our result was encouraging. The difference in our work compared with that study was that we compared two different methods of seton placement with or without tube drainage.
According to our preliminary result, the efficiency of hybrid seton placement with tube drainage was better than without tube drainage. We found that hybrid seton placement with tube drainage can clearly improve the efficiency of suprasphincteric fistula-in-ano. This technique helps to delay closure of the external opening as long as required. Hybrid seton placement with tube drainage can be used to facilitate closure of the long deeper part of the tract by preventing premature closure of the external opening. This point was just the new finding or novelty of our research.
Footnotes
Acknowledgements
The authors would like to thank to Chen Hui and Maimaitituerxun Tuerdi in the Xinjiang Medical University for their contribution and help of data source and recording work. The authors would like to thank to Adali and Prof. Xiang Yan of Xinjiang Medical University for their technical support to the protocol and careful statistical assistance to the data. The authors thank Dr Turgunjan Tuerxun of Xinjiang Medical University and Prof. Adili Abudoureyimu of ATLAN international Language Center for their careful language assistance.
Author contributions
M.M.T.J.A.B.B.K.R. contributed to conception and design and ultrasound technique (critically important intellectual content) and substantial contributions including research and study design. A.W. contributed to data source, recording, acquisition of data, and final approval of the version to be published. I.B. contributed to the analysis and interpretation of data.
Data sharing and biostatistical statement
Technical appendix, statistical code, and dataset of this original article are available from the corresponding author at
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the National Natural Science Fund, Healing Pathogenesis of Anorectal Fistula Using Fistula Plug, Fund Serial Number: 81460133; Innovation program of regional cooperation of Xinjiang Autonomous Region, Fund Serial Number: 2016E02063.